
Abstract
Objective:
To investigate an intensive asynchronous computer-based treatment delivered remotely with clinician oversight to people with aphasia.
Design:
Single-blind, randomized placebo-controlled trial.
Setting:
Free-standing urban rehabilitation hospital.
Participants:
Adults with aphasia (at least six months post-onset).
Interventions:
Experimental treatment was Web ORLA® (Oral Reading for Language in Aphasia) which provides repeated choral and independent reading aloud of sentences with a virtual therapist. Placebo was a commercially available computer game. Participants were instructed to practice 90 minutes/day, six days/week for six weeks.
Main measures:
Change in Language Quotient of the Western Aphasia Battery-Revised from pre-treatment to post-treatment and pre-treatment to six weeks following the end of treatment.
Results:
32 participants (19 Web ORLA®, 13 Control) completed the intervention and post-treatment assessment; 27 participants (16 Web ORLA®, 11 Control) completed the follow-up assessment six weeks after treatment had ended. Web ORLA® treatment resulted in significant improvements in language performance from pre-treatment to immediately post-treatment (X = 2.96; SD = 4.32; P < 0.01; ES = 0.68) and from pre-treatment to six weeks following the end of treatment (X = 4.53; SD = 3.16; P < 0.001; ES = 1.43). There was no significant difference in the gain from pre-treatment to post-treatment for the Web ORLA® versus Control groups. However, the Web ORLA® group showed significantly greater gains at the six-week follow-up than the control group (X = 2.70; SD = 1.01; P = 0.013; ES = 1.92).
Conclusion:
Results provide evidence for improved language outcomes following intensive, web-based delivery of ORLA® to individuals with chronic aphasia. Findings underscore the value of combining clinician oversight with the flexibility of asynchronous practice.
Rapid advances in technology and the growing popularity of digital devices have increased the potential availability of telerehabilitation and other computer-based applications for individuals with aphasia. These offer a cost-effective way to extend therapy beyond the hospital and clinic, allowing individuals with aphasia to receive therapy at home. Previous studies have established the feasibility of telerehab and the relative comparability of computer-delivered to clinician delivered programs. 1 However, the evidence for aphasia telerehabilitation is still emerging 2 and to date has been limited to case studies,3–6 small single case experimental design studies, 7 and preliminary trials. 8 As more telerehab applications become available, there is a critical need to demonstrate the efficacy of such services, with attention not only to the mode of delivery, but also the specific components of the speech-language treatment and the outcomes of interest.
In contrast to synchronous telerehabilitation services, self-managed computer-based programs permit asynchronous practice that is more intensive. For example, Des Roches and colleagues investigated outcomes from ten weeks of their iPad-based software, Constant Therapy, in a sample of 51 individuals with aphasia. 9 All participants attended a weekly one hour in clinic session. Participants randomized to the experimental group had the opportunity to practice an additional six hours (one hour per day) at home. Not surprisingly, the experimental group made more improvement than the control group on standardized language and cognitive tests, suggesting that more practice with the iPad therapy tasks resulted in greater changes. Palmer and colleagues also evaluated a self-managed computerized treatment for aphasia in the largest multicenter randomized controlled trial of computerized treatment for aphasia to date.10,11 Participants receiving computer-based word finding treatment in addition to usual care demonstrated clinically significant improvements in word finding that were greater than the improvements made by the group who received usual care or the attention control group. While improvements did not generalize to conversation, results lend support for the efficacy of their specific computer-based program for word-finding in aphasia.
An interesting finding from both of these studies was the amount of practice actually completed by participants. Des Roches et al. note that the treatment provided during the in clinic session was approximately 41 minutes, or 68.1% compliant with the ideal one hour of clinic time. 9 Furthermore, participants in the experimental group practiced at home for an average of four hours and eight minutes each week, which is 68.7% compliant with the instructed six hours/week of practice. In the Palmer et al. study, 20–30 minutes of daily practice on the computerized program was recommended over a six-month period. 11 However, a mean of 28 hours of practice was recorded, suggesting participants practiced approximately one hour a week, which is 43% compliant with the recommended amount. Because dosage and intensity are critical aspects of aphasia treatment that drive speech-language outcomes, programs that facilitate greater compliance with home practice are of interest.
Web-based Oral Reading for Language in Aphasia (Web ORLA®)
Individuals with aphasia may be more compliant with a computerized program that offers the experience of clinician interaction, without the potential for that contact to detract from critical treatment time. Web-Based Oral Reading for Language in Aphasia (ORLA®) is a program that uses an animated virtual therapist to deliver oral reading treatment remotely via the internet.
During ORLA® treatment the person with aphasia repeatedly reads aloud sentences or paragraphs, first in unison with the clinician, and then independently.12,13 ORLA® focuses on connected discourse rather than single words, permitting the modeling of more natural rhythm and intonations. It also allows practice on a variety of grammatical structures, rather than just one specific grammatical form. Preliminary studies have indicated that ORLA® is efficacious when provided by a speech-language pathologist.12,14 The treatment has been computerized using digital therapist technology that allows the individual with aphasia to read aloud, and ultimately speak, sentences at the same time as the words are produced by an anthropomorphically accurate virtual therapist. The virtual therapist produces natural speech with correct movements of the speech articulators, repeatedly reading aloud with the patient in exactly the same way as a therapist would administer ORLA®.
