
Abstract
Objectives:
To compare the efficacy of extracorporeal shock wave therapy versus standard care (ultrasound + hot pack + self-stretch-exercises) in treatment of neck and upper back myofascial pain syndrome.
Design:
Single-blind randomised clinical trial
Setting:
Outpatients setting.
Subjects:
Patients with neck and upper back myofascial pain
Intervention:
Participants were randomly allocated into shock wave group (n = 24), standard care (ultrasound + hot pack + self-stretch-exercises) group (n = 24) and control (self-stretch-exercises) group (n = 24) for four weeks.
Main Measures:
The primary outcomes were pain intensity (visual analogue scale), pain pressure threshold (algometer) and disability (neck disability index). Measures were performed at baseline (week 0), week 1 and post-intervention (week 4).
Results:
Shock wave and ultrasound improved visual analogue scale (7.50 ± 1.71 to 5.72 ± 2.20 and 6.22 ± 2.54 to 4.95 ± 2.86, respectively, P = 0.083) and disability index (54.24 ± 15.53 to 39.04 ± 19.58 50.23 ± 19.57 to 32.10 ± 18.34, respectively, P = 0.495) similarly at first week examinations that were significantly higher than control (P < 0.05). In week 4 measurements, additional improvements were achieved concerning visual analogue scale and disability index in the shock wave (–4.00 ± 2.22 and –20.24 ± 16.56, respectively) and ultrasound (–2.18 ± 2.71 and –21.79 ± 10.56, respectively) groups. However, visual analogue scale improved more significantly in shock wave group than ultrasound group in fourth week measurements (P = 0.012).
Conclusion:
Extracorporeal shock wave therapy was more effective in controlling of the pain intensity compared to ultrasound one month after treatment. However it had no superiority over ultrasound in improving neck disability index at this time point.
Trial registration
www.irct.ir, IRCT201608154104N5, registered 2016-09-25
Introduction
Neck pain is a very common complaint in the general population with a prevalence of 30% to 50%,1,2 characterises one of the most common work related musculoskeletal conditions. 3 Around one tenth of these patients experience chronic neck/shoulder pain. 4 Myofascial pain syndrome is an important cause of pain in patients with chronic nonspecific neck pain, described by hyperirritable spots in taut muscle bands, leading to pain, loss of function and impaired range of motion. 5 Careers comprising longsome static postures or continuous upper limb activities, for example computer work, may result the occurrence of myofascial neck and upper back pain.6,7 At the same time, about 40% of subjects express inadequate efficacy in the handling of chronic pain syndrome. 8 The main purpose of myofascial pain syndrome treatment is to disruption of the pain cycle via the omission of trigger points. 9 There are several approaches for the elimination of the trigger points. Several practical guidelines focus on self-management and physiotherapy, and less underline the medication usage and surgical intervention; 10 however the most efficient treatment approach is still under argument. Numerous conventional treatments applied to assist in managing neck pain and comprise different forms of exercise, ultrasound and acupuncture among others, but there is not enough evidence concerning their comparative efficiency.11,12
Education in self-management qualifies individuals with musculoskeletal pain to practice and exercise at any opportune time and location to prevent augmentation of the symptoms.13,14 Particularly, self-practice for myofascial release is endorsed for handling the musculoskeletal pain and recovery of soft tissue extensibility. 15 These comprise stretching and workouts to recover scapular stability and range of motion. 16
Therapeutic ultrasound is a frequently applied noninvasive modality in the treatment of musculoskeletal conditions. It has been suggested that ultrasound expresses thermal and mechanical properties on deep tissue by sending ultrasonic energy, leading to improved local metabolism, circulation and tissue repair. 17 Various studies have applied ultrasound to treat myofascial pain syndrome.11,18
Recently, the use of extracorporeal shock wave therapy has advanced as an alternative treatment of myofascial pain syndrome.19–21 Extracorporeal shock wave therapy is described as an arrangement of single sonic pulses, supplied by a proper generator to a particular area. The conduction of an acoustic shock wave signal into biological signal consequences in proliferation and differentiation of cellules through a mechano-transduction pathway. 22 Excellences of extracorporeal shock wave therapy are non-invasiveness and insignificant adverse events. 23
Currently, research on extracorporeal shock wave therapy has increased to discover its efficiency, principally for myofascial pain syndrome in the upper trapezius owing to its ability in applying analgesic properties and stimulating soft tissue renovation and repair. 24 Ji HM et al. established the efficacy of four sessions of extracorporeal shock wave therapy (0.056 mJ/mm2, 1000 impulses, semiweekly) in pain reduction compared to the placebo among patients with myofascial pain syndrome of upper trapezius. 25 Jeon JH et al. investigated the efficacy of extracorporeal shock wave therapy in comparison with trigger point injection in addition to transcutaneous electrical nerve stimulation in 30 participants with myofascial pain syndrome in trapezius muscle. The extracorporeal shock wave therapy was as effective as trigger points injection + transcutaneous electrical nerve stimulation in relieving pain and improving cervical range of motion. 21
While studies have revealed some degree of the efficiency, to our knowledge, no studies investigating the effectiveness of extracorporeal shock wave therapy in comparison with standard care and exercise in neck and upper back myofascial pain syndrome patients has been reported. So, we performed a prospective single-blind randomised clinical trial to compare the efficacy of radial extracorporeal shock wave therapy with standard care and self-stretching exercises.
