
Abstract
Objective:
The aim of this study was to determine whether perioperative breathing training reduces the incidence of postoperative pulmonary complications in patients undergoing laparoscopic colorectal surgery.
Design:
A randomized controlled trial.
Setting:
University hospital.
Subjects:
A total of 240 patients undergoing laparoscopic colorectal surgery participated in this study.
Intervention:
The enrolled patients were randomized into an intervention or control group. Patients in the intervention group received perioperative breathing training, including deep breathing and coughing exercise, balloon-blowing exercise, and pursed lip breathing exercise. The control group received standard perioperative care without any breathing training.
Main measures:
The primary endpoint was the incidence of postoperative pulmonary complications. The secondary objectives were to evaluate the effect of perioperative breathing training on arterial oxygenation, incidence of other postoperative complications, patient satisfaction, length of stay, and hospital charges.
Results:
The incidence of postoperative pulmonary complications in the breathing training group was lower than that in the control group (5/120 [4%] vs 14/120 [12%]; RR 0.357, 95%CI 0.133–0.960; P = 0.031). In addition, PaO2 and arterial oxygenation index on the first and fourth days after surgery were significantly higher in the breathing training group than in the control group (P < 0.001). In addition, patients with breathing training had shorter length of stay (6d [IQR 5–7] vs 8d [IQR 7–9]), lower hospital charges (7761 ± 1679 vs 8212 ± 1326), and higher patient satisfaction (9.46 ± 0.65 vs 9.21 ± 0.47) than those without.
Conclusion:
Perioperative breathing training may reduce the incidence of postoperative pulmonary complications and preserve of arterial oxygenation after laparoscopic colorectal surgery.
Introduction
Patients undergoing colorectal cancer surgery are at risk of postoperative pulmonary complications, which lead to increased postoperative length of stay, mortality, and medical consumption.1,2 The incidence of pulmonary complications after abdominal surgery has been reported to be between 4% and 21% depending on the definition of postoperative pulmonary complications and the diagnostic techniques used.3–5
The reduction in pulmonary volume and respiratory muscular activation after major abdominal surgery due to surgery-related shallow breathing, pain, long-term bed rest, mucociliary clearance disorder, and diaphragmatic dysfunction may be the main causes of postoperative pulmonary complications.6–8 Multiple studies have suggested that breathing training may help improve respiratory muscle activity, mobilize secretions, re-expand areas of collapsed lungs, and maintain high pulmonary volumes, although evidence is inconclusive.9–11 Thus, breathing training has been widely used to prevent postoperative pulmonary complications in patients undergoing major surgery.5,9
However, breathing training to prevent postoperative pulmonary complications has shown contradictory results, as some studies have shown little benefit from this intervention.12,13 Due to the considerable heterogeneity of these studies, it is impossible to accurately assess the effectiveness of breathing training. In addition, past research on preventing postoperative pulmonary complications has predominantly focused on open abdominal surgery, and there have been few studies on the laparoscopic surgical cohort. With the introduction of enhanced recovery after surgery (ERAS) pathways and minimally invasive surgery, laparoscopic surgery has become increasingly common in abdominal surgery. Although laparoscopic surgery can decrease the incidence of postoperative pulmonary complications compared to open abdominal surgery,1,14 prevention of postoperative pulmonary complications remains important in terms of perioperative management of laparoscopic surgery patients. 15 Thus, more research needs to be conducted to access adequate evidence regarding the effectiveness of breathing exercises and select appropriate strategies to prevent postoperative pulmonary complications in the laparoscopic surgical cohort.
As different types of breathing exercises can improve respiratory function in different ways, it is plausible to hypothesize that combined modalities are more likely to reduce the risk of postoperative pulmonary complications. Here we determined whether perioperative combined breathing training can reduce the incidence of postoperative pulmonary complications in patients undergoing laparoscopic colorectal surgery.
Methods
This was a single-blind randomized controlled trial performed from March 2019 to October 2019 in a single university-affiliated tertiary center. This study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of the First Affiliated Hospital of Chongqing Medical University (Chinese Clinical Trial registration: ChiCTR2000039120). The First Affiliated Hospital of Chongqing Medical University was responsible for the integrity and conduct of the study.
Patients who were waiting for elective laparoscopic colorectal resection for at least five days were invited to participate in this study. The patients were evaluated preoperatively for demographic data (including sex, age, and BMI), smoking history, clinical history, American Society of Anesthesiologists class, and nutritional risk screening score. Nutritional status assessment was evaluated using the Nutritional Risk Screening Tool (NRS2002). 16 Two surgeons who were involved neither in the data collection nor in the data analysis screened and recruited the participants into the study by face to face interview. All eligible patients were asked to provide informed consent before they were enrolled in this study.
Inclusion criteria were patients over 18 years old who had received elective laparoscopic colorectal surgery. Exclusion criteria were emergency surgery, cognitive dysfunction, neuromuscular diseases, American Society of Anesthesiologists class ⩾IV, history of spontaneous pneumothorax, coagulation dysfunction, acute respiratory failure, established respiratory infection, uncontrolled general infection, and failure to obtain informed consent.
