
Abstract
Objectives:
The aim of this study was to investigate the effects of inspiratory muscle training in post-stroke patients and to explore the effective training protocol.
Data sources:
PubMed/Medline, Web of Science, Scopus, Embase, Cochrane database, China National Knowledge Infrastructure, and China Science Periodical Database were searched through April 2020.
Review methods:
Trials examining effects of inspiratory muscle training on pulmonary function, cardiopulmonary endurance, pulmonary infection incidence, and quality of life in post-stroke patients were included. Subgroup analysis was performed to compare different training programs. Mean differences and risk ratios with 95% confidence intervals were presented. Risk of bias was assessed with the Cochrane tool.
Results:
Thirteen randomized controlled trials involving a total of 373 participants were identified. Meta-analysis conducted in 8 out of 13 trials revealed evidence for beneficial effects of inspiratory muscle training on forced vital capacity (MD: 0.47, 95% CI: 0.28–0.66), forced expired volume in 1 second (MD: 0.26, 95% CI: 0.18–0.35), 6-minute walk test (MD: 52.61, 95% CI: 25.22–80.01), maximum inspiratory pressure (MD: 18.18, 95% CI: 5.58–30.78), inspiratory muscle endurance (MD: 19.99, 95% CI: 13.58–26.40), and pulmonary infection incidence (RR: 0.11, 95% CI: 0.03–0.40). Omitting individual trials from the meta-analysis did not significantly change the results. The effective inspiratory muscle training protocol was suggested by subgroup analysis with three repetitions per week and more than 20 minutes per day for three weeks.
Conclusion:
Inspiratory muscle training can be considered as an effective intervention for improving pulmonary function and cardiopulmonary endurance, and reducing pulmonary infection incidence in patients after stroke.
Keywords
Introduction
Pulmonary function is essential to cardiopulmonary endurance and activities of daily living in post-stroke patients.1,2 Post-stroke patients are more likely to suffer from impaired pulmonary function due to long-term hospitalization–induced pulmonary infection. 3 Therefore, it is necessary to provide post-stroke patients with effective pulmonary rehabilitation in their subacute period.
It is known that inspiratory muscle strength in people after stroke is less than half of that expected in healthy adults.4,5 One of the key disciplines in stroke rehabilitation is inspiratory muscle training which is primarily aimed at restoring and maintaining pulmonary function. 6 Specifically, inspiratory muscle training improves pulmonary function by imposing a resistance to the inspiratory muscles and it may have an additional effect on respiratory muscle endurance which could translate into a more efficient use of the respiratory muscles in activities of daily living. 7
Several meta-analyses and systemic reviews have summarized interventions on pulmonary function. A recent umbrella review on five trials indicated that inspiratory muscle training can be expected to increase respiratory muscle strength and reduce the risk of respiratory complications in post-stroke patients. 8 The authors documented significant changes of maximal inspiratory pressure after inspiratory muscle training. Nonetheless, a Cochrane review concluded that there is insufficient evidence to support inspiratory muscle training as an effective intervention to improve pulmonary function after stroke. 6 Unfortunately, this Cochrane review had drawn the conclusion only based on two randomized controlled trials of 66 patients and did not examine the effects on respiratory endurance, the carryover effects to activity, or the incidence of respiratory complications. Based on these results, an updated meta-analysis of the current evidence is warranted.
In the current study, it was expected to make a comprehensive systematic review and meta-analysis, linking inspiratory muscle training specifically to the pulmonary function (e.g. forced vital capacity and forced expired volume in 1 second), pulmonary infection incidence, respiratory muscle strength, activities of daily living, and quality of life. The effectiveness of different training programs was also investigated with subgroup analysis.
Methods
We adopted the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) framework for reporting systematic reviews and meta-analyses to structure this review. 9 The following electronic databases were searched from their inception through April 2020: PubMed/Medline, Web of Science, Scopus, Embase, Cochrane database, China National Knowledge Infrastructure, and China Science Periodical Database. The detailed searching strategy is demonstrated in Online Appendix 1.