Methods
The present study is prospective, randomised, assessor-blinded, parallel group clinical trial to compare the efficacy of extracorporeal shock wave therapy with standard care and self-stretching exercises in patients with myofascial pain syndrome of neck and upper back area. The study has been conducted from March 2018 to September 2018 at the two Physical Medicine and Rehabilitation outpatient clinics (Imam Reza and Shohada) belong to Tabriz University of medical sciences, Tabriz-Iran. All participants provided written informed consent after a detailed clarification of the objectives and procedures of the study. This study has been approved by the Ethics Committee of the Research Vice-Chancellor of Tabriz University of Medical Sciences (IR.TBZMED.REC.1397.030) and registered on the website of the Iranian Clinical Trial Registry (IRCT201608154104N5). The investigation has been carried out in accordance with the principles of the Declaration of Helsinki and Good Clinical Practice. The CONSORT guidelines were followed and the CONSORT flowchart was provided to reveal the flow of the subjects at every phase of the project.
Patients referred to outpatient clinics were continuously considered for enrollment by a trained physiatrist via non-random convenience sampling method, if they were aged 18 to 55 years, had unilateral or bilateral chronic neck and upper back pain (upper and middle trapezius, levator scapulae, rhomboids, infraspinatus and supraspinatus muscles) lasting more than three months, met at least two of the three diagnostic criteria of myofascial pain syndrome which comprised a tangible taut band, the existence of a tender nodule in the taut band and referral pain. 26 and visual analogue scale ⩾3 mm.
The exclusion criteria were acute spinal pains (occurring for less than three months), radicular pain syndrome, discopathy on a different level of the spine, other diseases within the spine (spondylolisthesis, fractures, tumours, rheumatic diseases), undergoing neck spine operation, receiving analgesics or anti-inflammatory drugs, mental disorders, cancer, psoriasis, scleroderma, neurological deficit symptoms, viral and bacterial infections and contraindication of extracorporeal shock wave therapy such as pregnancy, pacemaker, cardiovascular diseases and coagulation disorders.
Baseline assessment comprised patients’ demographic characteristics (including age, sex and education), anthropometric indices, physical activity and clinical findings. Patients’ weight was assessed with minimal wear and without shoes through a standard scale (Seca 813 digital scale) in an overnight fasting state. Patients’ height was measured through a standard scale (Seca 206 roll-up measuring tape). Body mass index was calculated by dividing the weight (kg) to the square of height (m2). 27 Patients’ physical activity was assessed by the Persian version of International Physical Activity Questionnaire.28–30 Three categories of low, moderate and vigorous physical activity were defined. 31
A total of 72 patients who met the eligibility criteria were randomly allocated into three groups with the allocation ratio of 1:1:1 using the computer-produced random serial numbers and randomised block process via Random Allocation Software. A block size of six was sequentially applied with the allocation of two subjects to every group. The prearranged group allocations were attached in serially numbered, closed and opaque packets. A statistician, who was blinded to all clinical data, performed the random allocation sequence and the allocation. The packets were unlocked consecutively, and eligible subjects were randomly assigned to extracorporeal shock wave therapy group or standard care group or control group. The individuals performing the clinical tests and also the person who performed all the statistical analysis were blinded to group allocation.
This was an open-label study. Though, researchers involving of outcome assessing were blinded. Outcome evaluations were assessed before and after intervention by the same assessors. Statistical analysis was carried out by an independent researcher.
At baseline, one physiatrist performed a clinical examination of the neck and upper back region to identify the four most painful myofascial trigger points. Participants were then examined for pain intensity, pain pressure threshold and disability. These examinations were repeated after the first and fourth weeks of treatment on the weekend and none of the tests were performed on the day of the intervention.
