
Abstract
Objective:
To investigate the validity and test–retest reliability of mHealth devices (Google Fit, Health, STEPZ, Pacer, and Fitbit Ultra) to estimate the number of steps in individuals after chronic stroke and to compare whether the measurement of the number of steps is affected by their location on the body (paretic and non-paretic side).
Design:
Observational study with repeated measures.
Setting:
University laboratory.
Subjects:
Fifty-five community-dwelling individuals with chronic stroke.
Intervention:
Not applicable.
Main measures:
The number of steps was measured using mHealth devices (Google Fit, Health, STEPZ, Pacer, and Fitbit Ultra), and compared against criterion-standard measure during the Two-Minute Walk Test using habitual speed.
Results:
Our sample was 54.5% men, mean age of 62.5 years (SD 14.9) with a chronicity after stroke of 66.8 months (SD 55.9). There was a statistically significant association between the actual number of steps and those estimated by the Google Fit, STEPZ Iphone and Android applications, Pacer iphone and Android, and Fitbit Ultra (0.30 ⩽ r ⩾ 0.80). The Pacer iphone application demonstrated the highest reliability coefficient (ICC(2,1) = 0.80; P < 0.001). There were no statistically significant differences in device measurements that depended on body location.
Conclusions:
mHealth devices (Pacer–iphone, Fitbit Ultra, Google Fit, and Pacer–Android) are valid and reliable for step counting in chronic stroke survivors. Body location (paretic or non-paretic side) does not affect validity or reliability of the step count metric.
Introduction
Physical activity and exercise guideline recommendations after stroke highlight the importance of keeping the stroke survivor physically active; in part to offset the sedentary lifestyle and associated risk of a recurrent stroke. 1 An easy way to quantify physical activity during clinical practice is the number of steps. Although it is not clear how many steps provide the ideal benefit to health, 2 7000 steps per day have been recommended for non-neurologically impaired adults. 3 However, individuals after stroke present an average of 4355 steps per day; 4 an average of 4278 steps on weekdays and 3801 on weekends. 5
Many technologies currently have a step counting system, among these are mobile applications for different operating systems and other devices, such as wearable sensors. 6 In general, mobile health technology (mHealth) generates reports often available for analysis by the professionals, as well as patients and relatives. These resources could offer external feedback to motivate an increase in number of steps per day. 7 However, these technologies may not be sensitive when applied to people with neurological diseases, including stroke, because of abnormal gait patterns. Another limiting factor is the anatomical position of the resource, which varies in the literature 7 and, it is not known yet, which place is the most appropriate to capture physical activity levels of individuals after stroke. Therefore, the use of a step-by-step activity monitoring program can be useful to increase activity outside of a clinical facility in individuals after chronic stroke.8,9
The Statement from the American Heart Association 6 recommends investigation of the measurement properties of commercially available smartphone applications and wearable sensors, since this technology is largely already in use. However, there are few studies that have investigated the validity and reliability of mHealth devices in individuals after stroke. Thus, the aims of this study are:
Determine the validity of mHealth devices (Google Fit, Health, STEPZ, Pacer, and Fitbit Ultra) compared with the criterion-standard measure to estimate the number of steps in individuals chronically after stroke.
Determine the test–retest reliability of mHealth devices, and criterion measurement to estimate the number of steps in individuals chronically after stroke.
To compare whether the number of steps in individuals chronically after stroke measured using mHealth devices is affected by where the device is positioned (paretic and non-paretic leg) on the individual.
Methods
This is an investigation of the validity and reliability of mHealth devices approved by Ethics Committee of the Faculty of Medical Science of Minas Gerais (CAAE: 80069917.9.0000.5134) and Ethics Com-mittee of Physical Education and Sport School of São Paulo (CAAE: 10937219.0.0000.5391).
The study enrolled a sample of convenience in the chronic stage after stroke recruited from two facilities: Belo Horizonte and São Paulo- Brazil during the period between March 2018 and May 2019. Each participant engaged in a one-day assessment in the laboratory. Individuals were included who met the following criteria: (a) at least six months after stroke onset, 10 (b) older than 18 years, (c) ⩾18 on the Mini Mental State Examination, 11 (d) walking speed at least 0.1 m/s during 10-meter walk test, (e) able to walk independently without assistive devices, (f) able to follow verbal commands, and (g) read, agreed and signed the informed consent.
Sociodemographic and clinical data were obtained through a questionnaire developed by the research team. Walking speed, in m/s, was assessed with the 10-meter walk test for habitual and maximal speed.12,13 Bilateral strength of knee extensors and plantar flexors, in mmHg, was assessed using the modified sphygmomanometer test. 14 Fear of falling was assessed with the Falls Efficacy Scale—International (FES-I). 15 Physical activity level was assessed with the Adjusted Activity Score of Human Activity Profile (HAP). 16 Functional capacity was assessed with the Duke Activity Status Index (DASI).17,18 The tests and questionnaires were administered by trained researchers.
