
Abstract
Objective:
To evaluate the efficacy of a newly developed evidence-based low back pain (LBP) management smartphone application.
Design:
A double-blinded randomized controlled trial where participants randomly assigned to either an experimental group (EG) or a control group (CG).
Setting:
Governmental and private institutions.
Participants:
About 40 office workers, aged 30 to 55 years, had pain due to non-specific LBP > 3 on Visual Analogue Scale, and with pain chronicity > 3 months.
Interventions:
The EG received full version of the application ‘Relieve my back’ included evidence-based instructions and therapeutic exercises for LBP management, whereas the CG received placebo version included instructions about nutrition.
Main measures:
Primary outcome measures included pain measured by Visual Analogue Scale (VAS), disability measured by Oswestry Disability Index (ODI), and quality of life measured by Short-Form Health Survey (SF-12).
Results:
Following six weeks of using the application, compared to CG, the EG group demonstrated significant decrease in pain intensity (−3.45 (2.21) vs −0.11 (1.66), P < 0.001), in ODI score (−11.05 (10.40) vs −0.58 (9.0), P = 0.002), and significant increase in physical component of SF-12 (12.85 (17.20) vs −4.63 (12.04), P = 0.001).
Conclusion:
‘Relieve my back’ application might be efficacious in reducing pain and disability and improving the quality of life of office workers with non-specific LBP.
Introduction
Low back pain is the most prevalent work-related musculoskeletal disorder among office workers and one of the leading causes of disability. 1 It has maladaptive effects on psychological symptoms, sleep quality, and quality of life.2,3 In about 85% to 95% of low back pain cases, no specific pathology was identified as the cause of low back pain which is referred to as a non-specific low back pain.4,5 Low back pain classified as chronic when symptoms persist for more than 12 weeks. 6
Currently available self-management options for chronic non-specific low back pain need considerable improvements. 7 Educating the patients, proper ergonomics and postures and proper body lifting were found to be effective in reducing chronic low back pain and disability and improving quality of life alongside general strengthening and stretching exercises. 8 Home exercise programme showed to be effective in treatment of chronic low back pain, but there was low adherence to and improper application of exercises.6,9 All of these are available in numerous smartphone applications educating patients for self-management of low back pain. However, these applications were not developed by professionals, not based on scientific evidence, and/or their effectiveness was not established. 10
We developed an evidence-based smartphone application ‘Relieve my back’ targeting office workers with non-specific low back pain. The objective of this study was to evaluate the application’s efficacy in improving participants’ pain, disability, mental health symptoms, physical activity, quality of life and sleep quality. We hypothesized that following six weeks of using the full version of ‘Relieve my back’ application, office workers will demonstrate significantly less pain, disability and mental health symptoms as well as higher levels of quality of life, physical activity and sleep quality compared to those used the placebo version.
Creating a low back pain tailored smartphone application that is possibly effective, cost-effective, compatible with the modern lifestyle, easy to use and accessible at any time might help to reduce low back pain burden on patients and medical facilities.
Material and methods
This is a randomized controlled trial that was registered at the US National Institutes of Health (ClinicalTrials.gov) #NCT03994458. The study was conducted between January and August, 2019, and was funded (Grant #20180429) by Jordan University of Science and Technology (Irbid, Jordan). All of the study procedures and forms were approved by the Institutional Review Board at Jordan University of Science and Technology, Irbid, Jordan (approval #: 86/117/2018).
The study was conducted at participants’ workplaces (offices) and in the laboratories of Jordan University of Science and Technology. Principal researcher randomized participants (withdrawal of a card out of 10 without substitution and repeated the process for each new 10 participants) into either an experimental group who received the full version of the smartphone application or a control group who received a placebo application. The inclusion criteria for the study included being an office worker for at least five years with at least five hours of desk working a day. Participants’ needed to be between 30 and 55 years old (to avoid college-life and aging effects), have self-reported complaints of low back pain for at least three months, a minimum pain score of three points on a 0 to 10 Visual Analogue Scale, and using a smartphone with an Android operating system (since the application was programmed for android devices only). The exclusion criteria included pregnancy at screening time, a documented diagnosis of specific pathology related to low back pain including disc herniation with radiculopathy, structural deformities such as scoliosis, kyphosis or lordosis, spinal tumour, ankylosing spondylitis or spondylolisthesis, spine surgery or significant trauma in the past six months.
