
Abstract
Objective:
To evaluate whether an 18-month, physical activity coaching program is more effective than standard care in terms of upper-limb activity.
Design:
A prospective, randomized controlled trial.
Setting:
Three municipalities in Norway.
Population:
A total of 380 persons with stroke.
Intervention:
The intervention group received follow-up visits and coaching on physical activity and exercise each month for 18 months after inclusion, by a physiotherapist. The control group received standard care.
Main measures:
The primary outcome, in this secondary analysis, was Motor Assessment Scale items 6, 7, and 8. Secondary outcomes were National Institute of Health Stroke Scale item 5, the Stroke Impact Scale domain 7, and the Modified Ashworth Scale in flexion/extension of the elbow.
Results:
In total, 380 persons with stroke were recruited, with mean (SD) age 72 (11) years, and baseline scores total National Institute of Health Stroke Scale was 1.4 (2.2)/1.6 (2.4) and Motor Assessment Scale items 6, 7 and 8 in the intervention/control group was 5.5 (1.2)/5.5 (1.2), 5.4 (1.4)/5.4 (1.3), and 3.6 (2)/3.5 (2), respectively. There was no significant difference between groups in terms of upper limb function in any of the Motor Assessment Scale items. In this population with minor stroke, upper-limb activity was good at three months post-stroke (74% of the maximum) and remained good 18 months later (77% of maximum).
Conclusion:
After intervention, there was no difference between the groups in terms of upper-limb activity.
Introduction
Limitations in upper-limb activity are present in 48% of patients 72 hours after stroke and are associated with older age, longer stay in acute care, and higher early mortality. 1 After the first three months, 50% will have remaining limitations.2,3 The consequences, for those affected, are serious, considering that upper-limb activity is important for independent living and closely related to quality of life. Limitations in upper-limb activity may also lead to increased dependence and restrictions in social participation. 4 Strategies to compensate for the loss of upper-limb activity are energy consuming and may lead to fatigue. 5 Upper-limb activity is one of the major issues post-stroke for people with stroke, their family, and health professionals in interdisciplinary rehabilitation. However, currently there is no evidence to support any intervention for improving upper limb function in a general population of stroke. 6
A recently reported trial of physical activity, the Life After Stroke study (LAST), was to investigate whether an 18-month, home-based physical activity and exercise coaching program was effective in maintaining body function and structures as well as activity. 7 The primary outcomes in the main paper were reported from the total score of the Motor Assessment Scale. The intervention was proven to be feasible, as the intervention group revealed higher levels of physical activity than the control group. However, the results showed no differences between the groups regarding motor function, activities of daily living, walking ability, balance, or self-perceived health. 8 It may be of interest to know to what extent specific upper limb function was affected by the general physical activity and exercise program.
Therefore, the research question for this sub-study was, Is an 18-month, home-based coaching program on physical activity and exercise additional to standard care more effective than standard care in terms of upper limb activity, as measured with the three items for arm and hand with Motor Assessment Scale?
Method
This study was an analysis of a secondary outcome from the LAST study, a pragmatic, single-blinded, parallel-group, randomized trial, performed in accordance with Consolidated Standards of Reporting Trials (CONSORT). 9 The main results of this trial have been reported elsewhere. 8 The trial was registered at ClinicalTrial.gov: NCT01467206. Ethical approval for the trial was granted by Regional Committee for Medical and Health Ethics Central (REC no 2011/1428). Recruitment started in October 2011 and ended in June 2014.
Participants were consecutively recruited three months after stroke at two centers in Norway: Trondheim University Hospital and Bærum Hospital.
Patients were eligible if they were aged 18 years or older, had a confirmed first-ever or recurrent stroke, had been discharged from inpatient rehabilitation and were community dwelling, had a modified Rankin Scale (mRS) score <5, 10 had no other co-morbidities that made them unable to perform the intervention, and were capable of providing consent. They were excluded if they had cognitive deficits (Mini Mental State Examination score <21 points or <17 points for patients with aphasia), 11 contraindication to participation in motor training, or inclusion in another study.