Eligible patients were randomly assigned to either an intervention or control group using a computer-generated randomized block design. The randomization block size was two with equal numbers for both groups, and the numbers were sealed in sequentially numbered opaque envelopes organized in randomization sequence by an independent researcher not involved in recruitment, assessment, or treatment. After the baseline assessment, the independent researcher was in charge of opening the envelope to complete the random assignment.
All patients were admitted to our hospital at least five days before surgery. Patients in the intervention group received three types of respiratory training (including deep breathing and coughing exercise, balloon-blowing exercise, and pursed lip breathing exercise) daily in the hospital, three times a day, for at least five days before surgery, and continued training four days after surgery. On the day of admission to the hospital, the patients in the intervention group were instructed to perform breathing training by one of four rehabilitation physicians who had less than five years of rehabilitation experience. In addition, patients received brochures and a video with instructions that described the importance of breathing training and the method of breathing training. In order to ensure the best possible performance during the intervention, the patients were instructed by physiotherapists to perform three types of breathing training in the first session of each day, while the other sessions were supervised by trained nurses who were previously trained by physiotherapists. Compliance with treatment was recorded by the nurses. Perioperative breathing training in the intervention group was carried out as follows:
Deep breathing and coughing exercise
The patients were instructed to perform deep breathing and coughing exercises in the sitting position. Patients were instructed to inhale deeply through the nose while expanding their diaphragm and abdomen, and then keep holding their breath for three seconds. Then, patients were instructed to cough to mobilize the lung secretions. Patients rested for 30 seconds following each cough. The deep breathing and coughing exercise was to be repeated five times thrice daily.
Balloon-blowing exercise 17
Patients were asked to hold a balloon in one hand and raise the other hand above their heads. Maintaining this posture, the participants inhaled through the nose and slowly blew out into the balloon. They were then instructed to pause for three seconds with the tongue positioned on the roof of the mouth to prevent airflow out of the balloon. Simultaneously, patients were asked to inhale again through the nose, and then exhale through the mouth into the balloon. After the third or fourth breath in, the balloon neck was held and removed from the mouth. Patients relaxed for 60 seconds and repeated four more times. The balloon-blowing exercise was to be repeated five times thrice daily.
Pursed lip breathing exercise
Patients were asked to slowly inhale through their nose for at least two seconds while keeping their mouth closed, and then hold their breath for three seconds. They were then taught to slowly breathe out all the air through the mouth with their lips pursed for at least four seconds. Participants were taught to perform pursed lip breathing at a rate of 4–5 cycles per minute, exercising three times a day for 10 minutes each.
Patients in the control group received standard perioperative care without any breathing training. The perioperative care included but was not limited to preoperative education, preoperative medical optimization of chronic disease, preoperative nutritional care, preoperative smoking cessation, standard anesthetic protocol, goal-directed fluid therapy, restrictive use of surgical drains, early removal of urinary catheter, and encouragement of early ambulation and feeding.
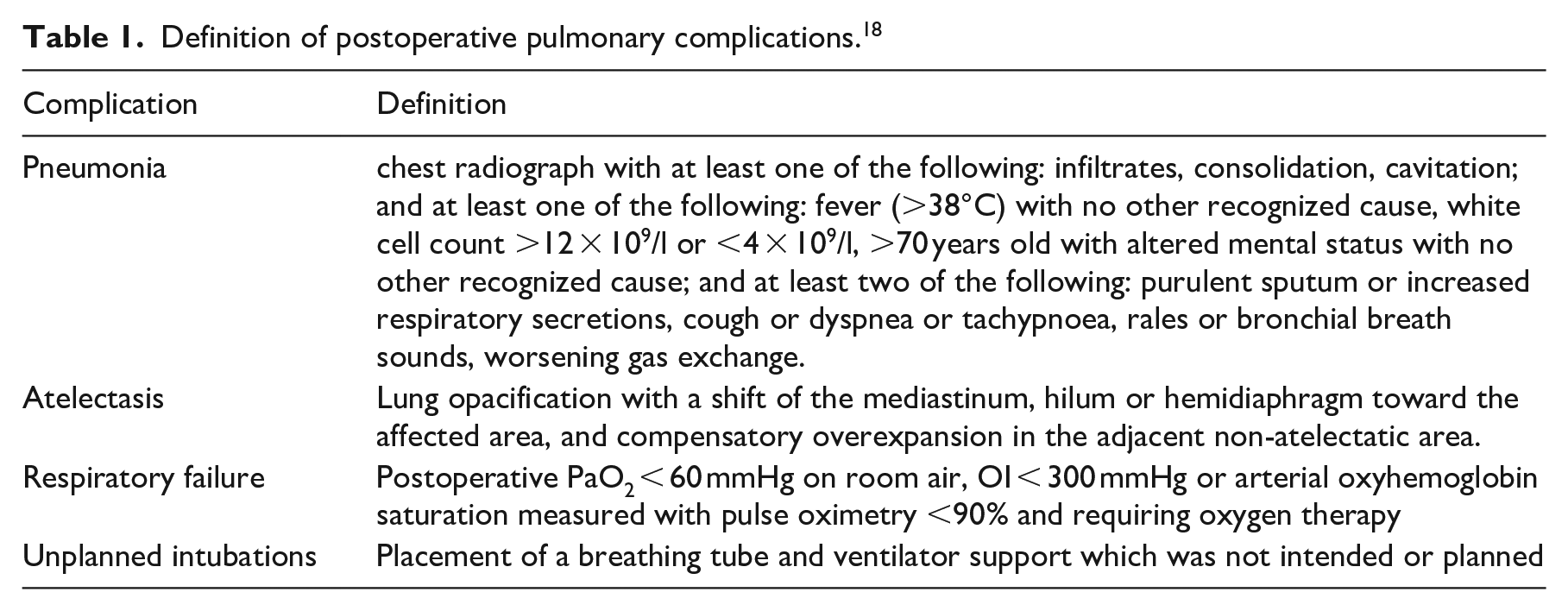
The primary endpoint of the study was the incidence of postoperative pulmonary complications, including pneumonia, atelectasis, respiratory failure, and unplanned intubations. Postoperative pulmonary complications were monitored until hospital discharge. They were defined according to the guidelines for European perioperative clinical outcome (EPCO) definitions, as shown in Table 1. 18 In order to detect all relevant postoperative pulmonary complications, chest radiographs were obtained on the fourth postoperative day. In addition, chest radiography should be performed in time if the patient has respiratory symptoms or other symptoms that may indicate pulmonary complications, such as fever, elevated or lowered white cell count, cough, purulent sputum, dyspnea, tachypnea, rales, bronchial breath sounds, and/or worsening gas exchange. The radiologist and radiographer who were blinded to the study group assignments made all measurements.