Study flyers were sent to many governmental and private institutions hiring office workers in Irbid and Amman (the biggest Jordanian cities). Furthermore, these flyers were posted on social media applications. Phone calls were used to screen eligible participants. Office workers who fully met the study criteria were assigned for a meeting with the research coordinator for signing consent forms and the blinded evaluators for baseline assessments. The principal researcher randomly assigned eligible office workers into an experimental group or control group. Then the link for downloading ‘Relieve my back’ was sent to participants with an invitation code specific to each study group. The project programmer oversaw the application downloads making sure that each participant is adherent to his/her designated version without any contamination. Participants were asked to use the application for six weeks. Participants and evaluators were blinded to participants’ assignments (full or placebo version). After finishing the six weeks of using the application, participants were reassessed (follow-up) by the same evaluator. All evaluators received the same training delivered by the study principal investigator to increase inter-rater reliability.
Except for demographics (collected at baseline only), the following assessments were conducted at baseline and follow-up after six weeks of having the interventions.
Basic demographics of participants were collected along with lifestyle characteristics including age, gender, marital status, smoking habits, average hours of driving, computer use, mobile phone use, office work hours per day and the number of working days per week.
Pain intensity during the day of assessment measured using the Visual Analogue Scale. The measure is scored from no-pain (score 0) to the most intense pain (score 10). 11 The scale was used among Arabic speaking populations and showed good psychometrics.12,13 A change of two scores in chronic low back pain is considered a clinically significant change. 14
The Oswestry Disability Index was used to assess the disability caused by low back pain. 15 The measure score range from 0 to100, where a higher score indicates a higher disability. When using ODI, at least 10 points change is considered clinically significant.14,16,17 The Arabic version of the questionnaire showed to be valid and reliable. 18
The 12-item Short-Form Health Survey was used for measuring health-related quality of life. The measure score ranges between 0 and 100 and includes physical component summary and mental component summary scores and was validated in Arabic language.19,20 A change of 3.29 and 3.77 units is considered clinically significant for physical and mental component summary scores, respectively. 21 The Arabic validated Depression Anxiety Stress Scale was used to assess mental health symptoms over the last week.22,23 The test score ranges between 0 and 21 points for each subscale where a higher score indicates a higher level of mental health symptoms. The cut-off points score is nine for depression, seven for anxiety and 14 for stress, with higher scores indicating severe symptoms. 24
Sleep quality over the previous month was assessed using the Arabic validated Pittsburgh Sleep Quality Index.25,26 The measure has a global score ranging from 0 to 21, with a higher score demonstrating worse sleep quality. 27 A total score of the measure of five or more reflected poor sleep quality. 28
Physical activity level was measured using the International Physical Activity Questionnaire. 29 The measure result is categorized into three categories according to the metabolic equivalent of task: low or trace physical activity (below 600 minute/week), moderate physical activity (600–1500 minute/week) and high physical activity (at least 3000 minute/week).30,31 The minimal detectable change for the measure was reported to range between 103 and 123 metabolic equivalent of task. 32
‘Google Play’ firebase logs (i.e. statistics of users) of the two application versions were collected to provide an objective measure of participants’ average use of the applications. These times only represent the time during which the application was active and does not represent the actual exercises practice time.
This study intervention consisted of using a smartphone application ‘Relieve my back’ for six weeks. This application had two versions (experimental and placebo) and was designed by an expert android programmer and the research team. The main screen of the two versions was similar and divided into three subunits: advice, at the office and home.
The experimental version included general advice and instruction, office-based stretching exercises and home-based strengthening exercises for lower back and abdominal muscles (full details in Supplemental Appendix 1). Furthermore, the full version had four phone notifications (sound and vibration along with instruction pop-up screen) through the day to notify the participants to take a walk break, a reminder of the right posture, a reminder of the stretching exercises and a reminder of the home-based exercises in the evening.