General pain intensity (neck/ upper back pain during the past week) was measured according to visual analogue scale in groups which is a common test, consisted of a direct line with the endpoints demonstrating extreme limits (‘0 = none’ and ’10 = unbearable’). This rating has been shown to have adequate psychometric powers to be applied in chronic pain investigations, and also to be more suitable when maximal reliability is required. 32 Consequently, minimal improvements of 20 percent in visual analogue scale were defined as minimal clinically important difference in the present study. 33 Furthermore, a decrease of 1.5 point was defined as minimum important difference in the present study. 34
Pain pressure threshold was always rated after measuring pain intensity. A digital algometer (Wagner Instruments, Greenwich, CT, USA) was applied to measure pain pressure threshold of four myofascial trigger point positions on both sides: upper and middle trapezius, levator scapulae, rhomboids, infraspinatus and supraspinatus. 35 It has a circular flat tip of 1 cm2, which is to be pushed slowly with 50 kPa/s pressure to the skin over the trigger points after exploration of a taut band with a normalised speed until the subject pressed a switch when the compression sensation altered to pain. This process was repeated three times with a 40-second pause in between and their average was considered as pain pressure threshold. 36 The pressure algometry has been considered as a reliable method for measuring pain pressure threshold with intraclass correlation coefficient of 0.75. 37 A mean difference of 0.94 kg/cm2 in pain pressure threshold was considered as minimal clinically important difference in the present study. 38
Neck functional disability was evaluated by a 10-item neck disability index including questions about activities of daily living, such as personal care, lifting, reading, work, driving, sleeping, recreational activities, pain intensity, concentration and headache. Each item was assessed on each item measured based on a 5-point scale (0 = ‘no disability’ and 5 = ‘complete disability’). The final score between 5 to 14, 15 to 24 and ⩾25 are considered as mild, moderate and severe disability, respectively. 39 We applied the Persian version of the neck disability index with the Cronbach α of 0.88 and intraclass correlation coefficient ranged from 0.90 to 0.97. 40 A 10 percent decrease in neck disability index was considered as minimal clinically important difference in the present study. 33
Any local tissue effects or adverse event happening throughout the trial was recorded and its relation to interventions assessed.
Group 1: radial extracorporeal shock wave therapy + exercise
Participants in extracorporeal shock wave therapy group were requested to lie down in a prone situation with their arms next to the body. One physiatrist evaluated the taut band of key muscles: upper and middle trapezius, levator scapulae, infraspinatus and supraspinatus and applied extracorporeal shock wave therapy (Zimmer enPuls Pro Medizin Systeme Gmbh -shock waves with 2000 impulse and 60 mj /m2 and 5 Hz frequency) to all affected muscles. Patients had four session of radial shock wave therapy (one session per week) in addition to self-neck-stretching exercises and accurate posture. It was planned according to a previous study by Ji HM et al. 41 in which participants with myofascial pain syndrome in the upper trapezius muscle were treated (56 mJ/m(2), 1000 impulses, semiweekly), resulting in significant decreasing of pain after four times therapies in two weeks.
Group 2: ultrasound + exercise
Standard care comprised of hot pack treatment followed by conventional ultrasound. A hot pack (74.5c) was located on the subject’s cervical, para-spinal and upper thoracic areas for 20 minutes. Patients were then given 1 MHz continuous conventional ultrasound treatment at a dose of 1.25 to 1.5 watts/cm2 for five minutes. Treatment was performed for 12 sessions (three sessions per week). In addition participants were educated and advices on accurate posture and self-neck-stretching exercises.
Control: exercise
Participants in all three groups, were educated in a similar way to perform self-neck-stretching exercises each complicated muscle group for 20 seconds and repeat it 10 times per session at home each day till the finalisation of all measurements. The workouts stretch the upper trapezius and scalene, levator scapulae, sternocleidomastoid, middle trapezius and rhomboid muscles and posterior neck musculature (neck flexion, extension, right/left lateral flexion, right/left rotation and pectoral muscle). Exercises were instructed to perform in the order described by Pesco et al. 42 Brochures comprising comprehensive description for stretching exercises were given to the subjects. When patients came for the treatment, they did the exercises under the physiatrist’s superintendence. To ensure compliance, tables for marking when fulfilment of each session were provided to participants. They also were educated on accurate posture in sitting, standing, working and sleeping.
This study aimed to compare the efficacy of extracorporeal shock wave therapy compared to ultrasound + exercise and exercise alone in patients with myofascial pain syndrome. Using G-POWER 3.1.9.2 (Faul, Erdfelder, Lang, & Buchner, 2007) software and considering two-sided α = 0.05, power = 80% and Effect size = 0.4 based on the study of Cho et al., 20 the total sample size was calculated to be 66 (22 in each group). Considering the 10% acceptable drop-out rate, the final sample size for each group will be 24 and a total of 72 for whole trial.
Mean, standard deviation and frequency and percent values are provided in the descriptive statistics of the data. The normal distribution of the variables was assessed with the Shapiro-Wilk test. For intergroup comparisons of baseline data, first three groups were compared using one way ANOVA or Kruskal-Wallis test. For intergroup comparisons of baseline ordinal and nominal variables χ2 test was used. To estimate within group alterations and between group differences, Mixed ANOVA test (time (within subject) * group (between subjects)) along with the sidak posthoc as adjustment procedure were applied. We described effect size in terms of Cohen’s d for outcome measures. We considered the effect sized of 0.2, 0.5 and 0.8 as small, medium and large, respectively. 43 All information obtained from the study were screened and analysed by the SPSS 17.0 software (IBM SPSS Statistics for Windows, Version 17.0. Armonk, NY: IBM Corp). A P value <0.05 was considered as statistically significant.
