
Abstract
Objectives:
The aim of this study was to determine the efficacy of cycling to improve function and reduce activity limitations in children with cerebral palsy; the optimal training parameters for improved function; and whether improvements in function can be retained.
Method:
Six databases were searched (until February 2019) and articles were screened in duplicate. Randomized or quasi-randomized controlled trials and pre–post studies were included. Methodological quality was assessed using the Downs and Black scale. Outcomes were reported under the International Classification of Functioning, Disability and Health domains of body functions and activity limitations. Quantitative analyses were completed using RevMan V5.3.
Results:
A total of 533 articles were identified and 9 studies containing data on 282 participants met full inclusion criteria. Methodological quality ranged from low (14 of 32) to high (28 of 32). Significant improvements were reported for hamstring strength (effect size = 0.77–0.93), cardiorespiratory fitness (effect size = 1.13–1.77), balance (effect size = 1.03–1.29), 3-minute walk test distance (effect size = 1.14) and gross motor function (effect size = 0.91). Meta-analysis suggested that cycling can improve gross motor function (standardized mean difference = 0.35; 95% confidence interval = (−0.01, 0.70); P = 0.05); however, the effect was insignificant when a poor-quality study was omitted.
Conclusion:
Cycling can improve muscle strength, balance and gross motor function in children with cerebral palsy; however, optimal training doses are yet to be determined. There was insufficient data to determine whether functional improvements can be retained. Conclusions were limited by small sample sizes, inconsistent outcome measures and a lack of follow-up testing.
Introduction
Children with cerebral palsy experience varying degrees of muscle weakness, muscle contracture, spasticity, impaired balance and coordination that limit their functional capacity to perform activities such as running, jumping, climbing and cycling.1,2 This reduced capacity to perform typical childhood activities contributes to low habitual physical activity and declining gross motor function in adolescence2,3 and has resulted in a global call for physical activity interventions appropriate for this population.4,5
Adapted cycling offers an alternate mode of exercise for people with mobility restrictions, including children with cerebral palsy. 6 Both stationary and dynamic forms of cycling can be adapted to suit a variety of physical requirements, making it an ideal form of physical activity for children who cannot participate in traditional gym-based programmes.7,8 Adapted cycling has also been advocated to improve well-being and social participation, allowing children to keep up with friends and to participate in family outings.6,9,10 Despite the postulated benefits of adapted cycling for children with cerebral palsy, there is a paucity of literature on the efficacy of cycling as an intervention to improve functional performance.
It is necessary to establish optimal training guidelines for adapted cycling to ensure that programmes are appropriately dosed for functional improvement and retention. This information is important to (1) assist families to weigh up the benefits of cycling in the context of alternative therapies, (2) to help service providers to justify the time and costs associated with delivering cycling interventions and (3) to help clinicians advocate for funding for families who wish to purchase cycling equipment for ongoing use in the community. The International Classification of Functioning, Disability and Health, known more commonly as the ICF, provides a framework to compare the efficacy interventions across multiple studies. 11 Within the ICF framework, outcomes related to functional performance can be categorized according to ‘body functions’ and ‘activity limitations’. To date, a comprehensive review of the efficacy of adapted cycling to improve functional performance in children with cerebral palsy has not been conducted.
Our primary objective was to determine the efficacy of cycling interventions to improve body functions and reduce activity limitations in children with cerebral palsy compared to alternative therapies or no intervention. Our secondary objectives were to explore the components of cycling interventions (such as frequency, intensity, duration, type and setting) that contributed to improved function and to determine whether effects are retained beyond the immediate intervention.
Methods
Prior to conducting this review, the International Prospective Register of Systematic Reviews was searched for existing systematic review protocols on cycling in children with cerebral palsy. A detailed protocol was then developed and registered online (CRD42017069603).
A comprehensive search strategy was developed with assistance from a health research librarian and used to identify articles in SCOPUS, PubMed, CINAHL, EMBASE, SPORTDiscus and the Cochrane Library. Each database was searched from inception through to February 2019. The exact search strategy is provided in Supplemental Appendix 1. The abstracts of studies identified through the database searches were screened by two reviewers (E.L.A. and S.S.), and an independent full-text review was completed for all articles that met the inclusion criteria. The reference lists of included studies were also searched for eligible studies and forward searches were conducted using Google Scholar. Discordance over study inclusion was confirmed by the third reviewer (M.J.K.).
Studies were included if (1) the study design was a randomized or quasi-randomized controlled trial (RCT), pre–post study with controls (n ⩾ 10 in the intervention group) or single-group pre–post study (n ⩾ 10) with a baseline and withdrawal phase (i.e. A-B-A design); (2) at least 80% of participants were aged 2–18 years with a diagnosis of cerebral palsy; 12 (3) the intervention was any upper or lower limb cycling task (e.g. recreational, static, dynamic, functional electrical stimulation, virtual or motor-assisted cycling); (4) at least one outcome was related to the body function or activity domains of the ICF and was assessed using a valid outcome measure; and (5) the intervention was compared with standard or usual care, no intervention or an alternate intervention.
The authors chose to include pre–post study designs due to the limited number of RCTs identified in preliminary searches. Non-RCTs should be considered for inclusion in systematic reviews when there are limited studies available, as they can provide meaningful information about intervention effectiveness and adverse events. 13 To minimize the risk of bias associated with including less rigorous research designs, non-RCT studies were only eligible if 10 or more participants received the intervention.