Definition of postoperative pulmonary complications. 18
Secondary endpoints included other postoperative complications, patient satisfaction, arterial oxygenation, postoperative length of stay, total hospital costs, and in-hospital mortality. Arterial blood gas measurements were performed at three time points: preoperatively prior to starting breathing training and on the first and fourth postoperative days. The patients had been without supplementary oxygen for at least 15 minutes. Patient satisfaction was evaluated using the 10-point numerical rating scale, with one indicating very dissatisfied and 10 indicating very satisfied. This score was built in as the results for the question “Please assess the satisfaction with the overall treatment you received in the hospital.” Length of stay was defined as the number of days patients stayed in the hospital after surgery. Hospital costs obtained from hospital databases were defined as the amount billed by healthcare providers for services during hospitalization. The costs were presented as RMB converted to Euro (April 2020).
A sample size calculation was based on the primary endpoint, the incidence of postoperative pulmonary complications. The study was powered based on two rationales: relative risk reduction in postoperative pulmonary complications of approximately 75% as reported by previous similar trials of breathing training,5,19 and a postoperative pulmonary complication rate of approximately 14% in our hospital, identified by a retrospective audit of consecutive patients requiring colorectal surgery. 20 A sample size of 113 patients per group was required to detect a statistically significant difference at a two-sided significance level of 0.05% and 80% statistical power. To account for patient dropouts and missing data, we planned to recruit 240 patients.
All statistical analyses were conducted using SPSS 23.0 (SPSS, Inc., Chicago, IL, USA). Normally distributed continuous variable data are expressed as mean ± standard deviation (SD), skewed continuous variable data as median (interquartile range) and categorical variable data as percentages. Continuous data were compared using independent t-test or Wilcoxon rank test or Kruskal-Wallis test in terms of data distribution. Chi square test was used to compare categorical data. Fisher’s exact test was used for categorical variables when the number of events was less than five. For all statistical analyses, a P value <0.05 was considered statistically significant.
Results
The flow of patients in the study is shown in Figure 1. We assessed the eligibility of a total of 268 patients to be included in this research from March 2019 to October 2019. From the initial sample of patients, 245 met the inclusion criteria and were randomly assigned to either the breathing training group (n = 122) or the control group (n = 123). After randomization, five patients (2%) were lost to follow-up from the trial, leaving 240 (98%) included in the primary analysis (120 in the breathing training group and 120 in the control group).