The placebo version only included posts of general nutrition advice in the first section along with four notifications (sound and vibration along with instruction pop-up screen) containing nutritional facts that would pop up through the day and were not related to low back pain management. Participants in both groups were allowed to continue their traditional medical care and control group participants were offered access to the full-version application at the end of the study. More details about the application is provided in Supplemental Appendix 1.
Based on the pilot study (n = 4), the mean change score for the Visual Analogue Scale was −3.5 (±2.12) with an effect size of 1.65. A priori sample size using GPower 3.1 was calculated. A total sample size of 18 participants (nine in each group) was required as applied on one tale hypothesis testing to guarantee a statistical power of 0.80. 33 Considering dropping-out and the other used outcome measures, 40 participants were recruited.
All statistical analyses were conducted using SPSS 23.0 (SPSS, Inc., Chicago, IL, USA). Descriptive data were presented in means and standard deviations (SD), or frequencies and percentages. For effect sizes, Cohen’s d values of 0.8, 0.5 and 0.2 are considered large, medium and small effect sizes, respectively. 34 To test homogeneity of the groups, student’s t-tests (for continuous and normally distributed variables) and chi-square (for categorical variables) were used to compare baseline characteristics including demographics, Visual Analogue Scale, Oswestry Disability Index, SF-12, Depression Anxiety Stress Scale subscores, Pittsburgh Sleep Quality Index and International Physical Activity Questionnaire. A MANOVA test was conducted to investigate the between-groups difference in change scores for primary and secondary outcome measures. Assumptions of MANOVA test were met. Groups (experimental and control) were used as an independent variable, whereas Visual Analogue Scale, Oswestry Disability Index, SF-12 mental component, SF-12 physical component, Depression Anxiety Stress Scale subscores, Pittsburgh Sleep Quality Index and International Physical Activity Questionnaire were used as dependent variables. When the P-value for the MANOVA model between groups effect was <0.05, univariate analyses using independent Student’s t-tests for each of the outcome measures were allowed without correction for α. Statistical significance was set at P < 0.05 for all statistical analyses.
Results
Figure 1 demonstrates the flowchart of participants and Table 1 demonstrates participants’ baseline characteristics comparisons for evaluating groups’ homogeneity. A total of 67 office workers were screened for eligibility and only 41 participants met the study criteria or agreed to participate. Participants were assigned into experimental group (n = 21) and control group (n = 20). There was one drop out of each group during the study due to personal preferences and lack of interest to continue. There were no significant statistical differences observed in pre-intervention scores of outcome measures or baseline characteristics.
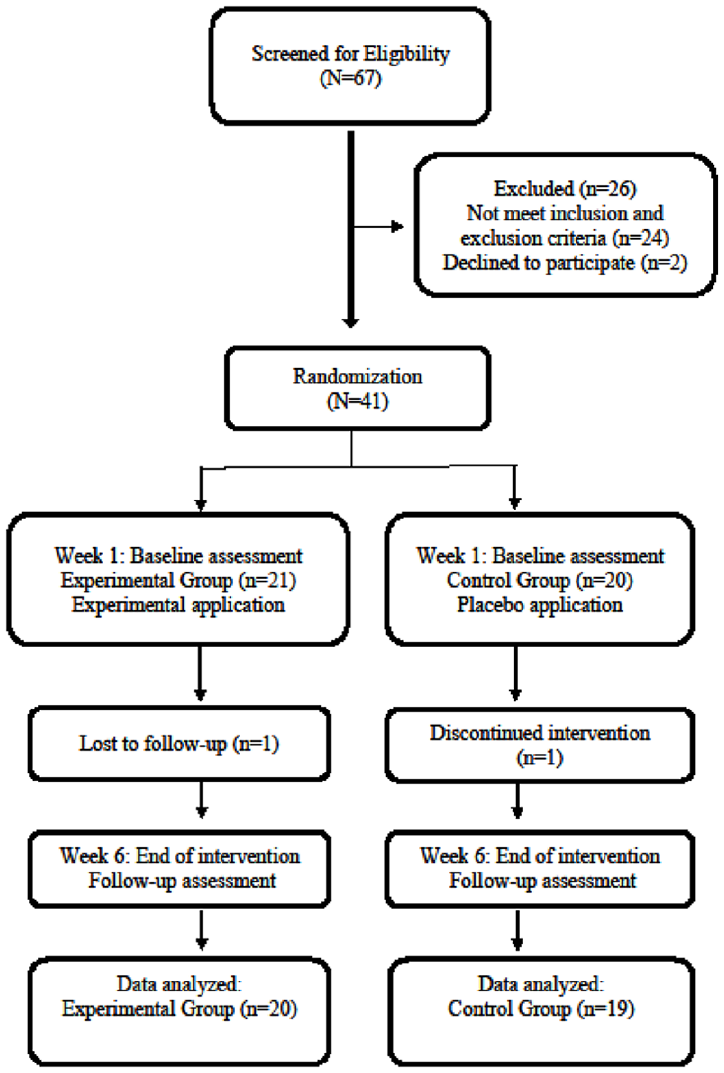
Flow of participants through the study.
