
Abstract
Objective
To investigate the effectiveness of functional electrical stimulation of the legs in patients with heart failure.
Methods
Data were obtained from PubMed, Cochrane Library, and Embase databases until August 12, 2021. We included randomized controlled trials that evaluated the effects of functional electrical stimulation applied to the legs of patients with heart failure, namely changes in cardiopulmonary function, muscle strength, and quality of life.
Results
In total, 14 randomized controlled trials (consisting of 518 patients) were included in our article. Pooled estimates demonstrated that functional electrical stimulation significantly improved peak oxygen consumption (peak VO2; standardized mean difference = 0.33, 95% confidence interval = 0.07–0.59, eight randomized controlled trials, n = 321), 6-min walking distance (mean difference = 48.03 m, 95% confidence interval = 28.50–67.57 m, 10 randomized controlled trials, n = 380), and Minnesota Living with Heart Failure Questionnaire quality of life score (mean difference = − 8.23, 95% confidence interval = − 12.64 to − 3.83, nine randomized controlled trials, n = 383). Muscle strength of lower extremities was not significantly improved in the functional electrical stimulation group compared with that in the control group (standardized mean difference = 0.26, 95% confidence interval = − 0.18 to 0.71, five randomized controlled trials, n = 218). Furthermore, the subgroup analysis revealed that functional electrical stimulation significantly improved peak VO2, 6-min walking distance, and Minnesota Living with Heart Failure Questionnaire quality of life score in the heart failure with reduced ejection fraction and heart failure with preserved ejection fraction subgroups.
Conclusion
Functional electrical stimulation can effectively improve the cardiopulmonary function and quality of life in patients with heart failure. However, functional electrical stimulation did not significantly improve muscle strength in the legs.
Introduction
Patients with heart failure commonly have functional capacity limitation associated with poor quality of life because of dyspnea and fatigue, namely exercise intolerance.1,2 Rehabilitation has been proven to play a positive and crucial role in improving the major limiting symptom of heart failure.3,4 However, some patients with heart failure do not adapt to or drop out of conventional exercise training programs, and some other patients with severe heart failure symptoms, such as New York Heart Association classes III and IV, 5 cannot perform even low-intensity physical exercise. Hence, functional electrical stimulation is considered for alternative replacement therapy. Functional electrical stimulation is a technique that employs low-energy electrical pulses to prompt muscle contractions. Functional electrical stimulation can improve the function of paralyzed muscles, such as those of patients with spinal cord injury or stroke.6,7 Recent studies, have demonstrated the potential benefits of functional electrical stimulation in patients with heart failure, including improved functional status, 8 exercise capacity, 9 endothelial function, 10 quality of life, 11 and emotional stress. 12
Three meta-analyses published in 2010, 2013, and 2016 included only two, five, and seven randomized controlled trials, respectively, that compared functional electrical stimulation and control treatments.13–15 Therefore, we performed a systematic review and meta-analysis of a greater number of randomized controlled trials to compare application of functional electrical stimulation to the legs in patients with heart failure with control treatments in terms of their effectiveness in improving cardiopulmonary function, muscle strength of the legs, and quality of life.
Method
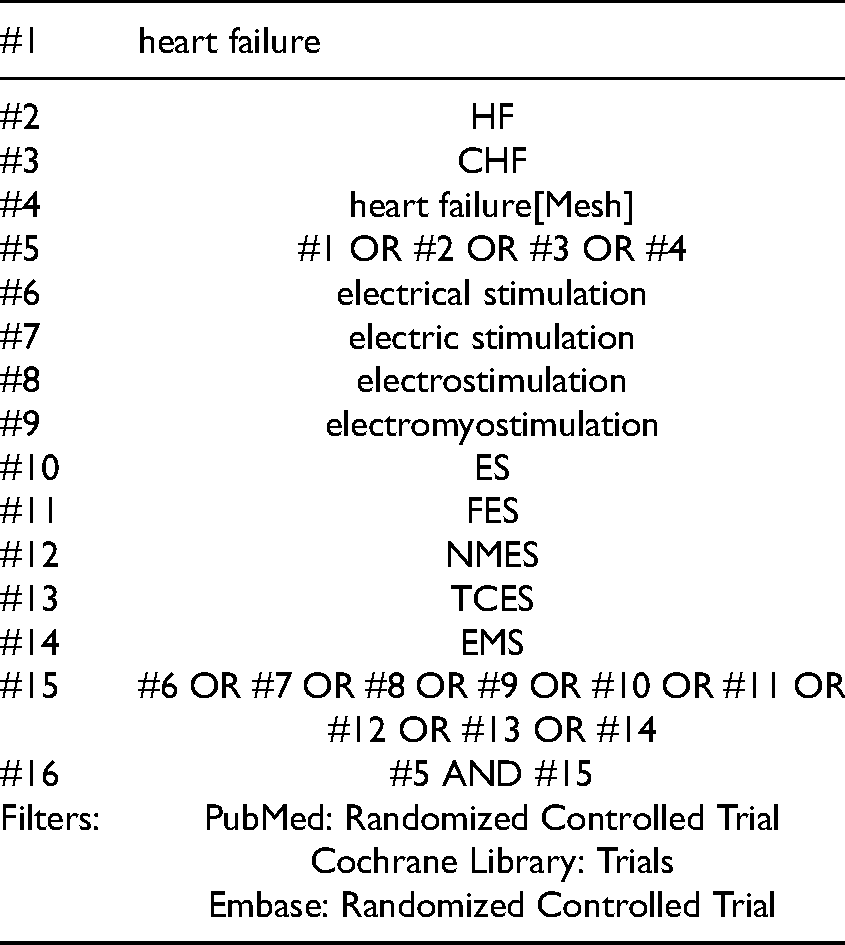
The PICO (patients, intervention, comparison, and outcomes) question of this study was as follows: compared with the placebo (C), does functional electrical stimulation (I) improve cardiopulmonary function, muscle strength of the legs, and quality of life (O) in patients with heart failure (P)? A search was conducted without language restrictions on the PubMed, Cochrane Library, and Excerpta Medica (Embase) online databases for relevant articles. Keywords from each of the following categories were determined before the search was conducted: types of patients, interventions, and studies. The following keywords were used in the search: “heart failure (or ‘HF’ or ‘CHF’ or ‘heart failure[Mesh]’)” for patient type and “electrical stimulation (or ‘electric stimulation’ or ‘electrostimulation’ or ‘electromyostimulation’ or ‘ES' or ‘FES' or ‘NMES' or ‘TCES’ or ‘EMS’)” for intervention category. The relevant randomized controlled trials were identified through a set intersection of the keyword “random*” or the limitation function in the databases. Search strategies used in this study are presented in Appendix 1. All databases were searched from the time of their inception to August 12, 2021.