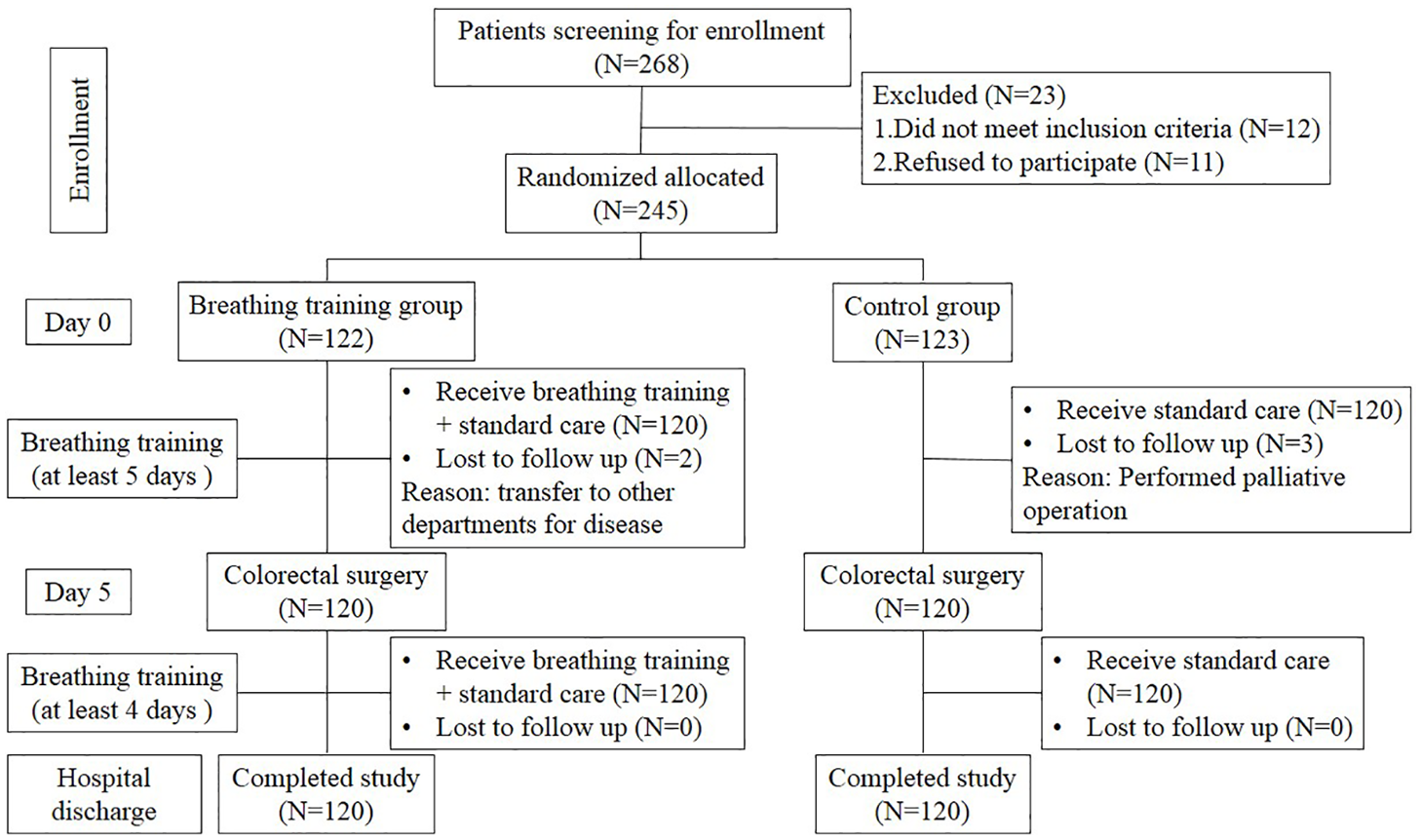
Study flow diagram.
Breathing training group and control group demographic characteristics and perioperative data are compared in Table 2. There were no significant differences in baseline characteristics between the two groups, including age, body mass index, sex, smoking history, nutritional risk screening score, ASA class, chronic obstructive pulmonary disease, coronary artery disease, hypertension, and diabetes. In addition, no differences were observed in anesthetic time, surgical time, or bleeding volume.
Demographics, preoperative complication, perioperative outcomes.
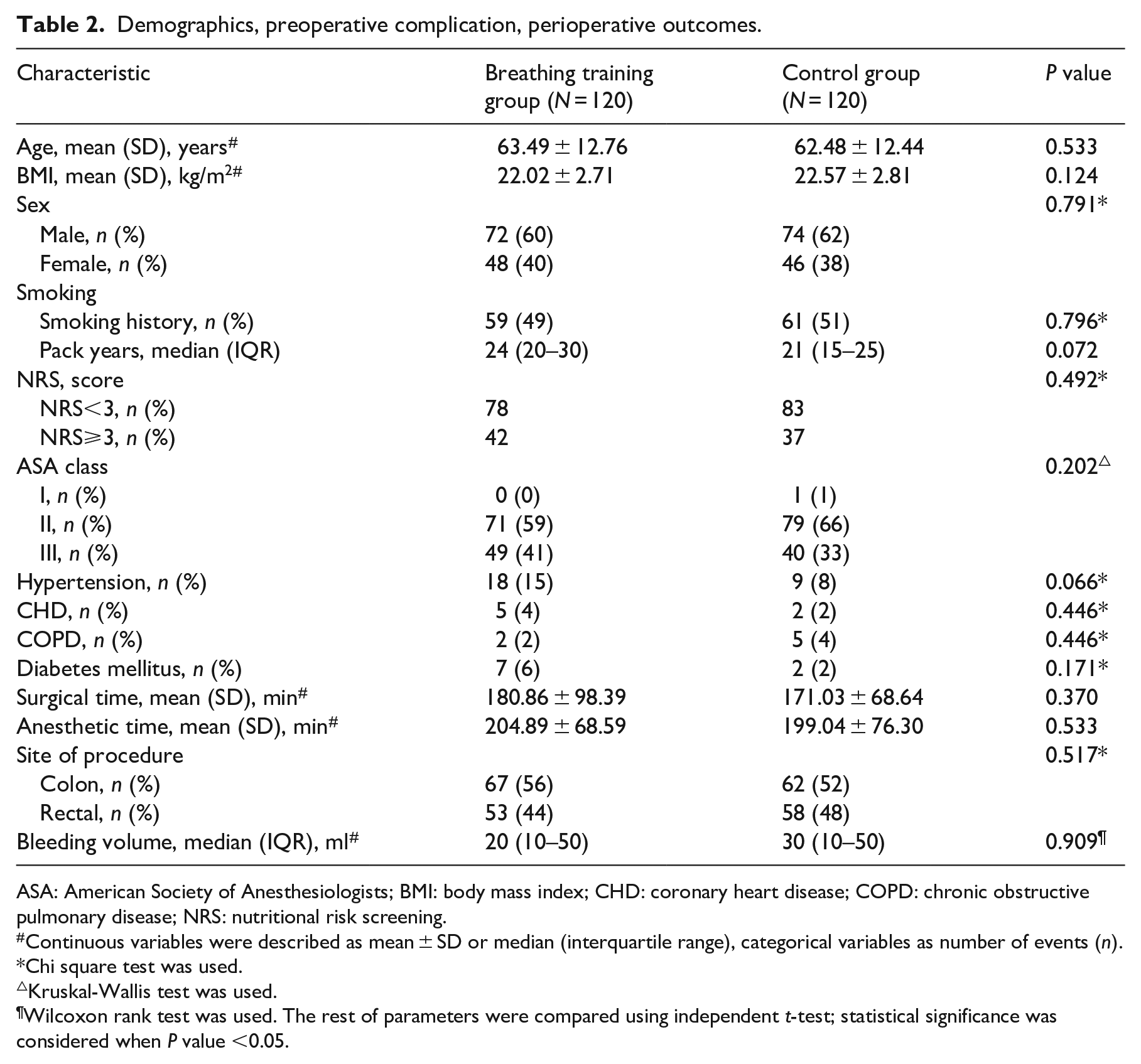
ASA: American Society of Anesthesiologists; BMI: body mass index; CHD: coronary heart disease; COPD: chronic obstructive pulmonary disease; NRS: nutritional risk screening.