Number of steps was measured by mHealth devices, as smartphone applications (Google Fit, Health, STEPZ, and Pacer), and wearable sensors (Fitbit Inc®), and criterion-standard measure (steps counted live and videotaped—for comparison—by two trained researchers) during a Two-Minute Walk Test with habitual speed.9,19 Both iOS and Android OS were chosen as operating systems.
Fitbit Inc® and Google Fit are already known to be accurate for step measurement in individuals after stroke.9,19,20 To the best of our knowledge, there are no previous studies which have investigated the accuracy of Pacer, Health, and STEPZ for step measurement after stroke. The Health device was previously validated only in non-disabled individuals. 21
All data were collected by two well-trained researchers, in a random order, during a one-day assessment. Participants were instructed to wear comfortable clothes and habitual shoes. After signing the consent term, the primary outcome (Two-Minute Walk Test) was performed.
The Two-Minute Walk Test was performed over 10 meters marked by two signaling cones. 19 The volunteers waited for the signal to start and to stop the test, using all devices. The mHealth devices used were: Google Fit, Health, STEPZ, Pacer, and the Fitbit Inc®. The smartphones used here were S480 Positivo and iphone 6s®—iOS.
The position of the monitors is illustrated in Supplemental Figure S1; the order of measurement was randomized. Prior to the test, the smartphones were positioned in the front pockets of the individuals’ paretic and/or non-paretic lower limb9,22 and the gender, body mass (Kg), and height (cm) of the individuals were input to the software system. The first test was performed with the Android OS phone (S480 Positivo) and Fitbit Inc® on the paretic side, and the iOS phone (iphone 6s®—iOS) on the non-paretic side. The second measure was performed with the inverse positioning. Rest intervals between measurement 1 and measurement 2 were provided between the tests until the heart rate returned to the basal levels.