Two researchers individually reviewed the full text of each retrieved article to identify potentially relevant studies. Only articles that met the inclusion criteria were selected. Studies were included in the systematic review if (1) patients were diagnosed as having heart failure; (2) reported outcomes included the effect of functional electrical stimulation of the legs on cardiopulmonary function, muscle strength of the legs, or quality of life; and (3) they were randomized controlled trials. The analyses of the researchers were compared, and discrepancies were evaluated by a third researcher and resolved through repeated discussions.
We excluded articles with only protocols and non–peer-reviewed articles, such as conference papers and letters to the editor. We excluded randomized controlled trials that investigated the effects of combination treatments in which the effects of functional electrical stimulation could not be isolated. Randomized crossover studies were considered a type of randomized controlled trial; therefore, they were included.
Two reviewers independently extracted data for the functional electrical stimulation and placebo groups for the following parameters: sample size, age, New York Heart Association functional classification, and left ventricular ejection fraction; functional electrical stimulation stimulus position, intensity, frequency, pulse width, and stimulus duration; and outcome measures. Studies that did not include all of the aforementioned data were included for meta-analysis if they were deemed to be of sufficient quality.
The quality of the included studies was assessed using the Physiotherapy Evidence Database (PEDro) scale, which is a widely used quality assessment tool for evaluating bias risk in randomized controlled trials. PEDro scale scores provided by two assessors were compared, and differences were resolved by a third researcher through discussion. The ratings of PEDro scale items 2–11 are summed to obtain a combined total PEDro scale score between 0 and 10. Scores of <4 are considered “poor,” 4–5 are considered “fair,” 6–8 are considered “good,” and 9–10 are considered “excellent.” 16
The main outcome measurements in this study comprised three parts. One is cardiopulmonary outcome, which include peak oxygen consumption and 6-min walking distance. These are objective measures for assessing functional capacity as well as important predictors of prognosis in patients with heart failure.17–19 The other outcomes are muscle strength of legs and quality of life. Certain other outcomes in the included randomized controlled trials were also reported. Outcomes reported by more than three randomized controlled trials were pooled into quantitative analysis.
A meta-analysis was conducted using RevMan (version 5.3; The Cochrane Collaboration, London, UK). All relevant data measured using different scales were converted to a single scale. The converted data are expressed using standardized mean differences (SMDs) and 95% confidence intervals (CIs) and were pooled by the software program for calculation. The pooled data were analyzed using the random-effects model considering that various study methods were used in the selected randomized controlled trials. Statistical heterogeneity, calculated using the I2 test, was considered high if I2 was >70%. In the case of high heterogeneity, a sensitivity analysis was conducted to confirm its effect after adjustment of included data. The results were considered statistically significant when p values of <0.05 were obtained in the equivalent z test
For a forest plot with >10 studies, publication bias was analyzed using a funnel plot.
Result
A flowchart illustrating the trial selection process is presented in Figure 1. The characteristics of patients and the functional electrical stimulation from the selected trials are listed in Tables 1 and 2, respectively. Of the studies that were retrieved from the databases and reviewed by the 2 reviewers, 14 randomized controlled trials comparing the effects of functional electrical stimulation of the legs and control treatments on patients with heart failure met the eligibility criteria and were included in the qualitative and quantitative analyses. Of the included articles, 1 was a crossover study and 13 were parallel studies; 12 of the 14 articles reported on patients with heart failure with a reduced ejection fraction and 2 articles reported on patients with heart failure with a preserved ejection fraction.
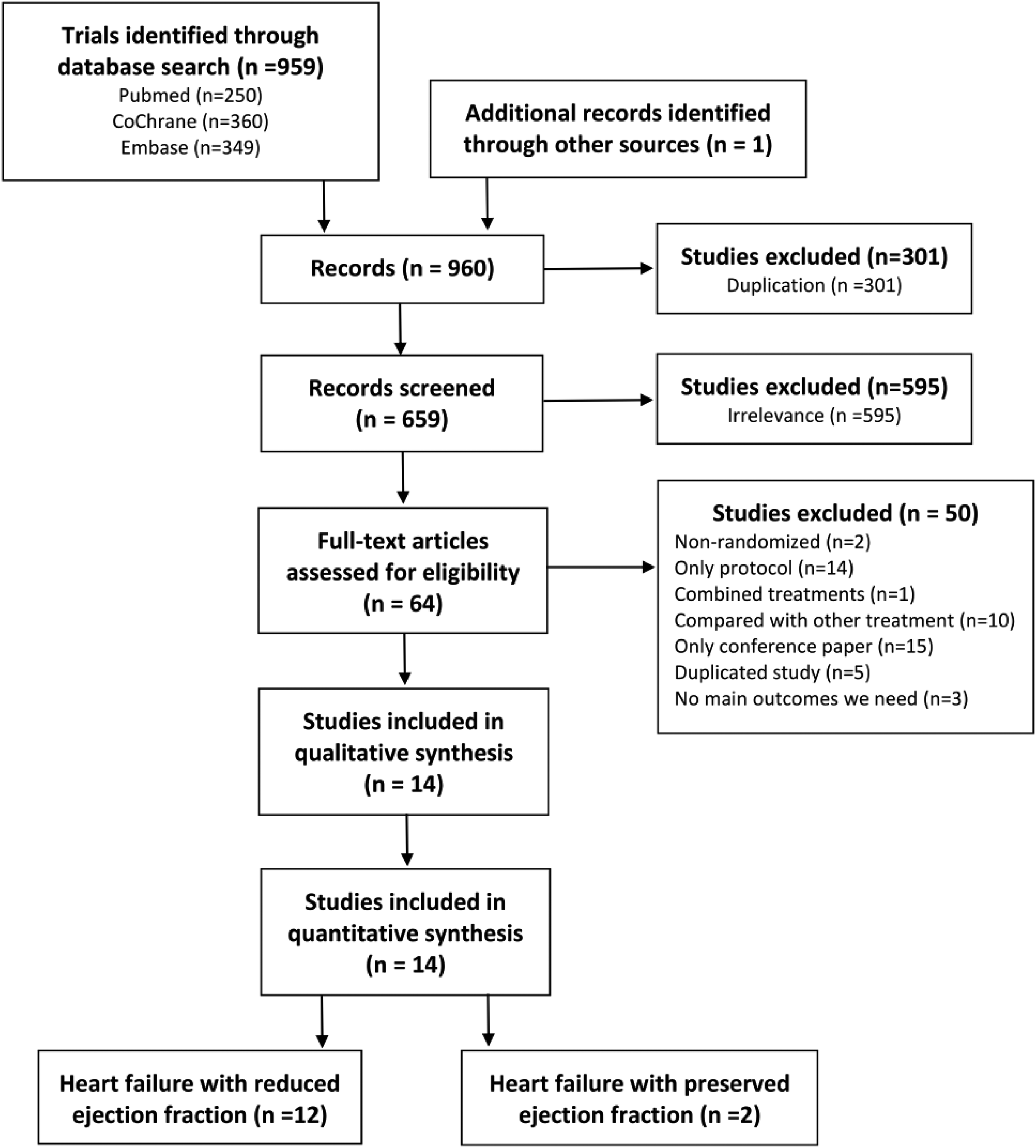
Flowchart of trial selection.