For the inclusion criteria, studies investigating the effectiveness of inspiratory muscle training in patients after stroke were included regardless of their design and publication language. Regarding outcome measurements, studies were included if they assessed at least one of the following clinician- or patient-oriented primary outcomes: (1) pulmonary function, presented as absolute or predictive forced vital capacity, forced expired volume in 1 second, and maximum inspiratory pressure, assessed by validated measures such as spirometry; (2) cardiopulmonary endurance, reflected as results of standardized tests such as the 6-minute walk test; (3) pulmonary infection incidence, operationalized as absolute values or percentages; (4) chest expansion, assessed by manual physical examination; (5) diaphragm thickness, operationalized as absolute values or proportions, assessed by ultrasound scanning; and (6) quality of life, assessed by validated disease-specific instruments.
Two reviewers (Y.D. and L.W.) independently read all eligible articles and cross-checked the information. For conflicting evaluations, the third senior author (X.L.) was consulted to solve the dispute and a final decision was made by the majority of the votes. The additional information was required and obtained from the corresponding author of the primary study if necessary.
Two authors (X.T.Z and Y.Z.) independently extracted data on demographics (e.g. age, gender, ethnicity, post-stroke duration), methodology (e.g. randomization, allocation concealment), experimental interventions (e.g. frequency, duration), control interventions (e.g. type, frequency, duration), outcomes (e.g. outcome measures, assessment time points), and results using an a priori developed data extraction form.
We used the Cochrane tool of bias to perform quality assessment in all the enrolled studies. 10 Aspects of random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessments, incomplete outcome data, selective reporting, and other biases were evaluated. Each criterion is rated as either low, unclear, or high risk of bias. 11 Two authors (X.T.Z and Y.Z.) were required to complete the assessments independently. If any disagreement persisted, the third senior author (X.L.) was consulted and discussed to reach a consensus.
The Review Manager software (RevMan Version 5.3; The Nordic Cochrane Centre, Copenhagen) was used to perform the meta-analysis if at least two studies assessed a specific outcome with a similar instrument. Statistical heterogeneity of included trials was evaluated with the chi-square test and I2 statistic. 12 The statistic was categorized as (1) I2 = 0%–24%: low heterogeneity; (2) I2 = 25%–49%: moderate heterogeneity; (3) I2 = 50%–74%: substantial heterogeneity; and (4) I2 = 75%–100%: considerable heterogeneity. As we expected to generate substantial statistical heterogeneity, analyses were performed with the random- or fixed-effects model according to the specific heterogeneity.
Variables including pulmonary function and cardiopulmonary endurance were analyzed for their positive mean difference with 95% confidence intervals indicating the beneficial effects of inspiratory muscle training as compared to the control interventions, whereas pulmonary infection incidence where we defined a negative risk ratios indicating beneficial effects (lower pulmonary infection incidence).
The influence of different post-stroke durations (<6 months vs >6 months) and different inspiratory muscle training protocols (duration of <4 weeks vs >4 weeks, frequency of <3 times per week vs >3 times per week, and <20 minutes each time vs 20–30 minutes each time vs >30 minutes each time) was assessed with subgroup analysis. To test the robustness of significant results, we conducted sensitivity analyses in all primary outcomes by omitting one study at each time to assess the influence of individual studies.
Results
Following PRISMA guidelines, Figure 1 summarizes the process of identifying eligible studies. 9 Thirteen enrolled trials randomized a total number of 373 patients either into the experimental group (n = 189) or the control group (n = 184).4,13–24 Inspiratory muscle training without co-interventions was applied in all the experimental arms. Of all the included control arms, six trials purely adopted conventional stroke rehabilitation program13–18 regardless of its frequency or duration,13,17–21 whereas other seven trials applied co-intervention program including self-selected intensity aerobic exercise, instrument-assisted exercises, or abdominal strengthening and breathing exercises.4,19–24 Table 1 presents the characteristics of the included trials, and Figure S1 demonstrates the risk of bias.