The individuals walked at their habitual speed with monitors allocated on their body according to the measurement order. Participants were supervised for safety by a member of the research team. The tests were videotaped by iphone 6® (Apple—iOS) on a tripod positioned 86 cm high and 1 meter away at the beginning of the test. The tripod was positioned at 40° from the beginning of the test. The actual steps were determined by a researcher, who counted the steps taken by the individuals live and from the videotape recordings on two occasions, separated by one or two weeks. We found excellent test–retest reliability (ICC (2,1) P < 0.001). Thus, the actual number of steps counted live was used as the criterion-standard measure.
Descriptive statistics and tests for normality (Shapiro–Wilk) were carried out for all variables. Pearson’s correlation coefficients were calculated to examine the associations between the criterion-standard measure (live actual steps) and those estimated by the devices (Google Fit, Health, STEPZ, Pacer, and Fitbit Ultra). Cut-off values 23 were: 0–0.25: little or none; 0.26–0.50: fair; 0.51–0.75: moderate to good; and > 0.75: good to excellent relationship. Intra-class correlation coefficients (ICC (2,1)) were calculated to investigate the reliability between the actual steps and those estimated by the five devices (Google Fit, Health, STEPZ, Pacer, and Fitbit Ultra). Bland and Altman plots were generated for steps count to assess the agreement between the tests 1 and 2. An ICC value < 0.4 was considered poor, 0.4 to 0.75 as fair to good, and > 0.75 as excellent. 24 The comparison between the device position was investigated using a t-test (95% confidence interval [95% CI]). The significance level was set at 5%. All analyses were performed using International Business Machines Statistical Package for the Social Sciences (IBM SPSS, IBM Corp, Armont, NY) (Version 19) by an independent researcher.
Results
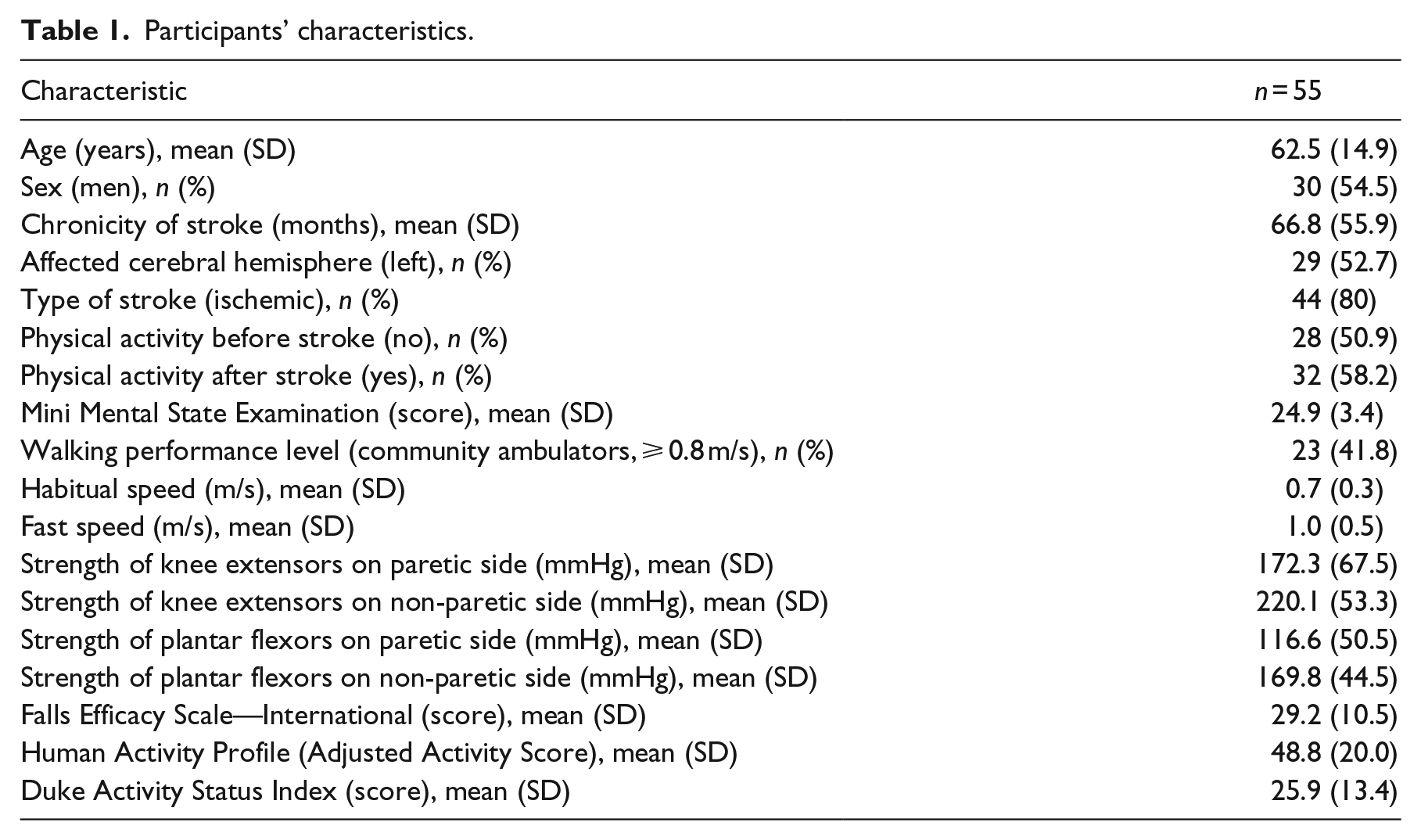
Fifty-five individuals with chronic stroke participated (Figure 1); they were 54.5% men, with a mean age of 62.5 years and a mean time from stroke onset of 66.8 months. Forty-one percent of the participants were community walkers. The participants’ characteristics are summarized in Table 1.
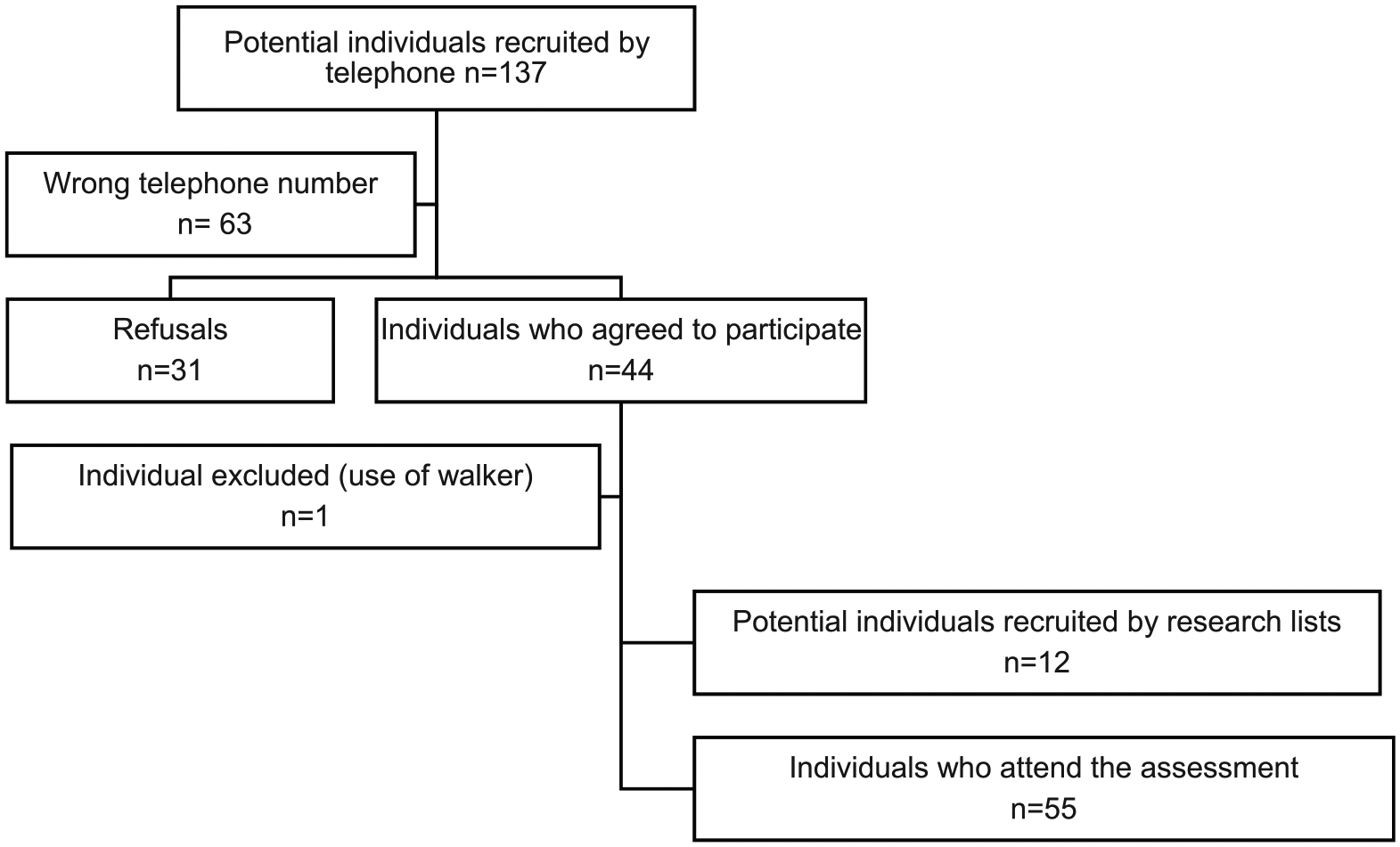
Flowchart of recruitment process.