Patient characteristics.
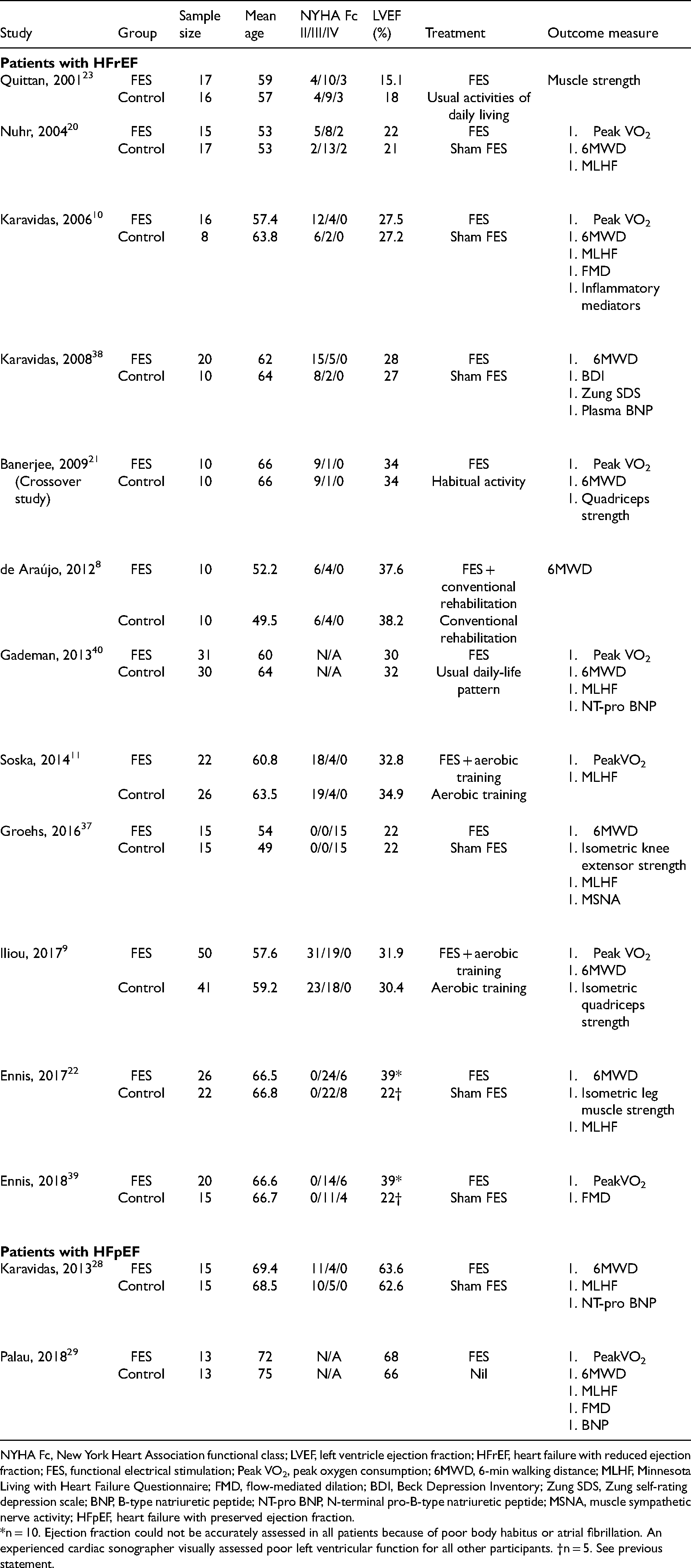
NYHA Fc, New York Heart Association functional class; LVEF, left ventricle ejection fraction; HFrEF, heart failure with reduced ejection fraction; FES, functional electrical stimulation; Peak VO2, peak oxygen consumption; 6MWD, 6-min walking distance; MLHF, Minnesota Living with Heart Failure Questionnaire; FMD, flow-mediated dilation; BDI, Beck Depression Inventory; Zung SDS, Zung self-rating depression scale; BNP, B-type natriuretic peptide; NT-pro BNP, N-terminal pro-B-type natriuretic peptide; MSNA, muscle sympathetic nerve activity; HFpEF, heart failure with preserved ejection fraction.
*n = 10. Ejection fraction could not be accurately assessed in all patients because of poor body habitus or atrial fibrillation. An experienced cardiac sonographer visually assessed poor left ventricular function for all other participants. †n = 5. See previous statement.
FES characteristics.
