
Abstract
Objectives
Repetitive peripheral magnetic stimulation (rPMS) is a non-invasive method that activates peripheral nerves and enhances muscle strength. This study aimed to investigate the effect of rPMS applied in early subacute stroke on severe upper extremity impairment.
Design
Randomized controlled trial.
Setting
Rehabilitation department of a university hospital.
Subjects
People aged 30–80 years with no practical arm function within four weeks of a first stroke.
Interventions
Participants were randomly assigned to either the rPMS group (n = 24, 20Hz and 2400 pulses of rPMS to triceps brachii and extensor digitorum muscles daily for two weeks in addition to conventional physiotherapy) or the control group (n = 20, conventional physiotherapy).
Main measures
The primary outcome was the upper extremity motor section of Fugl-Meyer Assessment after treatment. Secondary outcomes included Barthel Index and root mean square of surface electromyography for muscle strength and stretch-induced spasticity of critical muscles of the upper extremity. Data presented: mean (SD) or median (IQR).
Results
The rPMS group showed more significant improvements in the Fugl-Meyer Assessment (12.5 (2.5) vs. 7.0 (1.4), P < 0.001), Barthel Index (15 (5) vs. 10 (3.7), P < 0.001), and strength-root mean square (biceps brachii: 20.5 (4.8) vs. 6.2 (2.7), p < 0.001; triceps brachii: 14.9 (5.8) vs. 4.3 (1.2), p < 0.001; flexor digitorum: 5.1 (0.8) vs. 4.0 (1.1), p < 0.001) compared with the control group.
Conclusion
In patients with no functional arm movement, rPMS of upper limb extensors improves arm function and muscle strength for grip and elbow flexion and extension.
Keywords
Introduction
Peripheral magnetic stimulation of muscle has been investigated as a treatment of weakness in the arm after stroke. Magnetic stimulation has been developed for the non-invasive stimulation of the central and peripheral nervous system.1,2 Based on a physics principle that a changing magnetic field will induce a flow of electrons within the field, magnetic stimulation induces a controlled depolarization of adjacent nerves and subsequent muscle contraction. 3 The efficacy of repetitive transcranial magnetic stimulation has been widely studied on the motor, language, and cognitive impairment after stroke and showed the potential to modulate the brain cortex directly4–6—however, few studies on the application of repetitive peripheral magnetic stimulation (rPMS) in stroke. rPMS was indicated among non-surgical urinary incontinence therapies in the latest guidelines with the ability to increase the strength of pelvic floor muscle.7,8 A recent study has proved that rPMS of the suprahyoid muscles increased the strength of these muscles and improve the swallowing function for patients with post-stroke dysphagia. 9 rPMS is somewhat similar to that of electrical stimulation, but rPMS provides a greater range of depth and less pain, and there's no need to remove clothes. 3 So far, although some studies have shown that rPMS is effective for shoulder pain and arm function after stroke,10,11 there is no literature on the quantitative evaluation of the effect of rPMS on muscle strength and muscle tension of paralyzed upper limbs.12–14 There is still no definitive evidence to support rPMS as a routine adjunct treatment for hemiplegia. 15
This study was set up to investigate whether treatment with rPMS to the upper limb extensors in combination with standardized rehabilitation therapy improves the recovery of upper limb strength and function in people of subacute stroke with poor prognostic indicators of arm function.
Methods
The study was a single-centered single blinded randomized controlled trial with independent assessors conducted at the First Hospital of China Medical University between March 2018 to January 2020. This study was reviewed and approved by the Ethical Review Committee of the First Affiliated Hospital of China Medical University, registered at Chinese Clinical Trial Registry (ChiCTR1800016600) and drawn up in accordance with the CONSORT statement guideline. Written informed consent was obtained from each participant. Participants were assessed and enrolled in this study, if they fit the criteria and gave consent to participate.
Inclusion criteria included (1) first-ever unilateral ischemic or hemorrhagic stroke in the basal ganglia with a course of one week to four weeks; (2) medically stable; (3) age 30–80 years; (4) a Brunnstrom Stage of 1 to 2 for the upper limb and hand; and (5) ability to provide written informed consent. The exclusion criteria were (1) severe spasticity of an upper extremity, with a score of more than three on the Modified Ashworth scale; (2) severe aphasia or cognitive impairment that could prevent informed consent or interfere with the study's behavioral measurements; (3) infection near the stimulation site; (4) deep-vein thrombosis near the stimulation site; (5) unstable fractures of the paretic upper extremity; (6) any contraindications to rPMS (e.g. metal implants in the affected limb or use of a pacemaker); or (7) use of muscle relaxants such as baclofen or tizanidine or injections with Botulinum Toxin A for post-stroke spasticity. Using published data showing the baseline upper extremity upper extremity Fugl-Meyer Assessment scores of stroke patients 16 and clinical important changes induced by rehabilitation, 4 it was estimated that at least fourteen patients in each group would give 90% power to detect a significant (p < 0.05) difference between the groups.