Studies were excluded if they were reviews, letters or conference abstracts; if participants were diagnosed with neurological conditions that were not cerebral palsy; if cycling comprised less than 50% of the total intervention; or if the article was not published in English.
Studies that met full inclusion criteria were assigned a level of evidence score, 14 and the methodological quality was appraised by two reviewers using the Downs and Black scale. 15 The Downs and Black scale was chosen because it is valid and reliable and designed to evaluate both RCT and non-RCT designs. The maximum possible score was 32 points, and the following cut points were used: ⩾75% (⩾24 points, high quality), 50%–74% (16–23 points, moderate quality) and <50% (⩽15 points, low quality).15,16
Data extraction was completed by E.L.A. and verified by S.S. Data on the research design and participant characteristics were extracted as well as characteristics of the intervention and comparison conditions, such as the frequency, intensity, duration, mode, setting and length of follow-up. The outcome measures reported in each study were then mapped to the ICF domains of body structures, body functions, activities and participation. The third reviewer (M.J.K.) was consulted if there was disagreement over the classification of an outcome measure.
For outcomes relating to body functions and activities, pre- and post-treatment means and standard deviations (SDs) were extracted. Where means and SDs were missing or reported in an alternate format (e.g. 95% confidence interval), study authors were contacted via email. If the raw data could not be obtained, the SD was estimated using the measure of variance reported (e.g. standard error or 95% confidence interval). 17
Treatment effects for continuous outcomes were determined using post-intervention mean differences and SDs. Clinical heterogeneity was assessed by comparing the participant and intervention characteristics and outcome measures reported in each study, and statistical heterogeneity was determined using the I2 statistic and chi-square test (Q-test) at P < 0.1. A cut-point of >50% represented considerable heterogeneity.
Where studies were considered similar enough to pool data, a random-effects meta-analysis was conducted (RevMan V5.3). If a study assessed a construct using multiple outcome measures (e.g. gross motor function assessed using two different scales), the authors chose the outcome measure that was most relevant and/or most similar to the outcome measures used in other studies. In adherence with best practice recommendations for systematic reviews, the results from non-randomized trials were not considered for meta-analysis. 13
Results
A total of 533 articles were identified through database searches and screened by title and abstract. The number of articles included and reasons for exclusion are provided in Figure 1. Of which, 11 articles from 9 research studies met the full inclusion criteria, including 5 RCTs (7 articles),18–24 a quasi-RCT, 25 a comparison trial, 26 a pre–post study with a control group 27 and a single-group study with a control period. 28 Agreeance between reviewers was 96% for screening by title and abstract and 100% for full-text review.
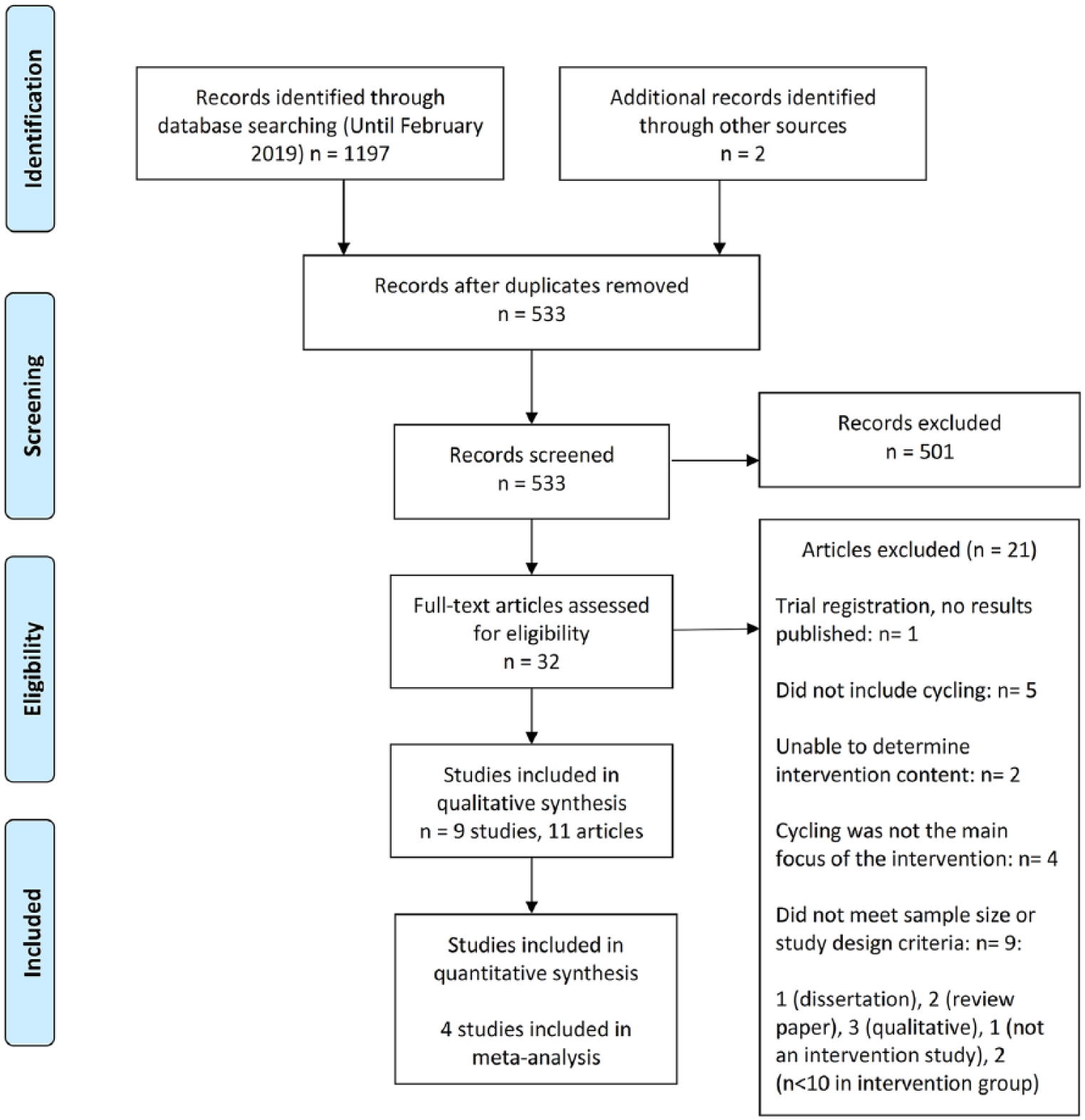
PRISMA flow diagram.
