
Abstract
Objective:
To compare the 1-year outcomes of patients with lumbar spinal stenosis treated with supervised physical therapy or unsupervised exercise.
Design:
A single-center randomized controlled trial with concealed allocation, blinded assessor and intention-to-treat analysis.
Setting:
Spine care center.
Subjects:
A total of 86 patients presenting with symptoms of neurogenic claudication caused by lumbar spinal stenosis.
Interventions:
The physical therapy group received supervised physical therapy sessions twice a week for 6 weeks and home exercise program. The home exercise group received 6-week home exercise program only.
Main measures:
The primary outcome was symptom severity on the Zurich claudication questionnaire at 1 year. Secondary outcomes included physical function, pain, health-related quality of life and the surgery rate after 1 year.
Results:
At 1 year, more patients in the physical therapy group than in the home exercise group achieved minimum clinically important differences in Zurich claudication questionnaire symptom severity (60.5% vs 32.6%; adjusted odds ratio [AOR] 4.3, [95% CI [1.5–12.3], P = 0.01); Zurich claudication questionnaire physical function (55.8% vs 32.6%; AOR 3.0 [1.1–8.1], P = 0.03); SF-36 bodily pain (48.8% vs 25.6%; AOR 2.8 [1.1–7.3], P = 0.03), and SF-36 general health (20.9% vs 7.0%; AOR 6.1 [1.1–33.0], P = 0.04). The surgery rate at 1 year was lower in the physical therapy than in the home exercise group (7.0% vs 23.3%; AOR 0.2 [0.04–0.9] P = 0.04).
Conclusions:
Supervised physical therapy produced greater improvements in symptom severity and physical function than unsupervised exercise and was associated with lower likelihood of receiving surgery within 1 year.
Introduction
Our previous study revealed that 6 weeks of supervised physical therapy for lumbar spinal stenosis provides greater short-term improvements in symptoms, physical function, and walking capacity than unsupervised exercise, although follow-up data have not been published. 1 Exercise therapy for patients with lumbar spinal stenosis has been reported to lead to better short-term outcomes in terms of disability and leg pain than no exercise. 2 However, little evidence is available that reports the 1-year effectiveness of exercise therapy,3,4 and it is unclear whether the therapeutic advantages of supervised physical therapy persist after completion of intervention.
Surgery for lumbar spinal stenosis is generally considered only if sufficiently bothersome symptoms persist after nonsurgical treatments, because symptoms are unlikely to worsen or neurological function to deteriorate rapidly. 5 A previous randomized controlled trial showed that physical therapy yielded similar effects to surgical decompression for lumbar spinal stenosis, although about half of the patients assigned to physical therapy crossed over to the surgery group. 6 The secondary analysis of the Spine Patient Outcomes Research Trial found that the patients with lumbar spinal stenosis who received physical therapy as nonsurgical treatment were less likely to cross over to the surgery group than those who did not receive physical therapy. 7 These findings suggest the possibility that physical therapy can help patients with lumbar spinal stenosis to avoid surgery. However, no study has investigated which type of exercise therapy can reduce surgery in patients with lumbar spinal stenosis. Therefore, it is unknown whether patients with lumbar spinal stenosis who receive supervised physical therapy are less likely to undergo surgery than those performing unsupervised exercise.
The aim of this study was to assess the 1-year follow-up outcomes of our previously published randomized controlled trial that compared supervised physical therapy with unsupervised exercise for patients with lumbar spinal stenosis. 1 We hypothesized that, even though the therapeutic advantages of supervised physical therapy on clinical outcomes decrease after completion of intervention, supervised physical therapy would be associated with a reduced likelihood of patients receiving surgery within 1 year compared with unsupervised exercise.
Methods
This study was a 1-year follow-up of a single-center, open-label, assessor-blinded previously published randomized controlled trial that compared supervised physical therapy with unsupervised exercise for patients with lumbar spinal stenosis. The study was approved by the Institutional Review Board at Wakayama Medical University (No. 1426) and was registered at the UMIN Clinical Trials Registry (UMIN000018981). All patients were required to provide written informed consent prior to participation. This study was conducted between September 2014 and May 2019 in Spine Care Center, Wakayama medical university Kihoku Hospital, in Japan.
Patients were recruited from Spine Care Center, Wakayama Medical University Kihoku Hospital. Screening for eligibility was carried out by one of three orthopedic spine surgeons in our Spine Care Center. To be eligible for enrollment in this study, the patients had to meet the following inclusion criteria: (1) presence of neurogenic intermittent claudication and pain and/or numbness in the lower extremities with or without low back pain; (2) lumbar spinal stenosis confirmed by magnetic resonance imaging (MRI); (3) a history of ineffective responses to pharmacotherapy for more than 3 months; (4) over 50 years of age; and (5) consent to be randomly assigned to the supervised physical therapy or home exercise program.