Results
At baseline, 84 patients were evaluated for eligibility and 72 of them allocated into study groups. A total of 22, 24 and 23 patients completed the study in (1) shock wave, (2) ultrasound and (3) control groups, respectively. The flowchart of participants is presented as Figure 1. Baseline demographic and clinical features of the participants were well balanced between the three groups (P-value >0.05) (Table 1). No serious adverse events or complications after treatments were detected in any of the three groups through the study period.
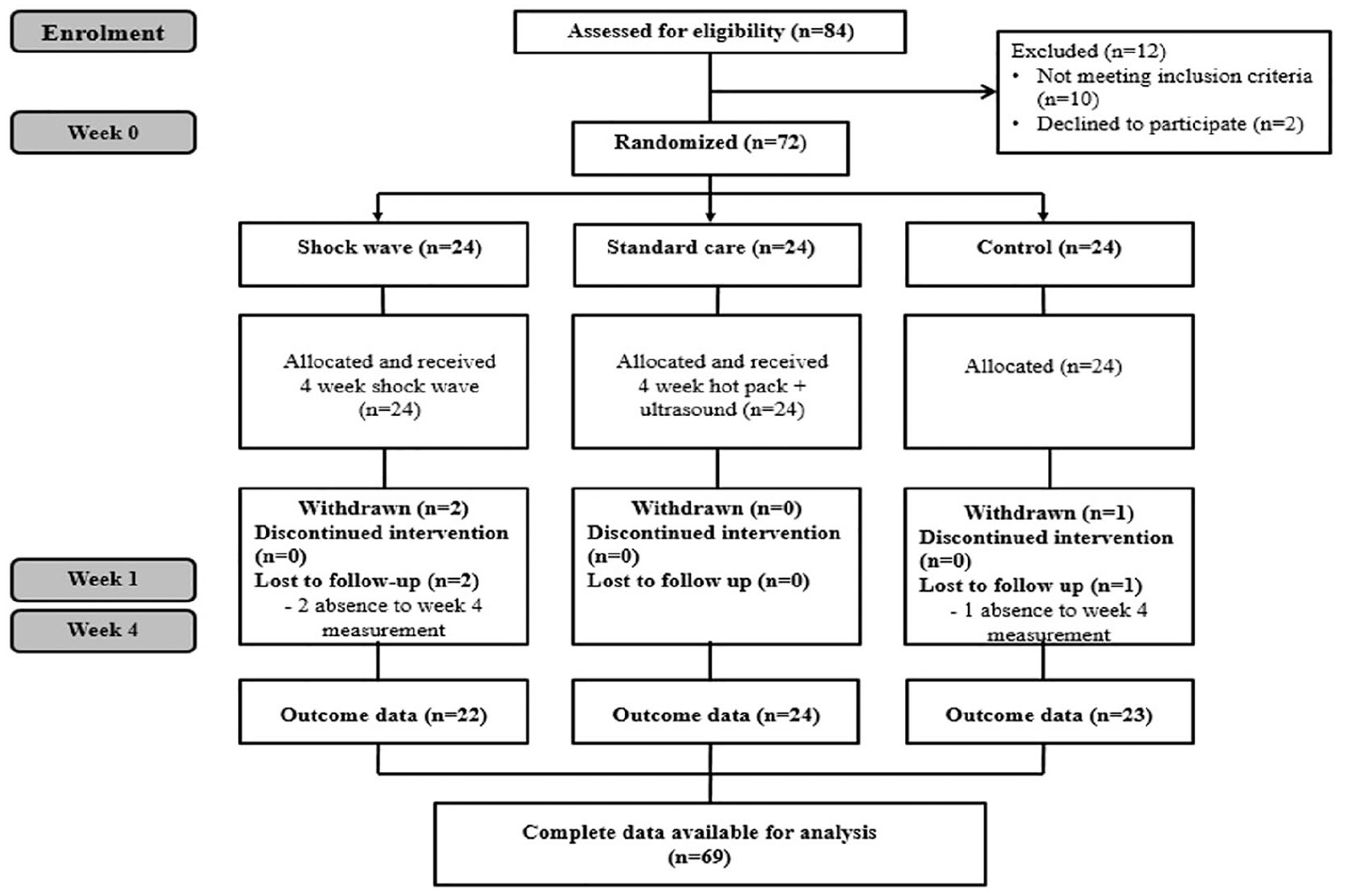
Study flow diagram.