Participant’s baseline characteristic.
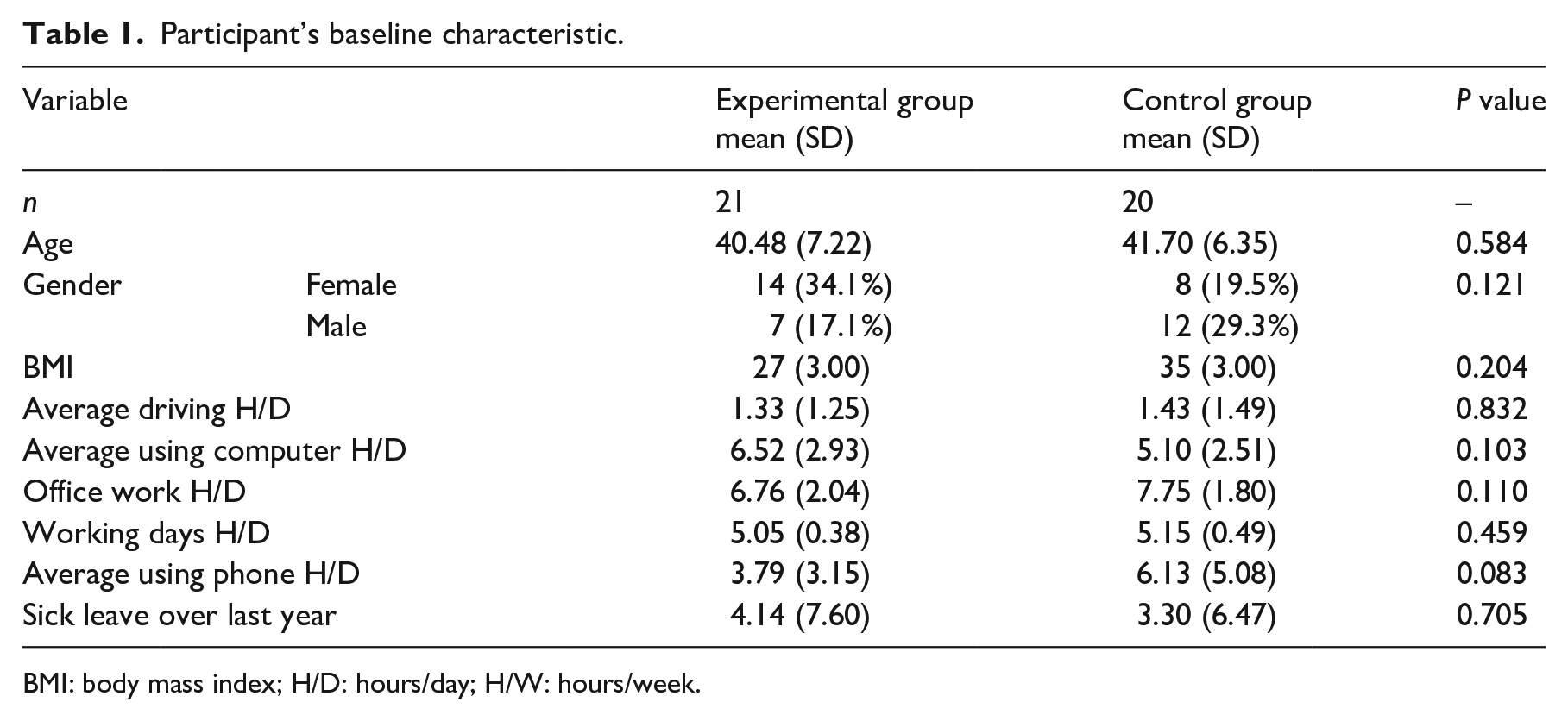
BMI: body mass index; H/D: hours/day; H/W: hours/week.