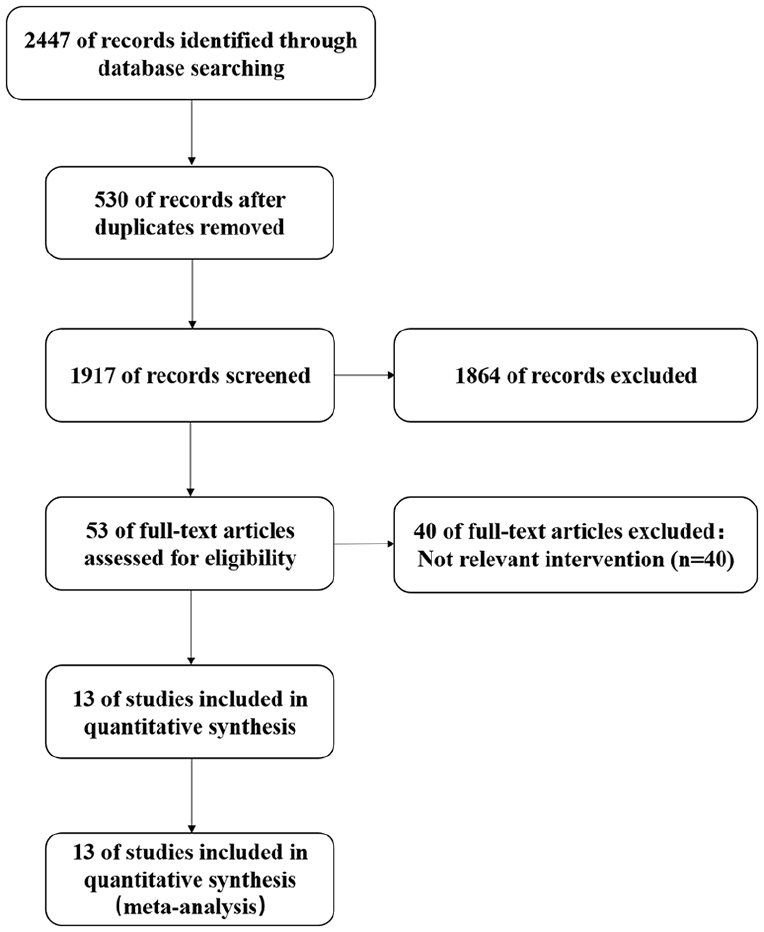
Flowchart of study selection.
Characteristics of included studies.
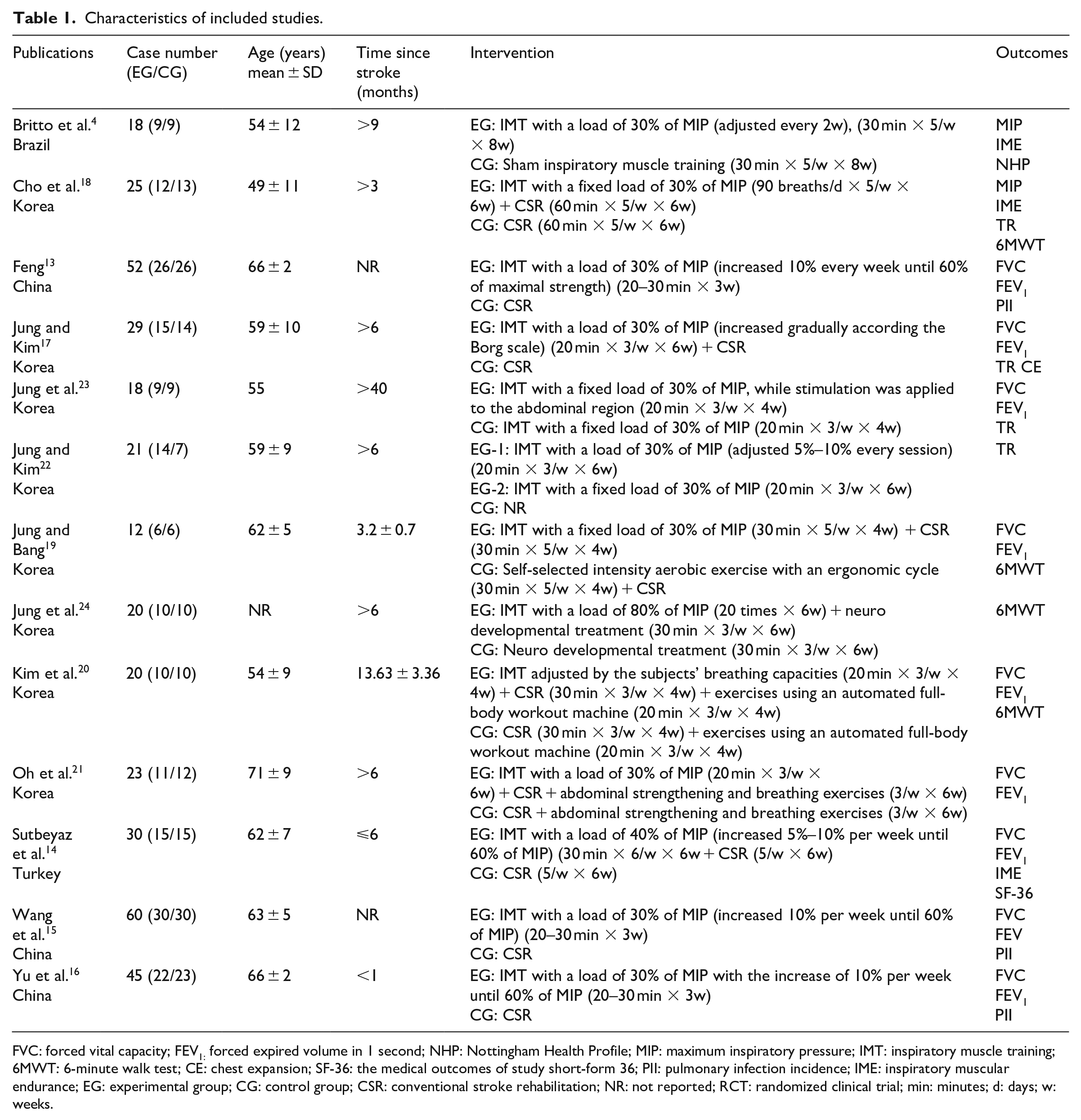
FVC: forced vital capacity; FEV1: forced expired volume in 1 second; NHP: Nottingham Health Profile; MIP: maximum inspiratory pressure; IMT: inspiratory muscle training; 6MWT: 6-minute walk test; CE: chest expansion; SF-36: the medical outcomes of study short-form 36; PII: pulmonary infection incidence; IME: inspiratory muscular endurance; EG: experimental group; CG: control group; CSR: conventional stroke rehabilitation; NR: not reported; RCT: randomized clinical trial; min: minutes; d: days; w: weeks.
Heterogeneity was found to be low for the overall inspiratory muscle endurance therefore a fixed-effects model was applied, whereas random-effects models were applied for the other outcomes and subgroup analysis. The effects of inspiratory muscle training on clinician-oriented outcomes were assessed by pooling data from eight of the included randomized controlled trials. As compared to the control interventions, beneficial effects of inspiratory muscle training were found on pulmonary function, pulmonary infection incidence, 6-minute walk test, maximum inspiratory pressure, inspiratory muscle endurance, and diaphragm thickening ratio at the paretic side, but not for diaphragm thickening ratio at the non-paretic side (Figure 2). In the sensitivity analyses of the above outcomes, omitting individual trials from the meta-analysis did not significantly change the mean differences.