In this web-based version, individuals with aphasia work independently on their home computer with oversight from the SLP. The SLP monitors participant use remotely either in real time during the treatment session or after the session at a convenient time. The system also permits the therapist to interact with participants in real time via audio and or video messaging.
We aimed to evaluate the efficacy of Web ORLA® for improving language performance in individuals with chronic aphasia in a pilot randomized control trial in which participants were randomly assigned to Web ORLA® or a control group. A commercially available game, Bejeweled 2©, by PopCap, was selected as the control because it was computerized, could be accessed for the same duration and frequency as Web ORLA®, and because it did not directly target verbal skills.
We hypothesized that Web ORLA® would result in significantly improved language performance, and that improvements would be maintained for six weeks after the end of treatment, as measured by the primary outcome measure, the Western Aphasia Battery-Revised Language Quotient (WAB-R LQ). The WAB-R LQ was selected because it is a comprehensive measure that addresses the modalities of auditory comprehension, oral expression, reading comprehension and writing – modalities that have been shown to improve with ORLA®. We also hypothesized that the Web ORLA® group would demonstrate significantly better language gains than the control group at both post-treatment and at six weeks following the end of treatment.
Methods
Experimental design
A single blind, randomized placebo-controlled design was used to evaluate the efficacy of Web ORLA® (ClinicalTrials.gov identifier: NCT04413136). The research speech-language pathologist who administered and scored the assessment protocol was blinded to the participants’ assigned group. The study was approved by the Institutional Review Board of Northwestern University (Protocol Record STU00000150).
Participants
Participants were recruited from across the United States. Study procedures, including pre- and post-treatment assessments and computer training, took place at a free standing urban rehabilitation hospital. Participants completed the experimental treatment and control computer activity remotely at home from loaned laptop computers. The inclusion/exclusion criteria were adults with chronic aphasia (at least six-month post onset) resulting from a single left-hemisphere stroke, absence of active substance abuse, significant psychological problems, or neurological conditions other than stroke; native speakers of English; sufficient auditory and visual acuity to interact with a laptop; and not receiving other speech/language treatment for at least one month prior to or during the study.
Participants were randomized in a 3:2 ratio to one of two conditions: Web ORLA® and control treatment. Sample size was determined using a five point difference between groups 15 and from prior research that revealed clinically meaningful changes on the WAB-R Aphasia Quotient (AQ) following a computer version of ORLA®. 16 The primary outcome measure for the current study, the WAB-R Language Quotient (LQ), is highly correlated with the AQ. 17 Stratified permuted block randomization was used with the stratifying variable of pre-treatment aphasia severity as measured by the WAB-R Aphasia Quotient (AQ) and using a cut-off of 60 to ensure balance of severity in each treatment arm. The randomization list was determined a priori by the statistician (KYK). Following confirmation of eligibility criteria including aphasia severity, participants were assigned to the experimental or control conditions sequentially from this list.
Intervention
Web-based ORLA® was the experimental intervention. Participants were seated at a 13-inch laptop computer with an audio-headset, which presented auditory stimuli and captured recordings of participants’ verbal output. The participant was presented with three to five word (level 1) or eight to ten word (level 2) sentences, depending upon the severity of the aphasia. Each sentence was chosen by the software program at random from a group of 150 sentences. The participant was instructed to look, listen, and point to words spoken by the virtual therapist, read highlighted words aloud, and then read the sentence aloud, both chorally with the virtual therapist and independently. Figure 1 shows the digital therapist with a sample level 1 sentence. The word being spoken is highlighted in green. Supplemental Appendix A shows the program features, instructions read aloud by the virtual therapist and the participant response.
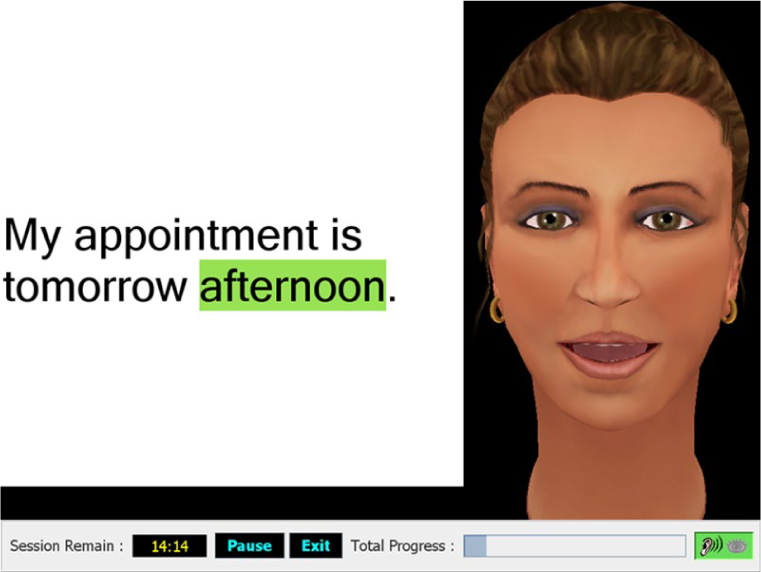
Screen shot of Web ORLA® level 1 sentence stimulus. The ear and eye icons displayed on the right bottom corner indicate to the participant when the research speech-language pathologist is observing remotely.