Patients meeting any of the following criteria were excluded: previous spine surgery, treatment with epidural steroid injection or selective nerve root infiltration, loss of bowel or bladder control, degenerative scoliosis, compression fractures at the level being considered for decompression, osteoarthrosis of the knee and/or hip, peripheral artery disorders, diabetes mellitus, cognitive impairment, or a history of psychiatric illness.
After screening for eligibility and providing informed written consent by a research assistant, participants were randomized to either the physical therapy or home exercise group as determined by random permuted block randomization with stratification by sex using an online statistical computer program (QuickCalcs; GraphPad Software, San Diego, CA, USA). A medical doctor who was not a contributor to the study conducted the randomization process and assigned participants to the interventions via telephone to a research assistant who obtained informed consent. The treating physical therapists were unaware of the block size. Allocation concealment was preserved until the first treatment appointment.
The primary outcome was symptom severity on the Zurich claudication questionnaire 8 at 1 year. Secondary outcomes included surgery rate after 1 year; physical function and satisfaction on the Zurich claudication questionnaire, back pain; leg pain, and leg numbness indicated using a numerical rating scale; 9 and scores on the Japanese Orthopedic Association Back Pain Evaluation Questionnaire, 10 Medical Outcomes Study 36-Item Short-Form General Health Survey (SF-36), 11 hospital anxiety and depression scale, 12 pain catastrophizing scale, 13 pain anxiety symptoms scale-20, 14 and Tampa scale for kinesiophobia-11 15 at 1 year.
The Zurich claudication questionnaire satisfaction subscale was modified from the original scale by replacing the word “surgery” with the word “rehabilitation” in each question. 3 The objective walking distance was measured using a self-paced walking test 16 at the baseline and immediately after completion of the 6-week program. Two authors who were blinded to group allocation and were not involved in the treatments collected the self-reported completed questionnaires and the results of the walking tests at the baseline, 6-week and 1-year follow-up.
The severity of stenosis was examined using a seven-grade classification based on the morphology of the dural sac on T2 axial MRI of the lumbar axial spine. 17 Two orthopedic spine surgeons who were certified as specialists by the Japanese Orthopedic Association and Japanese Society for Spine Surgery and Related Research determined the grade of the dura mater compression and reached consensus for all patients.
Patients assigned to the physical therapy group received supervised physical therapy sessions twice a week for 6 weeks. The physical therapy sessions comprised manual therapy, individually tailored stretching and strengthening exercises, cycling, and body weight-supported treadmill walking. The manual therapy procedures and individually tailored stretching and strengthening exercises were prescribed according to the underlying impairments identified by the treating physical therapist. The manual therapy procedures included manipulation, stretching, and massage of the thoracic and lumbar spine, pelvis, and lower extremities. The individually tailored stretching and strengthening exercises included those for the trunk and lower extremities. Both cycling and body weight-supported treadmill walking were performed for up to 20 minutes or as tolerated by the patients. Additional information about this program is available. 1
Patients assigned to the home exercise group were instructed how to perform the home exercise program under the supervision of the physical therapist at the first visit. After the first visit, patients in the home exercise group visited a physical therapist once a week for 6 weeks to monitor whether they performed home exercise. The manual therapy and any exercises under the supervision were not performed in the home exercise group.
All patients in both groups were prescribed the home exercise program comprising lumbar flexion and strengthening exercises and walking. Lumbar flexion exercises included three 30-second bouts of both single and double knee-to-chest exercises, and strengthening exercises consisted of ten 6-second bouts of trunk raises and bridging in the supine position, and a four-point kneeling exercise at least twice daily. The patients recorded their exercise in a diary and used a pedometer during the 6-week intervention. All patients were allowed to continue with previously prescribed medications, but were not allowed to change the type or dosage of these medications during the 6-week treatment period.
Sample size was estimated based on the primary outcome measure, Zurich claudication questionnaire symptom severity. The required sample size (n = 86) was determined a priori and was based on the ability to detect a difference between the treatment groups equivalent to the previously determined minimum clinically important difference (MCID) of 0.36 points for the Zurich claudication questionnaire symptom severity scale 18 and assuming a standard deviation of 0.5419,20 with power set at 80% (alpha = 5%) and allowing for a drop-out rate of 20%.
Linear mixed models were used to identify differences between groups in the improvement in patient-reported outcome scores over time after controlling for age, sex, body mass index, duration of symptoms, baseline Zurich claudication questionnaire symptom severity and physical function scores, and baseline self-paced walking test result. 21
Responder analyses was used to show the percentage of patients achieving MCID values using logistic regression models after adjusting for the same variables as those used in the linear mixed models. The MCID values used were based on the previously published values for the Zurich claudication questionnaire (0.36 points for symptom severity and 0.10 points for physical function subscales), the numerical rating scale (1.25 points for back pain and 1.5 points for leg pain), and each domain of the Japanese Orthopedic Association Back Pain Evaluation Questionnaire (20 points).18,22 The MCID for other outcomes was defined as a ⩾30% improvement between the baseline and follow-up scores. The surgery rate within 1 year after enrollment was compared between groups. Patients who had dropped out with missing follow-up data were counted as nonresponders for all outcomes or having had surgery according to the intention-to-treat principle.
