
Abstract
Objective:
The objective of the study is to analyse the psychometric properties of the Stroke Stigma Scale, a novel scale to assess perceived stigma of patients with stroke.
Design:
This is a psychometric study.
Setting:
Neurology or rehabilitation units in three hospitals in China.
Subjects:
A total of 288 patients with stroke.
Interventions:
None.
Measures:
The content validity of the Stroke Stigma Scale was assessed through expert consultation. Criterion validity was evaluated based on the scale’s relationships with the Stigma Scale for Chronic Illness and the Self-rating Depression Scale. Construct validity was assessed using exploratory factor analysis, and internal consistency was tested with Cronbach’s α.
Results:
The final version Stroke Stigma Scale consists of 16 items. It showed strong positive correlations with both the Stigma Scale for Chronic Illness (ρ = 0.89, P < 0.001) and the Self-rating Depression Scale (ρ = 0.82, P < 0.001). The exploratory factor analysis revealed four components of the Stroke Stigma Scale: internalized stigma, physical impairment, discrimination experience, and social isolation, which were strongly associated with our perceived stroke stigma model. Cronbach’s α for the total scale was 0.92, and that of each subscale was 0.77–0.86. The test–retest reliability with intra-class correlation coefficients of the total scale was 0.92 (P < 0.001), and intra-class correlation coefficients of each subscale were 0.74–0.89 (P < 0.001).
Conclusions:
The Stroke Stigma Scale is a reliable and valid measure of perceived stigma in patients with stroke, which may be useful in stigma prevention and stroke rehabilitation.
Introduction
Stigma is an ‘attribute that is deeply discrediting, and that reduces the bearer from a whole and usual person to a tainted, discounted, and inferior one’. 1 Perceived stigma commonly occurs when patients internalize assumed exclusionary attitudes towards them and inculcates a fear of enacted stigma due to social prejudice and discrimination. Its properties could be summarized concretely as six factors – concealability, course, disruptiveness, aesthetics, origin, and peril. 2 Stigma originates from a series of perception changes, including distinguishing between and labelling human differences, producing negative stereotypes, being separated from self or others, experiencing a loss of status, and discrimination. 3
Patients with stroke often undergo a major disruption in life course, leading to changes in their concept of self. 4 In a survey conducted with Western patients with stroke, approximately 80% of the cohort reported experiencing mild to moderate degrees of stigma, 14.5% thought they were to blame for having a stroke, and 13% felt embarrassed by their physical limitations. 5 Perceived stigma negatively affects patients’ rehabilitation process. Patients with stroke, especially those with disabilities, may consider stroke as a further significant burden to their current health status, leading to negative perceptions of physical, psychological, and social influences. 6
Quantification by measurement plays an important role in the prevention and treatment of stigma, and a number of existing measures could be used to assess stroke-related stigma. The Stigma Scale for Chronic Illness and Stigma Scale for Chronic Illness 8-item version were developed in recent years to evaluate both internalized and enacted stigma associated with all chronic illnesses.7,8 The Chronic Illness Anticipated Stigma Scale was developed in 2013 to evaluate anticipated stigma. 9 However, while these measures may be used for all chronic illnesses, their items may be too broad to reflect stigma attached to a single illness. As stroke survivors have much higher rates of hemiplegia, aphasia, dysphagia, and urinary incontinence compared to other chronic illnesses, it is necessary to explore stroke stigma in depth and to develop a measure containing items specifically related to the assessment of stroke impairments. This study aimed to develop such a scale and to examine its psychometric properties among patients with stroke, at different stages of their rehabilitation, ultimately confirming its utility in practice.
Methods
We utilized a prospective psychometric study design. All procedures and materials were approved by the ethics committee of Nanfang Hospital (No. NFEC-2018-054). The study was conducted from September 2017 to July 2018 and comprised the development, evaluation, and validation of the measure.
Part 1: development of the measure
We developed a model of perceived stigma related to stroke, based on the conceptual model of perceived HIV-related stigma developed by Berger et al. 10 It described the process of perceived stigma of patients with stroke and guided the development of items on the Stroke Stigma Scale (see Supplemental Appendix Figure 1).
Three main themes were confirmed after qualitative interviews conducted between September and October 2017, namely, perception of stigma, experience of discrimination, and possible response. Based on these themes, a 55-item pool was created. We consulted 10 patients with stroke in Nanfang Hospital on appropriate language use and potential triggers for negative emotions and, based on these consultations, developed a 32-item pool.
