
Abstract
Objective:
To evaluate the effectiveness and safety of oral administration of Linfadren® in addition to conventional treatment in patients with post-trauma/surgery persistent hand edema.
Design:
Parallel-group randomized controlled trial.
Setting:
Outpatient rehabilitation center.
Subjects:
A total of 60 outpatients (mean age 48.5 (standard deviation (SD) = 12.3) years) with post-trauma/surgery persistent hand edema.
Interventions:
Patients were randomized to either receive six-week conventional treatment plus Linfadren® (Study Group) or conventional treatment (Control Group).
Main Measures:
Primary outcome was hand edema as measured by figure-of-eight method. Secondary outcomes were hand function, patient’s overall perceived treatment effectiveness and rescue medication request. Tolerability of Linfadren® was also evaluated. Assessments were performed at baseline, at the end of treatment and three months after the end of treatment.
Results:
All patients completed the six-week program and 57 patients (95%) completed the three-month follow-up. At six weeks, the Study Group had significantly greater improvement in hand edema (423.3 (SD = 23.8) mm vs 439.4 (SD = 22.6) mm; P = 0.009) and upper limb function (Quick Disabilities of Arm, Shoulder and Hand questionnaire: 23.6 (SD = 13.6) vs 37.7 (SD = 15.9); P = 0.005) compared to the Control Group. Moreover, the percentage of patients who perceived treatment as effective was significantly higher in the Study Group than in the Control Group both after treatment (70% vs 37%, P = 0.002) and at follow-up (77% vs 30%, P < 0.0001). The rescue medication request was not different between groups. No adverse events were recorded.
Conclusion:
Linfadren® in addition to conventional treatment was safe and more effective than conventional treatment alone in patients with post-trauma/surgery persistent hand edema.
Introduction
Hand edema following trauma or surgery of distal forearm or hand is a normal response to the injuries of soft or bone tissues. 1 However, a persistent edema beyond two weeks leads to pain and functional limitation, delays the healing process and contributes to chronic hand disability and diminished quality of life.2–4
Currently, persistent edema is managed with conventional therapy including elevation of the injured limb, various forms of cryotherapy, external compression, active and passive exercises, different types of massage and therapeutic modalities.4–7 These interventions primarily remove fluid congestion from the tissues, without completely reducing the concentration of proteins in the interstitium. 8 The persistence of a high concentration of proteins in the interstitium maintains high oncotic pressure, which creates a vicious cycle with additional edema formation. 8
Therefore, a pharmacological treatment that could reduce the stagnant protein excess as well as fluid congestion from the interstitium is of interest in the management of persistent edema.
Benzopyrones (including diosmine and coumarin) are a group of drugs that have been found to be successful in treating lymphedema and chronic venous disease.9–14 Linfadren® (OMEGA PHARMA Srl, Cantù (CO), Italy) is a marketed formulation, which contains 200 mg of diosmin, 30.6 mg of coumarin and 3.7 mg of arbutin. The purpose of this study is to investigate the effectiveness and safety of Linfadren®, when used in addition to conventional treatment normally used in the management of patients with post-trauma/surgery persistent hand edema.
Methods
This randomized controlled clinical trial was carried out according to the Declaration of Helsinki and the International Conference on Harmonization Good Clinical Practice (ICH-GCP) guidelines in an outpatient rehabilitation center and at the University of L’Aquila between July 2017 and May 2018. The study was approved by the local institutional review board of the University of L’Aquila (Prot. 30262) and was registered at ANZCTR with the number ACTRN12618001033235.
The sample size calculation was based on the primary outcome using MedCalc (version 11.1.1.0 for Windows; MedCalc Software, Mariakerke, Belgium). It was assumed that at the end of treatment, patients in the study group would have a mean reduction of 25 mm, while patients in the control group would have a mean reduction of 10 mm, with a common standard deviation (SD) of 15 mm. Based on this, and assuming a level of significance of 5% and a power of 95%, the number of patients needed was calculated to be 26 per group. Assuming a dropout of 15%, 30 patients per group were required.