The Fragility Index was also used to determine the robustness of statistically significant result on primary outcome and surgery rate. The Fragility Index is the minimum number of patients who must be moved from the nonevent group to the event group to turn a significant result nonsignificant. 23 The surgery rate and Fragility Index value for surgery rate were also calculated for the as-treated analysis.
All statistical tests were two-tailed, and the significance level was fixed at 0.05 for all analyses. The statistical analysis was performed based on intention-to-treat analysis using JMP Pro (version 14; SAS Institute, Cary, NC, USA).
Results
A toal of 121 patients were screened between September 2014 and May 2018, and 86 patients (39 men and 47 women, average age 72.7 years) were recruited to this study. Follow-up data were available for 84 (98%) patients at the 6-week follow-up and 68 (79%) patients at 1 year (Figure 1). One patient in the physical therapy group and nine patients in the home exercise group underwent decompression surgery during the 1-year follow-up period. In addition to those who underwent surgery during the 1-year follow-up period, two patients in the physical therapy group and three patients in the home exercise group did not answer the self-reported questionnaire at 1 year.
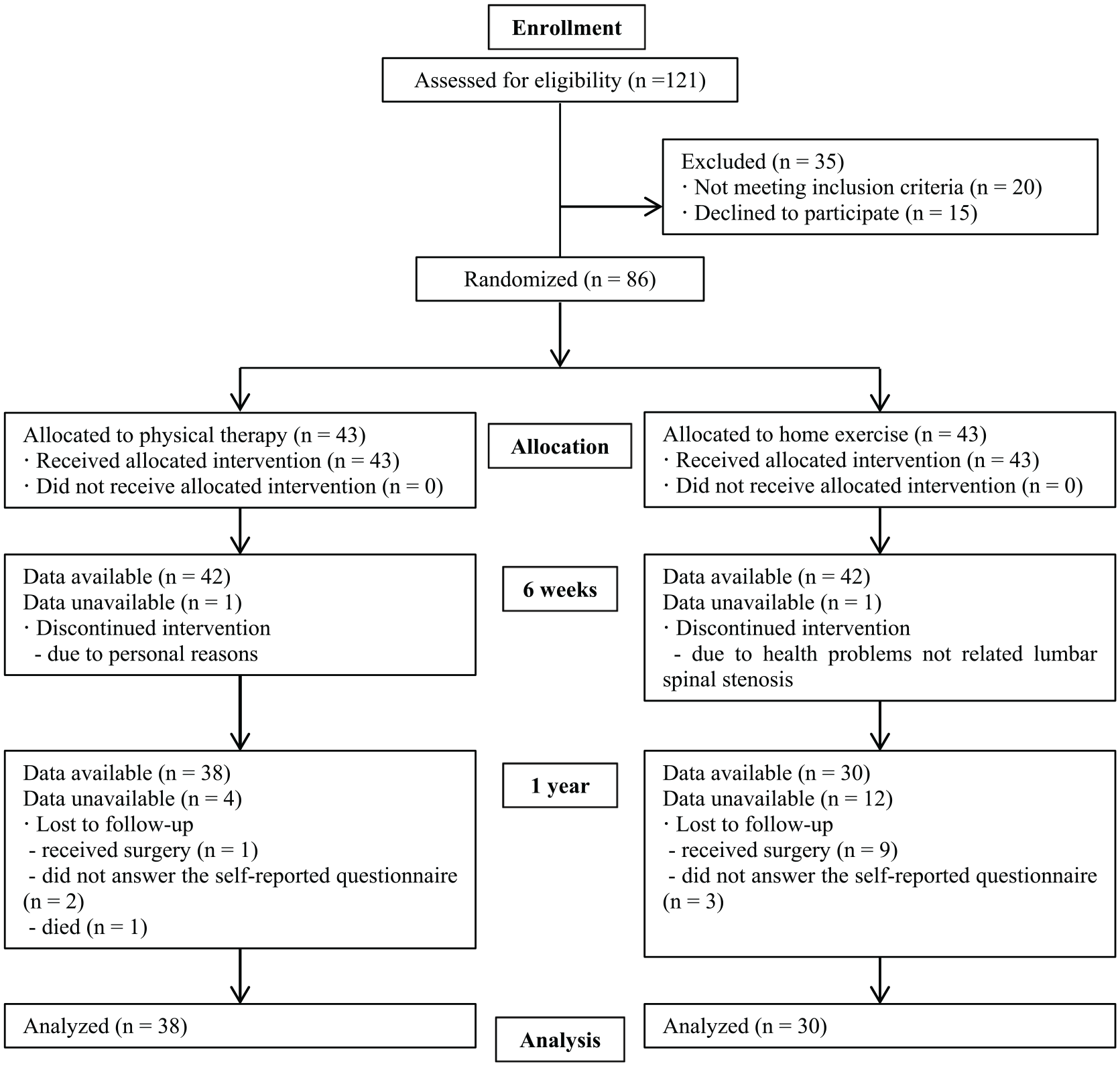
Flowchart.