Demographic characteristics of patients participating in the study by trial arm.
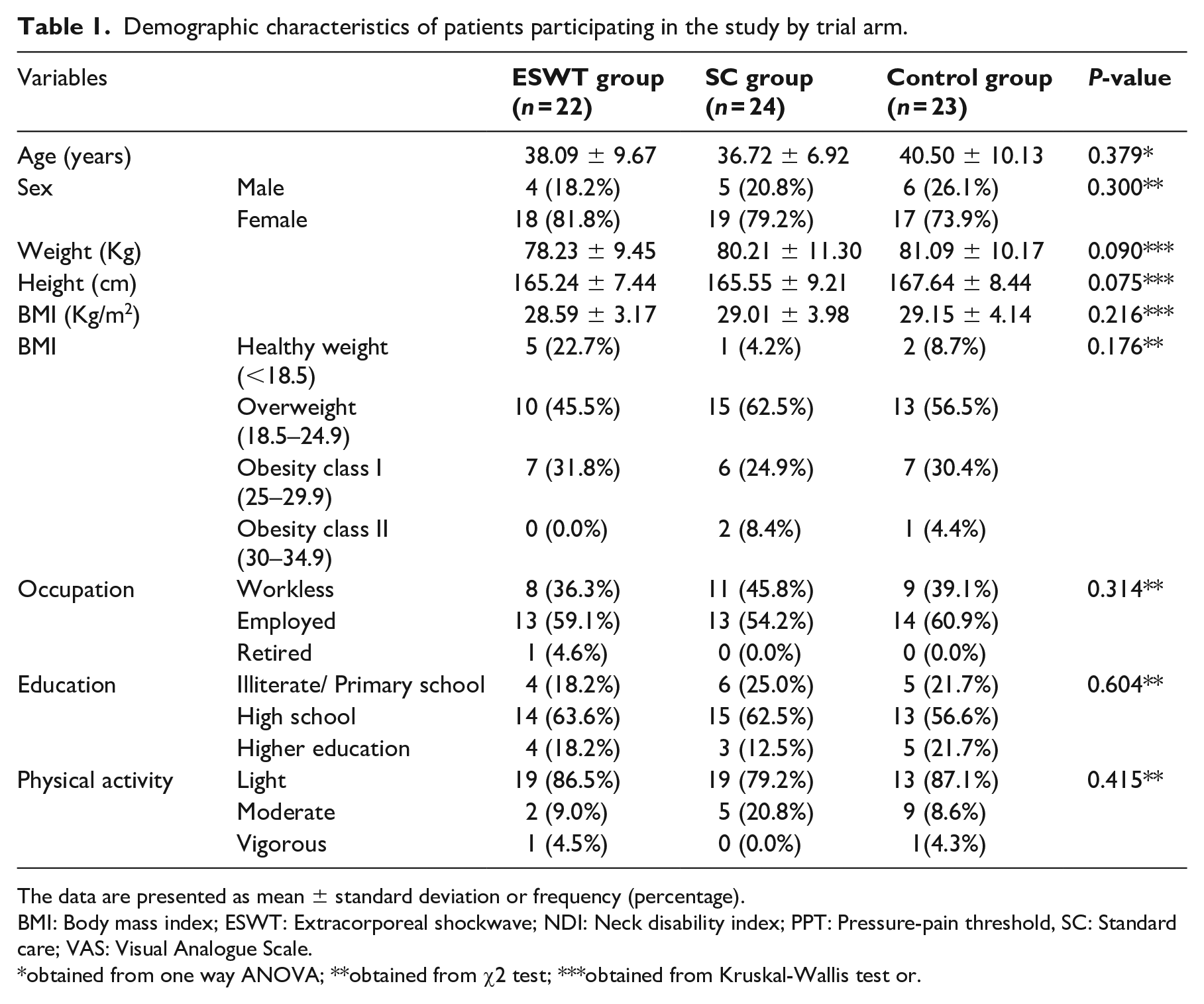
The data are presented as mean ± standard deviation or frequency (percentage).
BMI: Body mass index; ESWT: Extracorporeal shockwave; NDI: Neck disability index; PPT: Pressure-pain threshold, SC: Standard care; VAS: Visual Analogue Scale.
obtained from one way ANOVA; **obtained from χ2 test; ***obtained from Kruskal-Wallis test or.
Significant interaction was seen between time points (0, one week, four week) serving as the within-group factor and group (extracorporeal shock wave therapy vs ultrasound vs control) as the between-group factor concerning the study outcomes (neck disability index: P-value <0.01; pain pressure threshold: P-value <0.05; visual analogue scale: P-value <0.01). According to the interpretation of the Cohen’s d values, the findings referred to large effect size for study outcomes (d = 3.25, d = 1.07 and d = 4.55 for neck disability index, pain pressure threshold and pain intensity, respectively). So we determined the difference between study groups at each level of time factor.