All patients who are potential candidates for the treatment in routine clinical practice should be considered eligible for a pragmatic trial, including vulnerable populations. Patients with known contraindications should be excluded.
All patients who met the inclusion criteria and were potential candidates for the treatment that we usually applied in our clinical practice were eligible for this study. Inclusion criteria were 18 years or older, diagnosis of post-trauma/surgery persistent hand edema with a difference of ⩾20 mm between the affected hand and the unaffected hand as measured by figure-of-eight method.15–17 Persistent edema was an edema that persisted for more than two weeks. 18 Exclusion criteria were bilateral hand edema; pulmonary edema; congestive heart failure; coagulation defects; history of inflammatory, metabolic or neuropathic arthropathies; treatment with anticoagulant drugs; any contraindications limiting clinical evaluation and therapy of the patient. Therapy with low-molecular-weight heparin at preventive doses was not a contraindication for inclusion in the study.
Patients who met the inclusion criteria were informed with verbal and written information regarding the research and were then asked to give a written informed consent. Patients agreeing to participate in this study were randomly allocated into study and control groups with a computer-based 1:1 randomization scheme and sealed envelopes prepared by an assistant researcher at the University of L’Aquila, who was independent of the recruitment process. We elected to use randomized blocks with equal size using “Random Allocation Software” (Version 1.0, May 2004; Department of Anesthesia, Isfahan University of Medical Sciences, Isfahan, Iran) for parallel-group trials.
Patients in both groups were treated with a conventional treatment, as defined by Miller and colleagues, 2 including elevation, low-compression garments, retrograde massage and gentle hand movement, which are commonly performed in our outpatient rehabilitation centers to patients with post-trauma/surgery persistent hand edema. Patients in the study group received the same conventional treatment of the control group plus supplementary Linfadren®.
Conventional treatment was performed once a day by the same physiotherapist for five days a week for six weeks. Patients of Study Group were instructed to take Linfadren® on an empty stomach twice a day (at six-hour intervals: 11 a.m. and 5 p.m.) for two weeks and once a day for four weeks. In this study, Linfadren® was prescribed by physicians and purchased at the chemists by patients.
Pre-existing conditions or intercurrent diseases could be treated with commonly taken drugs. Taking of paracetamol tablets (1 g every six hours up to a maximum of 3 g daily) was permitted to the patients, as rescue medication, to treat pain in the hand or any other pain (e.g. headache) or fever (e.g. due to common cold) that they might experience during the study period. Other analgesic/anti-inflammatory agents (topical or systemic), modalities and alternative treatments (e.g. acupuncture, homeopathy) were not permitted during the study period.
To improve adherence to treatment with Linfadren® and also to monitor the consumption of the rescue medication, we asked patients to keep a daily diary. Patients were evaluated at three different times: at baseline, at the end of treatment (six weeks after baseline) and three months after the end of treatment (follow-up) by an independent physician blinded to the allocation and not involved in the treatment procedures and nor in data analysis. In the first assessment, the physician provided verbal and written information about the study (including that patients would be randomized to one of two groups and that each group would be managed with different but appropriate treatments), checked inclusion and exclusion criteria and, from those patients who agreed to participate in the study, collected the signed informed consent and scheduled an appointment with a physiotherapist for assigned treatment.
Our primary outcome measure was the reduction of hand edema as evaluated by figure-of-eight method, which is a valid and reliable instrument for measurement of hand edema following trauma or surgery.15–17 The secondary outcomes were the evaluation of the improvement of hand function, the patient’s overall perceived treatment effectiveness and the rescue medication request. Hand function was assessed using the Quick Disabilities of Arm, Shoulder and Hand questionnaire (QuickDASH), 19 which has also been validated in patients undergoing rehabilitation after hand injuries. 20 It consists of 11 core items designed to measure physical function, symptoms and social function and two optional items (musical or sport performance and work), which generate a disability score, ranging from 0 (no disability) to 100 (the most severe disability). 19
The patient’s overall perceived treatment effectiveness was assessed using a 5-point Likert-type scale ranging from “extremely effective” to “not at all effective.” Success rates were calculated by dichotomizing responses. Patients who referred to effectiveness of treatment as “extremely effective” or “very effective” were counted as successes, whereas patients who referred to treatment effectiveness as “somewhat effective,” “poorly effective” or “not at all effective” were counted as failures.