At the baseline, age, sex, body mass index, duration of symptoms, MRI findings, and the outcome measures did not differ significantly between groups (P ⩾ 0.05; Tables 1–3).
Baseline characteristics of patients.
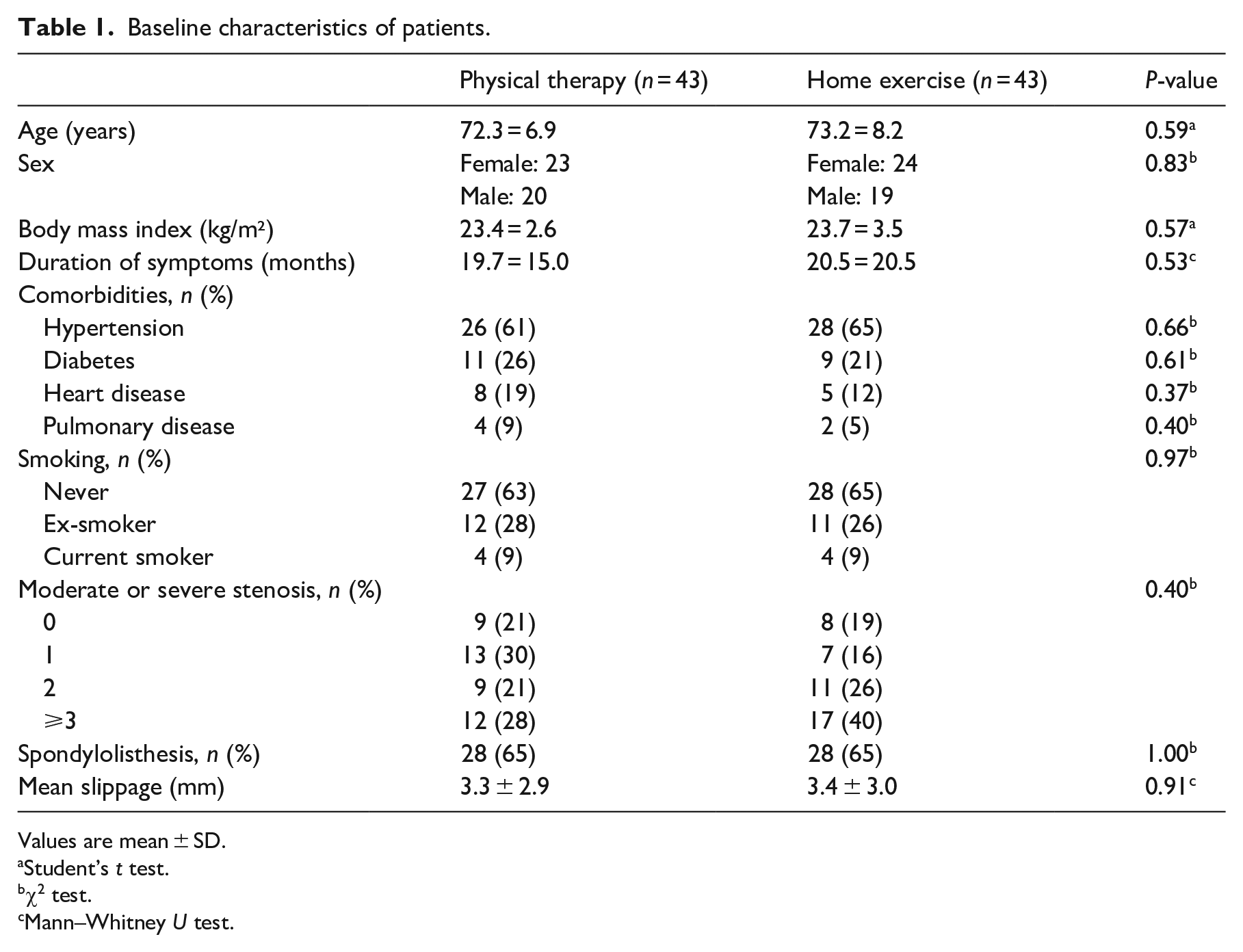
Values are mean ± SD.
Student’s t test.
χ2 test.
Mann–Whitney U test.
Number of patients with spinal stenosis at each spinal level.