Continuous variables were described as mean ± SD or median (interquartile range), categorical variables as number of events (n).
Chi square test was used.
Kruskal-Wallis test was used.
Wilcoxon rank test was used. The rest of parameters were compared using independent t-test; statistical significance was considered when P value <0.05.
Table 3 shows significantly fewer postoperative pulmonary complications in the breathing training group than in the control group (5/120 [4.17%] vs 14/120 [11.67%]; RR 0.357, 95% CI 0.133–0.960, P = 0.031). However, there were no significant differences in the incidences of non-pulmonary complications between the two groups.
Incidence of postoperative complications during hospital stay.
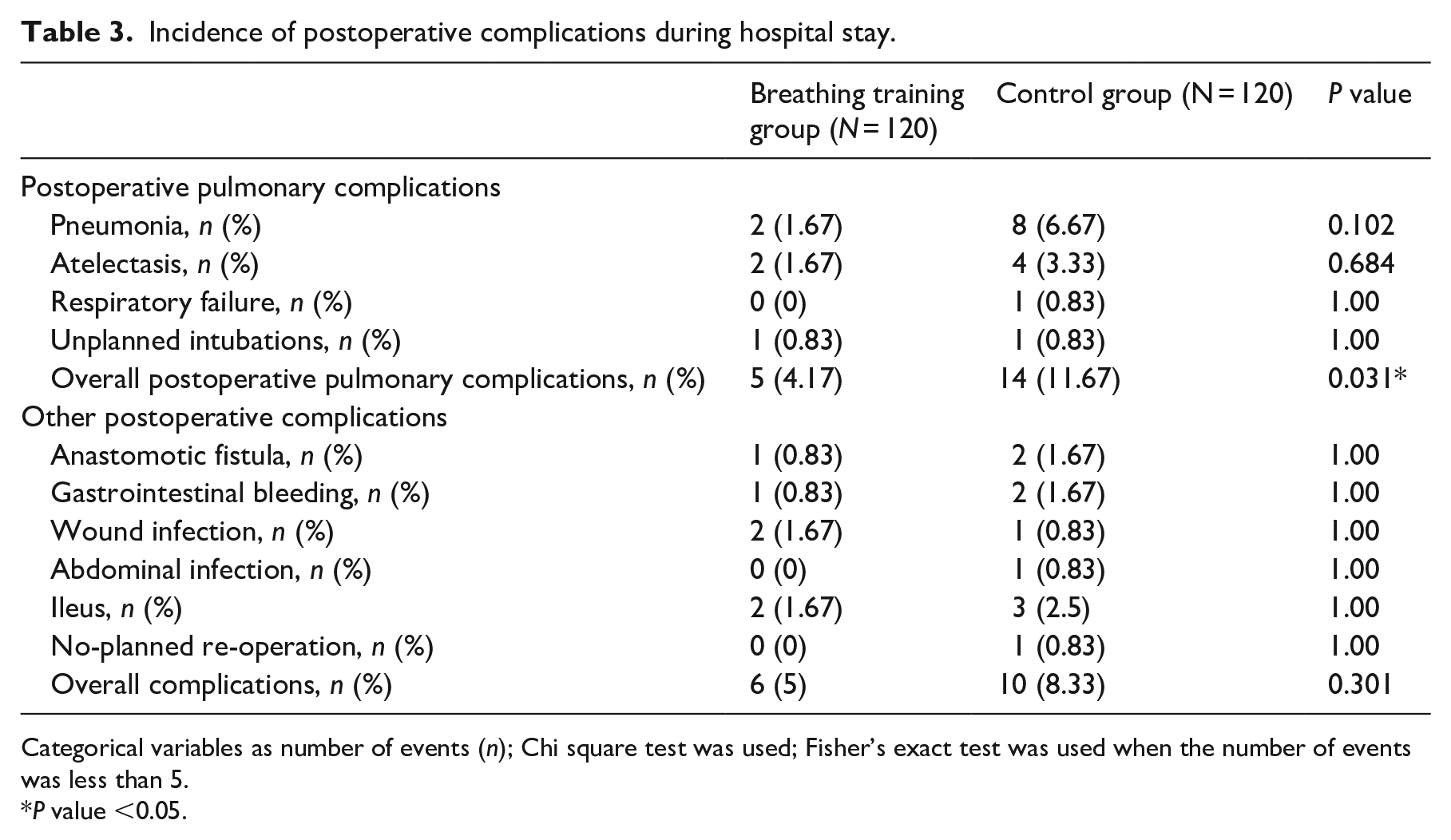
Categorical variables as number of events (n); Chi square test was used; Fisher’s exact test was used when the number of events was less than 5.