Next, an expert consultation was conducted using the Delphi technique. An invitation to participate in the consultation and a description of content were sent by email to identified experts, of whom 25 experts from five provinces in China agreed to participate in the consultation. They reviewed item content and evaluated each item score independently using a 9-point Likert-type scale (where 1 = not important and 9 = very important). After three rounds of consultations, eight items met the removal standard (total score <70%), and the initial 24-item scale was developed.
Part 2: evaluation and validation of the measurement
Participants
Patients who received treatment in neurology or rehabilitation units in Nanfang, Sanjiu Brain, and Baiyunshan hospitals in Guangdong were conveniently and consecutively recruited from March to July 2018. Participants were included if they met the following criteria: (1) aged ⩾18 years, (2) clinical manifestations and imaging examinations (computed tomography (CT) or magnetic resonance imaging (MRI)) were consistent with patients diagnosed with stroke, (3) the time of stroke after first confirmed diagnosis ⩾seven days, and (4) with clear consciousness and communication ability. Potential participants were excluded if (1) they had been diagnosed with another life-threatening illness, (2) showed cognitive impairment (Montreal Cognitive Assessment score <26 points), (3) withdrew during the interview, or (4) showed severe mood swings that may aggravate the illness.
Participants provided informed consent prior to participation and were asked to complete the sociodemographic and stigma items individually. If participants had difficulty writing due to physical impairment or other reasons, the research assistants would read out the questions and options one by one and recorded participants’ responses. The process lasted 10–20 minutes; research assistants would consider halting the examination if a participant showed severe mood swings. To assess test–retest reliability, 30 patients were invited to complete the same items again seven days after the first examination.
The sample size >100 in a validation study ensures stability of variance covariance matrix and is considered excellent. 11 Generally, exploratory factor analysis requires a sample of 200. 12 Therefore, we had to recruit more than 200 participants in our study.
Measures
The 24-item Stroke Stigma Scale
The test sheet of this scale contains 24 items. Participants were asked to rate their experiences of stigma over the preceding seven days, using a 5-point Likert-type scale (1 = never, 5 = always). Scores range from 24 to 120, with a higher score indicating more severe stigma.
The Stigma Scale for Chronic Illness
This scale contains 24 items, rated on a 5-point Likert-type scale (1 = never, 5 = always). Scores range from 24 to 120, and higher score indicates severer stigma. The scale has sufficient reliability and validity in patients with stroke, multiple sclerosis, Parkinson’s disease, epilepsy, and amyotrophic lateral sclerosis.8,13,14 The score obtained on this scale was used as criterion for the validity of the Stroke Stigma Scale.
The Self-rating Depression Scale
This is a widely used scale for assessing depression in general populations, including chronic illness patients with stroke.15–17 Participants complete the scale independently, rating their responses on a 4-point Likert-type scale (1 = never or little, 4 = most of the time or all the time). The scale contains 20 items, half of which are reverse-scored. Scores range from 0 to 100, with higher scores indicating more serious depression. The scale’s reliability and validity in patients with stroke are well supported.18,19 As previously reported, 20 stigma has an impact on depression, and in this study, scores on the Self-rating Depression Scale were used as criteria for the validity of the Stroke Stigma Scale.
Data analysis
All statistics analyses were conducted using the IBM SPSS 19.0 software, with an α of 0.05 for significance. General and disease-related characteristics were presented as number, mean, and standard deviation. The validity evaluation of the scale included content, criterion, and construct validity, while the reliability evaluation comprised internal consistency and test–retest reliability.
Content validity was assessed by comparing the scores given by members of the expert panel during the consultation. Items with a total score ⩾70% were designated as priorities 21 ; the remaining items were eligible to be removed.
Criterion validity was assessed by examining the relationships between the scores of the Stroke Stigma Scale and those of both the Stigma Scale for Chronic Illness and the Self-rating Depression Scale. Pearson’s correlation coefficients (ρ) were calculated; if P < 0.05, ρ ⩾ 0.75 represented high correlation; 0.40 ⩽ ρ < 0.75 was acceptable; and ρ < 0.40 was poor. 22
Construct validity was assessed using exploratory factor analysis. To assess the data suitability for exploratory factor analysis, the Kaiser–Meyer–Olkin index and Bartlett’s sphericity test were conducted. Principal component analysis with varimax rotation was used to detect structure and the components were selected if eigenvalues >1. 23 Items were considered for removal when its loading <0.35 on one factor, or >0.35 on two or more factors.
