
Abstract
Objective:
The objective was to evaluate the effectiveness of early rehabilitation on arm range of motion (ROM), strength and function after breast cancer surgery (BCS). Data sources: PubMed, MEDLINE, Bireme, Embase, LILACS and CINAHL databases were searched.
Methods:
Two independent reviewers selected randomized controlled trials evaluating women who underwent early rehabilitation to restore arm ROM, strength or function after BCS. Cochrane Collaboration recommendations and Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed. Methodological quality was assessed by the PEDro scale. The International Classification of Functioning, Disability and Health was considered to analyze results. Effect size (ES) was calculated for clinical relevance interpretation of the outcomes of interest, and the evidence was summarized through the Grading of Recommendations Assessment, Development and Evaluation (GRADE) system.
Results:
Up to June 2019, a total of 1658 references were identified and 15 studies were included. Twelve of them presented adequate methodological quality. A total of 1710 patients were evaluated. Few studies performed the simultaneous assessment of variables related to body structure and function and patient-reported outcomes. A moderate level of evidence was synthesized regarding the effectiveness of ROM exercises for improving arm flexion, abduction and external rotation (ES: 0.45–2.5). A low level of evidence was synthesized regarding the effectiveness of isolated strengthening exercises for patient-reported arm function. ROM exercises associated with muscle strengthening exhibited a moderate level of evidence for improving shoulder flexion (ES: 1.4–2.4).
Conclusion:
Both ROM and strengthening exercises associated with ROM exercises improved shoulder flexion, abduction and external rotation ROM after BCS. Shoulder abduction and external rotation showed less recovery, irrespective of the intervention applied.
Introduction
Breast cancer surgery is associated with reduced arm range of motion, weakness of the shoulder muscles,1,2 decreased arm function2,3 and altered scapular kinematics during arm movements.4,5 All these factors may limit activities of daily living, and exercise therapy could be an effective approach for preventing and restoring arm function after breast cancer surgery. 6
Protocols performed in the early and late postoperative period of breast cancer have been considered beneficial in improving shoulder 7 and arm function.8–10 Nevertheless, there is no consensus on the most effective exercise approach to prevent functional changes in the arms of these patients considering the different stages of the postoperative period.
Four systematic reviews11–14 evaluating the effects of upper limb exercises on arm range of motion and muscle strength after breast cancer surgery were identified. These studies, published between 2010 and 2015, focused on the effects of immediate versus late postoperative interventions after breast cancer surgery and identified positive effects of early rehabilitation.11–13 The study by De Groef et al. 14 included five randomized controlled trials (RCTs) that investigated the effectiveness of exercise therapy on pain and range of motion after six weeks of surgery. Nevertheless, none of these reviews provided specific recommendations regarding the type of exercise and protocol characteristics that should be used on clinical practice to improve shoulder function, range of motion and muscle strength in the immediate postoperative period of breast cancer surgery.
Considering that shoulder range of motion, muscle strength, scapular kinematics and upper limb function are impaired in the long term of surgery, 5 there is a lack of updated evidence regarding the effects and characteristics of early rehabilitation protocols applied following breast cancer surgery for improvement of upper limb clinical measures and patient-reported outcomes.
Thus, this systematic review aims to summarize evidence regarding the effectiveness of early rehabilitation in the immediate postoperative period of breast cancer surgery for arm function, range of motion and strength.
Methods
This systematic review followed Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines 15 and the recommendations of the Cochrane Collaborations for systematic reviews. 16 This review was registered in the International Prospective Register of Systematic Reviews (PROSPERO) under number CRD42017058279.
Up to June 2019, an electronic search was performed in the following databases: PubMed, MEDLINE, Embase, Bireme, CINAHL and LILACS. For the PubMed, the following keyword combination was used: (“Breast Neoplasms”[Mesh] OR breast cancer) AND surgery AND (upper limb function OR shoulder range of motion OR scapular kinematics OR muscle strength). The search strategy used is given in more detail in the Supplemental Material. Each electronic database was searched from the earliest year available to identify relevant studies.