P value <0.05.
After breathing training, patients had a better preservation of PaO2 on the first and fourth postoperative days (P < 0.001, Table 4). Similarly, postoperative OI in the breathing training group was higher than that in the control group (P < 0.001, Table 4). As shown in Table 5, patients in the breathing training group showed higher satisfaction scores, shorter postoperative length of stay, and lower hospital charges compared with patients in the control group.
Arterial blood gasses analysis in each group before starting breathing training and on the first and fourth postoperative days.
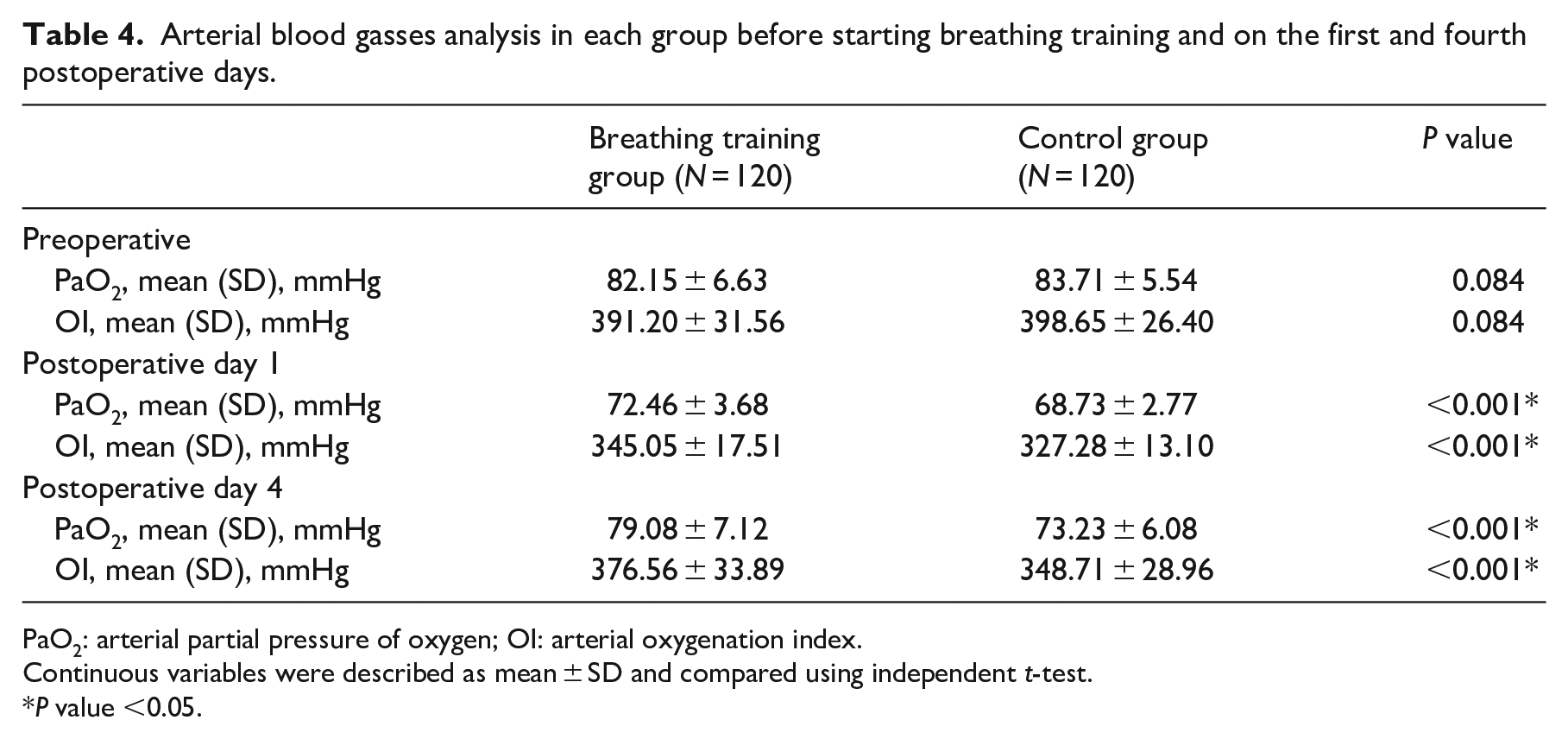
PaO2: arterial partial pressure of oxygen; OI: arterial oxygenation index.