Internal consistency and individual item consistency were assessed using Cronbach’s α and changes in α in the absence of each item. 24 If the absence of an item resulted in higher α of the total scale, this item was considered for removal. In order to shorten the scale, if the inter-item correlation coefficient >0.65 or item–scale/item–subscale correlation coefficient <0.5, these items were also considered for removal.
Test–retest reliability was examined through intra-class correlation, represented by calculating Pearson’s ρ of two assessments of the same participants. Intra-class correlation values of 0.80–1.00 were considered to show excellent test–retest reliability, 0.60–0.79 were good, 0.40–0.59 were moderate, and below 0.40 were poor. 24
Results
Psychometric evaluation of the 24-item Stroke Stigma Scale
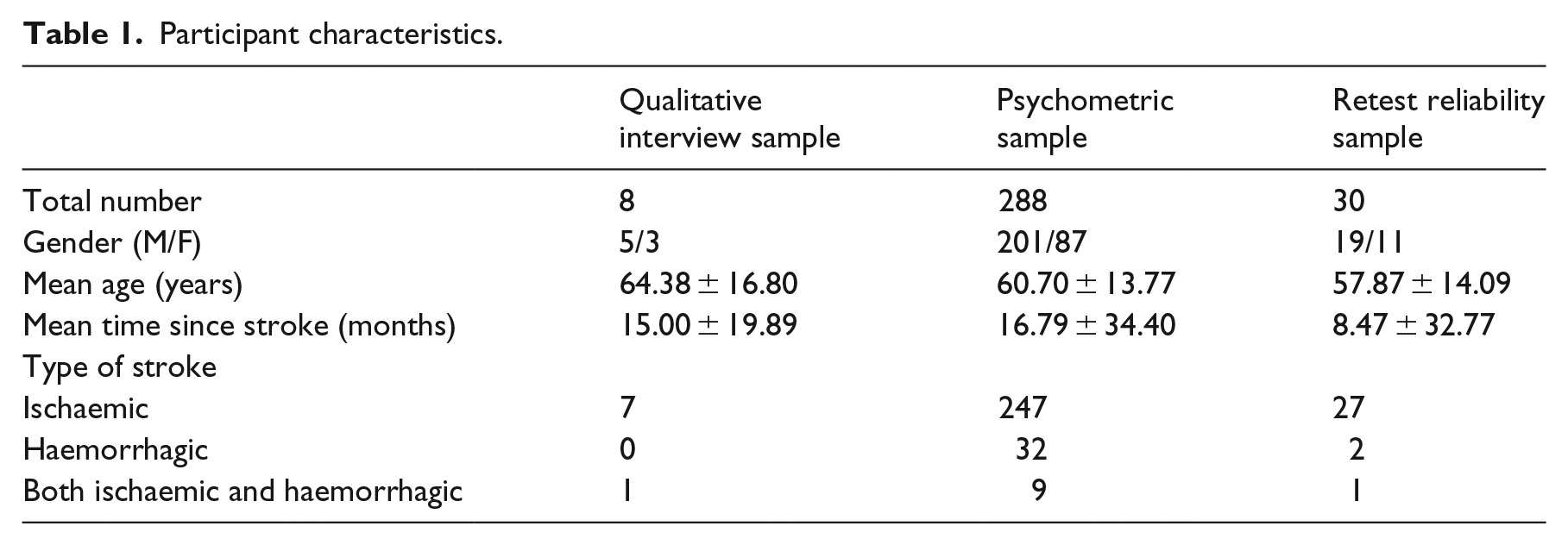
A total of 310 patients with stroke were invited to participate in our study; 15 declined to continue with the study, 3 were excluded based on severe mood swings, and 4 had incomplete assessments. A total of 288 participants (201 males and 87 females) completed all the assessments. Participants’ mean age was 60.70 ± 13.77 years, and mean time since stroke was 16.79 ± 34.40 months. Among the participants, 247 had ischaemic strokes, 32 had haemorrhagic strokes, and 9 had ischaemic and haemorrhagic strokes. General and disease-related characteristics are presented in Table 1.