Two independent reviewers performed the selection process based on titles, abstracts and full-text reading. Any disagreements were solved by consensus. Full texts of potentially relevant articles were retrieved for final evaluation. Manual search was performed through the screening of primary studies’ reference lists to identify possible relevant studies not retrieved by the electronic search.
This systematic review included only RCTs that evaluated women who had undergone breast cancer surgery and received early rehabilitation, in the immediate postoperative period. The rehabilitation program had to commence within the first eight weeks after surgery. Arm range of motion, strength and function reported by the patients were the primary outcome measures of interest.
The methodological quality of the included studies was assessed using the PEDro scale (www.pedro.org.au), 17 which is based on the Delphi list. 18 The studies indexed in the PEDro database had been previously rated. 19 For the present review, randomized trials with scores greater than or equal to 6 were considered of high methodological quality, those which scored 4 or 5 were classified as fair quality and those which presented a score less than or equal to 3 were classified as low methodological quality. 20
A standardized form adapted from the Cochrane Collaboration model 16 was used to extract data on participants (number of patients, age, body mass index, comparison groups and type of surgery), intervention (onset, characteristics, frequency, duration and setting) and outcome measures (outcome assessed, assessment tool, statistical outcomes and clinical relevance of the intervention). The clinical relevance of interventions was interpreted through the effect size (ES) with a 95% confidence interval (CI) for continuous outcomes in each comparison group, considering pre- and post-intervention values. The treatment effect was further classified as small (<0.20), moderate (between 0.21 and 0.79) and large (>0.80), according to the Cohen index. 21
Primary study results were interpreted according to the effectiveness of the rehabilitation program in promoting gains or preserving arm range of motion, strength or function after surgery. Results were considered positive when the comparison between intervention and control groups showed a statistically significant improvement in primary outcomes. The preventive effects of rehabilitation were also considered positive when impairments were not observed. Studies that showed a significant reduction in outcomes after the intervention were classified as having no effect. The ES was calculated for the studies that presented mean and standard deviation (SD) data for the primary outcomes.
Analysis and data synthesis
The quality of the evidence for each intervention was determined based on the Grading of Recommendations Assessment, Development and Evaluation (GRADE) 22 system as high, moderate, low or very low level of evidence. For evidence synthesis, follow-up periods of three and six months were considered. All tables were generated by GRADEpro software after the GRADE criteria analysis was performed by authors.
The outcomes presented by the primary studies were complementally analyzed taking into account the International Classification of Functioning, Disability and Health (ICF) perspective about functioning and disability. 23 Thus, outcomes were qualitatively analyzed considering measures of body structure and function, which allows the assessment of impairments and patient-reported outcome measures (PROMs), which measure patients’ activity limitations and participation restrictions, allowing the identification of functional loss and disability. 24
Results
The electronic search resulted in a total of 1658 references, 15 of which were included. The flowchart of this review selection process is presented in Figure 1.