To evaluate the amount of rescue medications taken during the study period, we used the patients’ daily diary. To evaluate the tolerability of the Linfadren® during the course of treatment, patients underwent a complete laboratory examination, including hematology, blood chemistry and urinalysis both before and after treatment. Patients also underwent a clinical examination to record vital signs and were asked to record all the adverse effects they observed.
A two-sample unpaired t-test and Chi-square (χ2) or Fisher’s exact test were applied to compare the differences in continuous and categorical variables, respectively. A two-way analysis of variance (ANOVA) with group (study vs control) as the between-subject factor and time (baseline–six weeks–three months) as the within-subject factor, followed by a Tukey post hoc comparison, was used to assess the presence of significant differences between the study and control groups for hand edema measured by figure-of-eight method and for hand function assessed by QuickDASH questionnaire.
All analyses of the primary and secondary outcome measures were performed according to the principle of intention-to-treat. The intention-to-treat analysis was carried out according to a “worst-case scenario” analysis. 21
The P values (two sides) less than 0.05 (P ⩽ 0.05) were considered significant. A 95% confidence interval (CI) was also calculated. MedCalc software (version 11.1.1.0 for Windows; MedCalc Software, Mariakerke, Belgium) was used.
Results
Among 73 eligible patients, 5 did not meet the inclusion criteria, 3 met the exclusion criteria and 5 refused to participate (Figure 1). Therefore, 60 patients (36 women and 24 men, with an average age of 48.5 (SD = 12.3) years, range 22–69 years) who satisfied the required sample size were enrolled for this study. The baseline characteristics that were similar and without statistical significance for both groups are shown in Table 1.
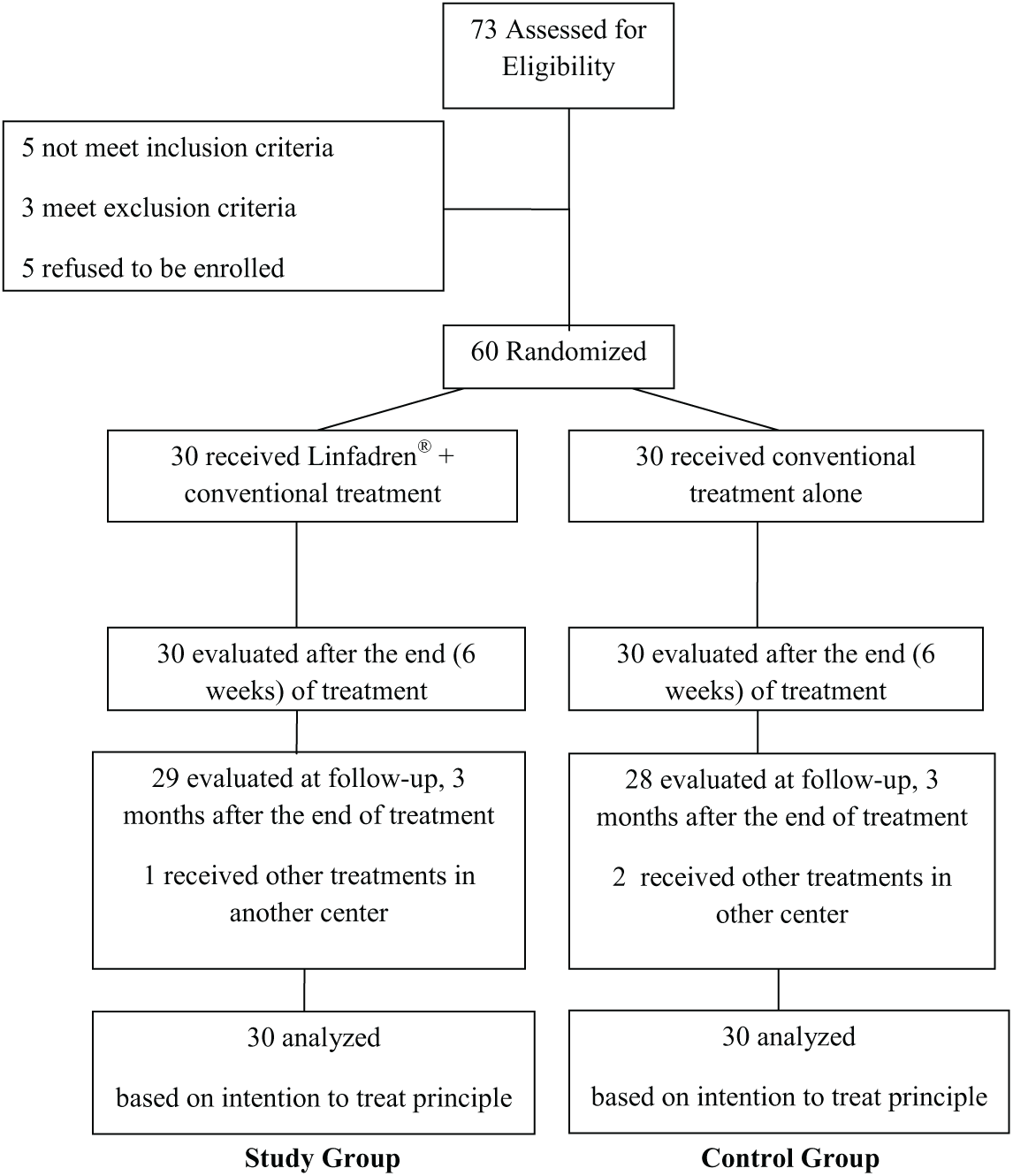
Flowchart of the study (CONSORT Diagram).
Baseline characteristics of the study and control groups.
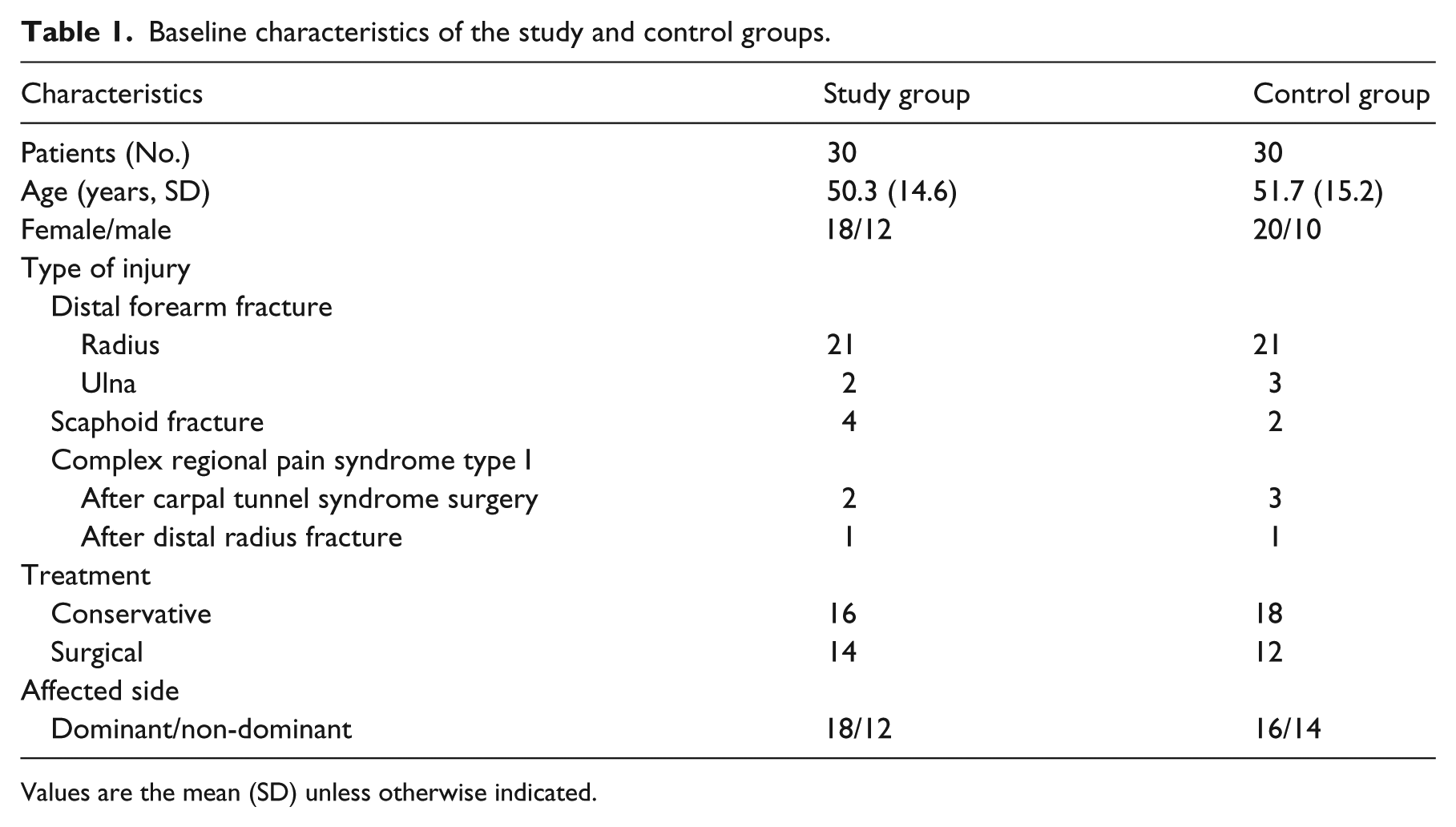
Values are the mean (SD) unless otherwise indicated.
All patients were re-examined at the end of treatment, whereas three months after the end of treatment (follow-up), three patients left the study (Figure 1). Nevertheless, based on the intent-to-treat principle, 21 the data for these three patients were included in the data analysis.
In the between-group analysis (Table 2) both at the end of treatment and at three months after the end of treatment, the amount of change in the hand edema and in hand function between the Study Group and the Control Group showed statistically significant differences: the reduction of hand edema and the improvement in hand function in the Study Group were significantly larger than those in the Control Group.