Continuous variables were described as mean ± SD and compared using independent t-test.
P value <0.05.
Length of hospital stay and hospital costs.
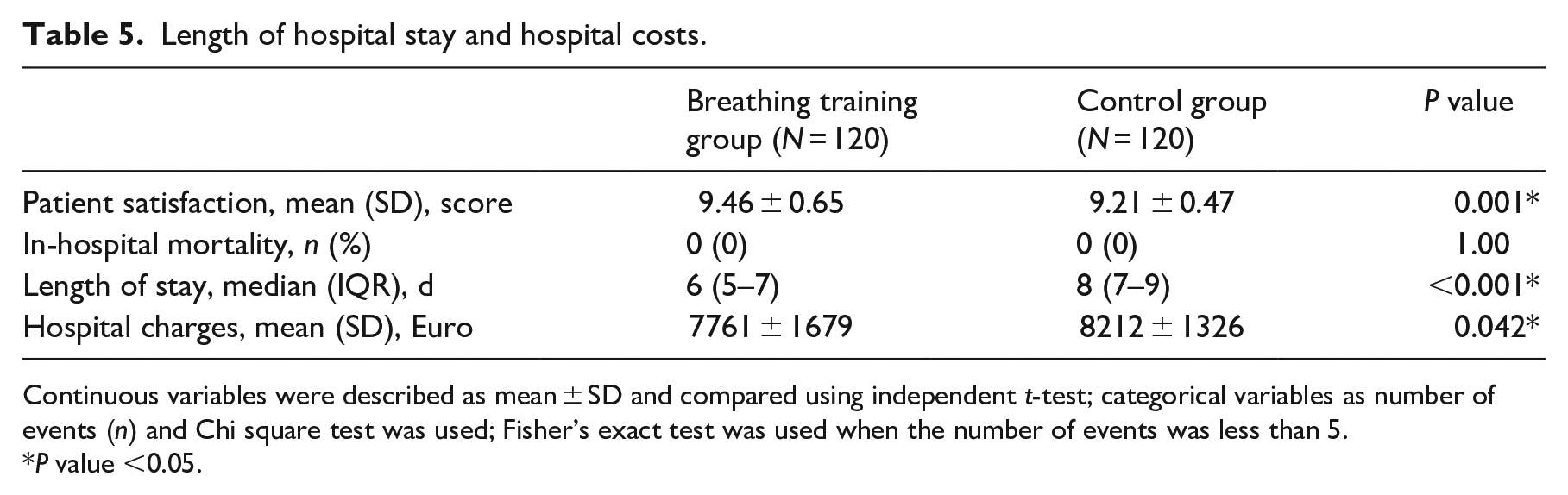
Continuous variables were described as mean ± SD and compared using independent t-test; categorical variables as number of events ( n ) and Chi square test was used; Fisher’s exact test was used when the number of events was less than 5.
P value <0.05.
Discussion
The results of the present study demonstrated that breathing training in the preoperative and postoperative periods could reduce the incidence of postoperative pulmonary complications and arterial blood gas disorders in patients undergoing laparoscopic colorectal cancer surgery. These results were in accordance with other randomized studies that found that breathing training was associated with an approximately 75% relative risk reduction in postoperative pulmonary complications.5,19
The patients in the intervention group were encouraged to perform three types of breathing exercises throughout the perioperative period, including deep breathing and coughing exercise, balloon-blowing exercise, and pursed lip breathing exercise. These methods of breathing training were chosen based on substantial clinical evidence. Sputum retention is common after major surgery, and is a main cause of postoperative pulmonary complications. 21 Compelling evidence has shown that deep breathing and cough could promote re-expansion of areas of collapsed lung and increase sputum excretion by increasing the instantaneous airflow in the airways during exhalation. 10 Previous studies have demonstrated that balloon-blowing exercise can improve pulmonary function and respiratory muscle activities in elderly smokers and young people, as shown by improving vital capacity, forced vital capacity (FVC), forced expiratory volume in one second (FEV1), FEV1/FVC, peak expiratory flow, and muscle activity in the rectus abdominis.17,22 In addition, pursed lip breathing exercises have been shown to improve breathing efficiency and reduce symptoms of dyspnea. 23 Therefore, we could speculate that these combined effects may be achieved through reversing the postoperative pathophysiological reduction of postoperative lung volume, respiratory muscle function, and mucociliary clearance to reduce postoperative pulmonary complications.
In our study, arterial blood gas measurements were performed before starting the breathing training and repeated on the first and fourth postoperative days. Compared to the preoperative arterial oxygenation, there was a significant reduction in PaO2 and OI in both the intervention and control groups on the first postoperative day, which was the same as the previous findings after coronary artery bypass grafting surgery. 24 This is mainly caused by residual anesthetics and neuromuscular blocking drugs, which can impair respiratory muscle function and reduce the ventilation perfusion (V/Q) ratio, leading to impaired oxygenation.25–27 Breathing training has been reported to improve postoperative oxygenation in patients undergoing cardiac surgery. 28 Another randomized controlled trial also found that patients who underwent breathing training had significantly higher oxygen saturation on the first three days after major abdominal surgery. 19 Similar results were found in our experiments that a slightly better preservation of arterial oxygenation was also seen in the breathing training group than in the control group on the first and fourth postoperative days.