Details of the study designs and participant characteristics are provided in Table 1. Participants included 282 children with cerebral palsy with a mean age of 10.4 years (SD = 2.3) and an even distribution of males and females (53% females).
Population characteristics and experimental design of included studies.
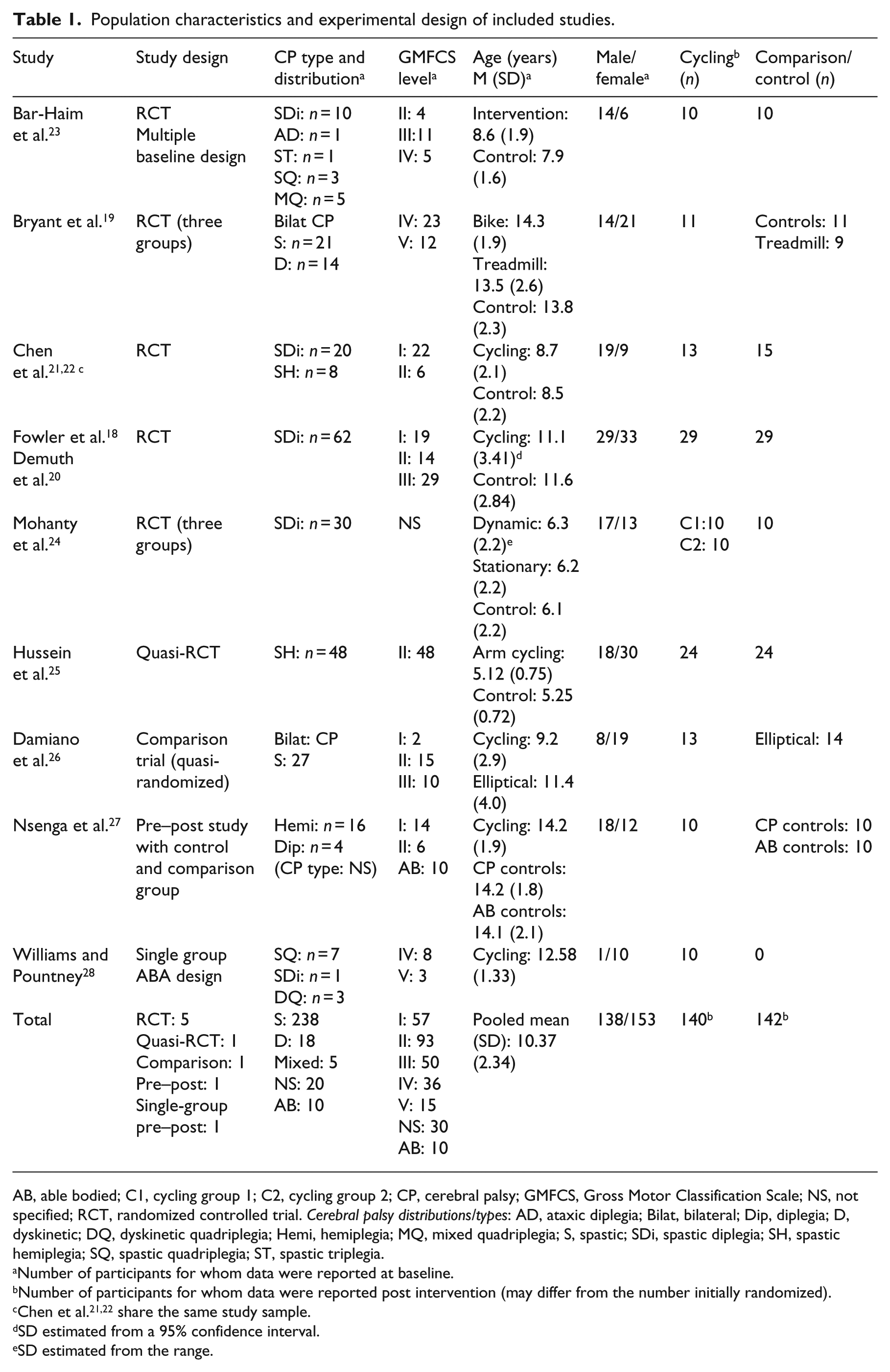
AB, able bodied; C1, cycling group 1; C2, cycling group 2; CP, cerebral palsy; GMFCS, Gross Motor Classification Scale; NS, not specified; RCT, randomized controlled trial. Cerebral palsy distributions/types: AD, ataxic diplegia; Bilat, bilateral; Dip, diplegia; D, dyskinetic; DQ, dyskinetic quadriplegia; Hemi, hemiplegia; MQ, mixed quadriplegia; S, spastic; SDi, spastic diplegia; SH, spastic hemiplegia; SQ, spastic quadriplegia; ST, spastic triplegia.