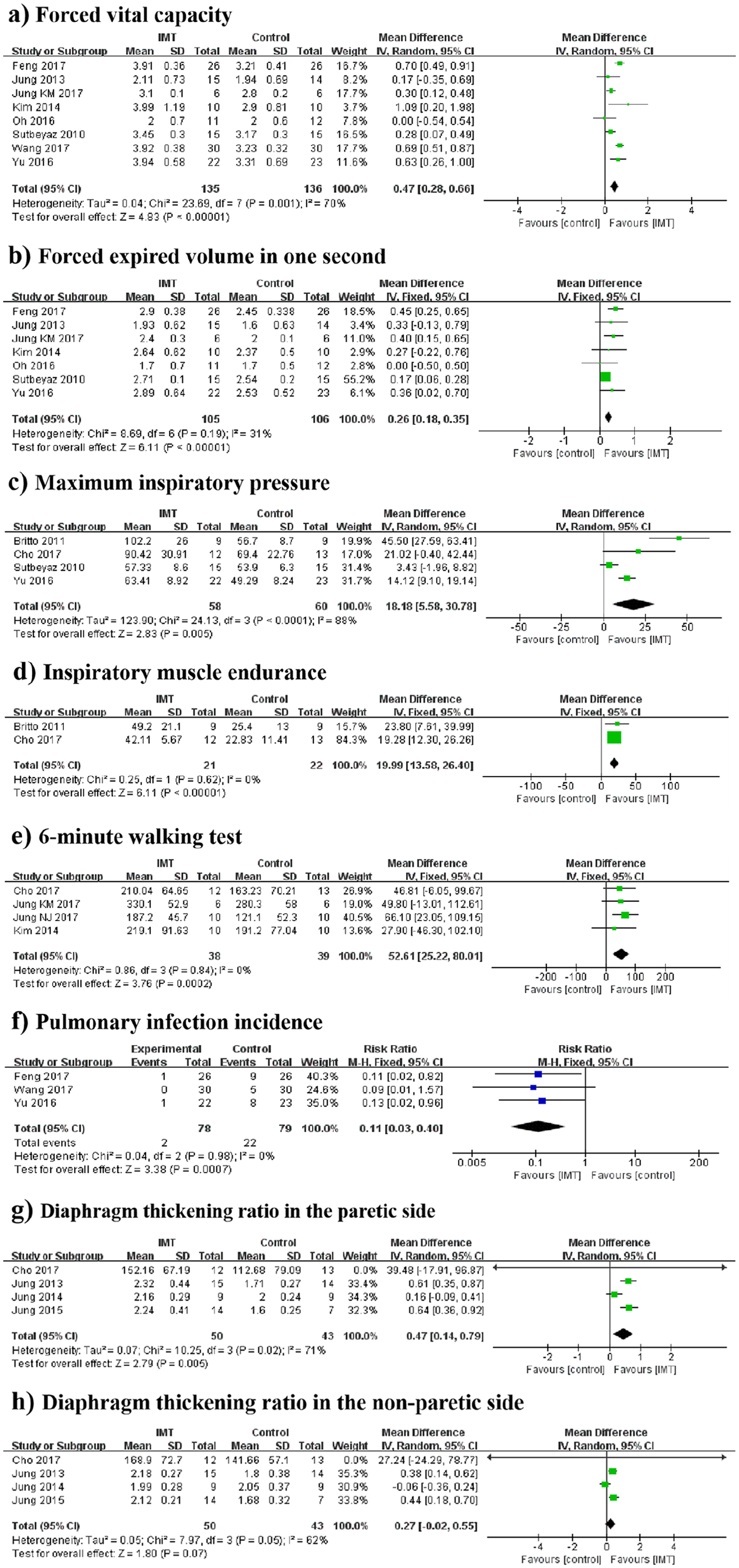
Meta-analysis of the effects of IMT versus control interventions.
Trials with different criteria for patient enrollment were performed with three applying “post-stroke duration less than 6 months” and three using “post-stroke duration more than 6 months.” Another two trials were excluded from this analysis due to the absence of information on post-stroke duration.13,15 The results showed that patients with post-stroke duration less than 6 months achieved significant improvement of forced vital capacity and forced expired volume in 1 second (Figure S2). Another subgroup analysis was done according to the training protocol. The effective training protocol was suggested with three repetitions per week and more than 20 minutes per day for three weeks (Figure 3; see also Figure S3).