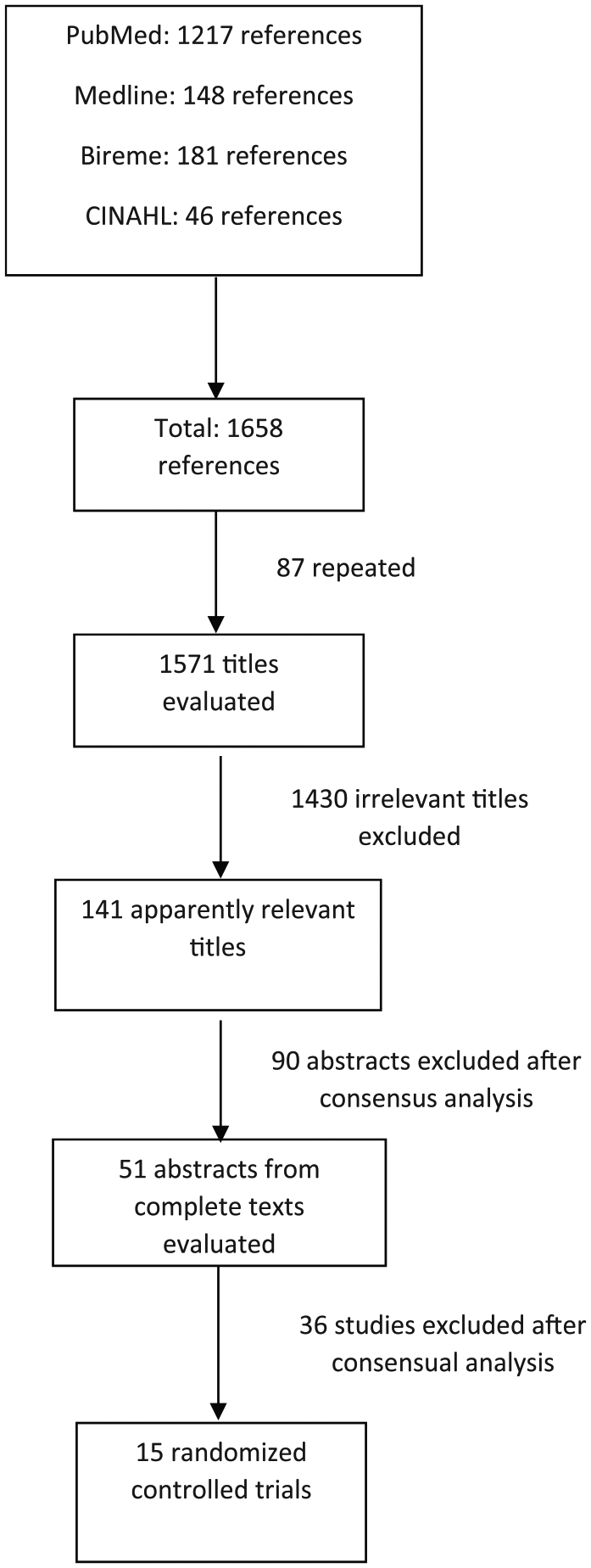
Selection process steps of the primary studies.
A total of 1710 patients were evaluated. Of the 15 studies included, 13 were classified as high methodological quality.7,10,25–35 The most critical criteria to be satisfied were related to participant (100%) and therapist blinding (100%) and intention-to-treat analysis (100%). Only five studies7,26,28,35 reported blinding assessors who measured at least one key outcome of the intervention applied.
The main characteristics of the studies in terms of participants, exercise programs and outcomes assessed are shown in the Supplemental Table S1. All the analyzed outcomes were categorized according to the ICF perspective about functioning and disability and its domains: body structure and function and PROMs (Supplemental Table S2).
In general, the exercise protocols started at the first week following the surgery and consisted of upper limb active exercises, passive and active stretching, shoulder range of motion and strengthening exercises combined with scar massage. Moreover, the protocols were carried out from 10 to 19 days in three studies,28,33,36 between one and two months in four studies,10,25,26,29 between three and six months in five studies7,31,32,34,35,37 and two studies did not report protocol duration.27,30
Only eight studies7,25,26,28,32,34,35,37 provided mean and SD data to calculate the ES of the intervention applied to the operated upper limb. Regarding shoulder range of motion, improvements were identified at three7,27–29,33,34,36 and six7,24–31,36 month follow-up periods. The ES ranged from 0.03 to 2.4. Considering the studies that reported a positive treatment effect,28,32 the ES ranged from 1.4 to 2.4 for flexion range of motion, 1.3–1.9 for abduction and 0.45–0.90 for shoulder external rotation. Moreover, 95% CI values ranged from 0.073 to 2.8 for shoulder flexion; from 0.69 to 2.2 for abduction and from −0.06 to 1.4 for shoulder external rotation. Regarding the improvement of shoulder function, the ES ranged from −0.31 to 2.5 and the 95% CI ranged from 0.12 to 2.5 in those studies with a positive treatment effect.7,28,34,35
Evidence synthesis regarding intervention effectiveness in improving upper limb range of motion, muscle strength and functional outcomes based on the GRADE approach is presented in Table 1 for the three-month follow-up and in Table 2 for the six-month follow-up period.