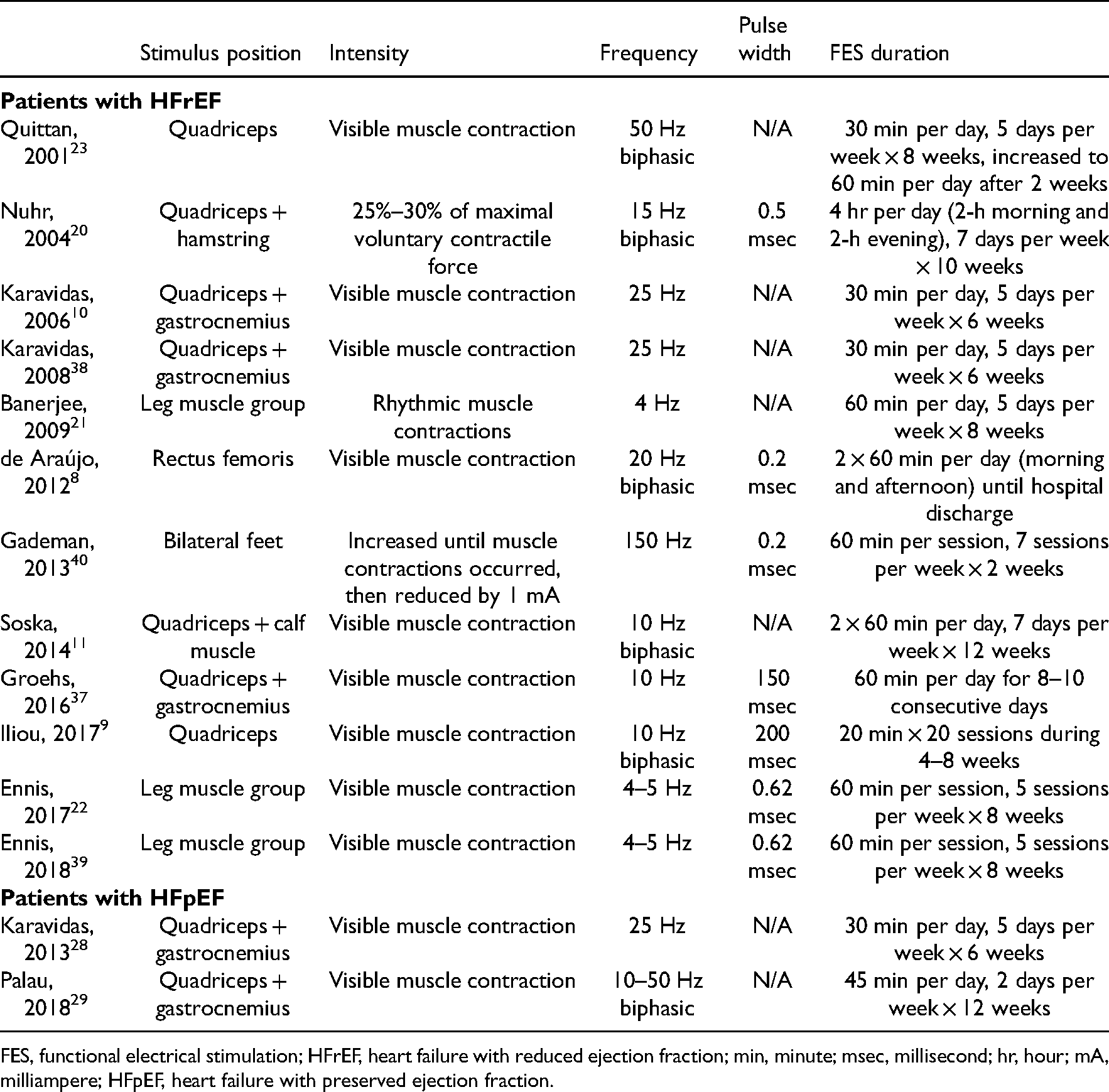
FES, functional electrical stimulation; HFrEF, heart failure with reduced ejection fraction; min, minute; msec, millisecond; hr, hour; mA, milliampere; HFpEF, heart failure with preserved ejection fraction.
The quality of the included randomized controlled trials was independently assessed by two reviewers on a PEDro scale. All PEDro scale scores in the included studies were between 4 and 8. On the basis of these scores, six studies were classified as “fair” and eight studies were classified as “good.” The detailed results of the risk of bias assessment are listed in Table 3.
PEDro scale.
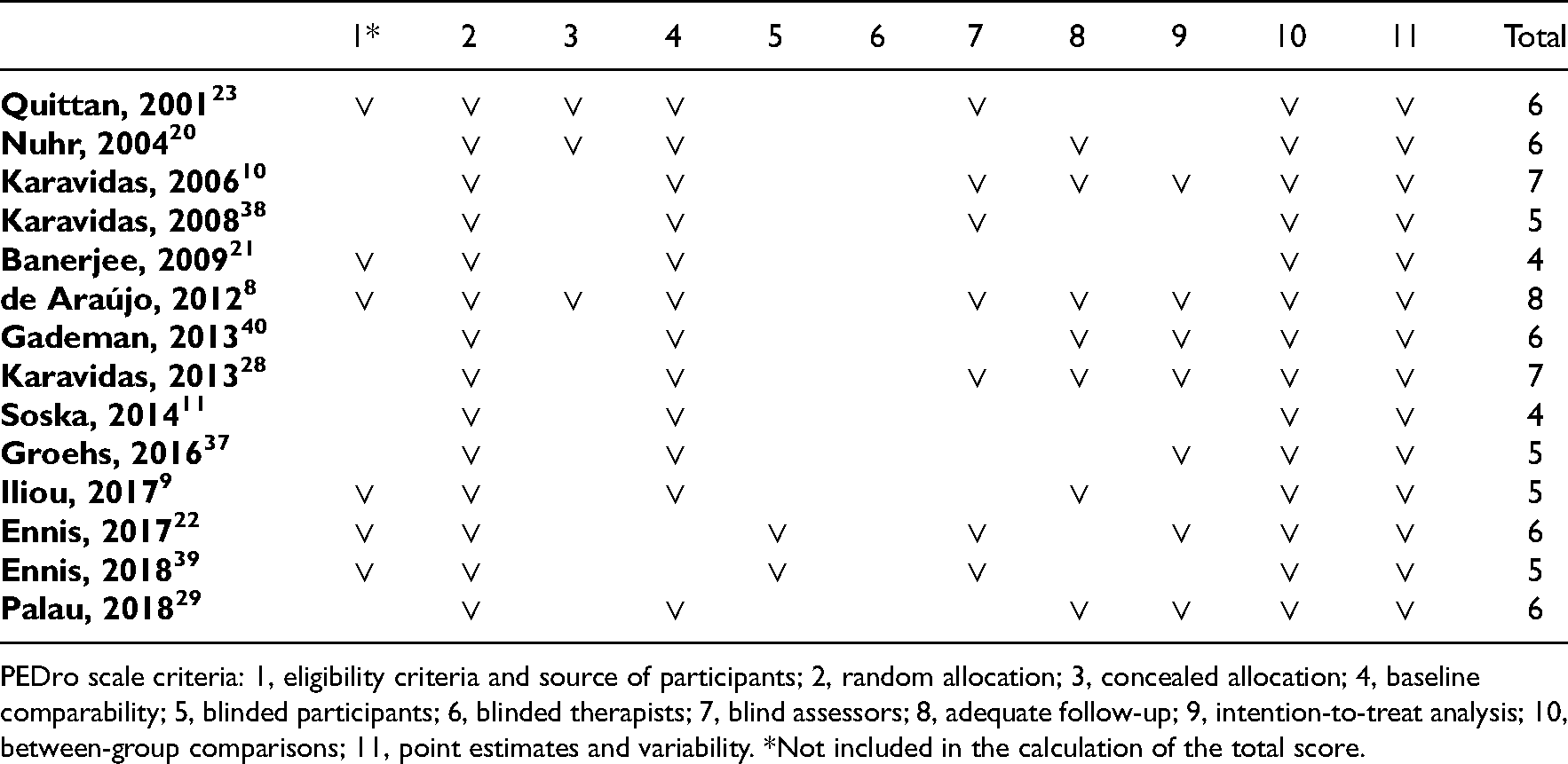
PEDro scale criteria: 1, eligibility criteria and source of participants; 2, random allocation; 3, concealed allocation; 4, baseline comparability; 5, blinded participants; 6, blinded therapists; 7, blind assessors; 8, adequate follow-up; 9, intention-to-treat analysis; 10, between-group comparisons; 11, point estimates and variability. *Not included in the calculation of the total score.