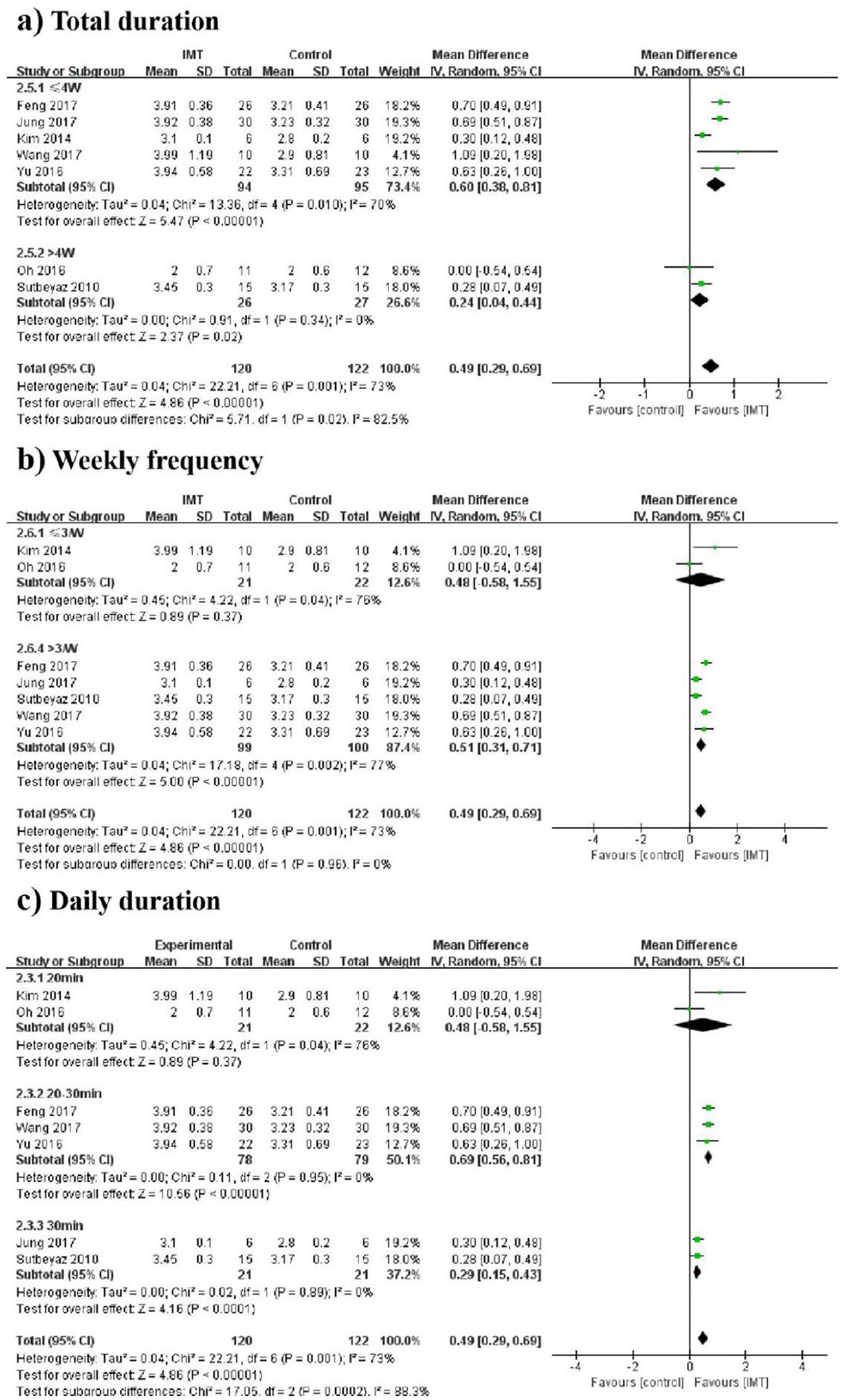
Subgroup meta-analysis of IMT versus control interventions on forced vital capacity by total duration, weekly frequency, and daily duration of intervention.