Summary of body of evidence for upper limb exercises in the three-month follow-up according to the GRADE approach.
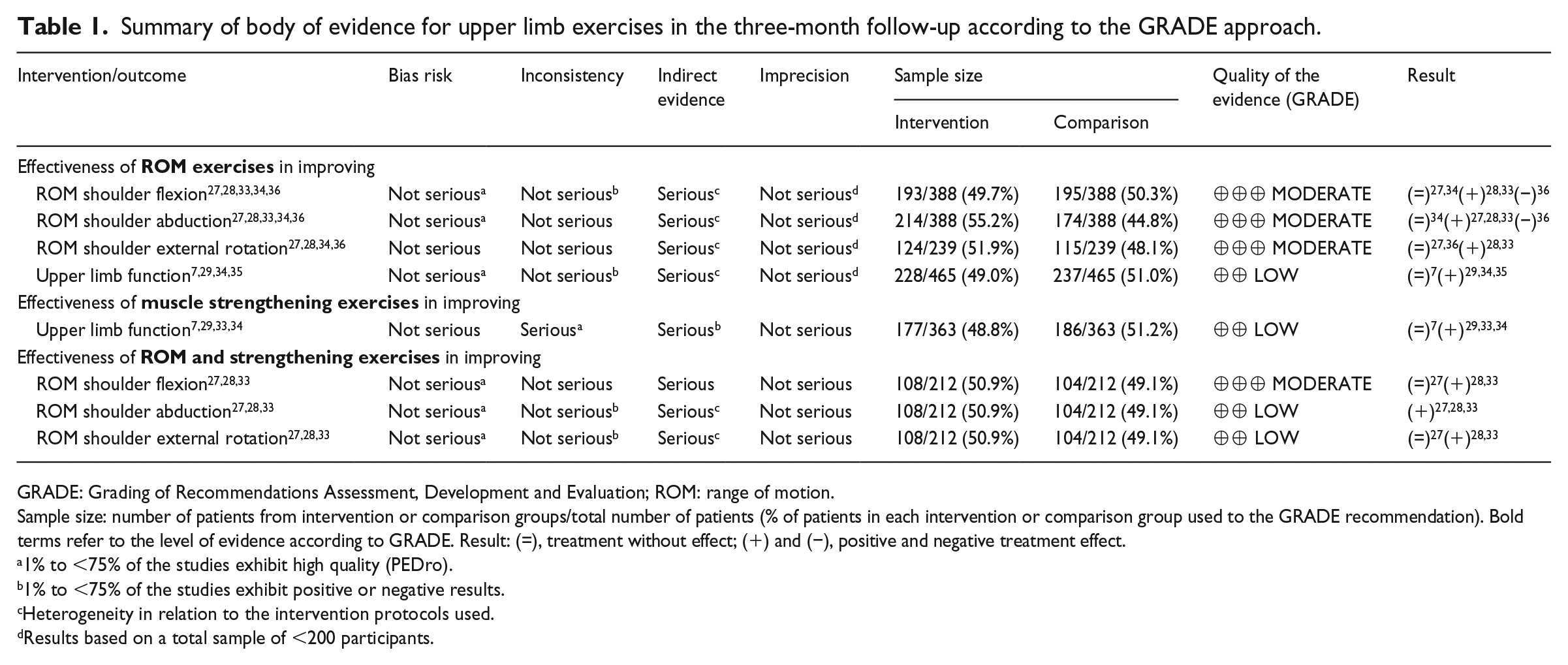
GRADE: Grading of Recommendations Assessment, Development and Evaluation; ROM: range of motion.