Web ORLA® allows interaction with the research SLP who is able to provide both synchronous and asynchronous monitoring of practice and real-time adjustments to the program remotely. For example, when both participant and SLP are online, messaging can be initiated by either party. The SLP can monitor participants by clicking on “ear” and “eye” icons to listen to streaming audio and/or watch streaming video of the participant’s practice. The SLP can temporarily pause the program to initiate conversation using audio, video or text messaging. Additionally, adjustments to the sentence level and/or rate of sentence practice can be made remotely. The participant can also click on one of these icons to initiate communication with the monitoring SLP. Participants’ practice information is available asynchronously in summative formats searchable by session, day and weekly periods.
The control group used a commercially available computer game, Bejeweled 2©, by PopCap. This game was selected as the control because its play does not require verbal production, auditory processing, or reading comprehension. Bejeweled has been used as the “non-language mind game” in recent research investigating computer delivered language therapy. 18 Participants used loaned 13-inch laptop computers to access the Bejeweled© interface, which displays an 8 × 8 grid of gems of varying shapes and colors. The objective is to match three gems of the same color and shape to score points and advance to more difficult levels (see Figure 2).

Bejeweled, selected as the placebo, attention control computer task.
Procedures
Participants were evaluated at baseline prior to treatment (week minus two), immediately following the six weeks of treatment (week seven) and at 6 weeks following the end of treatment (week 13) to assess maintenance.
The individual with aphasia, typically accompanied by caregiver or family member, participated in two sessions of in-person computer training following baseline evaluation and randomization. Participants in the Web ORLA® arm were oriented to the laptop and program log in, the software features, including the icons indicating that the SLP was online and how to initiate communication with the SLP. Participants were instructed on how to follow the virtual therapist through the ORLA® sentence practice sequence. The SLP guided the participant through the treatment sequence until he or she could follow the virtual therapist’s steps independently. The family member or caregiver was trained to set up the laptop, headset and webcam for the person with aphasia to complete the computer practice at home.
Training on the Bejeweled program consisted of orientation to the laptop, accessing Bejeweled 2© via internet web browser, using a mouse or touch pad to move gems, and the objective of the game. They were provided instruction on various features of the program, including the “Hint” button that highlights a gem that can be moved to create a match and the box at the top left corner of the screen that tracks points.
Participants in both arms were provided with aphasia-friendly written instructions with pictures and screen shots for logging into the laptop, using the various programs, completing the practice logs, and trouble-shooting technical issues (e.g., audio or recording). Both groups were instructed to practice 90 minutes a day, six days a week (i.e. nine hours of computer treatment per week) for a total of six weeks. Participants could practice either three 30-minute session per day or two 45-minute sessions per day, six days a week. Participants tracked their computer time on practice logs. Practice time was also recorded by the Web ORLA® program, so that participant-recorded and computer-recorded practice logs could be compared for accuracy and compliance.
During the six-week treatment period, participants in both arms had a weekly phone call with the SLP to check in on their practice. Participants in the Web ORLA® group had additional opportunities to interact with the SLP remotely via the software if assistance was requested or when they practiced during business hours and the SLP happened to also be online at the same time. As previously described, participants could communicate with the SLP via two-way messaging, and the SLP could pause the program to answer questions and/or make adjustments to the program as appropriate. Participants in the Bejeweled group did not interact with the SLP between weekly phone check-ins. Participants did not have access to either the Web ORLA® or the Bejeweled programs between post treatment and follow-up visits, and during this six-week period of time, the SLP had no interaction with participants in either group.
Outcomes
Western Aphasia Battery-Revised Language Quotient (WAB-R LQ)
The primary outcome measure was the WAB-R Language Quotient, 17 which encompasses the Reading and Writing subtests in addition to Spontaneous Speech, Comprehension, Repetition, and Naming. LQ scores range from 0 to 100.
Analyses
To assess whether Web ORLA® resulted in improvement in language performance, the mean change in WAB-R LQ scores from pre-treatment to post-treatment was compared to zero for those randomized to web-based ORLA®, using a two-sided paired t-test. To assess whether improvements in language performance were maintained at follow-up, the mean change in WAB-R LQ scores from pre-treatment to the six-week follow-up were calculated and compared to zero using a two-sided paired t-test. To assess whether Web ORLA® resulted in greater gains in language performance than the control treatment, the mean change in WAB-R LQ scores from pre-treatment to post-treatment and pre-treatment to follow-up for those randomized to Web ORLA® was compared to the mean change in WAB-R LQ scores for those randomized to Bejeweled using a two-sided two-sample t-test.