In total, 14 randomized controlled trials were included in the meta-analysis. Cardiopulmonary function was assessed through measurement of peak oxygen consumption and 6-min walking distance; the Minnesota Living with Heart Failure Questionnaire was used to assess patients’ quality of life. The treatment methods used in the control group were usual daily living, sham functional electrical stimulation, low-intensity functional electrical stimulation, aerobic training, and conventional rehabilitation. Because units of measurement for reported data were not uniform across the included articles, the SMD was used to measure the peak oxygen consumption and the muscle strength of the lower extremities. The units of measurement used to report data on 6-min walking distance and quality of life were consistent in all articles. Thus, the mean difference was used to measure the differences between the control and functional electrical stimulation groups.
Compared with the control group, the group that underwent functional electrical stimulation exhibited significantly greater improvement in peak oxygen consumption, 6-min walking distance, and Minnesota Living with Heart Failure Questionnaire score, but non-significant improvement in the muscle strength of lower extremities.
In the subgroup analysis of patients with heart failure with reduced ejection fraction, the group subjected to functional electrical stimulation reported greater improvements in peak oxygen consumption, 6-min walking distance, and Minnesota Living with Heart Failure Questionnaire score.
In the subgroup analysis of patients with heart failure with preserved ejection fraction, the group subjected to functional electrical stimulation demonstrated greater improvements in peak oxygen consumption, 6-min walking distance, and Minnesota Living with Heart Failure Questionnaire score. The forest plots of these outcomes are shown in Figures 2, 3, 5, and 6.
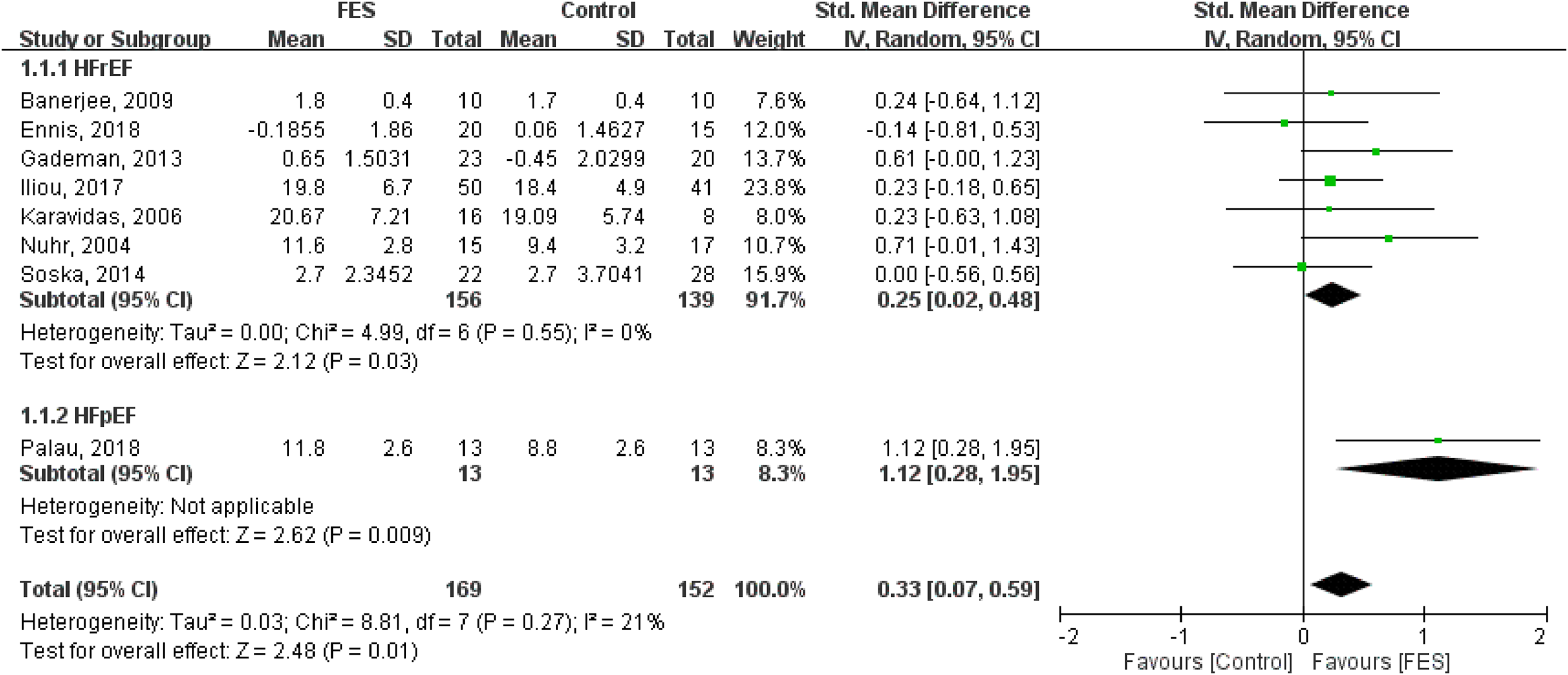
Forest plot of the effects of functional electrical stimulation of the legs on peak oxygen consumption.