Sample size: number of patients from intervention or comparison groups/total number of patients (% of patients in each intervention or comparison group used to the GRADE recommendation). Bold terms refer to the level of evidence according to GRADE. Result: (=), treatment without effect; (+) and (−), positive and negative treatment effect.
1% to <75% of the studies exhibit high quality (PEDro).
1% to <75% of the studies exhibit positive or negative results.
Heterogeneity in relation to the intervention protocols used.
Results based on a total sample of <200 participants.
Summary of body of evidence for upper limb exercises in the six-month follow-up according to the GRADE approach.
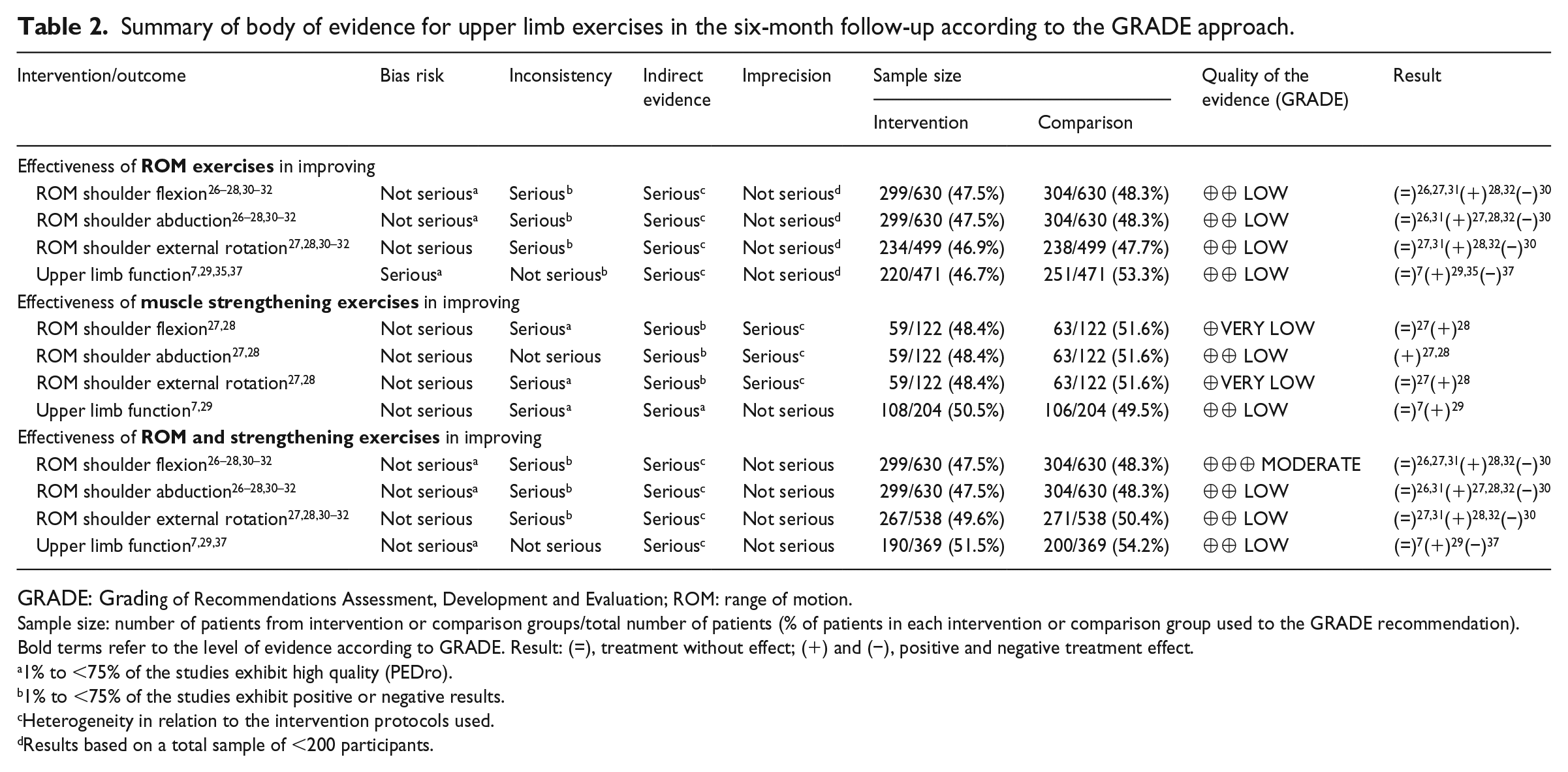
GRADE: Grading of Recommendations Assessment, Development and Evaluation; ROM: range of motion.