Results
Forty-one participants were recruited and assessed for eligibility between February, 2008 and July, 2010. Recruitment was stopped when the sample size was achieved, taking into account a potential 20% drop out. Figure 3 displays the progression through the study. 35 participants met eligibility and were randomized. 32 of these participants (19 Web ORLA®, 13 Control) completed the study procedures and 27 participants (16 Web ORLA®, 11 Control) returned to complete the follow-up assessments. Table 1 shows participant characteristics for the Web ORLA® and Bejeweled groups. There were no significant differences between the groups (P > 0.05) on demographic variables including sex, age, handedness, education, time post onset of stroke, and severity and type of aphasia.
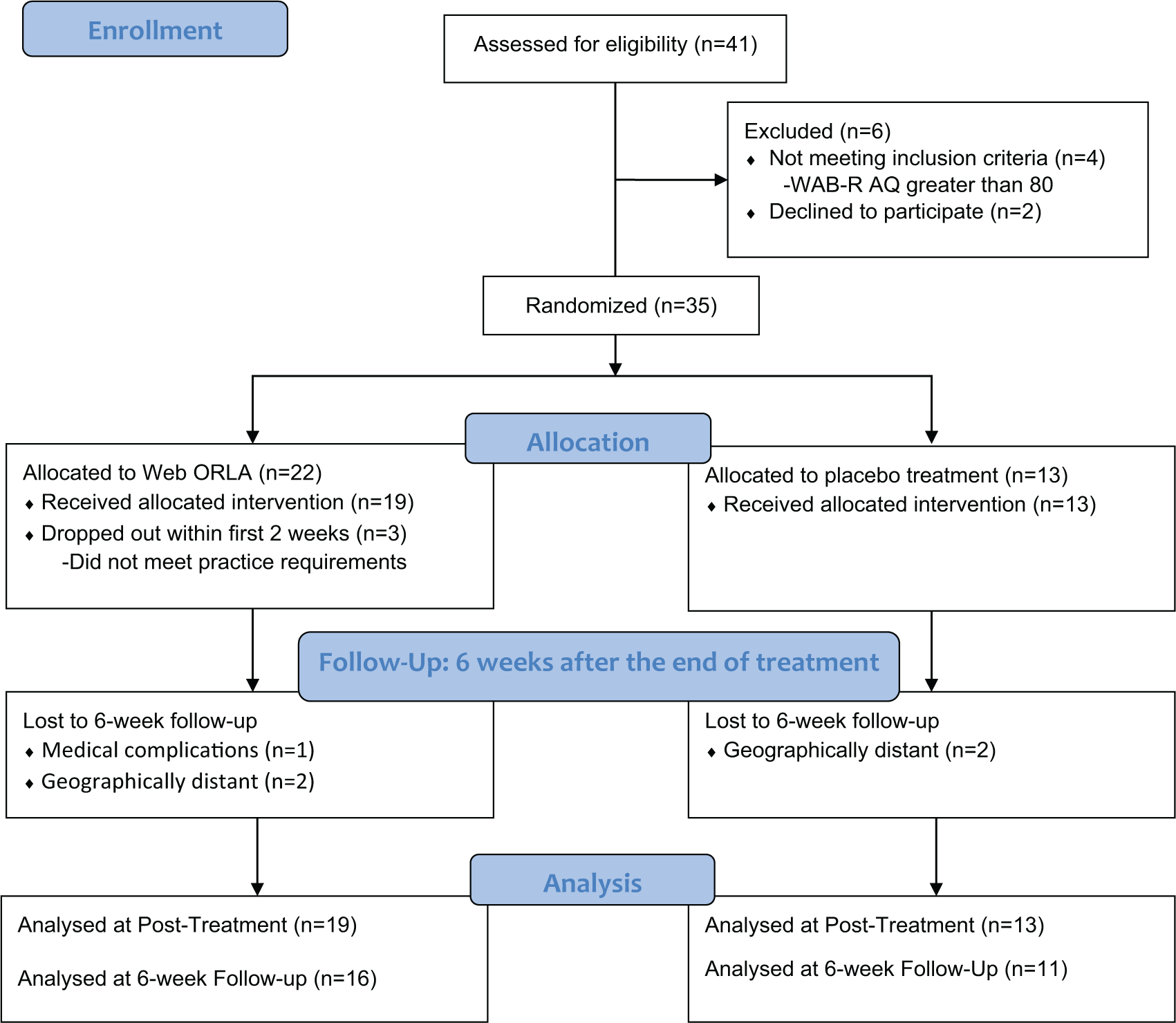
CONSORT diagram of participants’ progress through trial.
Participant characteristics across Web ORLA® and Bejeweled groups.