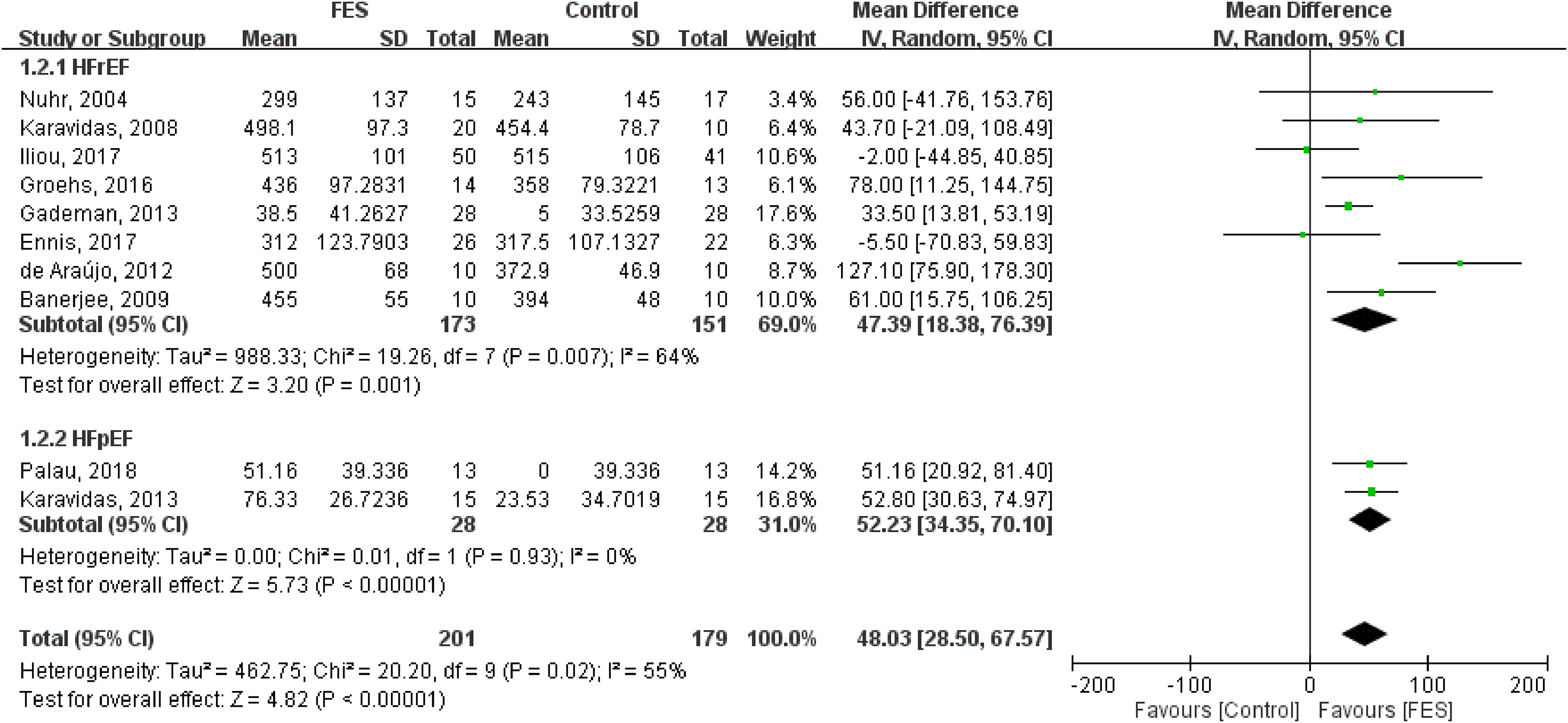
Forest plot of the effects of functional electrical stimulation of the legs on 6-min walking distance.
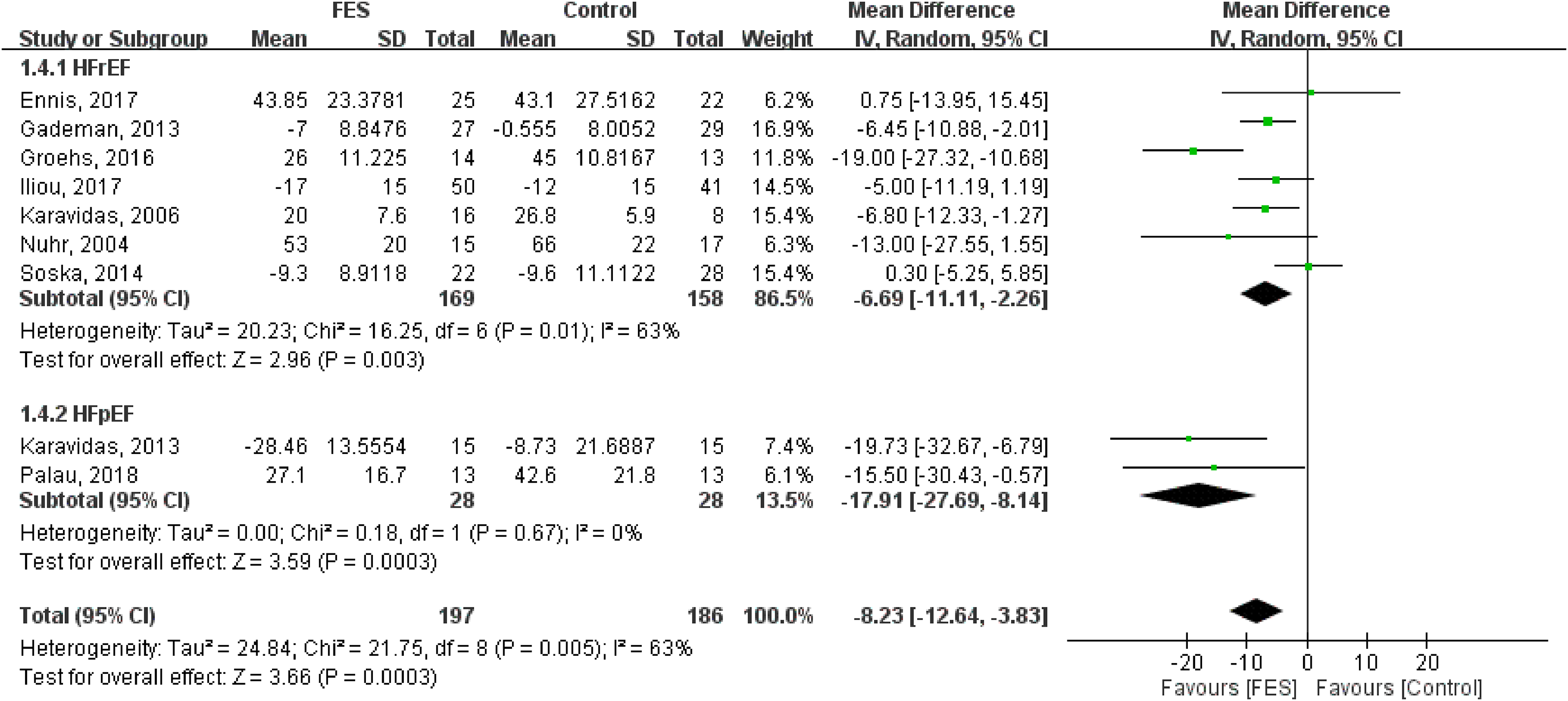
Forest plot of the effects of functional electrical stimulation of the legs on Minnesota living with heart failure questionnaire scores.