The overall MANOVA test showed statistically significant difference between experimental group and control group [Wilks’ Lambda = 0.388, F (11, 27) = 3.873, P = 0.002]. Therefore, a separate independent Student’s t-test was conducted for each of the outcome measures.
Table 2 demonstrates the baseline and follow-up outcome measures scores. Also, it demonstrates differences between groups change scores with effect sizes of these differences.
Between groups’ change scores univariate comparisons of and effect sizes for all outcome measures.
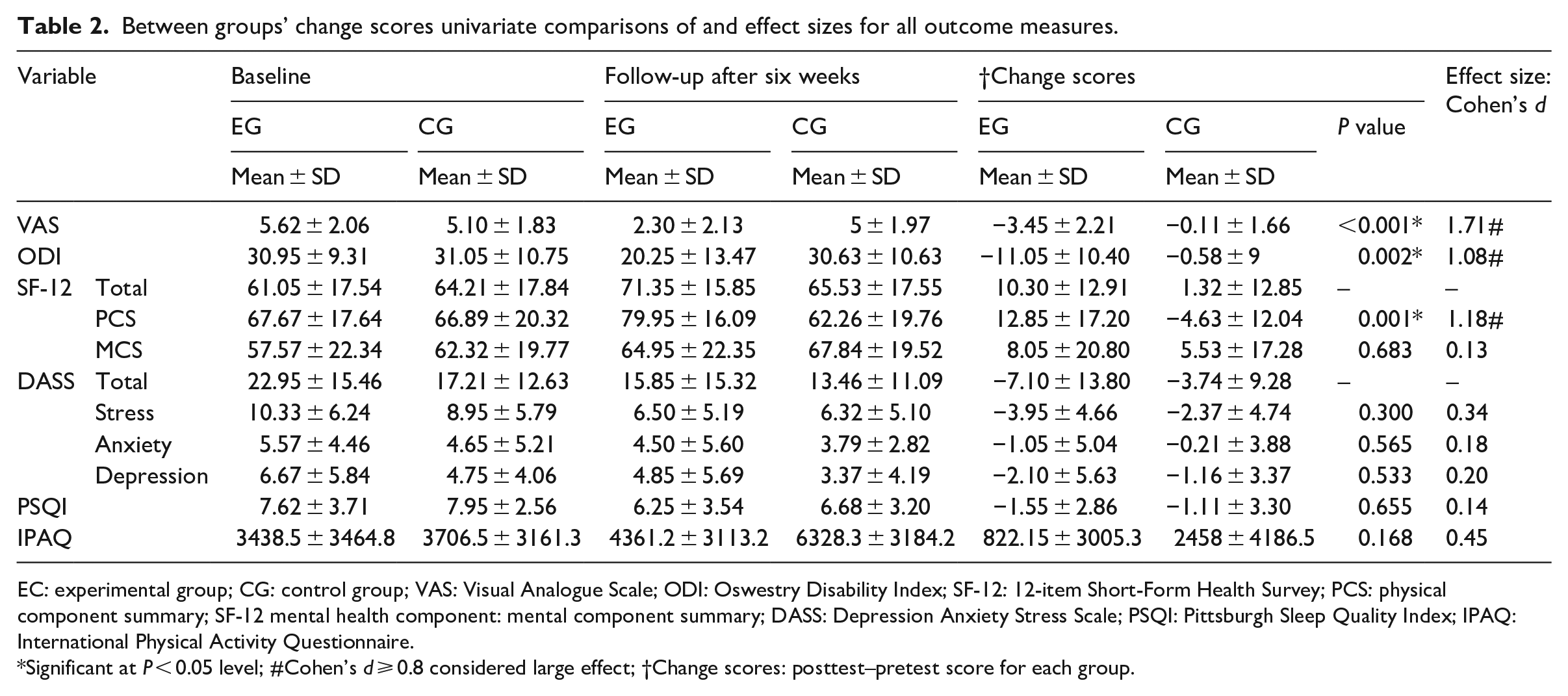
EC: experimental group; CG: control group; VAS: Visual Analogue Scale; ODI: Oswestry Disability Index; SF-12: 12-item Short-Form Health Survey; PCS: physical component summary; SF-12 mental health component: mental component summary; DASS: Depression Anxiety Stress Scale; PSQI: Pittsburgh Sleep Quality Index; IPAQ: International Physical Activity Questionnaire.