We investigated the efficacy of 2 weeks of daily rPMS on motor recovery. The subjects were randomly assigned to two groups: rPMS group treated with rPMS prior to conventional physiotherapy; control group treated with conventional physiotherapy. One clinician generated the allocation sequence according to a software-based randomization scheme. Another doctor of the team enrolled participants and assigned them to one of the two groups according to the randomization scheme.
Each individual in the rPMS group received rPMS daily for fourteen consecutive days using a magnetic stimulator connected to a round coil with a 15-cm diameter (VCY circular coil,Magneuro 60, Nanjing, China). rPMS was applied to the belly of paretic triceps brachii and extensor digitorum (Figure 1C, D). The protocol was as follows: 20 Hz stimulation for 0.5 s per session, with a 2 s interval between sessions, 120 sessions per muscle, a total of 2400 pulses per treatment. The stimulation intensity of triceps brachii was determined as follows: the participant took a comfortable sitting position and placed the hemiplegic upper limb on a smooth tabletop with shoulder abduction 90 ° and elbow joint flexion 90 °. The center of the VCY circular coil was placed in the belly of triceps brachii muscle, and the frequency was set at 20Hz; the intensity was gradually increased from 0% of the instrument's maximum output until 30 ° elbow extension was induced, and the intensity was set as the treatment intensity (Figure 1A). The method to determine the stimulation intensity of extensor digitorum was as follows: the participant was in a comfortable sitting position, the forearm of the hemiplegic side was placed on the smooth tabletop, the hand was in neutral position, the circle center of the coil was aligned with the muscle belly of the extensor muscles of the fingers; the magnetic stimulation intensity was gradually increased from 0% until the wrist joint was extended by 45 ° and this intensity was set as the treatment intensity (Figure 1B). After measurement, the magnetic stimulation intensity fluctuated from 15% to 30% of the maximum instrument output (4 Tesla).
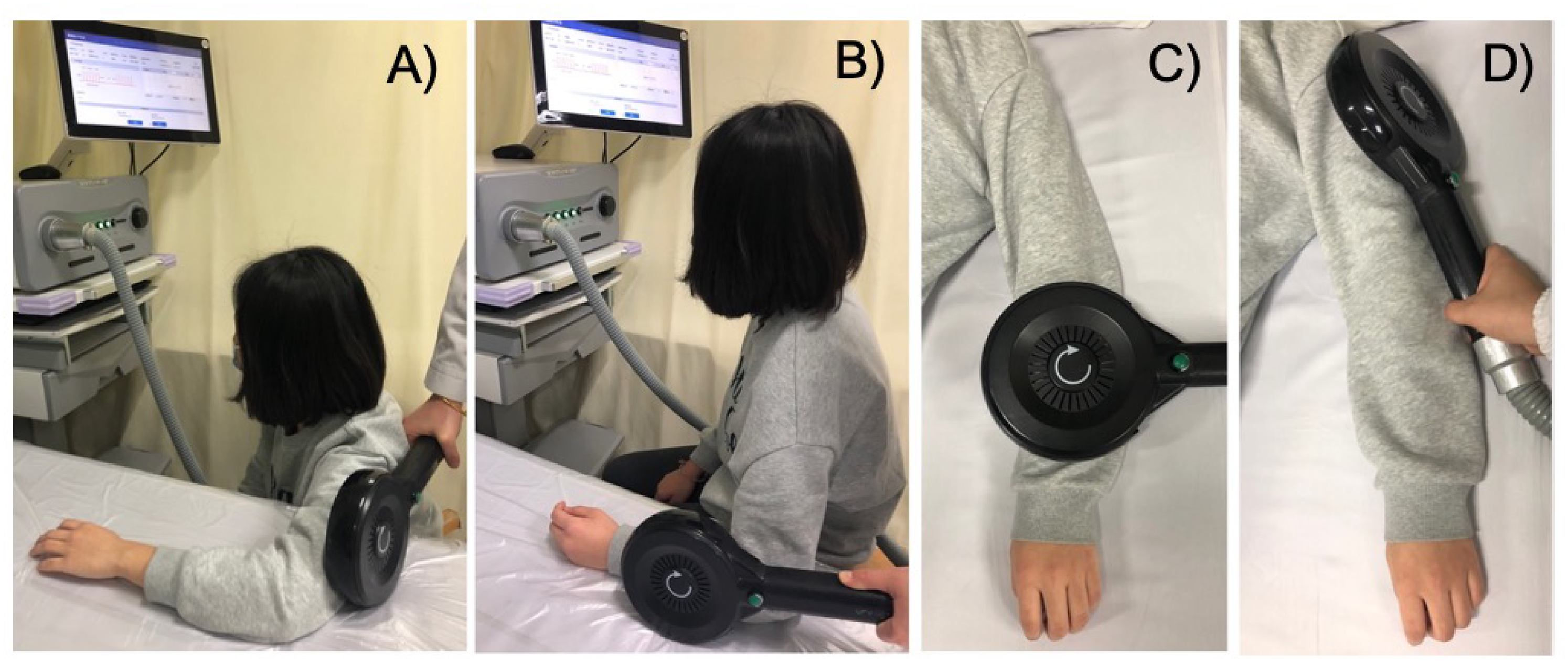
rPMS of triceps brachii and extensor digitorum mucsles to determine the intensity of stimulation (A, B) and to treat (C, D).
The conventional physiotherapy included one session per day of conventional physical therapy, occupational therapy and neuromuscular electrical stimulation. 17 Daily programs of physical therapy and occupational therapy included muscle stretching, passive and passive-assisted mobilization, progressive neuromuscular facilitation training, and task-oriented training lasting 40 min conducted by two therapists blinded to group allocation. The two groups of subjects also received the neuromuscular electrical stimulation therapy: three pairs of electrodes (VitalStim 5951, DJO, USA) were placed at the fullest part of the paretic supraspinatus muscle, deltoid muscle and triceps brachii muscle, respectively. The intensity of electric stimulation was set to induce apparent contraction of the above muscles (20–30mA) and not cause evident contraction of the upper limb's flexor muscles (20 min each time, once a day, for 14 days).