Number of participants for whom data were reported at baseline.
Number of participants for whom data were reported post intervention (may differ from the number initially randomized).
SD estimated from a 95% confidence interval.
SD estimated from the range.
Downs and Black scores are presented in Supplemental Table S1. Study quality ranged from low (14 of 32) 24 to moderate (⩾16–23)22,23,25–27 to high (⩾24)18,19 according to Downs and Black scores. Participants could not be blinded due to the nature of cycling interventions; however, only three RCTs ensured adequate blinding of the assessors.18,19,23 Randomization was violated in one study as some participants were too small to use an elliptical device and were subsequently re-allocated to the cycling group. 26 Greater than 70% adherence to the intervention was reported in five studies,18,19,22,26,28 while the remaining four did not report compliance. Adequate adjustment for confounding variables was unclear due to poor reporting or because final analyses were based on analysis of treatment rather than intention to treat. Just three studies achieved greater than 70% power to detect statistical significance on the primary outcome measures.19,24,27
The intervention, control and comparison group content for each study are summarized in Supplemental Table S2. Cycling interventions utilized semi-recumbent bikes with lower limb loading functions,18,20 upright exercise bikes 27 with postural supports,19,28 virtual reality cycling system21,22 and motorized stationary bike. 26 One RCT compared two modes of cycling (dynamic and stationary) to a control condition; 24 another included upper limb stationary cycling 25 and one investigated simultaneous upper- and lower limb passive cycling. 23 Three articles on adapted dynamic cycling were identified; however, only qualitative data were reported.6,9
As an adjunct to cycling, some interventions incorporated gross motor activities, 23 sit-to-stand exercises,21,22 conventional exercises 24 and gait training. 25 Study aims included increasing gross motor function,18,19,23,28 improving aerobic capacity, 27 muscle strength and bone mineral density,21,22 cardiovascular endurance, mobility and balance, 24 gait function 26 and arm swing during gait. 25
Interventions were delivered in participant’s schools,19,27,28 homes,21,22,26 community-based clinics, 18 a rehabilitation training and research institute 24 and an unspecified setting. 23 Interventions were led by physiotherapists18,19,23,27,28 or supervised by a parent or guardian.21,22,26 The mode of delivery was not specified in two studies.24,25 The duration of intervention programmes ranged from 4 weeks to 6 months, frequency ranged from 3 to 5 days per week and session duration ranged from 20 to 90 minutes. The overall dose of cycling ranged from 3 to 20 hours.
Comparison conditions included usual physiotherapy sessions, 19 general physical activity, 18 structured intensive training, 23 conventional exercises, 24 gait training 25 and a specified level of physical activity.21,22 One study included a second intervention arm of treadmill training 19 and another had two control groups, including one group of children with cerebral palsy and another group of typically developed children. 27 The frequency, duration and type of physical activity were described for able-bodied participants, but not for the cerebral palsy control participants. 27 Two studies did not include control groups.26,28
Except for bone mineral density, which was classified under the heading ‘body structures’, all extracted outcomes assessed body functions or activities. Participation-based outcomes were not reported in any study. Six studies (seven articles) assessed body functions using measures of muscle strength, cardiovascular fitness, selective motor control and balance.18,21–24,26,27 Activity measures were reported in 8 studies (10 articles) and included measures of gross motor function, mobility, activity capacity and functional ability.18–28
Quantitative results for body function measures are presented in Supplemental Table S3. Isokinetic dynamometry was the preferred method to assess lower limb muscle strength bilaterally 18 and on the impaired side.18,21,22,26 One moderate quality study (in two articles) reported significant improvements in knee flexor strength when tested at 90 and 120 degrees per second,21,22 although another moderate-quality study 26 and one high-quality study 18 did not report any significant improvements in muscle strength (Supplemental Table S3a). Consequently, there is weak evidence to support using stationary cycling to improve knee flexor strength of the impaired limb.21,22 A meta-analysis was not performed for muscle strength due to high variability in testing methods and angular velocities.
One moderate-quality, pre–post study reported significantly improved peak heart rate (HR), oxygen intake, respiratory minute volume and power after eight weeks of aerobic cycling training (Supplemental Table S3b). 27 Significant reductions in resting HR were also reported in a low-quality RCT after six weeks of dynamic cycling and conventional exercises, but not stationary cycling. 24 The third study, a moderate-quality RCT, reported no significant cardiovascular improvements; however, participants cycled against no resistance and the training parameters were poorly described. 23 These results demonstrate weak evidence in support of stationary and dynamic cycling interventions to improve cardiorespiratory outcomes in children with cerebral palsy.
Just one low-quality RCT assessed balance as an outcome and reported significantly improved Paediatric Balance Scale scores following both dynamic and stationary cycling interventions (Supplemental Table S3c). 24 In the absence of more rigorous trials, there is limited evidence to support using cycling as a tool to improve balance in this population.
The quantitative results for activity-based outcomes are presented in Table 2. Gross motor function assessed using the Gross Motor Function Measure (GMFM) was most frequently reported (Table 2), and sufficient data were available for meta-analysis (Figure 2). One study reported a combined GMFM section D (standing) and E (walking, running and jumping) score 18 and another reported scores separately. 24 In this case, a combined section D and E score was calculated in order to pool data for meta-analysis. 24 Insufficient data were available to perform subgroup analyses by age or level of gross motor function.