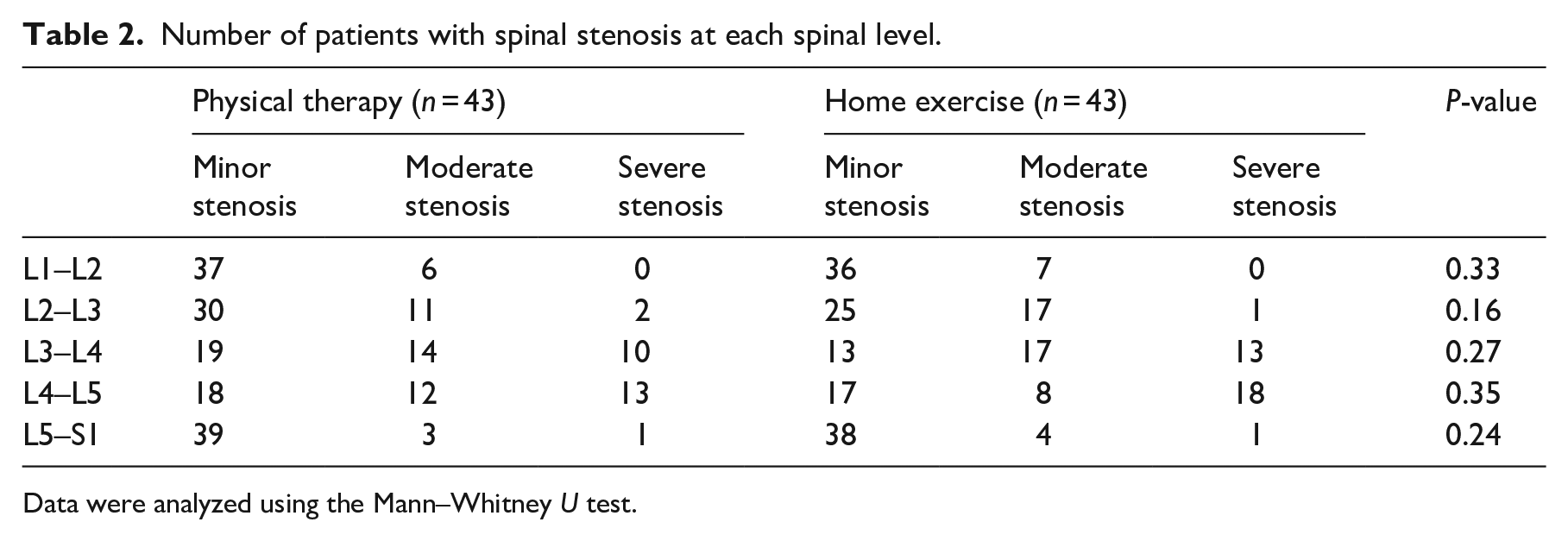
Data were analyzed using the Mann–Whitney U test.
Clinical outcome data at baseline, 6 weeks, and 1 year.
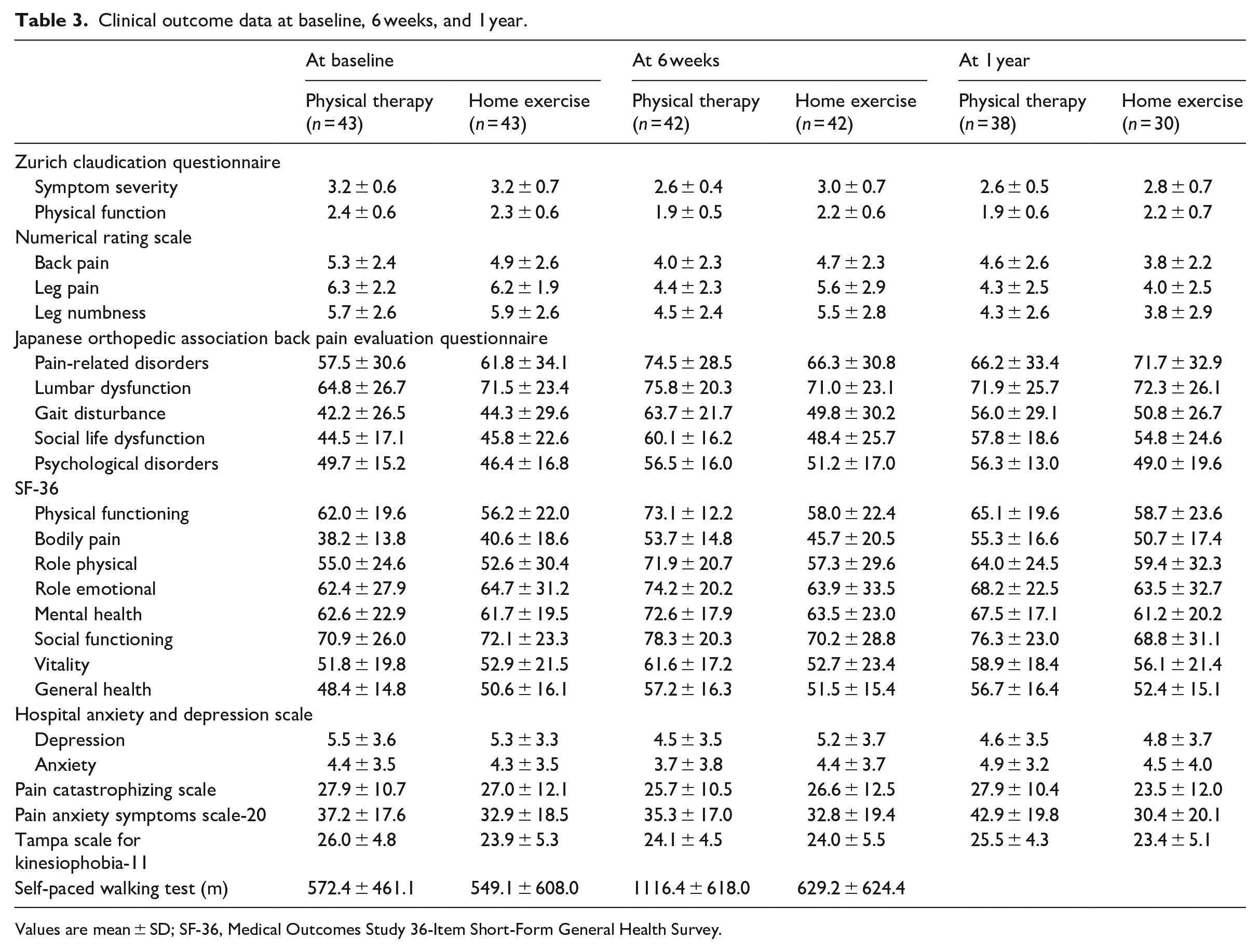
Values are mean ± SD; SF-36, Medical Outcomes Study 36-Item Short-Form General Health Survey.
Analysis of the mean changes after 1 year showed that the physical therapy group reported significant improvements compared with the home exercise group in Zurich