The results on the analysis of clinical outcomes are presented in Table 2. In first week measurements, visual analogue scale improved significantly in the shock wave and ultrasound groups that were significantly higher than the control group (P-value = 0.001, P-value = 0.023, respectively). However neck disability index improved more significantly only in ultrasound group versus the control group (P < 0.001). Shock wave and ultrasound were similarly successful in improving pain intensity, pain pressure threshold and neck disability index at first week after the beginning of the study (all P-values >0.05).
Assessment of the intragroup changes trend in participants.
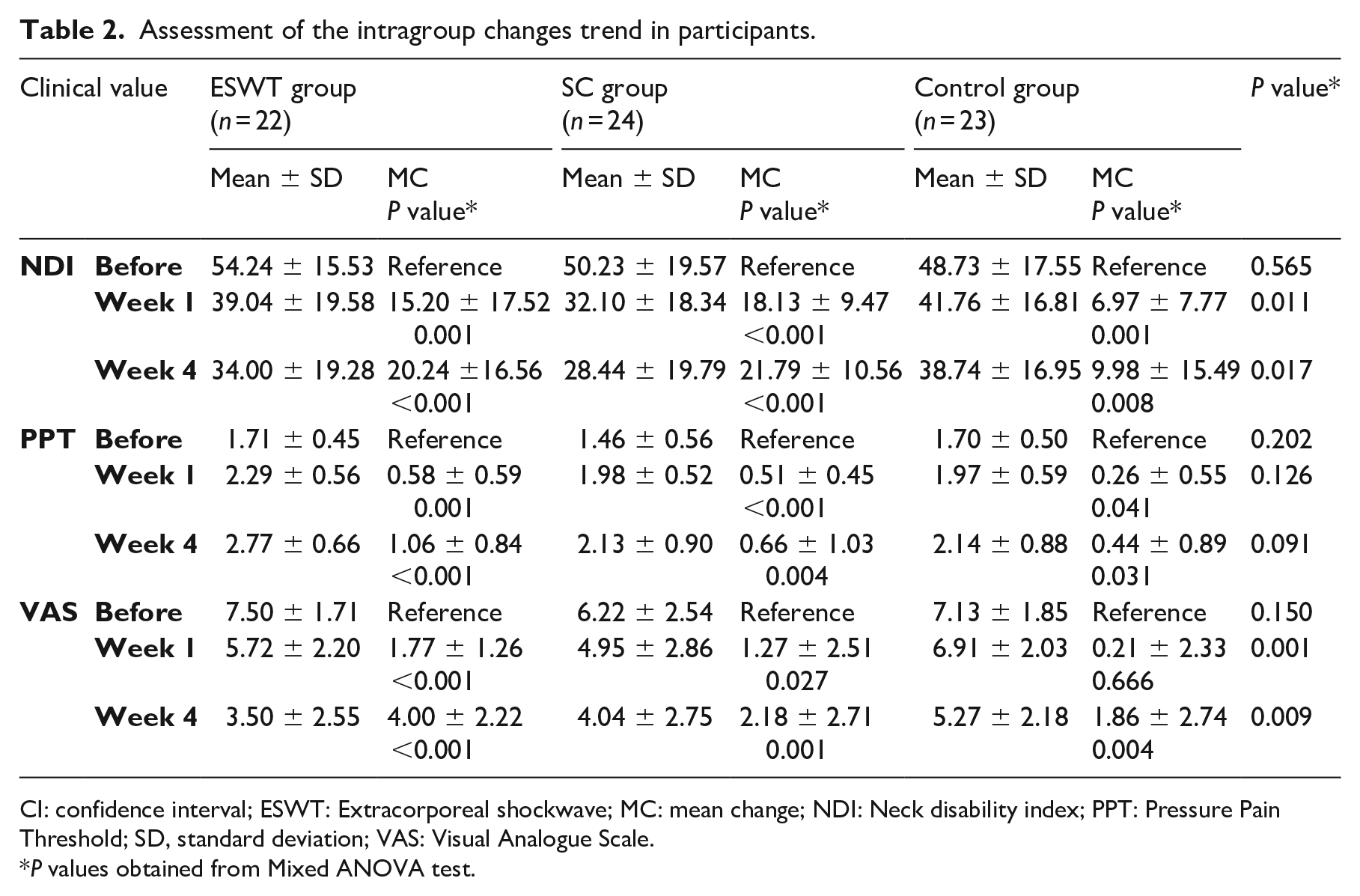
CI: confidence interval; ESWT: Extracorporeal shockwave; MC: mean change; NDI: Neck disability index; PPT: Pressure Pain Threshold; SD, standard deviation; VAS: Visual Analogue Scale.
P values obtained from Mixed ANOVA test.