Clinical efficacy was assessed by the upper-extremity motor section of the Fugl-Meyer Motor Assessment Scale, the Barthel Index, 18 and Modified Ashworth scale. Surface electromyography was used for muscle activation evaluation. Clinical scores and surface electromyography were assessed at baseline and after two weeks of treatment. Each evaluation was performed by a clinician (for clinical rating) and neurophysiologist (for surface electromyography recordings) who were blinded to the experimental condition of the participant.
The primary outcome was defined as the improvement in the upper extremity Fugl-Meyer Assessment after a 2-week treatment. Secondary measures included the absolute change in the Barthel Index and root mean square-surface electromyography after treatment.
Surface electromyography was used to quantify muscle strength and spasticity. The root mean square represents the signal power in the time domain and has been used to measure the muscle activation. 19 The root mean square signals of maximal isometric contraction and stretch-induced spasticity of the paretic upper limb's key muscles were collected at baseline and after treatment. After skin preparation (i.e. cleaning the skin with alcohol), the bipolar sensors of the circular electrode (1 cm diameter, CH55RD, CATHAY MANUFACTURING CORP., Shanghai, China) with adhesive skin interfaces were installed on each participant (fixed 1 cm distance between electrodes; 10-channel surface electromyography System, FlexComp Infiniti System, Thought Technology, Canada). The bipolar surface electromyography electrodes were placed around the recommended sensor location with the orientation parallel to the muscle fibers of the biceps brachii, triceps brachii, extensor digitorum, and flexor digitorum strictly following surface electromyography for non-invasive assessment of muscles (SENIAM) guidelines (http://www.seniam.org/) and using anatomical landmarks. Each electrode position was marked on the skin to ensure consistency between sessions.
The muscle strength evaluation method is as follows. The subject sat on a chair with arms resting in a relaxed position. According to the instrument's instructions, record the baseline electromyography signal with the subject completely relaxed for the first 20s. Then, the participant was instructed to do the maximum isometric contraction of the four muscles mentioned above lasting 5 s each: the movement of elbow flexion, elbow extension, grasping with fingers, and hand opening. Measurements were performed repeatedly three times with 5 s rest between sessions.