claudication questionnaire symptom severity and Zurich claudication questionnaire physical function (Table 4). The home exercise group showed significant improvement in pain anxiety symptoms scale-20 score compared with the physical therapy group.
Comparison of clinical outcomes between the physical therapy and home exercise groups at 6 weeks and 1 year.
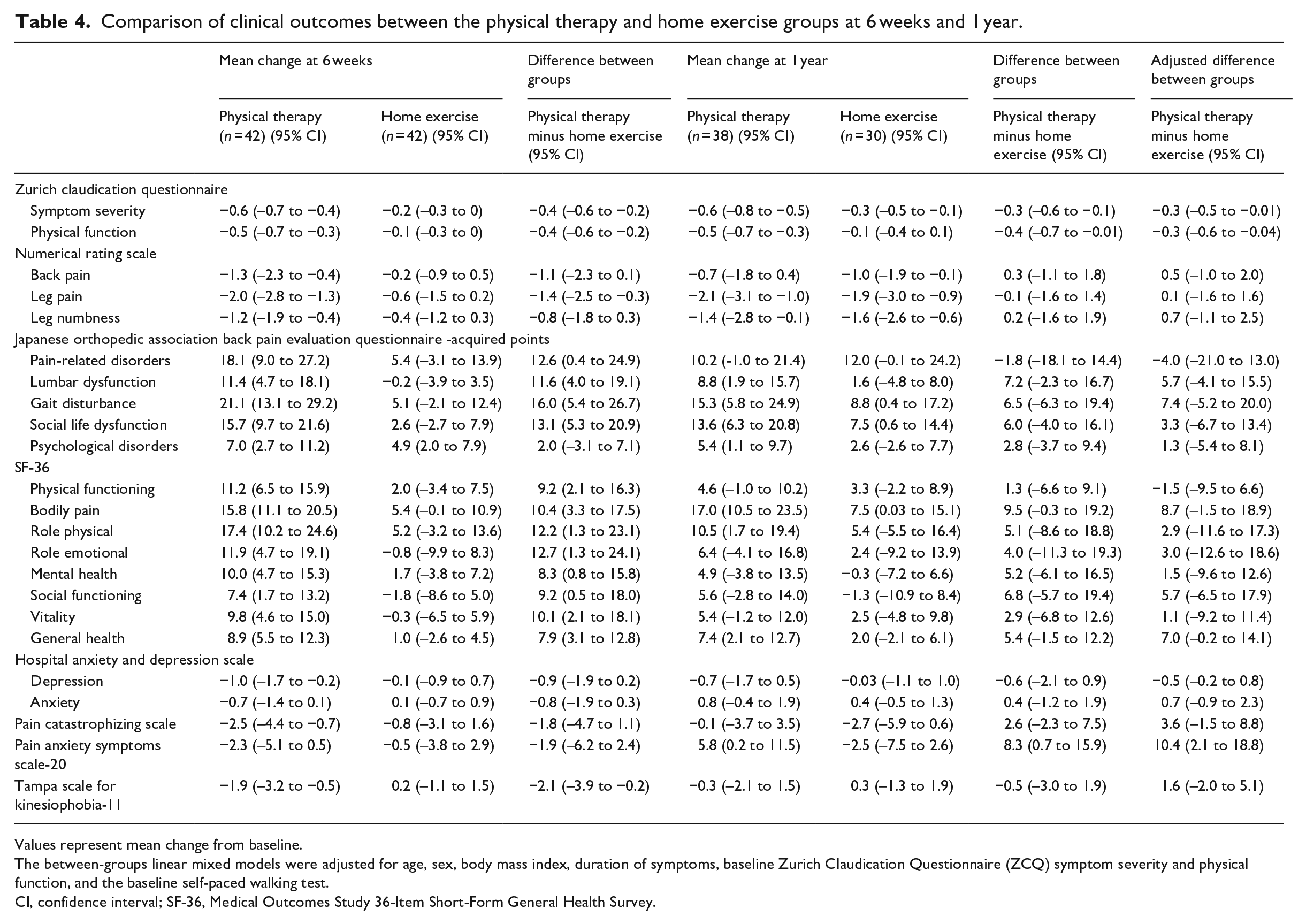
Values represent mean change from baseline.