In week 4 measurements, shock wave and ultrasound improved the neck disability index which significantly higher than control (P-value = 0.040, P-value = 0.005, respectively). However, only shock wave but not ultrasound improved the visual analogue scale and pain pressure threshold in comparison with control at this time point (P-value = 0.007 and P-value = 0.023 for shock wave and P-value = 0.577 and P-value = 0.447 for ultrasound). Shock wave was more successful than ultrasound in decreasing pain intensity (P-value = 0.012). However, there were no significant differences regarding improving pain pressure threshold and neck disability index between shock wave and ultrasound groups (all P-values >0.05).
On the other hand, the number of participants achieved the minimal clinically important difference concerning the visual analogue scale was 19 (86.4%), 15 (68.2%), 11 (50.0%) in shock wave, ultrasound and control groups respectively after four weeks of treatment (P-value = 0.037). The number of participants achieved the minimal clinically important difference regarding the neck disability index was 16 (72.7%), 20 (90.9%), 14 (63.6%) in shock wave, ultrasound and control groups respectively after four weeks of treatment (P-value = 0.103). The number of participants achieved the minimal clinically important difference regarding the pain pressure threshold was 12 (54.5%), 4 (18.2%), 7 (31.8%) in shock wave, ultrasound and control groups respectively after four weeks of treatment (P-value = 0.040).
Discussion
In this trial, we compared the pain intensity, functional disability and pain pressure threshold before and after one and four weeks of (1) extracorporeal shock wave therapy (shock waves with 2000 impulse and 60 mj /m2 and 5 Hz frequency in addition to self-neck-stretching exercises), (2) ultrasound + hot pack in addition to self-neck-stretching exercises and (3) only self-neck-stretching exercises as control in participants with myofascial pain syndrome of neck and upper back area, and recognised some significant variances. There were significant differences in the first and fourth week of treatment regarding functional disability and pain intensity bot not pain pressure threshold between the three groups. At first week evaluations, there were no significant differences between shock wave and ultrasound regarding improving the study main outcomes. At fourth week assessments, extracorporeal shock wave therapy was more effective than ultrasound in decreasing pain in patients. The number of patients achieved the minimal clinically important difference regarding the pain intensity was significantly higher in shock wave group in comparison with ultrasound and control groups after four weeks. In addition, the number of patients reached the minimal clinically important difference regarding the pain pressure threshold was significantly higher in shock wave group in comparison with other treatments. However, there was no significant difference between shock wave and ultrasound in improving disability index and also the number of patients reached the minimal clinically important difference regarding this index at fourth week evaluations.
The myofascial pain syndrome is a complex neuromuscular condition comprising the peripheral and also central pathophysiology. When we left the myofascial trigger points inadequate treated or untreated, the persistent pain would send continuous stimulus through afferent nerves to the spinal cord, and results the spinal segmental sensitisation. 44 Therefore, desensitisation of these trigger points must be objective to provide a persistent and impressive treatment. Generally, the trigger point treatments are categorised as invasive and the noninvasive approaches.
Recently, numerous studies have established the effectiveness of extracorporeal shock wave therapy in subjects with myofascial pain syndrome.20,21,25,45–47 Ji et al. has showed that extracorporeal shock wave therapy on 22 patients with myofascial pain syndrome of upper trapezius is more efficient than standard care in decreasing pain intensity and improving the pain pressure threshold in two weeks. 25 Taheri et al. confirmed that three session of radial extracorporeal shock wave therapy with 1000 impulse and 3 J/m2 and 10 Hz frequency and laser therapy had comparable effect in long-term for relieve of pain and eliminating symptoms in patients with myofascial, however laser provides a faster optimal results. 41 In another study, Király et al. compared the effects of shockwave therapy (once in a week for three weeks) and laser therapy (once daily in a three-week period for a total of 15 sessions) on pain intensity and neck disability index in participants with myofascial pain syndrome of the trapezius. In line with our results, participants in shockwave therapy group established significantly more improvements in pain intensity but also in neck disability. 47 In addition Lee et al. compared the effects of extracorporeal shockwave therapy (1000 impulse and 5 Hz frequency), proprioceptive neuromuscular facilitation and trigger point injection (0.2 mL of 0.3% lidocaine in the pain trigger points) on pain intensity and functional disability in participants with upper trapezius muscle myofascial pain syndrome. In line with our findings, visual analogue scale and neck disability index showed statistically significant differences among the participants in shock wave groups. 46 Moreover, the excellence of extracorporeal shock wave therapy (1000 impulse and 0.01–0.16 J/m2 and 2.5 Hz) for six weeks compared with conservative physical therapy (ultrasound + hot pack + transcutaneous electrical nerve stimulation) in decreasing pain intensity and disability has been confirmed by Han et al. in patients with chronic low back pain. 48
Despite its high cost (equipment cost and space limitation), the extracorporeal shock wave therapy could be considered as an alternative approach for myofascial trigger point treatment. The extracorporeal shock wave therapy has several advantages to other treatment. It is non-invasive, free from infection and feasible to apply in outpatient setting. It is possible to modify the intensity and impulses of extracorporeal shock wave according to patients’ toleration and compliance. This modality could be used to bigger surface by changing its probe position.