Significant at P < 0.05 level; #Cohen’s d ⩾ 0.8 considered large effect; †Change scores: posttest–pretest score for each group.
Pain mean change scores was significantly larger in the experimental group as compared to the control group (P < 0.001). Oswestry Disability Index mean change score was significantly larger in the experimental group compared to the control group score (P = 0.002). The experimental group SF-12 physical component summary mean change score was significantly larger than the control group (P = 0.001). On the other hand, the mental component summary mean change score was 2.52 units greater than the control group. However, this latter difference was not statistically or clinically significant. No significant differences between groups were found in the change scores of Depression Anxiety Stress Scale, Pittsburgh Sleep Quality Index and International Physical Activity Questionnaire.
Google firebase logs showed that the average daily use of the application (but not the exercise practice time) from the beginning to the end of the trial for experimental group was 6 minutes and 40 seconds, whereas control group daily usage of the application was 1 minute and 11 seconds.
Discussion
Using this newly developed evidence-based smartphone application, ‘Relieve my back’ showed potential evidence to decrease low back pain-related pain intensity and disability and to increase the health-related quality of life among office workers. However, this study failed to find significant improvements in mental health, sleep quality and physical activity level following six weeks of using the application.
This study results were clinically meaningful according to the published Minimal Clinically Importance Change for Visual Analogue Scale, Oswestry Disability Index and SF-12 physical component.14,16,21 Furthermore, this study improvements of pain, disability and health-related quality of life after using ‘Relieve my back’ were of large effect sizes (Cohen’s d > 0.8, as demonstrated in Table 2). 34 This supported the potential superiority of the experimental version of ‘Relieve my back’ over the placebo version in reducing non-specific low back pain and disability and improving health-related quality of life status among office workers who complain from non-specific low back pain.
The application ‘Relieve my back’ was designed based on the concepts of self-management in treating low back pain. This was done incorporating different home-based exercises and patients’ education in treating non-specific low back pain. We have used nutritional placebo to control for potential positive effects of using a therapeutic application or getting involved in research study. Nutritional placebo control was used in similar studies evaluated the effects of education and exercises in treating low back pain. 8 This study results showed a significant decrease in pain and disability which was consistent with previous studies used home-based exercises.35,36 Furthermore, Albaladejo et al., supported the effectiveness of using education along with strengthening exercises in reducing pain and disability in non-specific low back pain. 8 Previous studies, as concluded in one literature review, suggested that chronic pain (such as low back pain) may affect daily life activities and the quality of life of patients. 37 In this study, we found a significant improvement of SF-12 physical health component (12.85 units increase) gained through the use of this simple self-management application ‘Relieve my back’. Our results are much better than similar studies such as Albaladejo et al. who reported that treating low back pain using home-based exercises and education yielded in 2.9 units increase in SF-12 physical health component score. 8 Another study found that home-based exercises including trunk muscle strengthening and stretching exercises showed significant improvement in disability as measured by Roland–Morris Disability Question-naire (P = 0.021). 35 Another systematic review and meta-analysis showed that strengthening exercises and coordination stabilization exercises had more valuable effects compared to other low back pain treatment methods such as electrotherapies and manipulative therapies (P < 0.01). 36 These previous studies’ results are consistent with our study findings related to pain and disability. Strengthening exercises along with stretching exercises whether practiced home-based or clinic-based showed a general improvement in pain and disability in patients with low back pain.35,36
Noting that the SF-12 mental health component showed no significant difference between groups, the experimental group was perceptible and clinically meaningful as those increased more than 3.77 units. 21 The results related to the SF-12 mental health component might suggest that both application versions’ users had perceived the idea of using a smartphone application for their low back pain symptoms positively and appealing.