Although breathing training is commonly used in the management of patients undergoing major abdominal surgery in many countries, evidence for the efficacy of this treatment remains controversial.12,29 The reasons for these contradictory results of breathing training may be related to considerable diversity in intervention protocol, patient compliance, type of surgery, and population of intervention.
To the best of our knowledge, breathing training interventions to prevent PPCs usually focus solely on preoperative or postoperative prophylaxis in most clinical trials, and rarely focus on both preoperative and postoperative periods. Preoperative breathing training may increase respiratory muscle strength and lung function,9,19 and improve the time point of initiation of breathing exercises after surgery. Postoperative breathing training may reverse lung volume reduction and atelectasis caused by surgery and anesthesia. 11 Therefore, we speculated that breathing training that covered both the preoperative and postoperative periods would be more likely to achieve better results. In addition, the combined effect of the three types of breathing training may also help to achieve positive results.
Patient compliance is crucial to the efficacy of breathing training. Compared to breathing training methods of other trials, such as inspiratory muscle training, these three types of interventions can be easily accomplished without the use of any specialist equipment, and only the use of balloons, which can be easily purchased. Moreover, preoperative educational materials (brochures and video) and nurse supervision improved patient compliance to complete breathing training, ensuring the effectiveness of this program.
In addition, most evidence suggests that breathing training should be reserved for patients at high risk for postoperative pulmonary complications.30,31 In the current study, most patients had a history of smoking, were older than 60 years, and had a high ASA class, which were risk factors for developing postoperative pulmonary complications in patients undergoing abdominal surgery.32,33 The duration of surgery and anesthesia was longer than three hours. A previous study had identified that the odds ratio of postoperative pulmonary complications increased further as the operating time increased, to 9.7 over three hours. 34 Above all, we speculated that patients undergoing colorectal surgery could benefit from the breathing training program. As expected, our results showed that the incidence of postoperative pulmonary complications in the breathing training group decreased from 11.67% to 4.17% compared with that of the control group.
Compelling evidence has identified that postoperative pulmonary complications are associated with a considerable increase in mortality, morbidity, length of stay, and hospital cost. Thompson et al. found that patients with hospital-acquired pneumonia after abdominal surgery had an increased length of stay by 11.03 days and hospital charges by $28,000. 35 Reduction in the incidence of postoperative pulmonary complications has been shown to be associated with improved patient outcomes. 36 A recent health economic analysis of a multicenter randomized trial also suggested that preoperative physiotherapy aimed at preventing postoperative pulmonary complications was highly likely to be cost-effective from the hospitals’ perspective, and cost the hospitals less than the costs estimated to treat a postoperative pulmonary complication after surgery for each PPC prevented. 37 Our research also showed that the lower incidence of postoperative pulmonary complications in patients with breathing training was accompanied by shorter length of stay and lower hospital cost. In addition, the incidence of other postoperative complications in the breathing training group was similar to that in the control group. The results suggested that breathing training may not cause significant side effects. More importantly, patient satisfaction in the breathing training group was higher than in the control group. Therefore, we speculate that breathing training is acceptable and feasible.
There are several limitations to our study. First, our study is unable to evaluate the effect of breathing training on long-term outcomes, especially the lack of any other data about other aspects of functional recovery, such as return to independence in personal activities of daily living or return to work. In addition, this study did not compare the effects of different types of breathing training, including single modality and combined modalities. Moreover, we did not assess whether the increase or decrease in the dose, intensity, and duration of breathing training influenced its effectiveness in reducing postoperative pulmonary complications. Therefore, future studies are needed to address these points. Second, we did not accurately quantify the mobilization of patients during hospitalization, which was related to reducing the risk of postoperative pulmonary complications. Third, hospital charges did not include the cost of organizing the preoperative rehabilitation, which caused our cost to be rough. Fourth, the study was conducted at a single large academic hospital, which may have limited the generalizability of our results.
In summary, our study demonstrated that perioperative breathing training may be associated with reduced incidence of postoperative pulmonary complications and improved arterial oxygenation after laparoscopic colorectal cancer surgery. Perioperative breathing training should be considered for all patients awaiting colorectal surgery.
Clinical messages
Perioperative breathing training reduced the incidence of postoperative pulmonary complications and improved preservation of arterial oxygenation after colorectal cancer surgery.
Perioperative breathing training shortened postoperative length of stay, improved patient satisfaction, slightly reduced hospital charges, and did not cause significant side effects.
Footnotes
Authors contributions
P.P.Q., J.Y.J., W.J.W., S.M. designed the study methodology. P.P.Q. and W.J.W. collected the data. P.P.Q. analyzed the results and drafted the article. All authors reviewed and revised the work. All authors reviewed the final article and approved it for submission.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of the First Affiliated Hospital of Chongqing Medical University.