The possible adverse events of extracorporeal shock wave therapy comprise headache, syncope, skin erythema, pain and local tiny hematoma. Nonetheless, none of our participants experienced important side effects.
The mechanism of extracorporeal shock wave therapy in myofascial pain syndrome is not completely understood up to now. The myofascial pain syndrome is assumed to originate from an unusual increase in the acetylcholine secretion induce continuous depolarisation of the motor end plates, probably triggering a constant production and calcium2+ influx, leading muscle ischaemia by constant shortening of damaged fibres, production of taut bonds and secretion of sensitising cytokines. 49 The vicious cycle is supplemented through sensitising of the nociceptors and the muscle ischaemia is exacerbated.50,51 It seems that extracorporeal shock wave therapy can stimulate angiogenesis, enhance perfusion and change the pain signalling at ischaemic tissues. 25
To our knowledge, this is the first study comparing the extracorporeal shock wave therapy, ultrasound along with hot pack and self-neck-stretching exercises and also self-neck-stretching exercises alone concerning the pain intensity, functional disability and pain pressure threshold in participants with chronic neck and upper back area myofascial pain syndrome with promising and practical findings in favour of efficacy and safety of extracorporeal shock wave therapy in these patients. However, it has some limitations which should be acknowledged. First is the demographical limitations (a small number of participants and female predominance). The study sample size was relatively small to generalise the findings of the study. Second is the single-blind design. Though the participants and outcome assessors were blinded to the study group assignments, the therapist was not blinded when accompanying the treatments. Third, in participants with bilateral neck pain, we considered the more painful side, which may confound the results of the study. Fourth, the localisation of the myofascial trigger points may alter through the sessions of intervention and affect the findings of our study. Fifth, we did not consider psychological variables which may affect outcomes. Pain itself is an individual perception and can be associated to various factors. These limitations should be taken into account in future studies to present adequate evidence for clinical approaches. More participants from several medical centres with longer follow-up period are desirable for future study. In a clinical practice, and based on present findings, we can recommend the extracorporeal shock wave therapy as a safe, non-invasive and tolerable first line approach for managing the patients with chronic neck and upper back myofascial pain syndrome.
In conclusion, our study revealed the effect of extracorporeal shock wave therapy and ultrasound plus hot pack in addition to self-stretch-exercises on pain intensity, physical disability, pain pressure threshold in the treatment of myofascial pain syndrome of neck and upper back. Extracorporeal shock wave therapy was more efficient than ultrasound in alleviating pain intensity at fourth week of treatment. However, extracorporeal shock wave was not better than ultrasound in improving neck disability index at this time point. Further studies with different treatment protocol concerning dosage, frequency, duration and application locates are required to generalise and confirm these findings in patients with myofascial pain syndrome.
Clinical messages
Extracorporeal shock wave therapy for four weeks significantly improve pain intensity, neck disability index and pain pressure threshold in patients with neck and upper back myofascial pain syndrome.
Extracorporeal shock wave therapy for four weeks is more efficient than standard care (ultrasound + hot pack + self-stretch-exercises) in reducing pain intensity. However, it is not better than standard care regarding neck disability index at this time point.
Footnotes
Acknowledgements
We are grateful to all of the patients who assisted us to perform this study. The authors would like to acknowledge the personnel of the Physical Medicine and Rehabilitation Research Center of Tabriz University of Medical Sciences for their patronage with this study. The results presented in this article were a part of a thesis by M. Samandarian.
Authors’ contributions
Mohammad Rahbar, Maryam Samandarian and Neda Dolatkhah contributed to conception and design of the study, data analysis and interpretation, and drafting the manuscript. Maryam Samandarian collected all data and contributed to data interpretation and drafting the manuscript. Maryam Samandarian, Zhila Khamnian and Neda Dolatkhah drafted the first manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was received from the Vice Chancellor of Research, Tabriz University of Medical Sciences, Tabriz, Iran. The funding body had no role in the design of the study, collection, analysis, or interpretation of the data, or writing of the manuscript.
Ethics approval and consent to participate
All participants were provided written informed consent and endorsement has been acknowledged from the Ethics Committee of the Research Vice-Chancellor of Tabriz University of Medical Sciences (IR.TBZMED.REC.1397.030). Patients’ personal data about patients were conserved in a database to keep patients’ security. The study was also registered in the clinical trial registry under number IRCT201608154104N5 code.