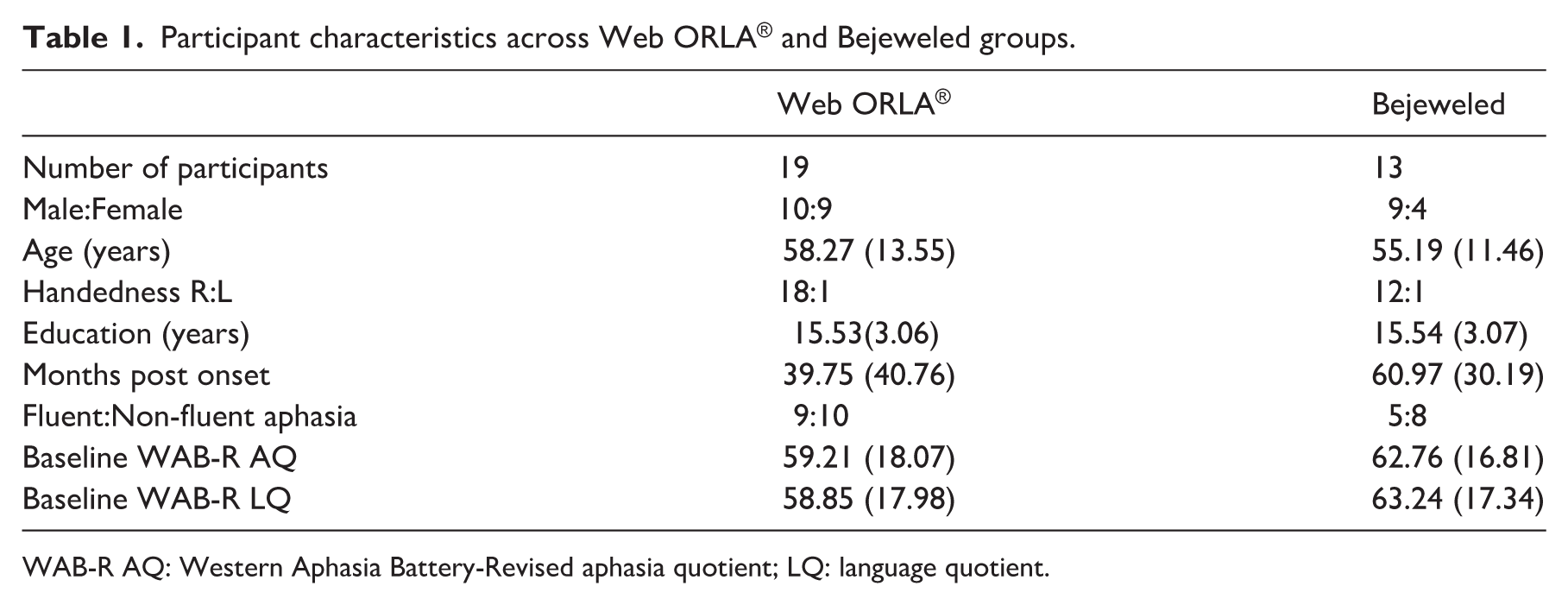
WAB-R AQ: Western Aphasia Battery-Revised aphasia quotient; LQ: language quotient.
Practice time
There was no significant difference between groups in the amount of time that participants practiced weekly on the computer. For the Web-ORLA® group, the computer program recorded a mean (SD) of 8.92 (1.6) hours per week; this was consistent with their self-reported logs which showed a mean (SD) of 8.85 (0.76) hours per week. Similarly, the Bejeweled group reported on their practice logs that they practiced a mean (SD) of 8.66 (1.65) hours per week. See Supplemental Table 1 for Web ORLA® participants’ minutes practiced per week.
Table 2 shows WAB-R LQ scores at each test time for the Web ORLA® group and within group analyses from pre-treatment to post-treatment and from pre-treatment to follow-up. Table 3 shows the between group results from pre-treatment to post-treatment and from pre-treatment to follow-up for the Web ORLA® versus control groups.
Web ORLA® group performance on the Western Aphasia Battery-Revised language quotient.
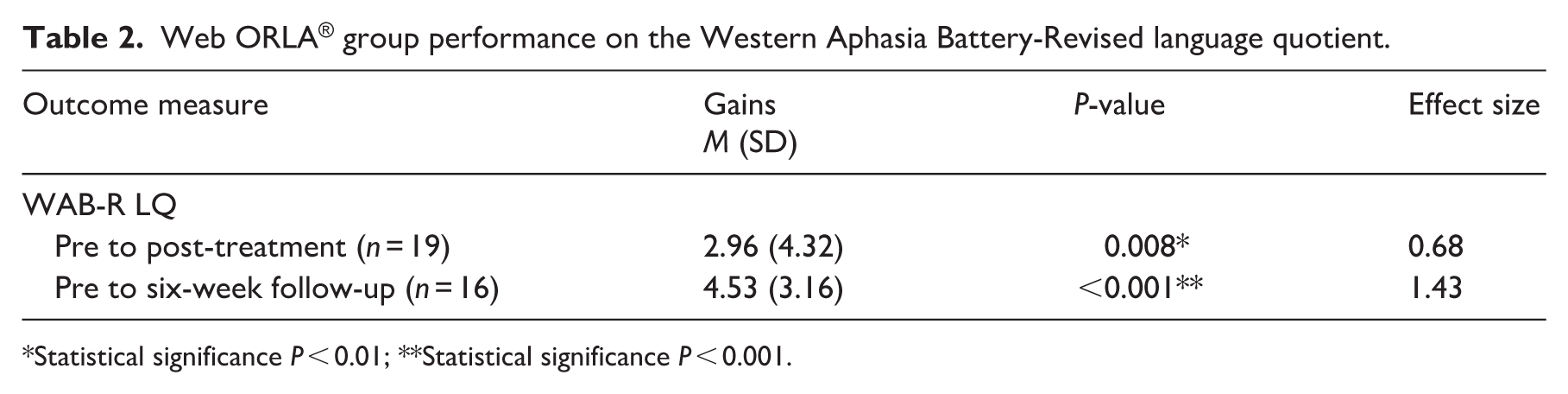
Statistical significance P < 0.01; **Statistical significance P < 0.001.