Comparison of hand edema (as measured by Figure-of-Eight method) and hand function (as measured by QuickDASH questionnaire) in the study and control groups.

CI, confidence interval; MD, mean difference.
Values are the mean (SD).
Six weeks after baseline.
Three months after the end of treatment.
The within-group analysis showed statistically significant differences at the end of treatment in the Study Group, but not in the Control Group, with respect to the reduction of hand edema (Study Group: −31.1 (SD = 14.3) mm, P = 0.0004; Control Group: −11.2 (SD = 9.4) mm, P = 0.2) and improvement of hand function (Study Group: −22.6 (SD = 8.4) points, P < 0.0001 vs Control Group: −7.1 (SD = 3.8) points, P = 0.07). At three months after the end of treatment (follow-up), the reduction of hand edema, in both groups, was not significant compared to the reduction measured at the end of the treatment (Study Group: −3.9 (SD = 6.9) mm, P = 0.4; Control Group: −3.7 (SD = 5.8) mm, P = 0.5). The analysis of hand function, between the end of the treatment and three months after the treatment, showed a not significant improvement in the Study Group (−5.1 points, P = 0.2) and a not significant worsening in the Control Group (+2.1 points, P = 0.6).
The patient’s overall perceived treatment effectiveness of both groups are shown in Table 3. The Study Group obtained the best results, with a statistically significant differences both at the end of treatment (P = 0.002) and at three months after the end of treatment (P < 0.03).