Participants’ characteristics.
Validity
As Shapiro–Wilk test revealed a normally distributed data, the Pearson correlation was used for all analyses. It was found positive and statistically significant associations between the criterion-standard measure and the Google Fit, STEPZ iphone and Android applications, Pacer iphone and Android, and Fitbit Ultra. There was no association between the criterion-standard measure and Health iphone and Android applications (Table 2 and Figure 2).
Validity of the devices compared with the criterion-standard measure.
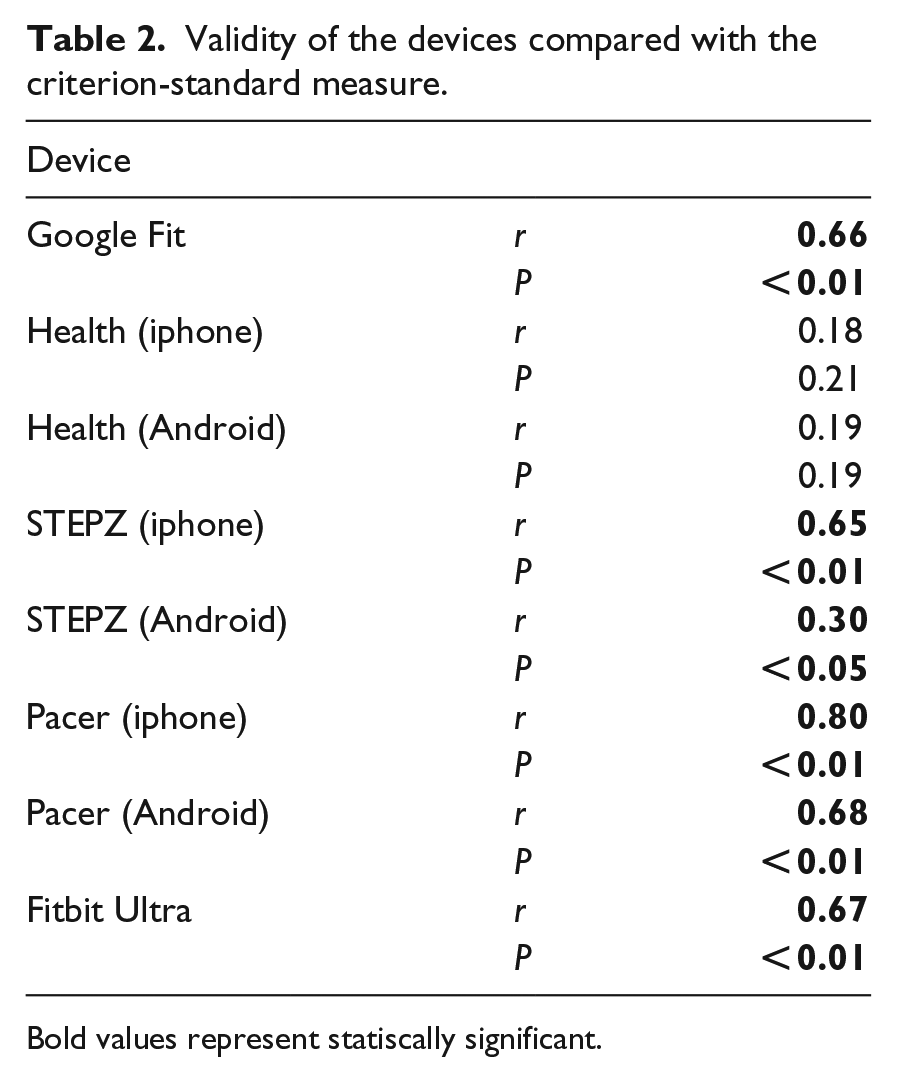
Bold values represent statiscally significant.