Participant characteristics.
Following expert consultation, the 24-item scale showed a positive correlation with the Stigma Scale for Chronic Illness (ρ = 0.91, P < 0.001), as well as the Self-rating Depression Scale (ρ = 0.84, P < 0.001). The 24 items were initially submitted for factor analysis, and 3 ( ‘Others still treat me in a friendly manner after the stroke’, ‘Someone looks down upon me because of the stroke’, and ‘I was excluded from family discussions after the stroke’) were removed because their loadings were >0.35 on two or more factors; one item ( ‘I experience obstacles in my job after the stroke’) only belonged to one factor.
Cronbach’s α for the total 24-item scale was 0.94 (P < 0.001), while that of each subscale ranged between 0.80 and 0.88 (P < 0.001). One item (‘Others treat me the same as before, after the stroke’) was eliminated because its absence resulted in a higher α on both the total scale and subscales. All inter-scale and inter-subscale correlation coefficients were >0.5 (P < 0.001). To minimize the scale, three items (‘I can still keep clean and tidy even though I had a stroke’, ‘I lost some friends after the stroke’, and ‘I feel powerless to do many things after the stroke’) were removed as the inter-item correlation coefficient >0.65. A total of eight items were removed, leaving the final scale with 16 items.
Psychometric evaluation of the 16-item Stroke Stigma Scale
Items on the 16-item Stroke Stigma Scale are presented in Table 2 and Supplemental Table 3. This scale contains four factors: ‘physical impairment’ contains four items, ‘social isolation’ has three items, ‘discrimination experience’ comprises four items, and ‘internalized stigma’ contains five items. We assessed the validity and reliability again, based on the responses of 288 patients with stroke.
The Stroke Stigma Scale with 16 items (English version).

‘Reverse-scored’.
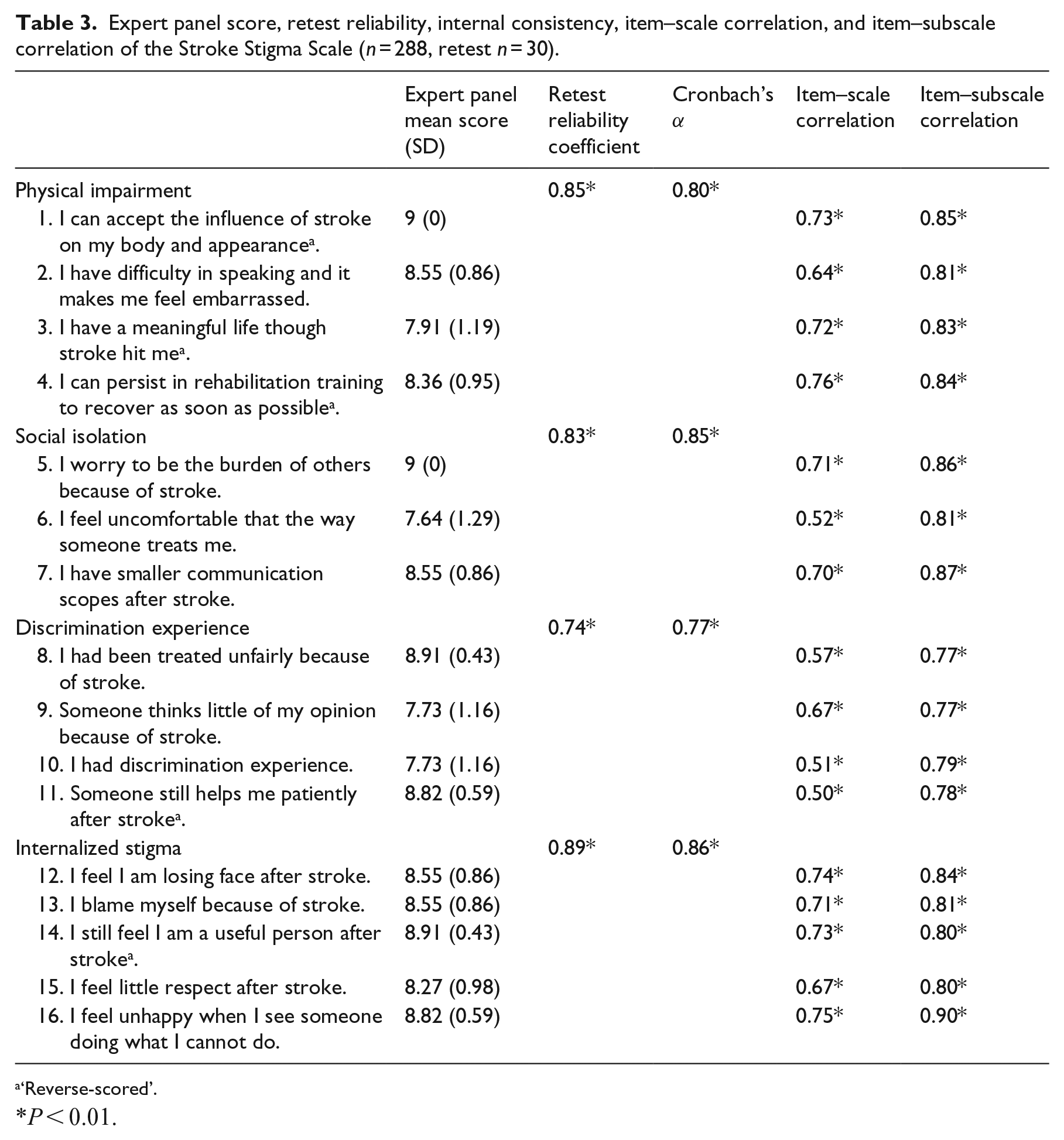
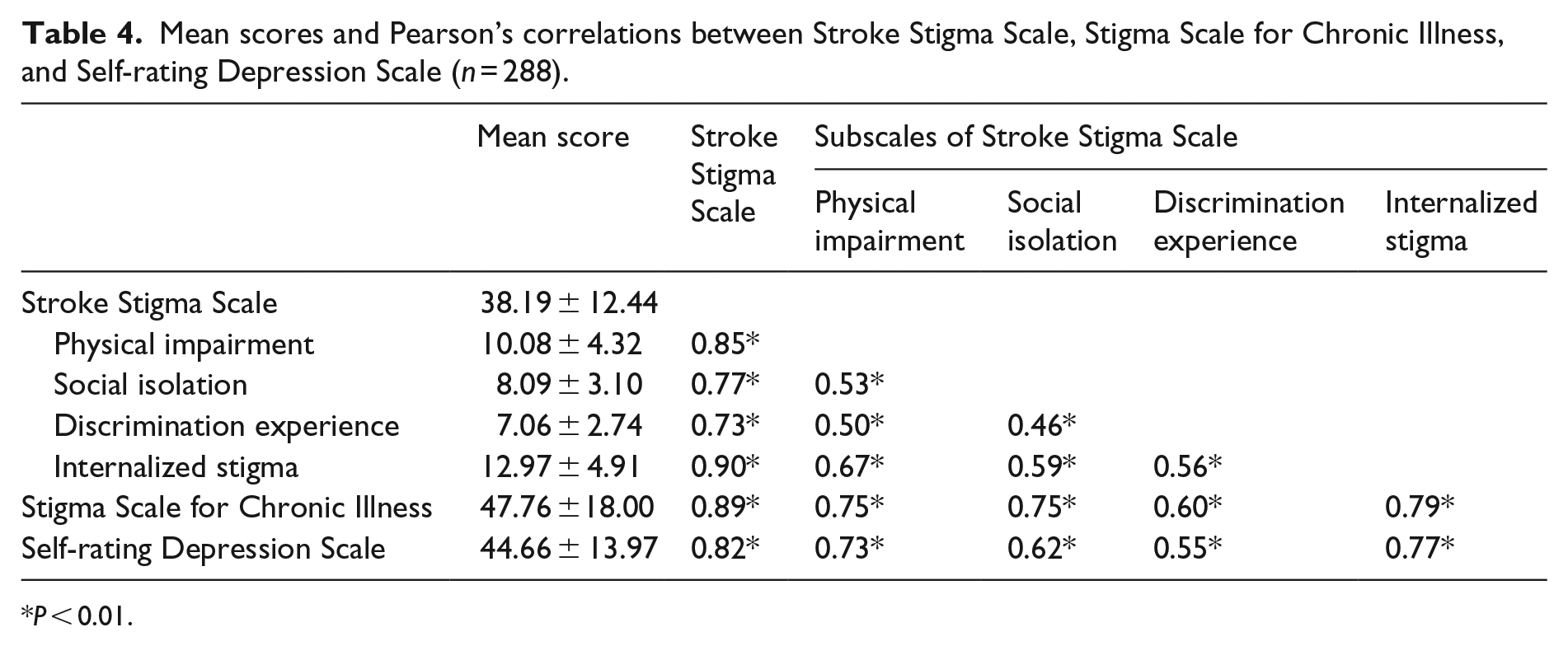
Table 3 shows that all 16 items were scored >7 points, indicating good content validity. The Stroke Stigma Scale had strong positive correlations with both the Stigma Scale for Chronic Illness (ρ = 0.89, P < 0.001) and the Self-rating Depression Scale (ρ = 0.82, P < 0.001) (Table 4). Before exploratory factor analysis, the Kaiser–Meyer–Olkin index was 0.931 and Bartlett’s sphericity test was suitable (χ2 = 2245.49, df =120, P < 0.001).