Only 1 out of the 13 studies reported chest expansion. Significant increase was detected neither in the inter-group nor in the intra-group comparison. 17 Another two studies investigated the effects of inspiratory muscle training on quality of life (patient-oriented outcome); however, one used the 36-Item Short Form Survey (SF-36) and the other used the Brazilian version of the Nottingham Health Profile.4,14 Due to different scales adopted in these two studies, a meta-analysis was impossible to be performed. Nonetheless, both studies reported consistent results that no statistically significant differences were observed between the inspiratory muscle training group and the control group for quality of life.
Discussion
In this systematic review and meta-analysis of 13 randomized controlled trials on inspiratory muscle training in patients after stroke, the quality of the trials varied from medium to low according to the Cochrane criteria. We found evidence for beneficial effects of inspiratory muscle training on pulmonary function, cardiopulmonary endurance, and pulmonary infection incidence. Patients with the post-stroke duration less than 6 months benefitted more from inspiratory muscle training. A preliminary evidence-based training protocol was also suggested based on the results of subgroup analysis.
In comparison with one of the previously published meta-analyses 25 and three systematic reviews,6,8,26 our updated study mainly focused on the inspiratory muscle training instead of respiratory muscle training. As compared to the expiratory muscle strength, weaker inspiratory muscle strength was observed in post-stroke 27 patients. This is not due to the discrepancy in the intrinsic loss of peripheral muscle function but due to the impaired cortical motor controlling of the inspiratory muscle strength, which leads to decreased pulmonary function. 27 Apart from that, inspiratory muscle weakness leads to a reduced lung volume at the beginning of a cough and may underlie significant impairments of cough which in turn increases the pulmonary infection incidence. However, inspiratory muscle training can promote diaphragm hypertrophy and increase the proportion of type I fibers and the size of the type II fibers of the external intercostal muscles. 28 Therefore, the specific inspiratory muscle training is assumed to achieve more benefits on the recovery of pulmonary function, cardiopulmonary endurance, and pulmonary infection incidence. Moreover, no meta-analysis suggested the effective inspiratory muscle training protocol.
Generally, our results are in line with previous meta-analysis and systematic reviews to some extent. At the first glance, inspiratory muscle training seems to be effective in enhancing the pulmonary function. At a closer look, however, all of the previous studies focused on the improvement of respiratory muscle strength after inspiratory muscle training or respiratory muscle training.6,8,25,26 One of the systematic reviews concluded that inspiratory muscle training can improve strength and endurance of respiratory muscle strength with the enrollment of two randomized controlled trials, one pilot study, and three cross-sectional studies. 26 The Cochrane review conducted by Xiao et al. 6 also documented that inspiratory muscle training was associated with a significant increase in maximum inspiratory pressure when compared with the sham inspiratory muscle training group. Due to the enrollment of two small heterogeneous randomized controlled trials, there was insufficient evidence from which to make any generalized conclusions about the effects of inspiratory muscle training.
Our study investigated the variation of forced vital capacity and forced expired volume in 1 second since they can be linked to the variation of pulmonary function and the effectiveness of training. While the current meta-analysis concluded that inspiratory muscle training is effective in increasing forced vital capacity and forced expired volume in 1 second by different training protocols, subgroup analysis in the current study identified the effective inspiratory muscle training protocol including a total duration of three weeks, more than three repetitions per week, and more than 20 minutes per day. Although systematic reviews may suggest the effective protocol (i.e. 8 weeks intervention with a frequency of 3–6 days per week, 15–30 minutes per day with one or two daily sessions) with objective measures, 26 to the best of our knowledge, the subgroup meta-analysis of training protocol had not been conducted, while an evidence-based training protocol can be documented as reference in future studies for further data integration.