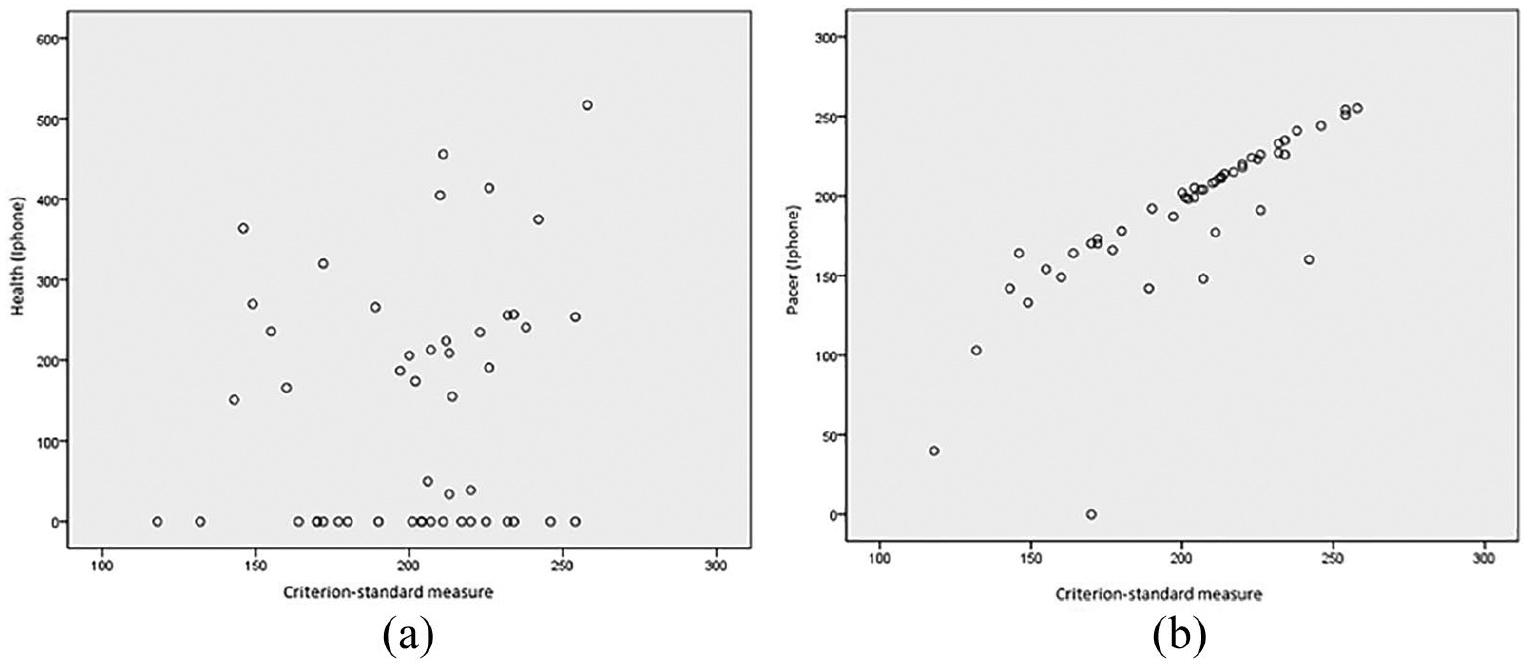
Scatter plots of the validity of the (a) Health (iphone) (r = 0.18) and (b) Pacer (iphone) (r = 0.80) with the criterion-standard measure (live actual steps).
Reliability
The ICC (2,1) analysis demonstrated no agreement between the Health (iphone) and criterion-standard measure, which showed excellent test–retest reliability (ICC = 0.99) (Table 3 and Figure 3). The other four devices/apps showed agreements ranging from poor (Health Android, STEPZ iphone, and STEPZ Android) to excellent (Google Fit, Pacer iphone, and Fitbit Ultra).
Reliability of the devices.