The between-groups linear mixed models were adjusted for age, sex, body mass index, duration of symptoms, baseline Zurich Claudication Questionnaire (ZCQ) symptom severity and physical function, and the baseline self-paced walking test.
CI, confidence interval; SF-36, Medical Outcomes Study 36-Item Short-Form General Health Survey.
At 1 year, a greater percentage of patients in the physical therapy group compared with the home exercise group achieved MCID values in Zurich claudication questionnaire symptom severity, Zurich claudication questionnaire physical function, Zurich claudication questionnaire satisfaction, Japanese Orthopedic Association Back Pain Evaluation Questionnaire lumbar dysfunction, SF-36 bodily pain, SF-36 general health, and hospital anxiety and depression scale depression (Supplemental Table 1). The surgery rate at 1 year was lower in the physical therapy group than in the home exercise group in the intention-to-treat analysis (7.0% vs 23.3%; adjusted odds ratio 0.2 [0.04–0.9], P = 0.04) and the as-treated analysis (2.3% vs 20.9%; adjusted odds ratio 0.03 [0.002–0.5], P = 0.02). The Fragility Index values were 2 for Zurich claudication questionnaire symptom severity, 0 for the surgery rate in the intention-to-treat analysis, and 2 for the surgery rate in the as-treated analysis.
Discussion
In this study, 1 year after the 6-week supervised physical therapy or home exercise for patients with lumbar spinal stenosis, a higher percentage of patients achieved MCIDs in symptom severity, physical function, lumbar dysfunction, bodily pain, general health, and depression compared with the home exercise group. Patients with lumbar spinal stenosis who received supervised physical therapy were less likely to undergo surgery within 1 year.
Our paper describing the early results 1 showed a higher percentage of patients achieved MCIDs in leg pain, Japanese Orthopedic Association Back Pain Evaluation Questionnaire pain-related disorder and gait disturbance, and physical functioning as assessed by the SF-36 compared with the home exercise group at 6 weeks. However, these differences were not observed at 1 year. A previous randomized controlled trial that compared medical care, group exercise, and manual therapy with individualized exercise delivered as a chiropractic or physical therapy intervention for patients with lumbar spinal stenosis reported that the 6 weeks of chiropractic/physical therapy intervention had better short-term outcomes for Zurich claudication questionnaire score and walking capacity at 2 months, but that none of the interventions were superior to each other at 6 months. 21 One possible explanation is that patients in the control groups showed improvement after the 6-week intervention because the natural course of disease is favorable in one-third to one-half of patients with clinically mild to moderate lumbar spinal stenosis. 24
By contrast, another randomized controlled trial that compared a 6-week structured comprehensive training program with a 6-week self-directed program for patients with lumbar spinal stenosis reported that Zurich claudication questionnaire physical function and SF-36 physical functioning and bodily pain scores showed greater improvements after the comprehensive program at 1 year. 4 In that study, the structured comprehensive training program included manual therapy, an exercise program, and a cognitive behavioral approach. 4 In our study, the psychological factors measured by the pain catastrophizing scale, pain anxiety symptoms scale, and Tampa scale for kinesiophobia-11 did not improve significantly in either group at 1 year. Psychological factors such as pain catastrophizing and fear-avoidance beliefs can influence pain and disability, and can contribute to poor outcomes in people with lumbar spinal stenosis.25,26 Therefore, it is possible that physical therapy that includes the management of psychological factors may help to sustain the therapeutic effects and improve clinical outcomes in patients with lumbar spinal stenosis.