Outcomes relating to activity limitations in the included studies.
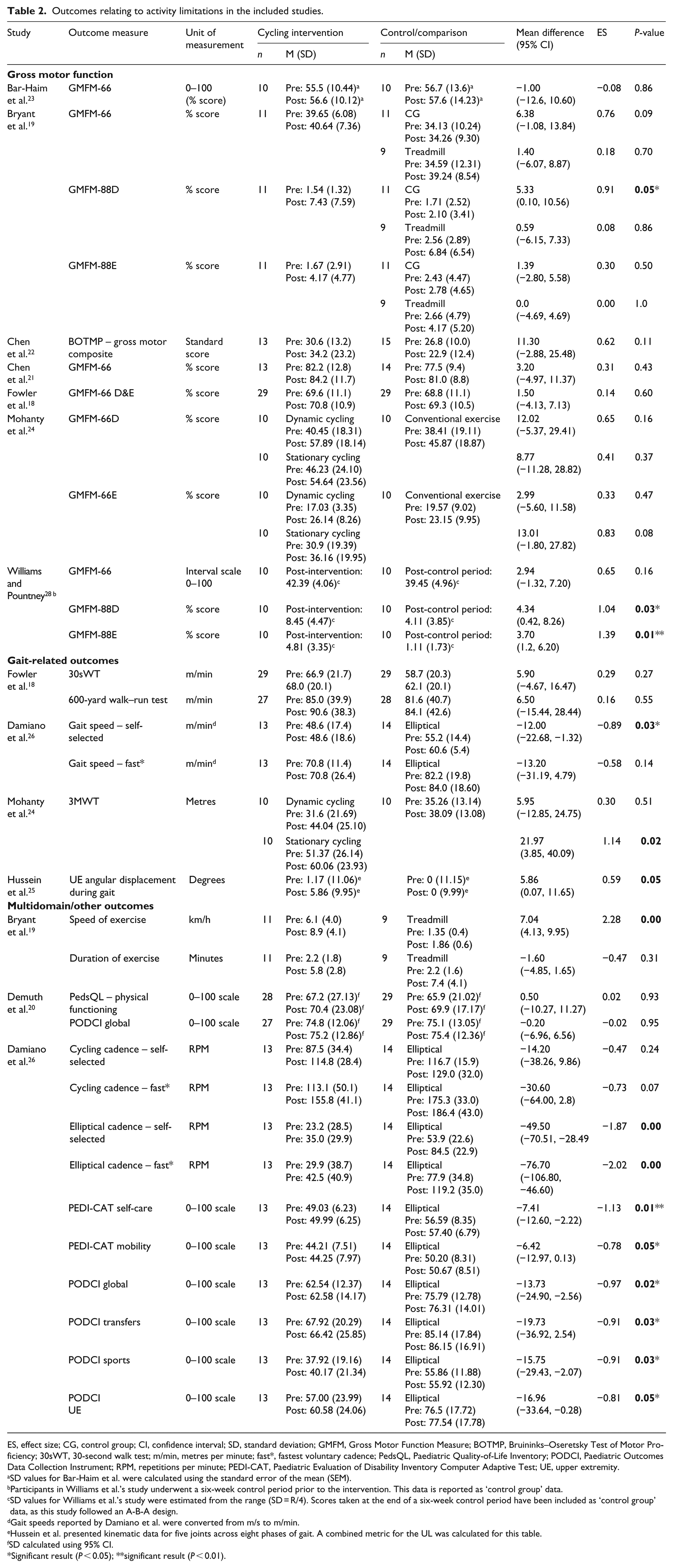
ES, effect size; CG, control group; CI, confidence interval; SD, standard deviation; GMFM, Gross Motor Function Measure; BOTMP, Bruininks–Oseretsky Test of Motor Proficiency; 30sWT, 30-second walk test; m/min, metres per minute; fast*, fastest voluntary cadence; PedsQL, Paediatric Quality-of-Life Inventory; PODCI, Paediatric Outcomes Data Collection Instrument; RPM, repetitions per minute; PEDI-CAT, Paediatric Evaluation of Disability Inventory Computer Adaptive Test; UE, upper extremity.
SD values for Bar-Haim et al. were calculated using the standard error of the mean (SEM).
Participants in Williams et al.’s study underwent a six-week control period prior to the intervention. This data is reported as ‘control group’ data.
SD values for Williams et al.’s study were estimated from the range (SD = R/4). Scores taken at the end of a six-week control period have been included as ‘control group’ data, as this study followed an A-B-A design.
Gait speeds reported by Damiano et al. were converted from m/s to m/min.
Hussein et al. presented kinematic data for five joints across eight phases of gait. A combined metric for the UL was calculated for this table.
SD calculated using 95% CI.
Significant result (P < 0.05); **significant result (P < 0.01).