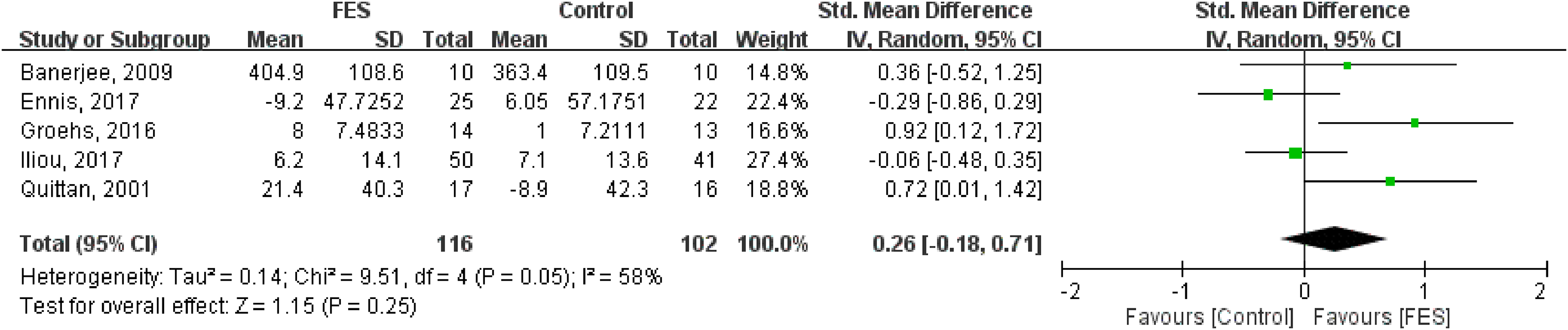
Forest plot of the effects of functional electrical stimulation of the legs on muscle strength of the lower extremities.
A symmetric funnel plot for 6-min walking distance showed minimal evidence of publication bias. The funnel plot for 6-min walking distance is shown in Figure 4.
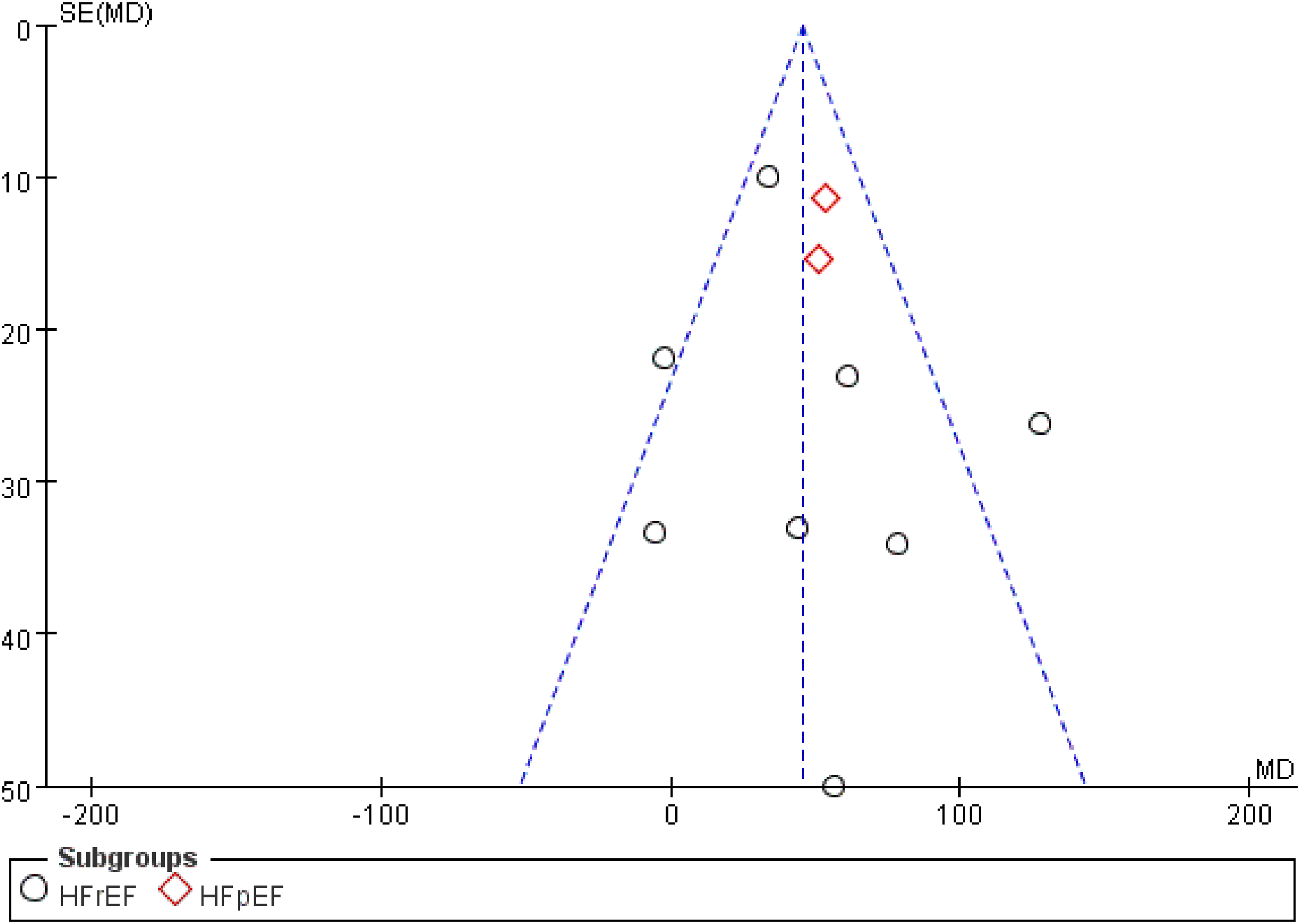
Funnel plot of the effects of functional electrical stimulation of the legs on 6-min walking distance.
The I2 values for all the outcomes were <70%. Low statistical heterogeneity (I2 < 50%) was observed in peak oxygen consumption. Moderate statistical heterogeneity (I2: 50%–70%) was noted in 6-min walking distance, Minnesota Living with Heart Failure Questionnaire score, and muscle strength of lower extremities. Therefore, these comparisons were consistent.
In total, four studies reported adverse outcomes. Three studies reported that functional electrical stimulation and sham functional electrical stimulation were well tolerated in patients.20–22 No adverse event due to the intervention was recorded in either group. Only one study by Quittan et al. reported the adverse event muscle soreness in four patients after the stimulation period onset, but this symptom was tolerable and subsided after treatment. Furthermore, increasing heart rates above resting values were monitored, but clinical signs of exertion or dyspnea were not found. 23
Discussion
Our analysis suggested that, compared with the control group, use of functional electrical stimulation in patients with heart failure resulted in greater improvement in cardiopulmonary function and quality of life. We did not identify significant differences between the improvement of muscle strength in the legs of the functional electrical stimulation group and that of control group. Previous studies have revealed that a SMD of 0.2 may be a cutoff for “small effect” and “moderate effect” and may also be the threshold for clinical meaningfulness.24–26 Therefore, the improvement in peak oxygen consumption after functional electrical stimulation (SMD of 0.33 in our meta-analysis) can be considered clinically meaningful. One study also suggested that a change in 6-min walking distance of approximately 30 m to 32 m can be considered clinically meaningful. 27 Hence, compared with control group, the increase in 6-min walking distance after functional electrical stimulation (mean difference of 48.03 m in our meta-analysis) can be considered clinically meaningful.