Between group analyses performance on the Western Aphasia Battery-Revised language quotient.
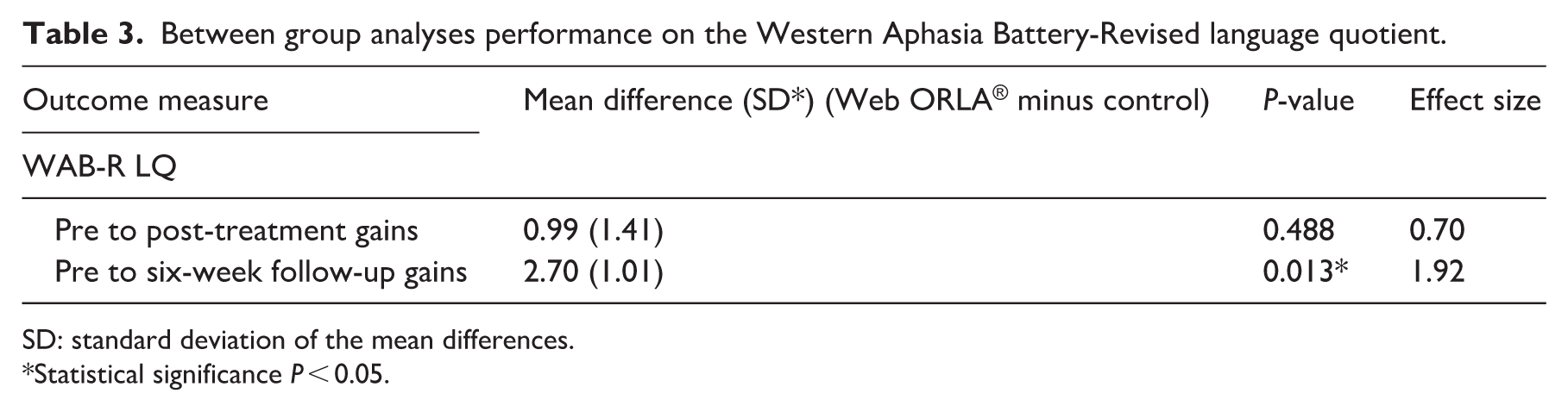
SD: standard deviation of the mean differences.
Statistical significance P < 0.05.
To assess whether Web ORLA® resulted in improvement in language performance, the mean change in WAB-R LQ scores from pre-treatment to post-treatment for the Web ORLA® groups was compared to zero using a two-sided paired t-test. The mean (SD) difference was 2.96 (4.32; P < 0.01), and the effect size was 0.68. Thus, six weeks of Web ORLA® treatment resulted in a significant improvement in language performance, as measured by the change in WAB-R LQ scores.
To assess whether improvements in language performance for the Web ORLA® group were maintained at follow-up, the change in LQ from pre-treatment (week two) to six weeks post-treatment (week 13) was compared to zero using a two-sided paired t-test. The mean (SD) change in LQ scores was 4.53 (3.16; P < 0.001), and the effect size was 1.43 indicating that the LQ scores were not only maintained at the six-week follow-up, but increased over the maintenance period. LQ scores, including reading and writing subscores, at pre-treatment, post-treatment and follow-up assessments for each participant in both groups can be found in Supplemental Tables 2 and 3.
To assess whether Web ORLA® results in greater improvement in language performance than the control treatment, the mean change in LQ from pre-treatment (week two) to post-treatment (week seven) for those randomized to Web ORLA® was compared to the mean change in LQ score for those randomized to Bejeweled using a two-sided two sample t-test with significance level 0.05. The difference in the gain from pre-treatment to post-treatment for the Web ORLA® versus Control groups was 0.989 (SD = 1.41; P > 0.05). Using a pooled variance, there was insufficient evidence to conclude that the web-based ORLA® group performed better (or worse) than the placebo computer treatment (P = 0.488).
To assess whether improvements in LQ for the Web ORLA® group were better maintained over time, the mean change in WAB-R LQ from pre-treatment (week two) to six weeks post-treatment (week 13) was compared to the mean change in LQ score for those randomized to Bejeweled using a paired t-test with significance level 0.05. The difference in the gain from pre-treatment to follow-up for the Web ORLA® versus Control groups was 2.70 (SD = 1.01; P = 0.013), indicating that the Web ORLA® group showed significantly greater gains at follow-up than the control group.