Expert panel score, retest reliability, internal consistency, item–scale correlation, and item–subscale correlation of the Stroke Stigma Scale (n = 288, retest n = 30).
‘Reverse-scored’.
P < 0.01.
Mean scores and Pearson’s correlations between Stroke Stigma Scale, Stigma Scale for Chronic Illness, and Self-rating Depression Scale (n = 288).
P < 0.01.
Table 5 presents the results of the exploratory factor analysis. Four components with eigenvalues >1 emerged, accounting for 68.05% of the variance in the set of variables (factor 1 = 44.92%, factor 2 = 9.08%, factor 3 = 7.68%, and factor 4 = 6.37%). Five items loaded on the first factor with loadings ranging from 0.62 to 0.74, all related to patients’ internalized stigma. Four items, relating to physical impairment, loaded on the second factor with loadings ranging from 0.70 to 0.80. The four items of discrimination experience loaded on the third factor, with loadings ranging from 0.52 to 0.80. The last three items, describing social isolation, loaded on the fourth factor with loadings ranging from 0.74 to 0.56.
Rotate component matrix of the final Stroke Stigma Scale.

Extraction method: principal component analysis; rotation method: varimax with Kaiser normalization (n = 288).
Bold values: items’ maximum loading.
‘Reverse-scored’.
Considering consistency, Cronbach’s α of the total scale was 0.92 and 0.77–0.86 for each subscale. All item removals resulted in a lower α of the total scale. The item–scale correlation coefficients were 0.50–0.76, and item–subscale correlation coefficients were 0.77–0.90 (Table 3). The test–retest reliability achieved strong agreement, with intra-class correlation coefficients at 0.92 (P < 0.001) for the total scale and 0.74–0.89 (P < 0.001) for each subscale (see Supplemental Appendix Figure 2).
Discussion
In this study, we showed that the Stroke Stigma Scale is a reliable and valid instrument to measure perceived stigma among patients with stroke. It is the first stroke scale to evaluate perceived stigma using the subscales physical impairment, social isolation, experience of discrimination, and internalized stigma. The physical impairment subscale elucidated the level of stigma attributed to poor body image, while the social isolation subscale assessed stigma related to social interactions after stroke. The effect of stigma associated with limited opportunities or experiences of injustice was assessed using the experience of discrimination subscale. Finally, stigma associated with negative shifts in identity was evaluated with the internalized stigma subscale. Not only did these four subscales match the factors that emerged from exploratory factor analysis, but they also satisfied the phenomenon of perceived stigma related to stroke, as per our perceived stroke stigma model, positioning the Stroke Stigma Scale as a unique measure for the assessment of perceived stigma of patients with stroke.
The initial interviews revealed that stigma may emerge in patients with stroke at different stages of their illness. Stigma is potentially a major contributor to social isolation and depression and may hinder poststroke recovery at all stages of the illness, resulting in changes in social roles, communication difficulties, and challenges related to transportation and employment. 25 An accurate measurement of stroke stigma is therefore in the best interests of the patient.