Sample size: number of patients from intervention or comparison groups/total number of patients (% of patients in each intervention or comparison group used to the GRADE recommendation). Bold terms refer to the level of evidence according to GRADE. Result: (=), treatment without effect; (+) and (−), positive and negative treatment effect.
1% to <75% of the studies exhibit high quality (PEDro).
1% to <75% of the studies exhibit positive or negative results.
Heterogeneity in relation to the intervention protocols used.
Results based on a total sample of <200 participants.
Nine studies investigated the effectiveness of protocols in improving upper limb range of motion and involved 988 patients,26–28,30–36 whereas five studies with 769 patients investigated effectiveness of protocols in improving shoulder function through patient-reported outcomes assessed by questionnaires7,10,29,35,37 (Tables 1 and 2).
Isolated range of motion exercises exhibited a moderate level of evidence for increasing shoulder flexion, abduction and external rotation after three months of follow-up with a low level of evidence regarding shoulder function improvement (Table 1). After six months of follow-up, this protocol presented a low level of evidence in improving shoulder range of motion and function (Table 2).
Isolated muscle strengthening exercises revealed a low level of evidence in improving shoulder function reported by the patients after three months of follow-up (Table 1). Moreover, the same protocol presented a low level of evidence in improving shoulder abduction and a very low level of evidence in improving shoulder flexion and external rotation and function after six months of follow-up (Table 2).
A range of motion exercises associated with muscle strengthening exhibited a moderate level of evidence for improving flexion range of motion after three and six months of follow-up and a low level of evidence for improving abduction and external rotation range of motion both at three and six months after breast cancer surgery (Tables 1 and 2).
Range of motion exercises, muscle strengthening exercises and range of motion exercises associated with muscle strengthening exhibited a low level of evidence for improving upper limb function after three and six months of follow-up (Tables 1 and 2). Upper limb function was assessed by patient self-reporting through questionnaires in five studies.7,26,29,35,37 Nevertheless, three studies28,33,35 used a series of 10 questions related to upper limb function without reporting the validity of these questionnaires for breast cancer patients.
Discussion
This systematic review aimed at evaluating the effectiveness of early rehabilitation protocols on range of motion, muscle strength and arm function after breast cancer surgery. All the analyzed outcomes were categorized according to the ICF perspective about functioning and disability.
A moderate level of evidence was identified regarding the effectiveness of protocols that used range of motion exercises to improve shoulder flexion, abduction and external rotation range of motion after a three-month follow-up. The evidence was also moderate for protocols that associated range of motion exercises with strengthening exercises to enhance shoulder flexion after three- and six-month follow-ups. A low level of evidence was identified regarding the effectiveness of the range of motion exercises, muscle strengthening exercises and range of motion exercises associated with muscle strengthening exercise protocols to improve arm function.