The patient’s overall perceived treatment effectiveness as assessed by 5-point Likert-type scale in the study and control groups.
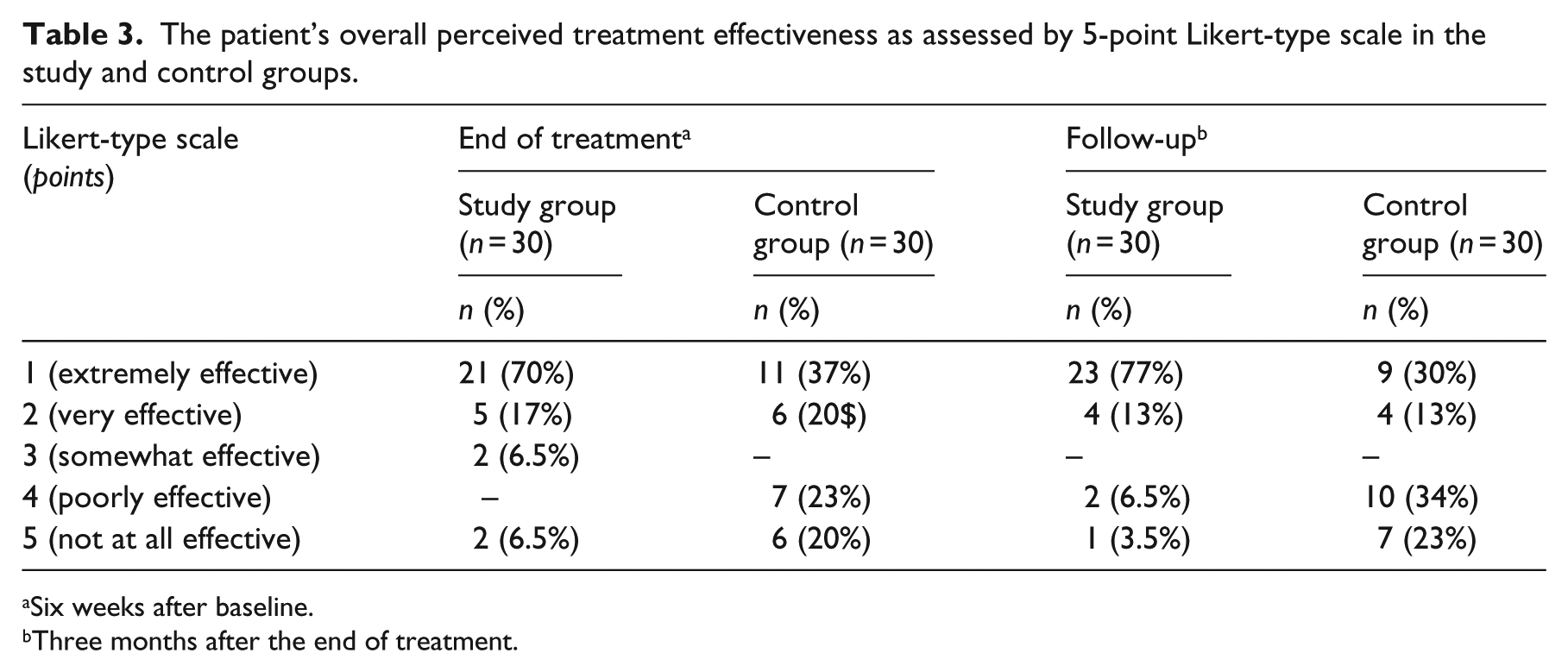
Six weeks after baseline.
Three months after the end of treatment.
A total of eight patients in the Study Group and 10 patients in the Control Group (P = 0.8) took paracetamol as rescue medication; the mean number of tablets taken was 5.7 (SD = 3.4) and 6.6 (SD = 4.1) in the study and control groups, respectively. No statistically significant difference (mean difference (95% CI) = 0.9 (−1 to 2.8), P = 0.3) was observed between the two treatment groups.