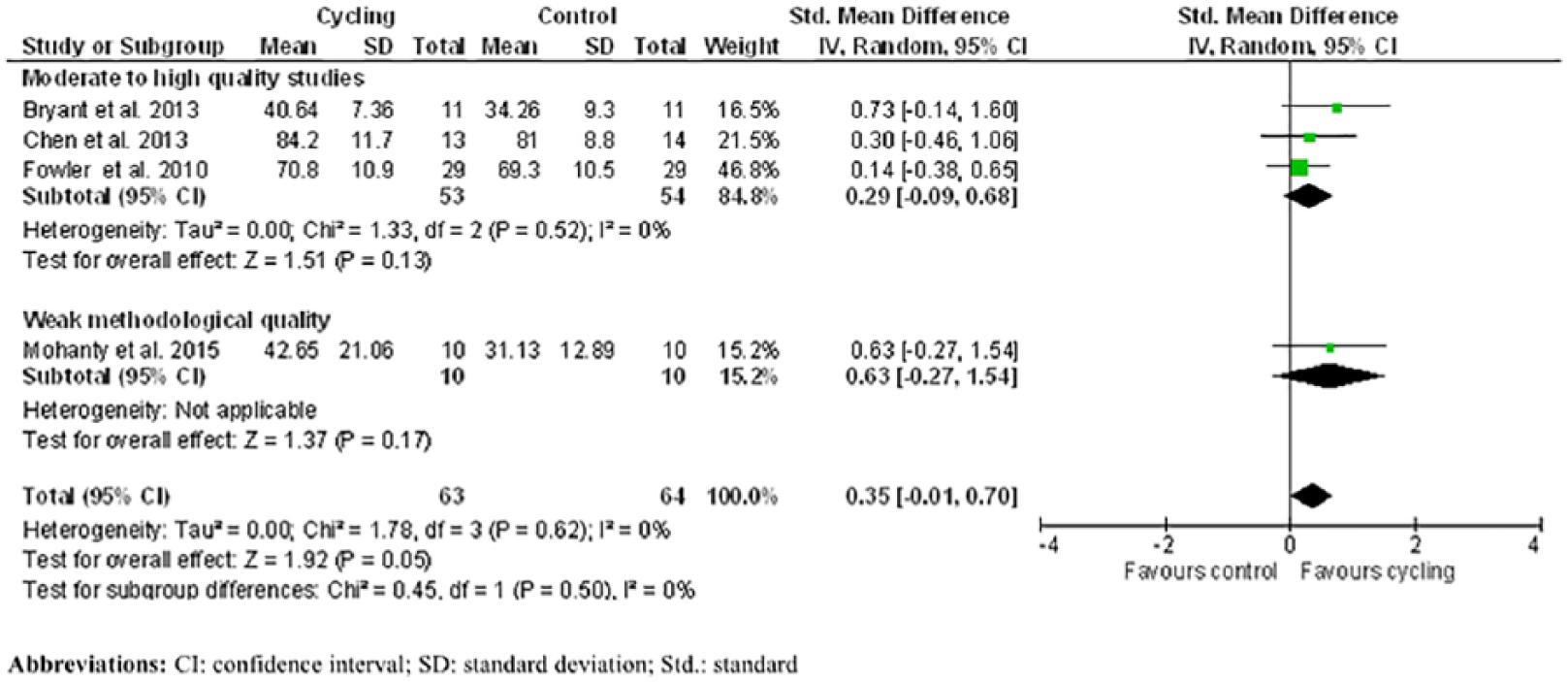
Meta-analysis.
When GMFM data from four studies19,21,23,24 on stationary cycling were pooled (n = 63 intervention; n = 64 control participants), cycling interventions were significantly more effective at improving gross motor function compared to control conditions (Figure 2). When a low-quality RCT was excluded from the analysis, the standard mean difference was no longer significant, indicating bias of the low-quality RCT. 24 These findings present inconclusive evidence that cycling improves gross motor function in children with cerebral palsy; however, it should be noted that all of the interventions were stationary cycling, and no conclusions can be drawn on the effects of other modes of cycling (e.g. adapted cycling) in this population.
The Paediatric Endurance and Limb Strengthening (PEDALS) study was the largest RCT (n = 58), contributing 45% of the total participants in the meta-analysis. 18 The PEDALS study only included ambulant children with cerebral palsy and a ceiling effect was reported on the GMFM. 18 In contrast, the two studies including non-ambulant children reported large improvements in the standing domain, 19 and the walking, running, jumping domain,19,28 of the GMFM. The GMFM assesses skills that are expected of a typically developed five-year old 29 and may be less sensitive to changes in children who function above this level. 30
Mobility and gait-related outcomes included the 30-second walk test, 18 600-yard walk–run test, 18 self-selected and fastest gait speed, 26 a 3-minute walk test 24 and angular displacement of arm swing during gait (Table 2). 25 The 3-minute walk test times were significantly improved after stationary cycling, but not dynamic cycling in one study 24 and another reported improvements in upper extremity angular displacement following a combined intervention of upper limb cycling and gait training. 25 Self-selected gait speed improved significantly for participants in an elliptical training group, but not for participants who trained on a cycle ergometer. 26 Based on these limited findings, there is insufficient evidence to conclude that cycling improves mobility and gait in children with cerebral palsy.