Discussion
Summary of results
Following six weeks of intensive Web ORLA® treatment, participants demonstrated significant improvements in language performance, as measured by the WAB-R LQ. Furthermore, gains were maintained six weeks following the end of treatment. The difference in WAB-R LQ scores between the two groups at post-treatment was not significant. However, at the six-week follow-up period, gains for the Web ORLA® group were significantly better compared to the group who received Bejeweled. Results support previous findings investigating the efficacy of ORLA® for reading comprehension in individuals with chronic aphasia,12,16 as well as evidence indicating cross-modal improvements in written expression resulting from ORLA®. 19
Individual data patterns
Within and between group analyses were employed to address our research questions. Nonetheless, examination of individual participant data yields several interesting patterns. It is notable that participants across both groups presented with a wide range of reading and writing abilities as demonstrated by their pre-treatment performance on the WAB-R LQ. In the Web ORLA® group, LQ performance ranged from 26.0 indicating severe reading and writing deficits to 83.5, indicating only mild impairments. Similarly, in the Bejeweled group performance ranged from 24.6 to 87.1 at the pre-treatment assessment. In the Web ORLA® group, 16 of the 19 participants demonstrated improved LQ performance post-treatment (eight of the 16 demonstrated at least a five point gain); furthermore, of these 16 participants, seven continued to improve at the follow-up assessment. For example, Web ORLA® P2 demonstrated a 10.9 point LQ gain from pre-treatment to follow-up. In addition, participants at both ends of the severity spectrum are among those who made improvements that continued beyond immediately post-treatment, including Web ORLA® P1 (Pre-treatment LQ = 26.0; Follow-up LQ = 34.2) and Web ORLA® P12 (Pre-treatment LQ = 83.5; Follow-up LQ = 90.0).
Participants in the Web ORLA® group did not have access to the program nor did they receive any other speech-language treatment after the six-week treatment period. The improvements observed at the follow-up (six weeks post-treatment) may reflect enhanced neural plasticity and changes in network connectivity resulting from intensive treatment, as suggested by studies that have examined neural mechanisms underlying language recovery in aphasia. 20 Perhaps treatment-induced brain reorganization resulting from intensive Web ORLA® primed the brain to respond to environmental stimuli and continue to change even after the treatment itself was discontinued.
In comparison, four of the 13 participants who received Bejeweled demonstrated at least a five-point LQ gain at post-treatment, but only one of these participants (Control P9) maintained this improvement at follow-up. None of the Bejeweled participants with post-treatment gains continued to improve based on scores at follow-up.
Potential moderators of language improvement
Bejeweled was selected as the control because its play does not require explicit verbal production, auditory processing, or reading comprehension. Consequently, it was somewhat surprising that language gains were observed in participants who received Bejeweled. One consideration is that Bejeweled is verbally mediated and that engaging in this type of computer play sparked participants’ inner speech. A recent review of studies that have employed both objective and subjective measures to examine inner speech in individuals with aphasia suggests that inner speech can be preserved. 21 Inner speech is believed to have a role in language learning and reading, though according to the authors, questions remain as to whether people with aphasia are able to use inner speech to improve performance on cognitive tasks. In addition to the possibility that playing Bejeweled sparked inner speech that led to observable language improvements, participants in the Bejeweled group may have also experienced more opportunities for communication surrounding this new activity.
Attention is another potential moderator of language improvement observed in the control group. Bejeweled play likely engages visual attention, as well as working memory and executive attention processes that are employed during the strategic behavior of planning moves to earn points. Impaired performance on standardized measures of attention have been reported in individuals with aphasia, 22 and the relationship between attention and language is well recognized.23–26 In addition, attentional models of aphasia have motivated various treatments for aphasia with compelling findings.27–30
Telepractice/advantages of Web ORLA®
Results from this trial raise interesting discussion related to telepractice. Web ORLA® combines the flexibility of asynchronous modes of delivery with the oversight and clinician feedback afforded by synchronous modes of delivery. 31 The SLP was able to observe participants live during practice and offer feedback, as well as make adjustments to the program (e.g., change rate at which sentences were read aloud by virtual therapist) to individualize the program to participants’ needs. At the same time, participants had the autonomy to set their own practice schedules. In addition, they could request to speak with the research SLP during live observations. Although we did not collect objective data about the amount of time the SLP spent with participants during their practice sessions, the SLPs reported that they spent about 5–10 minutes per day with each participant during the first week of practice. This typically decreased to about five minutes per week by the final week of practice.
Compliance
Researchers were able to monitor compliance with recommended practice amount via the Web ORLA® program. As shown in Supplemental Table 1, the majority of participants (nine out of 13) met or exceeded the recommended 540 minutes of practice per week (i.e., 90 minutes/day, six days per week). As a group, the computer program recorded a mean of 8.92 (SD = 1.6) hours per week, or 98.5% compliance with the recommended nine hours of practice per week. Interestingly, compliance in this study was much greater than the compliance achieved in the recent Des Roches et al. 9 and Palmer et al. 10 studies. The presence of Web ORLA®’s virtual therapist and accessibility to the research SLP through the program may have had a positive impact on participants’ compliance.