No adverse events were recorded during the study in either group. The results of the clinical and laboratory examinations revealed no signs of systemic toxicity due to Linfadren® administration.
Discussion
Our results showed that the patients treated with both Linfadren® and conventional treatment achieved better results, both at the end of treatment and at three months after the end of treatment, than those treated with conventional treatment alone, in terms of hand edema reduction, functional improvement of the affected hand and in patients’ overall perceived treatment effectiveness.
No difference was observed between the two groups in the consumption of rescue medication (paracetamol). Despite factors responsible for the pathogenesis of persistent edema have not yet been clearly understood, 22 the involvement of the lymphatic system has received little attention in the formation of persistent edema. Our results would seem to confirm that besides the venous system, the lymphatic system is also involved in the pathogenesis of persistent edema, as suggested by previous studies.5,23 The effectiveness of Linfadren® in our patients, may explain, at least in part, why many of the strategies used until now to manage persistent edema have not produced the expected results.
The two main components of Linfadren®, coumarin and diosmin, have been used in the management of lymphatic disorders showing good results.9–12,24 The mechanism by which the two main components of Linfadren®, coumarin and diosmin, act to improve the function of lymphatic system are still poorly understood. It has been postulated that coumarin activates proteolytic activity of macrophage, 11 and diosmin acts on the lymphatic system by increasing lymph flow and lymph oncotic pressure. 13 It has been shown that the activation of the lymphatic system facilitates the removal of high-protein edema,18,25 counteracting the persistent edema. This possibility is supported by data from this study wherein Linfadren® increases the reduction of the post-trauma/surgery persistent hand edema in our patients.
Although a direct comparison with other studies is difficult due to differences in patient characteristics as well as in the drugs and dosages used, our findings are an important extension of previous studies showing the effectiveness of coumarin and diosmin in lymphatic disorders, particularly if used in combination with conservative treatments.9–12
In our study, Linfadren® was well tolerated and remarkably free of systemic adverse effects. Regarding the supposed hepatotoxicity of coumarin, no hepatotoxic effect was found in our study at doses of 61.2 for two weeks and 30.6 mg/day for four weeks. Analyzing the literature, it would seem that greater toxicity has been found at doses of 400 mg/day, 26 while poor and transient effects have been reported at doses of 135 and 90 mg/day. 27 Taken together, the foregoing findings would seem to suggest that the possible adverse effects of coumarin are dose-dependent.
The strengths of this study are its randomized prospective design in a real-scenario, blinded collection of data and the fact that this is, to our knowledge, the first trial comparing the association of a supplement drug as Linfadren® to conventional rehabilitation treatment with respect to conventional rehabilitation treatment alone in patients with post-trauma/surgery persistent hand edema.
Possible limitations of our study are the small number of patients enrolled, although it did meet the power requirement, and the results proved to be very consistent; the lack of a true placebo-control group, which we did not include due to the pragmatic nature of the study; and a follow-up period that was not sufficiently long enough to determine the long-term effects of both treatments used.
Finally, this is a single-center study, thereby its external validity could be not guaranteed. Due to aforementioned limitations, extrapolation of our results to the general population should be done with caution, and additional studies in patients with post-trauma/surgery persistent hand edema of other anatomic areas, such as the ankle, or with a long-term follow-up period are needed to confirm these findings and to improve generalizability of recruiting trial patients from different settings. 28
Moreover, mechanisms of action, the most suitable dosage, interaction with other therapeutic strategies and cost/effectiveness results of Linfadren® are not fully known and they need to be investigated, so that it can be applied more efficiently.
Nevertheless, our data indicate that Linfadren® must be considered a valuable, safe and effective supplement drug, in synergy with conventional treatment, in the management of patients with post-trauma/surgery persistent hand edema.
Clinical message
Linfadren® when used in combination with conventional treatment seems to provide a greater reduction of hand edema with respect to conventional treatment alone in patients with post-trauma/surgery persistent hand edema.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.