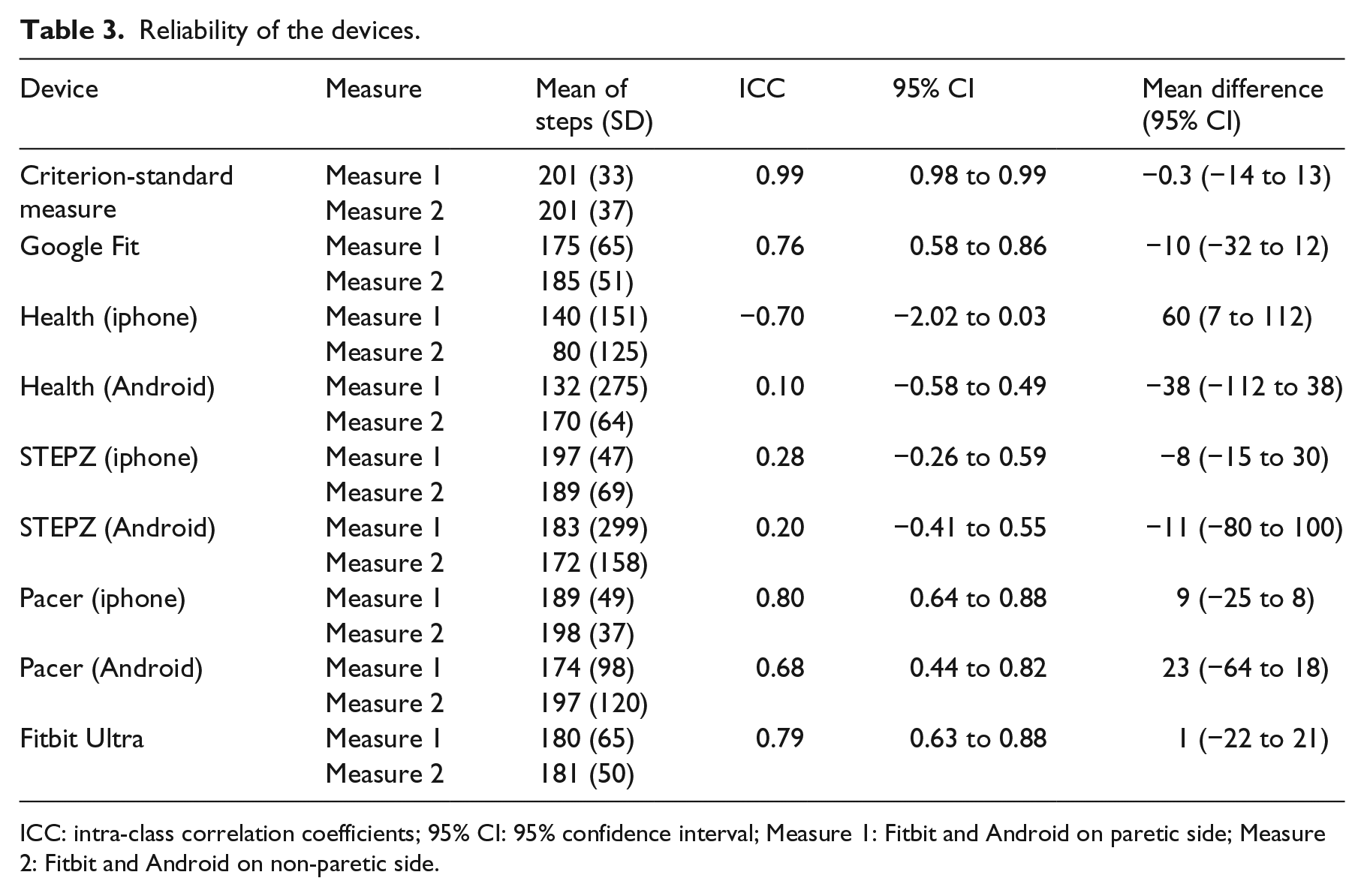
ICC: intra-class correlation coefficients; 95% CI: 95% confidence interval; Measure 1: Fitbit and Android on paretic side; Measure 2: Fitbit and Android on non-paretic side.
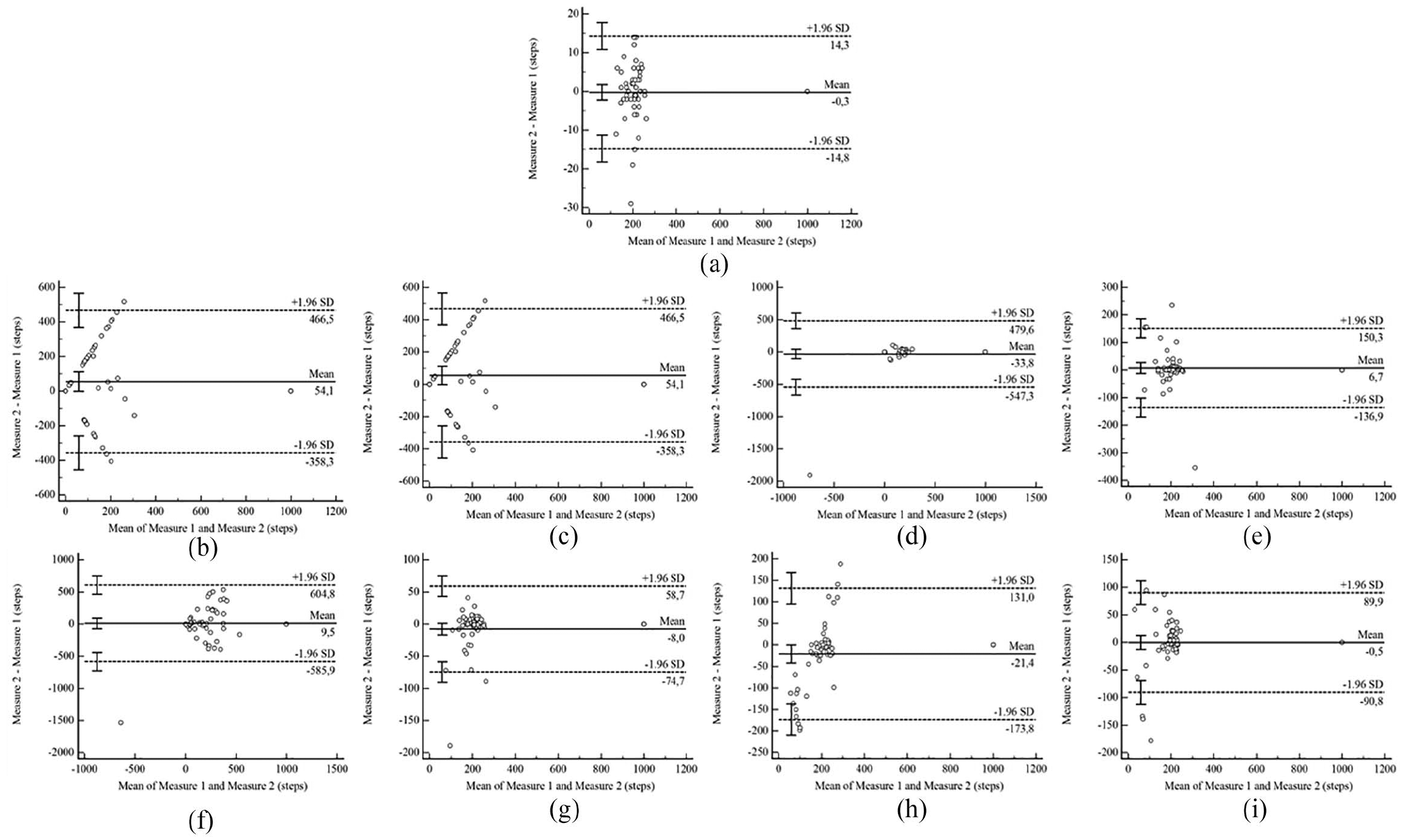
Bland and Altman plots. Individual difference in steps count between Measurement 1 and 2, plotted against individual mean (Measurement 1 and 2). Dashed line shows the group mean steps between Measurement 1 and 2. The 95% upper and lower limits of agreement represent 2 standard deviations above and below the group mean difference in steps between Measurement 1 and 2, for (a) criterion-standard measure, (b) Google Fit, (c) Health (iphone), (d) Health (Android), (e) STEPZ (iphone), (f) STEPZ (Android), (g) Pacer (iphone), (h) Pacer (Android), and (i) Fitbit Ultra.
Location on the body