Treatment intensity
Perhaps the greatest advantage of telepractice is that it allows for the provision of intervention with greater intensity than is feasible with traditional face-to-face therapy. There is a pressing need for evidence-based treatment that can be delivered remotely and at a high intensity, particularly in the current healthcare climate in which there is decreasing financial support for extended rehabilitation post-stroke. Web ORLA® offers multi-modal language stimulation with high rates of practice, which can be delivered over a short period of time. This dosage is consistent with studies that suggest intense aphasia therapy delivered over a short period has greater impact than less therapy delivered over longer period of time. 32
While conversational interaction from the clinician are integral to the therapy process for some treatment approaches,33,34 other interventions, such as ORLA® are aimed at improving disrupted language processes and require intensive targeted practice. 35 As such, interaction with the clinician has the potential to detract from focused time on treatment tasks which can impact intensity. For example, in the Des Roches et al. study, 9 the feedback delivered by the clinician in the face-to-face session was likely one of the factors that limited the amount of actual treatment time on the tasks, resulting in decreased practice time than researchers had anticipated. Removing this face-to-face variable with telepractice options may actually result in more targeted practice. In Web ORLA®, the virtual therapist guides and prompts participants without detracting from practice opportunities.
Limitations and future directions
There are several limitations to this study. As planned, the study was well powered at 97.12% to detect a five point difference in LQ scores between Web ORLA and control groups. However, the actual difference revealed in the current study was smaller. With a three point difference between groups, the study was only powered at 64.25%. A larger sample of participants would provide greater power for detecting a three point difference between groups. A larger sample would also allow for examination of subtypes of aphasia to determine if Web ORLA® is more efficacious for one type of aphasia over another. This trial was not double blinded because participants were aware of whether they received the language-based treatment, Web ORLA®, or the non-language control. Therefore, any expectation for language improvements based on the treatment group could have been a source of bias. Furthermore, because a significant difference in language improvements between groups was not observed immediately post-treatment, further research is needed to determine the effects of Web ORLA® compared to more generalized computer stimulation.
This study also identifies areas in which Web ORLA® could be improved. Various computer-based treatments developed for individuals with acquired brain injury incorporate performance feedback following tasks,36,37 which may be a factor that helps drive self-regulatory behavior and more positive outcomes following computer training. 27 In Web ORLA®, participants have the opportunity to self-assess their independent oral productions of sentences. However, a future improvement could include program generated feedback on sentence production accuracy. Currently, Web ORLA® is only available on a PC. A future direction would be to expand the technology to include app based software.
In conclusion, this randomized controlled trial provides evidence for improved language outcomes following intensive, web-based delivery of Oral Reading for Language in Aphasia in individuals with chronic aphasia. Findings underscore the value of web-based programs that combine clinician oversight with the flexibility of asynchronous practice.
Clinical implications
Web based aphasia treatment that combines clinician oversight with the flexibility of asynchronous practice is feasible.
Participants with aphasia are compliant with recommendations for home practice schedule.
Oral Reading for Language in Aphasia (ORLA®) elicits multi-modality language improvements.
Supplemental Material
sj-pdf-1-cre-10.1177_0269215520988475 – Supplemental material for Web-based Oral Reading for Language in Aphasia (Web ORLA®): A pilot randomized control trial
Supplemental material, sj-pdf-1-cre-10.1177_0269215520988475 for Web-based Oral Reading for Language in Aphasia (Web ORLA®): A pilot randomized control trial by Leora R Cherney, Jaime B Lee, Kwang-Youn A Kim and Sarel van Vuuren in Clinical Rehabilitation
Supplemental Material
sj-pdf-2-cre-10.1177_0269215520988475 – Supplemental material for Web-based Oral Reading for Language in Aphasia (Web ORLA®): A pilot randomized control trial
Supplemental material, sj-pdf-2-cre-10.1177_0269215520988475 for Web-based Oral Reading for Language in Aphasia (Web ORLA®): A pilot randomized control trial by Leora R Cherney, Jaime B Lee, Kwang-Youn A Kim and Sarel van Vuuren in Clinical Rehabilitation
Footnotes
Acknowledgements
We thank Rosalind Hurwitz and Rachel Hitch for their assistance with data collection during assessment and treatment. We also acknowledge Nattawut Ngampatipatpong and Jariya Tuantranont for technical support for Web ORLA®. Finally, we thank the participants with aphasia for their time and effort.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: A beta version of ORLA® is commercially available from the Shirley Ryan AbilityLab. Dr. Cherney receives salary from the Shirley Ryan AbilityLab but has no financial interest in the software sales.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Grant H133G06055 from the National Institute on Disability, Independent Living, and Rehabilitation Research (PI: L. R. Cherney). Manuscript preparation was supported by the Coleman Foundation.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.