The muscle tension evaluation method is as follows. The subjects completely relax and lie on their backs on the bed. After obtaining the baseline electromyography signals, the target muscle was passively stretched within 1–2s, collecting the electromyography signal for 5s, then relaxed for 5s, repeated the passive stretching three times. The methods of the passive stretch of muscles are as follows: biceps brachii-constant speed passive movement of elbow joint from complete flexion to full extension; triceps brachii-constant speed passive movement of elbow joint from full extension to complete flexion; flexor digitorum-constant speed passive movement of metacarpophalangeal joint, interphalangeal joint and wrist joint from complete flexion to complete extension; extensor digitorum-metacarpophalangeal joint, interphalangeal joint, and wrist joint move passively at a constant speed from full extension to complete flexion. The sampling frequency was set to 2048 Hz. The Biograph Infiniti software (Thought Technology, Canada) automatically analyzes the average root mean square value of three active contractions and three passive drafting, representing muscle strength (strength-root mean square) and spasticity (tension-root mean square) respectively.
Statistical analysis was performed using the SPSS software (version 26.0, Inc. Chicago.) The groups’ baseline values were compared by either a t-test for continuous data or a chi-squared test for categorical data. We evaluated whether the assessment scores were normally distributed using the Shapiroe Wilk test A paired t-test or Wilcoxon rank-sum test was used to compare the Fugl-Meyer Assessment, Barthel Index, and root mean square-surface electromyography values between baseline and posttreatment within each group. The absolute change of upper extremity Fugl-Meyer Assessment, Barthel Index, and root mean square values from baseline to after treatment was compared by the t-test or Mann-Whitney U. Outcomes were expressed as mean with standard deviation (SD), median (inter- quartile range (IQR)), or n. P < 0.05 was considered significant.