One study comparing elliptical training with stationary cycling reported significant improvements in favour of the elliptical group for self-selected elliptical cadence, Paediatric Outcomes Data Collection Instrument (PODCI) scores and the Paediatric Evaluation of Disability Inventory Computer Adaptive Test (PEDI-CAT) scores. 26 These results should be interpreted with caution, as participants who were too short to use the elliptical device were swapped to the cycling group, which violated randomization and resulted in lower baseline scores in the cycling group. 26
Follow-up data were collected and reported in just three studies.19,26,28 One RCT reassessed outcomes at 6 and 12 weeks post intervention, noting a significant reduction in GMFM-D (standing) scores for the cycling group, but not the control group, indicating a detraining effect. 19 The single-group study reported data at six weeks post intervention, with no significant detraining observed. 28 One study included a 12-week no-training period, although the order of the training versus no-training period depended on the availability of equipment. 26
Adverse events (or lack of adverse events) were reported in five studies (six articles).18,19,21,22,26,28 A total of 28 mild adverse events were reported in a single study, which included 6 falls, 17 complaints of mild pain, 4 reports of fatigue and 1 report of skin rash from a HR sensor. 18 Four studies (five articles) indicated no adverse events19,21,22,26,28 and four failed to report adverse events altogether.23–25,27
Discussion
The objective of this systematic review was to determine the efficacy of cycling interventions to improve functional performance in children with cerebral palsy and to determine factors that lead to superior outcomes. To facilitate literature comparisons, we categorized functional performance according to the ICF domains of body functions and reduced activity. Overall, the results for the body function domain indicated weak evidence for improved knee flexion (but not extension) strength, aerobic capacity and balance as assessed by the Paediatric Balance Scale. Results for the activity limitation domain indicated strong evidence, supported by meta-analysis, for improved gross motor function following stationary cycling interventions; however, the effect was insignificant when a low-quality study was removed from the meta-analysis.
Due to the heterogeneity of the reported cycling interventions, a thorough evaluation of study quality and functional performance outcomes was required to identify specific components of cycling interventions that led to superior outcomes in children with cerebral palsy. Indeed, of the moderate- to high-quality studies in this review, only two met all18,27 and four met most19,22,26,28 of the recommended training guidelines for people with cerebral palsy. 31 Of the two interventions that met the guidelines for cardiorespiratory training, one was associated with improved aerobic capacity. 27 This study demonstrated that children with mild cerebral palsy are capable of achieving levels of fitness that are comparable to able-bodied peers, after 8 weeks of stationary cycling for 30 minutes, 3 days per week at a starting intensity of 50% VO2 max. 27 In contrast, the PEDALS study did not report significant improvements in the 600-yard walk–run test, used as an estimate of cardiorespiratory fitness. 18 An obvious explanation for the lack of improvement in the PEDALS study was that participants struggled to achieve the target training intensity of >70% HR max, reflected by an average training intensity of 52.2% of HR max. Consequently, the actual training intensity was likely insufficient to result in cardiorespiratory improvements. To assist children with cerebral palsy to achieve and maintain higher intensities of exercise while cycling, future studies might consider employing adaptations such as motorized support or functional electrical stimulation.32,33
Despite not meeting the recommended training guidelines for cardiovascular fitness, one study reported significantly improved resting HR following outdoor dynamic cycling, but not stationary cycling. 24 The stationary cycling group cycled in an indoor clinical environment with no resistance, and the dynamic group cycled outdoors on paths around a research campus. In adults, outdoor cycling promotes greater task endurance because the environment facilitates thoughts that are unrelated to the exercise task. 34 Dynamic cycling may also be more physiologically taxing than stationary cycling, as it has been linked to increased hip and knee flexor muscle activity, 35 increased lower limb power and training HRs while cycling at the same level of perceived exertion. 36 It is possible, therefore, that the outdoor cycling group trained at a higher intensity than the stationary group due to the increased physiological demands of outdoor cycling and potentially, a more stimulating exercise environment. Future studies should consider monitoring exercise intensity throughout training sessions to help inform the best choice of cycling mode for improved cardiovascular fitness.
Interventions associated with improved muscle strength or balance included exercise programmes that aligned with the intervention goals, which is common in therapy interventions for children with cerebral palsy (e.g. increased strength or balance).21,22,24 A combined cycling and sit-to-stand intervention that was based on the principles of progressive resistance training led to increased hamstring strength.21,22 The programme involved home-based, virtual reality cycling training that was performed for 40 minutes, 3 times per week for 12 weeks. Similarly, the cycling intervention that led to improved balance outcomes incorporated an exercise programme that challenged components of static and dynamic balance. 24 The intended total exercise dose in this study (30 hours) was relatively high and was delivered over a relatively short period of time (6 weeks). The intensity of the cycling training was poorly defined and the actual dose completed was not reported. 24
Two interventions that reported no improvement in muscle strength involved cycling only.18,26 The cycling focussed PEDALS study, attempted to incorporate a resistance training component using elasticized bands attached to a stationary bike. 18 A ceiling effect occurred for some participants who reached the maximum load capacity of the resistance bands before the end of the intervention. It is possible that the actual training load was therefore insufficient to cause an increase in strength in those participants, as training loads need to be progressive to satisfy the overload principle of exercise training. 37 Both studies reported improved pedalling ability and cycling endurance after the intervention, which is consistent with other studies that did not directly measure isokinetic muscle strength.6,19
Studies associated with improved gross motor function were identical school-based interventions using a stationary bike.19,28 Both met the current recommendations for time, frequency and intensity; however, the programme duration was limited to six weeks. 28 Clinically meaningful improvements in gross motor function scores were reported in both studies despite the short training period, and one study reported significant between-group differences for the standing domain of the gross motor assessment post training. 19 Improvements in gross motor function observed during the training periods were maintained at 6-week follow-up in one study 28 but not at 6 or 12 weeks in another. 19 The follow-up period of just six weeks in the single-group study may have been insufficient to detect a significant detraining effect in the convenience sample of 10 participants.