The randomization process was concealed and performed by a web-based system administered by Unit of Applied Clinical Research, Faculty of Medicine and Health Science, Norwegian University of Science and Technology.
Participants randomized to the control group received standard care only. Standard care typically consisted of physiotherapy intervention at moderate intensity 45 minutes once per week for three to six months performed in the home or at an outpatient clinic, 8 as recommended by the guidelines. It was aimed at improving activities of daily living and was directed at both the lower and upper limb.
The intervention group received individual coaching on physical activity and exercise by a community-based physiotherapist as an adjunct to standard care for 18 months. In order to achieve their personal goals, the participant chose type of vigorous exercises, in addition to type of physical activities. Exercise was outlined to be for 45–60 minutes once per week, with an intensity between 15 and 17 on Borg Scale of perceived exertion. 12 The exercises could be performed in a training centre, in an outpatient clinic or at home, individually or in a group. The physical activities were performed for 30 minutes for seven days a week by choice of the individuals. 13 For example, to achieve a goal of independent walking, a participant could perform vigorous strengthening and endurance exercises and walks to the post box and in the close neighbourhood as physical activities.
The coaching took place once every month over 18 months, when the physiotherapist visited each participant. In these monthly meetings, elements of motivational interview was used to define, and up-date, one to three goals for the individuals using the Goal Attainment Scale, 14 to give advice for progression of exercises and to collect training diaries, monitoring adherence to the exercises and physical activity.
The outcome, which is the focus of this study, is upper-limb activity measured using the Motor Assessment Scale for stroke, 15 items 6, 7, and 8 (i.e. arm function, hand function, and advanced hand and arm function) because in combination, they represent upper-limb activity. The Motor Assessment Scale is reported on a scale from 0 to 6, where 6 is maximum performance. The Norwegian translation of the Motor Assessment Scale has shown good psychometric properties. 16 The outcomes were measured by a blinded assessor at baseline, and 18 months later.
National Institute of Health Stroke Scale, item 5a and b, was used to evaluate motor function in both upper limit at baseline, scores ranging from 0 to 4. 17
In addition Stroke Impact Scale, a self-evaluating scale with 59 items divided into 8 domains, assessed on a scale from 1 to 5, where 5 is maximum, was performed at 18 months. 18 Summative scores are generated for each domain and scores range from 0 to 100. Domain 7, concerning upper-limb activity is reported in this study.
The Modified Ashworth Scale to evaluate tone in flexion/extension of the elbow was also performed at 18 months. The Modified Ashworth Scale is a clinical measure of muscle tone with an ordinal scale to grade the resistance encountered during passive muscle stretch, graded 0, that is, no increase in tone, to 4, when the affected part is rigid in flexion or extension. 19 Modified Ashworth Scale and Stroke Impact Scale were only measured at 18 months.
Information, such as age, sex, and time from stroke, was collected and is presented descriptively.
The upper-limb activity (Motor Assessment Scale 6, 7, and 8) is presented descriptively, and the difference between the intervention and the control groups at end of follow-up was analyzed using independent sample t-tests with a significance level of p < 0.05. The mean difference (95% confidence interval (CI)) is presented. Participants were analyzed in the group to which they were assigned, and imputation of missing data and sensitivity analysis were performed as recommended by van Buuren.8,20
Results
Between 11 October 2011 and 30 June 2014, 1324 individuals were screened for inclusion. In total, 380 participants were included and randomly assigned to the intervention group (n = 186) or to the control group (n = 194). The most common reasons for exclusion were that patients declined participation or were institutionalized (24% and 22% of the 1324 individuals, respectively). In the intervention group, 33 (18%) participants were absent at follow-up; 9 died and 24 were lost to follow-up (17 withdrew, 2 had a serious illness, 4 were not available, and 1 was missing for unknown reason). In the control group, 32 (17%) were absent at follow-up; 9 died and 32 were lost to follow-up (20 withdrew, 1 had a serious illness, 1 was not available, and 1 was randomized in error). Therefore, at 18 months, 153 (82%) intervention participants were measured compared to 162 (83%) control participants.