No statistically significant differences were found for any of the devices in relation to location on the paretic or non-paretic side. There was considerable variance on 95% CI (Table 4).
Comparison of measurement of the devices in relation to positioning on the paretic and non-paretic sides.
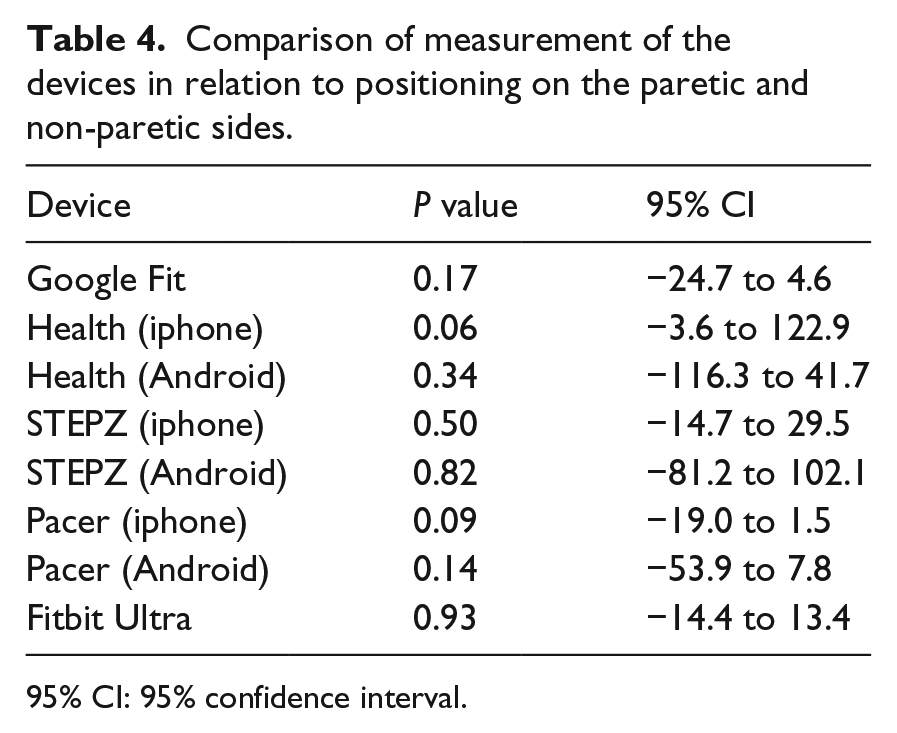
95% CI: 95% confidence interval.
Discussion
Our main findings provide evidence that mHealth devices (Pacer–iphone, Fitbit Ultra, Google Fit, and Pacer–Android) that measure the number of steps over a given period of time are all valid and reliable in comparison with a criterion-standard measure, with the exception of the Health with iphone and Android. In addition, location on the body does not appear to affect the measurement when the smartphone is positioned on the paretic or non-paretic side at hip level. Therefore, the investigated mHealth devices could be used as a valid and reliable tool to promote an increase in the number of steps in chronic stroke survivors.