The two studies that reported improved gross motor function included non-ambulant children with cerebral palsy.19,28 Children with more severe physical impairments have a greater capacity for improvement in gross motor function, particularly in the standing tasks that they do not frequently practice. 38 The lack of significant improvements in studies of ambulant children may be due to ceiling effects on the GMFM or insufficient training doses and lack of appropriate exercise progression. An alternative explanation is that the interventions lacked specificity to the gross motor tasks assessed. Careful consideration should be taken to ensure that outcome measures are sensitive enough to detect changes in the population of interest and to ensure that training programmes adhere to basic principles of exercise prescription.
Anecdotal reports of improved cycling performance (e.g. ability to pedal independently) were made in some articles following cycling interventions, although formal assessments of cycling capacity were completed in just three studies.19,26,28 Cycling speed and duration were assessed in one RCT, 19 and a single-group study reported cycling resistance, speed and duration for each participant. 28 The results from the pre–post study were presented in a graph and could not be extracted for this review, although significant improvements were reported in-text for all participants. 28 It seems reasonable that cycling training leads to improved cycling capacity; however, future efforts should be made to assess cycling-specific outcomes and to determine optimal training parameters for improved cycling capacity and performance.
Overall, cycling is a safe and efficacious activity that can be undertaken by children with cerebral palsy when supervised. Although 28 intervention-related adverse events were reported, the severity was considered mild and most were reports of muscle soreness and fatigue which can be reasonably expected during a physical activity intervention. 18 To reduce the incidence of muscle soreness in future interventions, clinicians should take care to tailor sessions to the child’s level of ability and ensure that adequate rest and recovery time is provided between sessions. 31 Six observed falls were also reported; however, the authors categorized these as mild events and did not specify when or how the falls took place (e.g. during bike transfers or while cycling). 18 Indeed, there are risks associated with cycling interventions; however, they appear to be minimal and are likely outweighed by benefits such as an improved sense of enjoyment, achievement and well-being.9,10 It should be noted that the majority of interventions included some variant of supervised stationary cycling, and less is known about the safety of dynamic cycling in this group.
A number of considerations should be taken into account in interpreting the findings of this review. (1) Only a limited number of RCTs have been conducted on cycling interventions in children with cerebral palsy and therefore this review included pre–post studies (with N ⩾ 10) to provide a more detailed examination of the available evidence. The inclusion of non-randomized trials may introduce bias, and caution should be exercised when interpreting results from such studies. We recommend that well-designed RCTs are developed to address the research questions and to provide stronger evidence for the efficacy of cycling to improve function in children with cerebral palsy, particularly those who are non-ambulant or rely on walking aids to mobilize. (2) The heterogeneity in the quality of the reported cycling interventions provides a challenge determining the components of cycling interventions (such as frequency, intensity, duration, type and setting) that contributed to improved function. Greater consistency is needed in terms of intervention and control content and care should be taken to select outcome measures that are sensitive to change in the population of interest. Improved reporting of usual care and control conditions will assist future reviewers to more accurately pool data for meta-analysis. (3) Finally, this review was limited to studies that were published in the English language and available through six online databases.
Our comprehensive review has identified important gaps in the existing literature that will help inform future research on the efficacy of adapted cycling in children with cerebral palsy. Given the extensive range of cycling interventions that are prescribed to people with neurological impairments, future research on this topic is crucial for informed clinical practice.39–44 We found preliminary evidence for cycling interventions to improve components of gross motor function in non-ambulant children with cerebral palsy, and limited evidence for improved muscle strength, balance and cardiorespiratory fitness. The meta-analysis of gross motor function results demonstrated that cycling may improve gross motor function more than standard care or control conditions; however, the risk of bias in one of the included studies means that results must be interpreted with caution. No consensus was reached on the optimal parameters for improved function, although children with more severe cerebral palsy may require additional support to achieve therapeutic exercise intensities. No conclusions could be drawn on the retention of effects beyond the immediate intervention as few studies included follow-up testing.
Clinical messages
Cycling interventions have led to improved gross motor function, cardiovascular fitness, hamstring strength and balance in children with cerebral palsy.
Cycling studies have predominantly focused on stationary cycling in ambulant children with cerebral palsy.
High-quality research is required to establish optimal training parameters for cycling programmes for children with cerebral palsy.
Supplemental Material
Supplemental_Material – Supplemental material for Efficacy of cycling interventions to improve function in children and adolescents with cerebral palsy: a systematic review and meta-analysis
Supplemental material, Supplemental_Material for Efficacy of cycling interventions to improve function in children and adolescents with cerebral palsy: a systematic review and meta-analysis by Ellen L Armstrong, Sian Spencer, Megan J Kentish, Sean A Horan, Christopher P Carty and Roslyn N Boyd in Clinical Rehabilitation
Footnotes
Acknowledgements
All authors were actively involved in developing the selection, quality assessment and data extraction criteria. E.L.A. and S.S. completed the article selection and review process, and M.J.K. was the third reviewer. R.N.B., C.P.C., S.H. and M.J.K. were guarantors and assisted in manuscript preparation and publication. All authors read, reviewed and approved the final manuscript prior to submission. This study was completed in part fulfilment of E.L.A.’s doctoral thesis, under a Griffith University Higher Degree Research Scholarship (GUHDRS).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: R.N.B. is supported by an NHMRC research fellowship (1105038) and C.P.C. is supported by an Advance Queensland Mid-Career Research Fellowship (00459/2017).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.