Demographic and baseline characteristics were similar in both groups (Table 1). The participants were on average only mildly disabled, independent in activities of daily living and able to walk on average 390 m in 6 minutes, which is about 80% as far as their healthy peers (Table 1).
Baseline characteristics of participants, therapists, and centers.
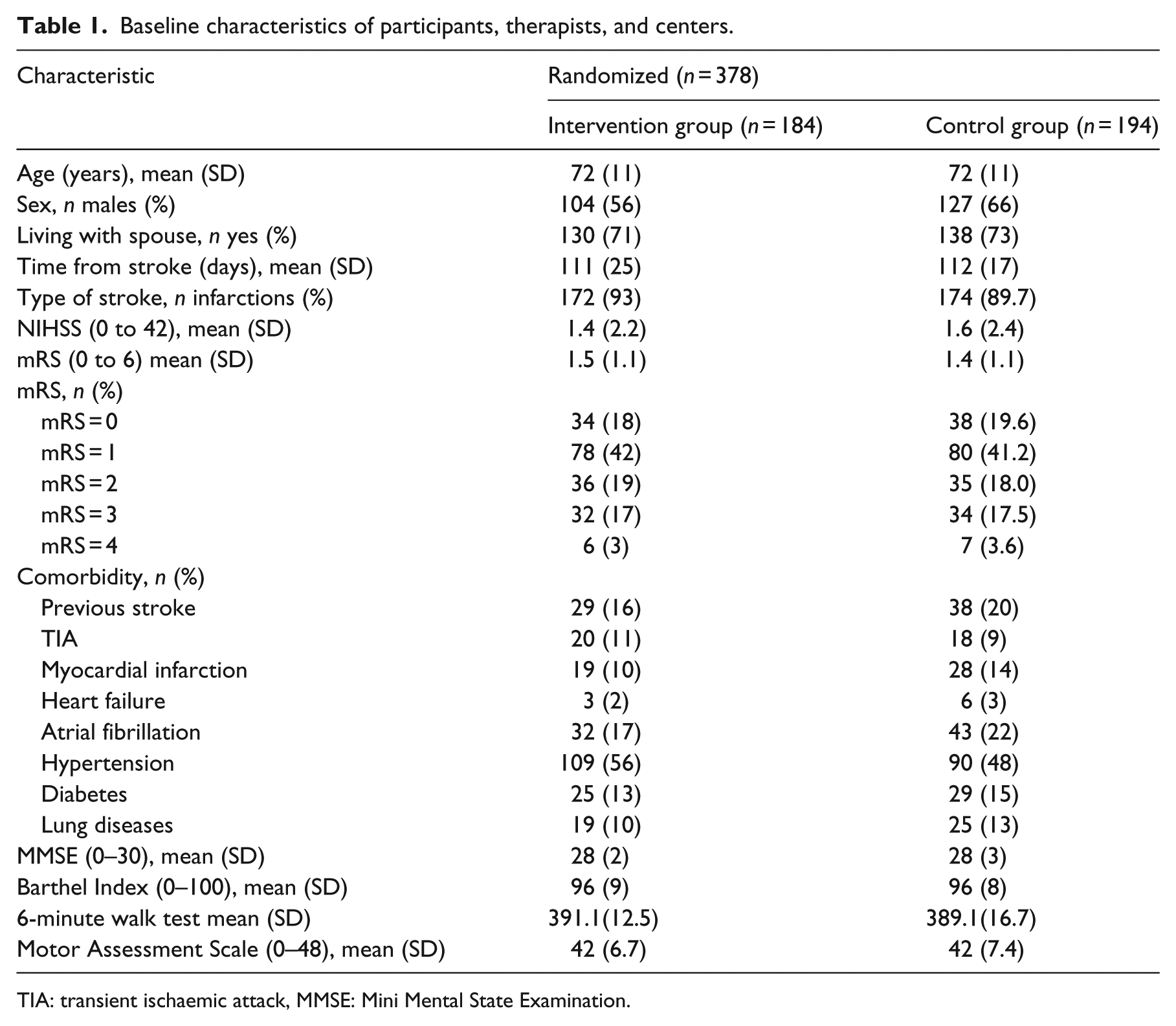
TIA: transient ischaemic attack, MMSE: Mini Mental State Examination.