The Health application did not demonstrate adequate values for validity in individuals after chronic stroke in either operating system (iOS and Android OS). In contrast, a previous study with non-disabled individuals demonstrated validity for walking and running using smartphone application Health for Android OS. 21 One explanation for this discrepancy may be associated with the relatively reduced walking speed of individuals after stroke, which is approximately half the rate of non-disabled individuals (1.4 m/s vs. 0.7 m/s). Indeed, faster speeds have been shown to have better accuracy using the Health application. 21
Consistent with this idea, a previous study, which investigated the validity of Health and Pacer in both smartphone systems (iOS and Android OS) in non-disabled individuals with a Smartphone (iphone and Samsung Galaxy S6 Edge) positioned in different locations (pant pocket on dominant and non-dominant side, bag transverse in shoulder and backpack) found that the smartphone application was not valid for slow speeds in any position (0.4 m/s). 25 However, Health for Android iOS was validated for non-disabled individuals for fast speeds and running. 26 In addition, Health for iOS was not found to be valid for any speed, fast or slow (0.7 m/s, 1.4 m/s, 2.8 m/s) with iphone on the left hand in non-disabled individuals. 27 Together, the Health application is not recommended for step counting in individuals after stroke, especially those who have a low walking speed. Although STEPZ presented lower values of correlation and ICC than other devices, this device presented fair to good magnitude of correlation with criterion-standard measure (live actual steps). In addition, the mean of the steps detected by STEPZ was similar to criterion-standard measure. These measurements are similar to the other devices, which presented mean differences ⩽ 11 steps. On the other hand, Health presented mean differences of 38 and 60 steps between Measure 1 and Measure 2, respectively. Thus, although STEPZ provide data statistically supported of validity and reliability, if a clinician or a researcher wants to choose a device, it is recommended to use Pacer (iphone), Fitbit Ultra, Google Fit, and Pacer (Android).
Here, we found that the location of the device (paretic or non-paretic side, at hip level) did not influence the step count. The literature reports that the smartphone application placed at the ankle or hip of the non-paretic side during walking did not influence the step count in individuals after chronic stroke during the 6-minute walk test, ramps, or stairs. 28 When the smartphone application was positioned on the non-dominant hand and right pocket, there were no significant differences in step count, regardless of placement, in a study with non-disabled individuals. 21 Thus, the individual should position the device on the most convenient side.
The results of this study have important clinical implications. It is well known that limiting sedentary time is associated with a lower risk of cardiovascular events and mortality. 29 Free and easy-to-use tools/strategies to improve physical activity levels are necessary, since these devices are used on a daily-basis without the need for specialized training or calibration. The literature reports that mHealth technology can improve outcomes such as adherence to medical therapy, awareness of diet and exercise, and ability to reach exercise goals. 30 Therefore, the use of valid and reliable smartphone applications should be implemented during the rehabilitation epoch, in order to set goals for these individuals, follow their results, and promote healthy competition between participants to enhance motivation and adherence to treatment.
Here, the number of smartphone applications was small when compared with what is commercially available. Individuals were evaluated in a laboratory setting, on a flat and standardized surface, and only individuals who were in the chronic stage after stroke, and able to walk without assistive devices were included. Also, we investigated the measurement properties during short distances, what does not reflect long distances on the community. As such, the results of this study should not be generalized beyond those individuals with the same characteristics, or other population. Also, it is important to notice that the sample size was not large enough to extrapolate the data to the entire stroke population.
Our results indicate that mHealth devices (Pacer–iphone, Fitbit Ultra, Google Fit, and Pacer–Android) provide a valid and reliable measure of step count in chronic stroke survivors. Placement of the device on the body (paretic or non-paretic hip) does not appear to affect the measure of step count.
Clinical messages
Pacer (iphone), Fitbit Ultra, Google Fit, and Pacer (Android) are valid for step counting.
Pacer (iphone), Fitbit Ultra, Google Fit, and Pacer (Android) are reliable for step counting.
The location of the smartphone (paretic or non-paretic front pocket) does not influence the accuracy of the step count.
Supplemental Material
Supplemental_Material – Supplemental material for An investigation into the validity and reliability of mHealth devices for counting steps in chronic stroke survivors
Supplemental material, Supplemental_Material for An investigation into the validity and reliability of mHealth devices for counting steps in chronic stroke survivors by Pollyana Helena Vieira Costa, Thainá Paula Dias de Jesus, Carolee Winstein, Camila Torriani-Pasin and Janaine Cunha Polese in Clinical Rehabilitation
Footnotes
Author contributions
J.C.P. conceived the original idea. P.H.V.C. and T.P.D.J. carried out the recruitment process and the tests. C.T.P. and J.C.P. were involved in planning, writing, and supervising the work. C.J.W. provided editorial assistance and scientific oversight for the manuscript. All authors discussed the results and contributed to the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support for this study was given by FAPEMIG (Fundação de Amparo a Pesquisa de Minas Gerais) and FAPESP (Fundação de Amparo à Pesquisa do Estado de São Paulo).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.