Although the majority of study protocols were started in the first week following surgery,7,26–37 the exercises used were heterogeneous, as were the frequency and duration of the sessions and total treatment duration. The evaluation tools used in the studies were also heterogeneous. Another critical point is related to the follow-up periods, which ranged from the five postoperative days to 12 months after surgery. Periodic reassessment is recommended to identify the minimum intervention period required to observe effective responses in muscle strength, range of motion and upper limb function. Thus, we recognize that strength of the evidence synthesized was compromised by this protocol heterogeneity. Based on the included primary studies of this review, no recommendations on the total duration of timing of beginning rehabilitation program could be done. Nevertheless, a previous systematic review by De Groef et al. 14 appoints that exercises should be started in the first few days after surgery and can be increased gradually. 14
Effectiveness of range of motion exercises
The analysis of 10 studies including 825 patients26–28,30–36 revealed a moderate level of evidence regarding the effectiveness of the range of motion exercise protocols for range of motion flexion, abduction and external rotation in the three-month follow-up, with moderate to high ES. On the other hand, a low level of evidence was observed for the effectiveness of this type of intervention in improving upper limb function reported by patients and assessed through questionnaires, after the analysis of five studies7,29,33–35 including a total of 763 patients. It is important to highlight that four studies identified a preventive effect of the applied intervention. Three of them reported improved upper limb function,10,29,35 while one reported function maintenance after treatment 7 and just one reported a decrease in upper limb function. 37
Previous research has shown that loss of range of motion is common after breast cancer surgery. 5 As such, the use of upper limb range of motion exercises during rehabilitation may contribute to recovering shoulder movement and upper limb function. 12 Thus, the perception of shoulder function maintenance after surgery must be recognized as a positive result.
The evidence on the effectiveness of range of motion exercises for improved abduction, flexion and external rotation six months after surgery was low. A number of important factors, such as the lack of information about session frequency and duration, the protocol used 27 and the lack of training for external rotators27,32 should be highlighted. The heterogeneity of the exercise protocols regarding the type of training, session’s frequency and duration as well as the total duration of the protocols applied associated with the different results obtained after treatments are also important factors that led to the low level of evidence synthesized by the GRADE system.
According to our study, a moderate level of evidence was identified regarding the effectiveness of range of motion exercises on shoulder range of motion improvement at three and six months after surgery. Literature demonstrates that after approximately six months of breast cancer surgery, among 1%–67% of patients who had undergone surgery and radiation present a decrease of shoulder flexion and abduction, ranging from 132° to 175°. 6 The emphasis on preserving limb function, primarily in the immediate postoperative period, may minimize long-term function loss after surgery.
Effectiveness of muscle strengthening exercises
After the analysis of four studies28,32–34 involving 661 participants, a low level of evidence was synthesized regarding the effectiveness of muscle strengthening exercises for upper limb function improvement at three months of follow-up.7,29,33,34 A low and very low level of evidence was synthesized regarding the effectiveness of this protocol for improving shoulder flexion, abduction and external rotation, based on the analysis of two studies27,28 involving 122 patients in the six-month follow-up period. Moreover, a low level of evidence was synthesized, based on two studies7,29 which included 422 patients, regarding the effectiveness of muscle strengthening exercise protocol in improving upper limb function. The reduced number of available studies, heterogeneity of the protocols and low methodological quality 27 of the primary studies limited the strength of the recommendations. Moreover, we considered that valid, reliable and reproducible questionnaires should also be applied to analyze upper limb function in surgically treated breast cancer patients.
Effectiveness of range of motion exercises associated with muscle strengthening
After the analysis of eight studies7,10,26–28,30–32 involving 907 patients, a moderate level of evidence was synthesized regarding the effectiveness of range of motion exercises associated with muscle strengthening to improve flexion range of motion after three and six months of follow-up. Moreover, a low level of evidence was identified regarding the effectiveness of the same protocol to improve shoulder abduction and external rotation27,28,33 in the three months of the follow-up period. After six months of follow-up, a moderate level of evidence was synthesized regarding the effectiveness of range of motion exercises associated with muscle strengthening protocols to improve flexion range of motion, while a low level of evidence was identified regarding improvements on abduction and external rotation range of motion and upper limb function.26–28,30–32
The level of synthesized evidence was low, although studies have shown a positive result from exercise protocols applied.10,37 Muscle strength is of importance for an adequate biomechanical functionality of the shoulder joint 38 and could be an efficient therapeutic strategy to maintain shoulder strength after surgery 39 in order to avoid altered scapular kinematics and poor upper limb function.4,5 The low number of studies assessing the effectiveness of this type of protocol, heterogeneity of the protocols applied and lack of specificity between the type of exercise and outcome analyzed are recognized as the mains factors, which hindered the evidence synthesis.