When comparing the total scores, the Stroke Stigma Scale showed a strong linear correlation with the Stigma Scale for Chronic Illness, 8 suggesting excellent criterion validity for the Stroke Stigma Scale. However, not all the dimensions of the Stroke Stigma Scale had high correlations (ρ ⩾ 0.75) with the Stigma Scale for Chronic Illness. The dimension related to discrimination experience, for example, had a low correlation (ρ = 0.60). Many stroke survivors believe that stroke completely changed their lives and they may think that it is almost impossible to live and work as before. They desire but fear a return to society, as they always consider themselves to experience discrimination, including limited opportunities and being treated unfairly. 6 It is therefore necessary to assess stroke-related stigma associated with the experience of discrimination, and the Stroke Stigma Scale is a useful tool to do so.
Although a strong linear correlation was found between the Stroke Stigma Scale and the Stigma Scale for Chronic Illness, several distinctions between these two scales show the superiority and necessity the novel Stroke Stigma Scale in the assessment of perceived stroke-related stigma, not least of all the fact that the measurement objectives of the two scales are completely different. Unlike the Stigma Scale for Chronic Illness, a general scale that is used with all patients with neurological chronic illness, the Stroke Stigma Scale is only used in patients with stroke, showing more specificity in evaluating stroke stigma. Different measurement objectives further result in different item content, which is the second major distinction between the two scales. The Stroke Stigma Scale not only distinguishes between internalized and enacted stigma but also evaluates more dimensions associated with stroke stigma, including the stigma related to physical impairment, social isolation, and experience of discrimination. Item expression is the third major distinction, resulting in different scoring methods. In order to avoid the unpleasant effect of negative word usage, we formulated the items to reflect a positive approach, which necessitated the inclusion of five reverse-scored items in the Stroke Stigma Scale. This distinction improved the scale’s acceptability in our preliminary evaluation. Furthermore, there are only 16 items in the Stroke Stigma Scale compared to 24 items in the Stigma Scale for Chronic Illness. With acceptable reliability and validity, the shorter length of the new scale may improve completion rates.
Depression was assessed in this study based on previous studies. In 2001, Berger et al. 10 proposed that ‘how patients respond to illness, including many of the possible consequences of stigma such as depression, is at the very heart of nursing’, suggesting that depression could be a consequence of stigma. Recent research with people with depressive disorder also came to the conclusion that stigma is strongly associated with deep depression.26,27 Moreover, in research on patients with multiple sclerosis, 13 lung cancer, 28 and neurological illnesses,8,9 depression was regarded as one of the main causes of psychological distress and used as one of related criteria to evaluate the stigma measure scales. Similarly, we used depression as a related criterion in our study to evaluate the Stroke Stigma Scale. Our findings showed positive correlation between the stigma level established by the Stroke Stigma Scale, and level of depression, as evaluated by the Self-rating Depression Scale in patients with stroke.
Certain limitations should be taken into account when interpreting our results. First, the qualitative interview, psychometric, and test–retest reliability samples were all recruited conveniently. Although these samples were drawn from three different hospitals, all the assessments were completed while the participants were inpatients. Stigma among stroke survivors living in their communities therefore remains unaccounted for. The second limitation is our small sample size. Although the Stroke Stigma Scale was developed based on perceived stigma theory, and while focusing on perceived stigma only in patients with stroke was regarded as one of the advantages of the Stroke Stigma Scale in comparison with the Stigma Scale for Chronic Illness, more studies using larger sample sizes are needed to confirm this advantage. Third, in this study, we only used depression as a related criterion to help evaluate the Stroke Stigma Scale. While depression is one of the most common sources of psychological distress among patients with stroke, further research is required to evaluate the Stroke Stigma Scale against other sources of psychological distress, such as anxiety, loneliness, self-esteem, and loss of social support.
Clinical messages
The Stroke Stigma Scale is the first stroke scale to assess perceived stigma using the subscales physical impairment, social isolation, experience of discrimination, and internalized stigma.
The Stroke Stigma Scale is a reliable and valid measure of perceived stigma in patients with stroke.
Supplemental Material
Supplementary_material – Supplemental material for The Stroke Stigma Scale: a reliable and valid stigma measure in patients with stroke
Supplemental material, Supplementary_material for The Stroke Stigma Scale: a reliable and valid stigma measure in patients with stroke by Minfang Zhu, Hongzhen Zhou, Weibin Zhang, Yingying Deng, Xiaoyan Wang, Xuejie Bai, Muling Li, Ruidan Hu, Jiakun Hou and Yangyang Liu in Clinical Rehabilitation
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Science and Technology Program of Guangzhou, China, under Grant 201803010084.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.