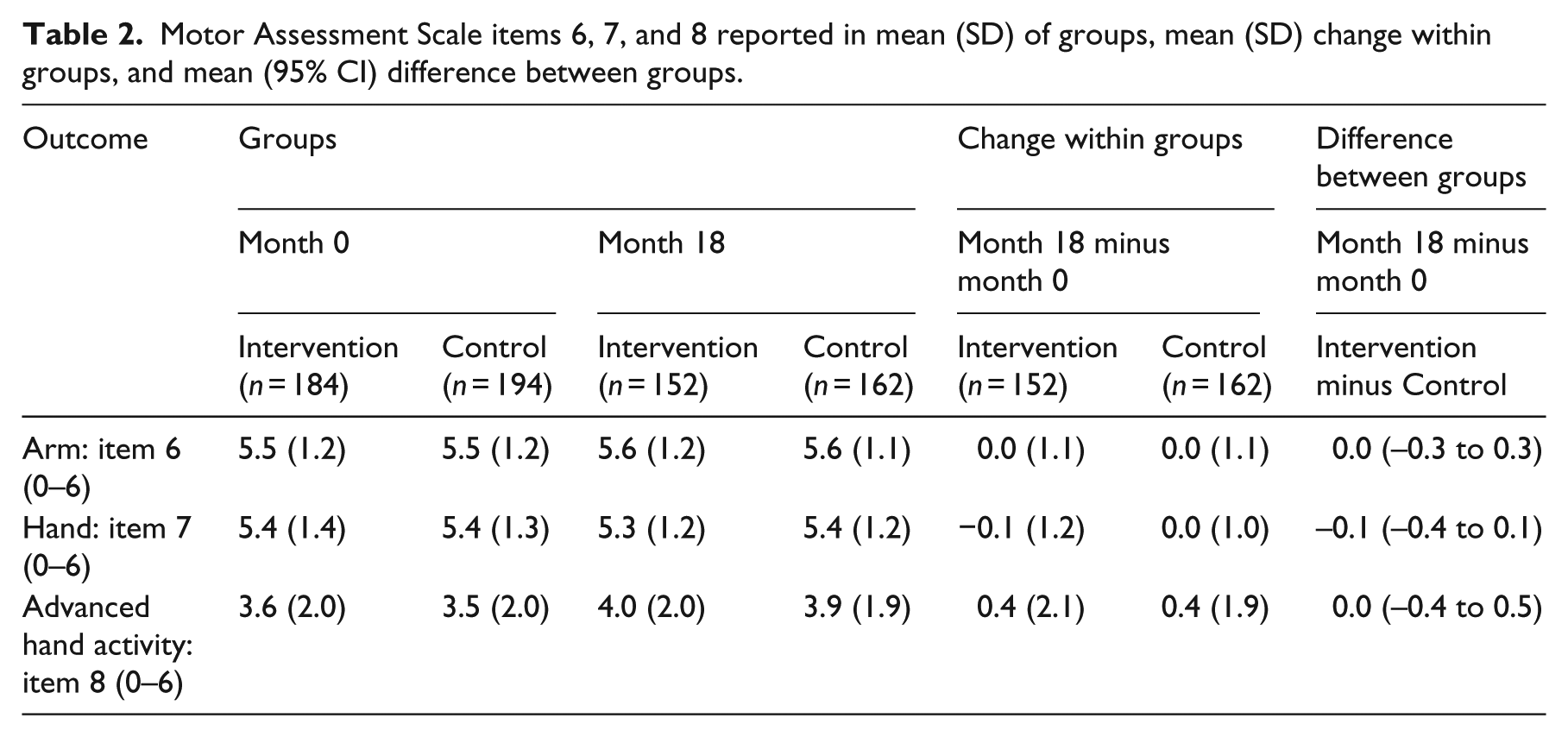
There were no significant differences between groups in terms of upper-limb activity (Table 2). Since there was no difference between groups, participants were combined into one group. Higher tonus, with a score 1 on Modified Ashworth Scale in the arm (biceps and triceps), was found in 59 (18.7%) of 315 participants. Of these, 40 (12.7%) had a score of 1, (slight increase in tonus) 14 (4.4%) had a score of 2 (marked increase), 3 (0.9%) had a score of 3 (considerable increase), and 2 (0.6%) had a score of 4 (affected parts in rigid flexion or extention). Scores of Stroke Impact Scale domain 7 was 83 in the total sample.