Effectiveness of protocol exercise to improve shoulder function
Among the 15 studies included in this review, 97,10,26,28,29,33–35,37 considered PROMs. Three7,29,34 studies analyzed the results of upper limb function based on the Disability of Arm, Shoulder and Hand (DASH) score, 40 three10,35,37 used the Constant–Murley score 41 and one 26 study assessed shoulder function based on the shoulder rating score. 42 Only four studies evaluated function report and PROMs simultaneously,26,28,33,34 and among them, only two26,34 used valid PROMs. It is essential to use valid assessment tools to investigate disability levels and monitor progress throughout treatment. The importance of PROMs must be recognized as they capture information about the impact of a musculoskeletal shoulder condition on aspects related to physical, emotional and social functioning. 24
According to our findings, shoulder function showed less potential of recovery, irrespective of the intervention applied. Among the nine included studies, which used PROMs, only five28,29,33–35 presented a positive treatment effect associated with moderate to high ES (0.31–2.5). It is important to consider that different types of questionnaire used may also have influenced the results. On the other hand, 426,28,33,34 of the 15 included studies that evaluated both function reported by the patients and clinically based measures of body structure and function (representative by the ROM) presented positive results on shoulder function which were accompanied by positive results of PROMs too. Thus, PROMs must be recognized as an important measure of the treatment impact.24,43 Based on these results, we can conclude that both standardized clinical measures and PROMs deserve researchers’ attention to measure quality of care for breast cancer patients.
Limitations and scientific recommendations
Some limitations should be mentioned as factors which hindered the quality of the evidence synthesized: as the different types of exercise protocols applied, a large variety of follow-up time frames, the heterogeneity among the methods used to assess clinical measurements and patient-reported outcomes among included studies. Regarding primary studies’ internal validity, the allocation concealment, blinded evaluation of the outcomes and inclusion of intention-to-treat analysis deserve researcher’s attention for future studies’ design.
With respect to external validity, there was also a lack of detailed information on the protocol used, such as session frequency, treatment duration and lack of ES and CI measure’s presentation. Future studies should be conducted considering these gaps, so that more conclusive evidence can be summarized regarding the effectiveness of early rehabilitation programs in restoring shoulder range of motion, strength and upper limb function in the immediate postoperative period of individuals submitted to breast cancer surgery.
Thus, future RCTs should be carried out, providing more specific information on the protocols used to allow their reproducibility in clinical practice. Another important recommendation is to evaluate these patients based on the ICF model, considering outcomes related to body function and structures as well as to patients’ activities and participation. Patient assessment considering the ICF model will contribute to provide a scientific basis for better understanding the changes in health status and functioning after breast cancer surgery and must be considered.
Clinical messages
In patients who have had surgery for breast cancers, range of motion protocols associated with strengthening exercises may improve shoulder flexion, abduction, range of external rotation and arm function.
There is little evidence regarding frequency, intensity, the exact type of exercise or duration of treatment.
Supplemental Material
Supplemental_Material – Supplemental material for Effectiveness of early rehabilitation on range of motion, muscle strength and arm function after breast cancer surgery: a systematic review of randomized controlled trials
Supplemental material, Supplemental_Material for Effectiveness of early rehabilitation on range of motion, muscle strength and arm function after breast cancer surgery: a systematic review of randomized controlled trials by Ivana Leão Ribeiro, Roberta Fátima Carreira Moreira, Angélica Viana Ferrari, Francisco Alburquerque-Sendín, Paula Rezende Camargo and Tania Fátima Salvini in Clinical Rehabilitation
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The study was supported by the Research Support Foundation of São Paulo State (FAPESP) (Process: 2011/22122-5 and 2015/50303-5). T. F. Salvini was funded by the National Research Council (CNPq) (Process: 3013442013-2).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.