Moreover, the pooled data suggested that inspiratory muscle training is only effective in patients with post-stroke duration of less than 6 months. This meets the conclusion of one systematic review conducted by Lynch et al., 29 where the results favored earlier transfer to rehabilitation services for the improvement of post-stroke function.
While recent preliminary clinical studies have indicated that inspiratory muscle training might have the potential to improve pulmonary functions and cardiopulmonary endurance, and decrease pulmonary infection incidence, we do reach the same conclusion here. Previous studies have detected increased diaphragm thickness asymmetry in patients after stroke, leading to asymmetric contraction of the diaphragm and impaired pulmonary function.14,30 Our pooled results also presented that diaphragm thickening ratio in the paretic side was significantly increased by inspiratory muscle training, while changes were not observed at the non-paretic side. This also verified the effects of inspiratory muscle training on improving the diaphragm thickness asymmetry ratio.
Furthermore, inspiratory muscle training was unable to significantly change the chest expansion and quality of life as compared to the control interventions. As the expansion of the chest is mainly due to the descending of the diaphragm, interventions (i.e. implanted electrical stimulator) directly improving the function of diaphragm may be more effective than inspiratory muscle training. In terms of quality of life, it is supposed that inspiratory muscle training mainly focuses on the physical function instead of the mental health.
We are aware that a meta-analysis may have several limitations. Currently, this meta-analysis only included 13 randomized controlled trials. This is due to the real status that there is a limited number of high-quality trials conducted in this research field. At the database searching stage, relevant studies can be missed due to language restriction although Chinese literature databases have been comprehensively screened. Nonetheless, because of its value in routine clinical practice, the mild heterogeneity and good robustness allowed us to carry out pooling analyses and making specific conclusions of inspiratory muscle training on the recovery of post-stroke patients. Furthermore, disease duration since stroke, training load, and intervention duration were different in individual trials, all of which would have essential impacts on outcome measures. Therefore, caution should be taken that the effective training protocol was suggested based on the results of forced vital capacity and forced expired volume in 1 second, in other words it was only effective on pulmonary function. In terms of quality assessment, only half of the trials were blinded with outcome assessment. Assigning blinded coordinators for outcome assessment would be helpful to reduce risk of detection bias.
In conclusion, our findings revealed the beneficial effects of inspiratory muscle training on several clinical outcomes such as pulmonary function, cardiopulmonary endurance, and pulmonary infection incidence. However, it is believed that even if one meta-analysis strictly adhered to relevant guidelines for undertaking reviews, it might not be considered to be as convincing as a large randomized trial. Therefore, high-quality, large-scale randomized trials are warranted to verify its effectiveness to guide clinical practice.
Clinical messages
Inspiratory muscle training can be an effective intervention in post-stroke patients, particularly on the pulmonary function, cardiopulmonary endurance, and pulmonary infection incidence.
The suggested inspiratory muscle training protocol consisted of a training duration of >20 minutes/day and >3 repetitions/week for three weeks.
There are insufficient large trials at present to make firm recommendations.
Supplemental Material
Supplementary_Material – Supplemental material for Can inspiratory muscle training benefit patients after stroke? A systematic review and meta-analysis of randomized controlled trials
Supplemental material, Supplementary_Material for Can inspiratory muscle training benefit patients after stroke? A systematic review and meta-analysis of randomized controlled trials by Xintong Zhang, Yu Zheng, Yini Dang, Lu Wang, Yihui Cheng, Xiu Zhang, Mao Mao and Xiao Lu in Clinical Rehabilitation
Footnotes
Authors’ contribution
X.L. was responsible for conception and design of the study. X.T.Z., Y.Z., Y.D., L.W., Y.C., X.Z., and M.M. were responsible for trial screening, data extraction, and data analysis. X.T.Z. and Y.Z. drafted the manuscript. All authors gave final approval of the version to be published and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Key Research and Development Project of China (Project No. 2017YFB1303203).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.