Motor Assessment Scale items 6, 7, and 8 reported in mean (SD) of groups, mean (SD) change within groups, and mean (95% CI) difference between groups.
Discussion
After intervention, there was no difference between the intervention and control group in terms of upper-limb activity.
An explanation for the lack of difference between the groups may be that the participants already had good function at three months, where they had regained 92% and 90% of the maximum score in upper limb (Motor Assessment Scale, item 6) and hand activity (Motor Assessment Scale, item 7), but only 58% of the maximum score in advanced hand (Motor Assessment Scale, item 8). Comparably, 69 persons (18%) had remaining impairments on the National Institute of Health Stroke Scale in this study which would indicate a population with minor stroke. A slightly higher incidence of upper limb limitations was noted in Motor Assessment Scale where 95 persons (25%) had limited activity in the arm, 109 (29%) with hand function and 248 (65%) with advanced hand and arm function.
Higher tonus and spasticity in the arm was not a big problem in this group of home dwelling people with stroke with approximately 4%–5% experiencing minor to moderate increase of tonus and only 0.01% (n = 2) spasticity in the arm.
One could argue that there was little room for improvement. However, where there was room for improvement, that is, in advanced hand and arm function where a small amount of improvement, about 7% was noted; there was still no difference between the groups. This improvement may have been as a result of standard care, but may also have been as a result of ordinary activity practiced during everyday activities. It appears as if once people with stroke are at a good level of upper-limb activity, some improvement may be expected and levels seem to be self-sustaining. On the contrary, a reason for lack of effect may be that the intervention was not task specific, that is, it did not target upper-limb activity in particular but rather targeted general physical activity.7,8
Nevertheless, the results in this study indicate a low incidence of reduced upper extremity function at three months, which is in line with other studies.1,21,22 The most important predictive factors for upper limb recovery following stroke appears to the initial severity of motor impairment or function. 23
There are both strengths and weaknesses in this study. The main strengths of the study lie in the large sample size, the long follow-up time of 18 months, and the good retention of participants at 83%. The main weakness is that the sample, being mildly disabled, is not representative of all strokes, and therefore findings may not be generalizable to severe stroke.
The implications for clinical practice from the findings of this sub-study are that, in order to improve specific activities and tasks, the exercises need to be specifically addressed to the same specific activities and tasks. The results may be viewed as an addition to the knowledge base for goal and task-oriented exercises.
In summary, in this population of people with mild disability after stroke, upper-limb activity was good at three months post-stroke (74% of the maximum) and remained good 18 months later (77% of maximum). After intervention, there was no difference between the intervention and control group in terms of upper-limb activity.
Clinical messages
Coaching on regular physical activity and exercise does not influence arm recovery in persons with mild stroke, discharged from inpatient stroke rehabilitation.
To improve specific activities and tasks, the exercises need to be specifically addressed to the same specific activities and tasks.
Footnotes
Acknowledgements
The authors are grateful for help and collaboration from Asker, Bærum, and Trondheim community and the staff at the hospitals St Olavs and Bærum. They also would like to thank the participating people suffering stroke.
Author contributions
T.A., B.I., and B.L. contributed to the conception and design of the LAST study. B.L., T.A., M.G., H.I.-H., and B.I. contributed to the acquisition and interpretation of data. B.L. and L.A. analyzed the data. B.L. drafted the work. L.A., T.A., M.G., and H.I.-H revised the work critically for important intellectual content. B.L., L.A., M.G., H.I.-H, B.I., and T.A. finally approved the version to be published and agreed to be accountable for all aspects of the work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Norwegian Research Council. This study was supported by the Research Council of Norway—Drammensveien 288, 0283 Oslo.