To our knowledge, this is the first meta-analysis to perform a subgroup analysis to determine the effectiveness of functional electrical stimulation in patients with heart failure with reduced ejection fraction and patients with heart failure with preserved ejection fraction. In our study, both groups exhibited significant improvements in peak oxygen consumption, 6-min walking distance, and Minnesota Living with Heart Failure Questionnaire score after functional electrical stimulation. Furthermore, compared with the subgroup of heart failure with preserved ejection fraction, the subgroup of heart failure with reduced ejection fraction exhibited greater improvements in terms of peak oxygen consumption, 6-min walking distance, and Minnesota Living with Heart Failure Questionnaire score after functional electrical stimulation. However, only two randomized controlled trials discussed the outcomes of patients with heart failure with preserved ejection fraction.28,29 Therefore, additional randomized controlled trials are required in the future.
Three meta-analyses regarding functional electrical stimulation in patients with heart failure have been published.13–15 The results of these studies revealed that functional electrical stimulation significantly improved peak oxygen consumption, 6-min walking distance, and quality of life. However, two of them had high statistical heterogeneity (I2 > 90% in the meta-analysis of peak oxygen consumption), and all of them had an insufficient number of randomized controlled trials (seven or fewer) for comparing functional electrical stimulation with control groups; thus, the effectiveness of functional electrical stimulation in treating patients with heart failure was not fully revealed in these studies. In our meta-analysis, 14 randomized controlled trials comparing functional electrical stimulation with control groups were identified after comprehensive database searches and detailed screenings were conducted. Of them, seven randomized controlled trials were not included in the most recent meta-analysis by Gomes Neto et al. which included only randomized controlled trials published before 2013. 13 Our meta-analysis, therefore, provides additional evidence to elucidate the effectiveness of functional electrical stimulation in improving cardiopulmonary function and quality of life in patients with heart failure.
Up to 19.5% of patients with heart failure experienced muscle wasting, which may be caused by inflammatory processes and metabolic changes.30,31 Functional electrical stimulation is considered an effective treatment for muscle weakness in adults with advanced progressive disease including chronic obstructive pulmonary disease and heart failure. 32 Furthermore, functional electrical stimulation has been used as an additional form of physical therapy to prevent lower limb muscle atrophy in critically ill patients.33–36 Our meta-analysis indicated that the functional electrical stimulation group exhibited potentially greater improvements in the muscle strength of the legs compared with the control group. However, the outcomes did not reach statistical significance, which may be due to the insufficient number of patients with data allowing for muscle strength outcomes to be retrospectively measured. Hence, further research is required to clarify the effectiveness of functional electrical stimulation in improving muscle strength.
Several outcomes were not pooled in the quantitative analysis. Compared with the control group, the functional electrical stimulation group exhibited a significantly lower muscle sympathetic nerve activity burst frequency, 37 level of inflammatory mediators (tumor necrosis factor-α, intercellular adhesion molecule-1, and vascular cell adhesion molecule-1), 10 capacity of aerobic-oxidative energy metabolism, 20 and rate of depression (as measured through a depression scale). 38 The functional electrical stimulation group also exhibited possible amelioration of the endothelial function of the brachial artery.10,39 However, levels of plasma B-type natriuretic peptide, 38 N-terminal pro-B-type natriuretic peptide, 40 left ventricle ejection fraction, 10 and interleukin-6 and interleukin-10 10 were not significantly improved through functional electrical stimulation.
Clarifying the reasons that functional electrical stimulation of lower extremities is helpful for patients with heart failure is important. Inflammatory activation and endothelial dysfunction led to the progressive syndrome of heart failure by promoting vascular dysfunctions.41–43 According to previous studies, functional electrical stimulation attenuated the inflammatory mediators and oxidative stress in heart failure patients.10,20 Endothelial function may be also improved after treatment with functional electrical stimulation.10,12 We suggest that this reported efficacy of functional electrical stimulation can improve cardiac function in patients with heart failure.
Muscle soreness and increasing heart rate were reported by one randomized controlled trial, 23 and no adverse event was reported by three randomized controlled trials.20–22 However, we could not draw an assertive conclusion that functional electrical stimulation is safe for patients with heart failure, because most randomized controlled trials did not mention whether an adverse event was observed. More studies are required in the future to clarify whether adverse events occur after functional electrical stimulation.
Nevertheless, our meta-analysis had limitations. First, according to a bias risk assessment, most of the included studies had potential bias risks, which limited the strength of the results. Second, because the available databases used in this study are limited, some relevant trials may not have been included for analysis. Third, diverse protocols of functional electrical stimulation, including the frequencies, durations, and numbers of different training sessions as well as different stimulated muscles, were used in the selected randomized controlled trials. Fourth, seven randomized controlled trials included in our meta-analysis used sham functional electrical stimulation with sensory input or low-intensity stimulation in the control group, which might have influenced the outcomes. Fifth, only two articles using functional electrical stimulation to treat patients with heart failure with preserved ejection fraction were identified, indicating that further study on this subject is required.
According to the results of this meta-analysis, functional electrical stimulation is effective in improving cardiopulmonary function and quality of life in patients with heart failure either with reduced ejection fraction or with preserved ejection fraction. Therefore, functional electrical stimulation is an alternative therapy for those patients with heart failure who cannot perform conventional exercise. However, randomized controlled trials investigating the effectiveness of functional electrical stimulation on heart failure with preserved ejection fraction are insufficient, so further large-scale studies are required. Future studies should also investigate the related adverse events.
Footnotes
Appendix 1. Search strategy
| #1 | heart failure |
|---|---|
| #2 | HF |
| #3 | CHF |
| #4 | heart failure[Mesh] |
| #5 | #1 OR #2 OR #3 OR #4 |
| #6 | electrical stimulation |
| #7 | electric stimulation |
| #8 | electrostimulation |
| #9 | electromyostimulation |
| #10 | ES |
| #11 | FES |
| #12 | NMES |
| #13 | TCES |
| #14 | EMS |
| #15 | #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14 |
| #16 | #5 AND #15 |
| Filters: | PubMed: Randomized Controlled Trial Cochrane Library: Trials Embase: Randomized Controlled Trial |
Acknowledgements
This manuscript was edited by Wallace Academic Editing.
Author’s note
Hsun-Yi Wang, Department of General Medicine, Kaohsiung Medical University Hospital, Kaohsiung Medical University, Kaohsiung, Taiwan.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Funding
No specific grant was received from any funding agency in the public, commercial, or not-for-profit sector.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.