Our study showed that the rate of decompression surgery up to 1 year after the 6-week exercise intervention was lower in patients with lumbar spinal stenosis who received supervised physical therapy compared with those who received home exercise alone. However, the Fragility Index value of the surgery rate was 0 which indicates the lack of robustness. Although one patient in the physical therapy group and nine patients in the home exercise group underwent decompression surgery, two patients in the home exercise group and one patient in the home exercise group who had dropped out were counted as having had surgery in the intention-to-treat analysis. The Fragility index value in the as-treated analysis was 2 which indicates that if two patients in physical therapy group received decompression surgery, the difference between groups lose statistical significance (P ⩾ 0.05). The Fragility Index is correlated with total sample size and total number of events. 23 A previous systematic survey showed that the median Fragility Index values in randomized controlled trials of spine surgery interventions was 2 and the statistical significance of results was frequently fragile because of relatively small sample sizes with few outcome events. 27 It is important to take into account the sample size and number of events when interpreting the findings from this study. Several randomized controlled trials have been conducted to confirm the efficacy of exercise therapy for patients with lumbar spinal stenosis,3,4,21 yet it is unknown whether exercise therapy can help to avoid decompression surgery. We believe that our findings provide information that will be important to making decisions about the treatment of patients with lumbar spinal stenosis in clinical practice.
This study has some limitations. The objective assessments were not performed at the 1-year follow-up, although the self-paced walking test was used to assess walking distance and the pedometer was used to assess physical activity at the baseline and for the 6-week intervention. 1 We did not assess compliance with the home exercise programs after the 6-week intervention, which may have identified differences between the physical therapy and home exercise groups, although all patients in both groups were prescribed the same programs comprising lumbar flexion and strengthening exercises and walking.
The 1-year follow-up period was insufficient for evaluating the long-term outcomes and whether a 6-week physical therapy intervention can reduce the likelihood of receiving surgery. Previous long-term follow-up randomized controlled trials that have evaluated physical therapy showed that clinical outcomes remain stable up to 2 years after a 6-week physical therapy intervention.3,6 Our previous retrospective study showed that the patient-reported outcomes of these lumbar spinal stenosis patients who were followed up after the 6-week physical therapy intervention were maintained or improved and did not differ significantly from those in patients who underwent surgery after less successful physical therapy at the 2-year follow-up. 20 Further trials with longer follow-up periods are required to determine the efficacy of physical therapy for patients with lumbar spinal stenosis.
Differences in exercise volume between the physical therapy and home exercise group might have influenced the results of this study more than did level of supervision. If we had ensured a similar volume of exercise, we may have been able to identify more clearly the differences between supervised and unsupervised exercise. Finally, the additional effect of manual therapy might affect the therapeutic advantages of supervised physical therapy, because patients in the physical therapy group received manual therapy along with supervised exercise sessions. In previous randomized controlled trials evaluating effectiveness of exercise therapy, manual therapy was also performed at exercise sessions.3,4,21 However, the differences between the experimental and control group were not only receiving manual therapy, but also different exercise programs. Therefore, the additional effect of manual therapy is uncertain because of the lack of an appropriate control group. Future trials are needed to compare supervised exercise in addition to manual therapy with supervised exercise alone.
This study show that supervised physical therapy produced greater improvements in symptom severity and physical function than unsupervised exercise and was associated with lower likelihood of receiving surgery within 1 year. Our findings suggest that patients with lumbar spinal stenosis should be managed with an intensive and supervised exercise program to obtain the maximum benefits from exercise therapy. However, the therapeutic advantages of supervised physical therapy decreased during 1-year follow-up period. Furthermore, the psychological factors such as pain catastrophizing and fear-avoidance beliefs did not improve significantly in either group at 1 year. Future study should focus on whether physical therapy that includes the management of psychological factors can help to sustain the therapeutic effects and improve clinical outcomes over the natural course of the disease in patients with lumbar spinal stenosis.
Clinical messages
Six weeks of supervised physical therapy for patients with lumbar spinal stenosis produced significant improve-ments in symptom severity and physical function compared with unsupervised exercise at the 1-year follow-up.
Patients with lumbar spinal stenosis who received supervised physical therapy were less likely to undergo surgery within 1 year.
Supplemental Material
sj-pdf-1-cre-10.1177_0269215520986688 – Supplemental material for Supervised physical therapy versus unsupervised exercise for patients with lumbar spinal stenosis: 1-year follow-up of a randomized controlled trial
Supplemental material, sj-pdf-1-cre-10.1177_0269215520986688 for Supervised physical therapy versus unsupervised exercise for patients with lumbar spinal stenosis: 1-year follow-up of a randomized controlled trial by Masakazu Minetama, Mamoru Kawakami, Masatoshi Teraguchi, Ryohei Kagotani, Yoshimasa Mera, Tadashi Sumiya, Masafumi Nakagawa, Yoshio Yamamoto, Sachika Matsuo, Nana Sakon, Tomohiro Nakatani, Tomoko Kitano and Yukihiro Nakagawa in Clinical Rehabilitation
Footnotes
Author contributions
MM, MK MN, and YY initiated this study and designed it. MT, RK, YM, SM, NS, and TN collected the data. MM and TK organized the data and did the statistical analysis. MK, TS, and YN monitored the progress. MM and YN supervised the research, advised in all steps of the research. MM wrote the manuscript and all co-authors contributed to critically revising it.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.