Smartphone applications are broadly available worldwide and it is estimated that there are about 325,000 health smartphone applications available in application stores. 38 Research articles speculated that these applications (in contrast with traditional educational methods) might provide a more personalized health promotion method that effectively enhances clients’ compliance, self-management and awareness of many health-challenging issues.39,40 However, the usability and effectiveness of the numerously available health promotion smartphone application should be always evaluated before recommending these applications for patients. 38
This study is unique as it created a health-promotion smartphone application tailored to patients with low back pain and evaluated its efficacy using a rigorous double-blinded randomized controlled trial design. The study provided a valuable and probably effective, self-management approach to treat low back pain which is considered one of the most prevalent and costly health conditions around the world.3,41,42
A potential limitation of this study is the lack of long-term follow-up. A long-term follow-up may evaluate the long-term maintenance of effects post-treatment. Additionally, low back pain duration was not collected in this study and consequently was not included in the analyses. This was small sample study that showed positive results, and larger sample sizes with higher statistical power might be more conclusive to evaluate improvement in mental health, sleep quality and physical activity. The placebo control might be not credible for the participants, therefore; testing the application against more comparable control conditions including other types of low back pain interventions is recommended. Future studies are also encouraged to evaluate ‘Relieve my back’ in a standardized way, for example, using Mobile Application Rating Scale, and the effects of such applications on the recurrence of low back pain. 43 The generalizability of these findings may be limited to non-specific low back pain and office workers. Other specific low back pain populations may need more individualized exercise and may respond differently to this application.
In conclusion, the use of evidence-based low back pain application ‘Relieve my back’ for treating non-specific low back pain appeared to be an innovative and might be an efficacious method to reduce pain and disability as well as improve health-related quality of life for office workers. The experimental group participants demonstrated significant and clinically meaningful improvements in pain, disability and health-related quality of life measured by the Visual Analogue Scale, Oswestry Disability Index and SF-12. Future studies with larger sample sizes and longer follow-up periods are needed.
Clinical messages
Providing office workers with non-specific chronic low back pain with a mobile application containing evidence-based exercises and proper body mechanics education for six weeks appeared beneficial in reducing their pain, disability and improving their quality of life.
Supplemental Material
Supplemental_Appendix_proofs – Supplemental material for Efficacy of an innovative smartphone application for office workers with chronic non-specific low back pain: a pilot randomized controlled trial
Supplemental material, Supplemental_Appendix_proofs for Efficacy of an innovative smartphone application for office workers with chronic non-specific low back pain: a pilot randomized controlled trial by Khader A Almhdawi, Donia Saleh Obeidat, Saddam F Kanaan, Alaa O Oteir, Zaid Modhi Mansour and Hassan Alrabbaei in Clinical Rehabilitation
Footnotes
Acknowledgements
The authors would like to thank the programmer Ahmad Almhdawi, and the evaluators Lamees Al-Khader and Nader Alabbasi.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was supported by Jordan University of Science and Technology (Grant #20180429) and European Union; this manuscript is the academic outcome of a master student who attended a programme funded project by the Erasmus+ Programme of the European Union entitled (Establishment of an interdisciplinary Clinical rehabilitation sciences master programme at JUST JUST-CRS; Project No: ‘573758-EPP-1-2016-1 JOEPPKA2-CBHE-JP’).
Clinical trial registration
This trial is registered at the US National Institutes of Health (ClinicalTrials.gov) #NCT03994458.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.