Results
A CONSORT diagram explaining flow of participants through the study is shown in Figure 2. The groups’ demographic characteristics were quite similar at a baseline level in age, sex, lesion side, stroke type and location, number of days from the stroke event, or severity of hemiplegia as assessed by upper extremity Fugl-Meyer Assessment score and Brunnstrom stages (Table 1). The procedure was well tolerated, and all the participants complete the whole course of treatment. No adverse reactions occurred during the treatment.
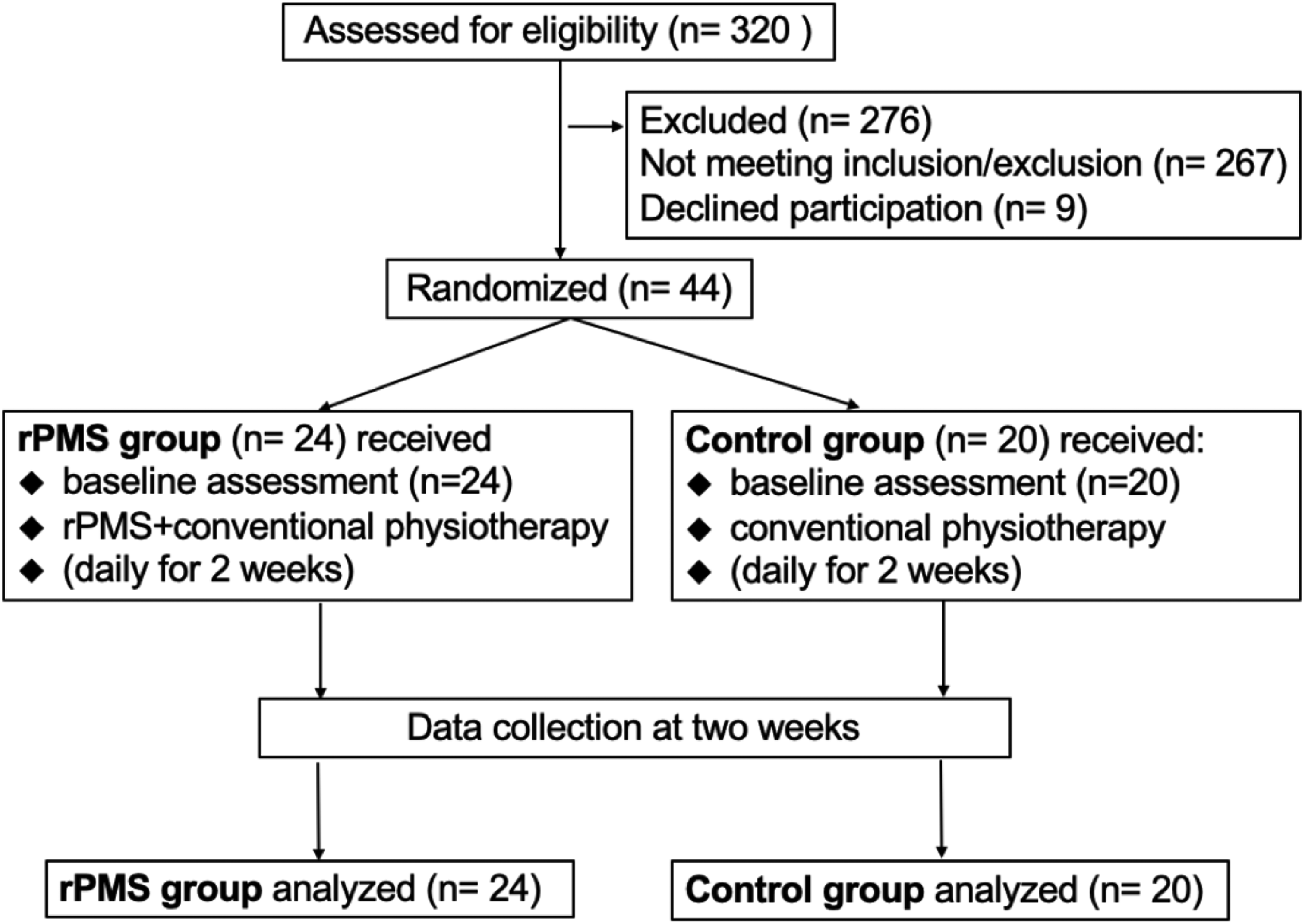
CONSORT flow diagram.
Demographic and clinical data.
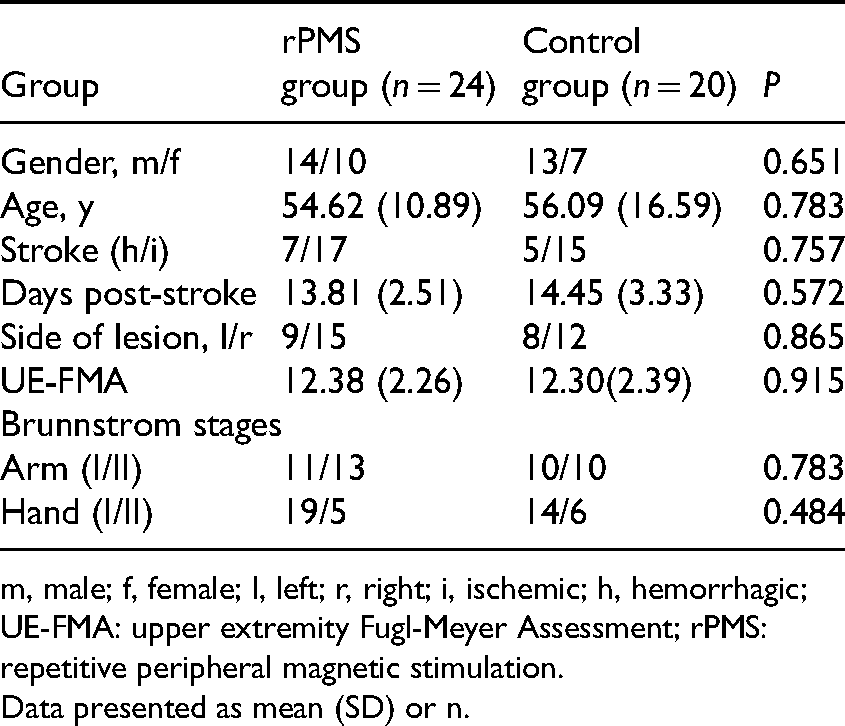
m, male; f, female; l, left; r, right; i, ischemic; h, hemorrhagic; UE-FMA: upper extremity Fugl-Meyer Assessment; rPMS: repetitive peripheral magnetic stimulation.
Data presented as mean (SD) or n.
Both of the groups had a progressive improvement in the upper extremity Fugl-Meyer Assessment and Barthel Index scores over time (both group P < 0.001, post-intervention compared with baseline, Table 2). All participants in both groups presented a clinically meaningful improvement in the upper extremity Fugl-Meyer Assessment score of 5-point compared with the baseline assessed after treatment. 7 rPMS group showed more significant improvements in the upper extremity Fugl-Meyer Assessment and the Barthel Index (P < 0.001, Table 2) compared to control group. The rPMS group presented a much larger increase rate than the control group in upper extremity Fugl-Meyer Assessment (100.8% vs. 56.9%) and Barthel Index (50.0% vs. 33.3%).
Changes in muscle strength and tension represented by strength-root mean square and tension-root mean square.
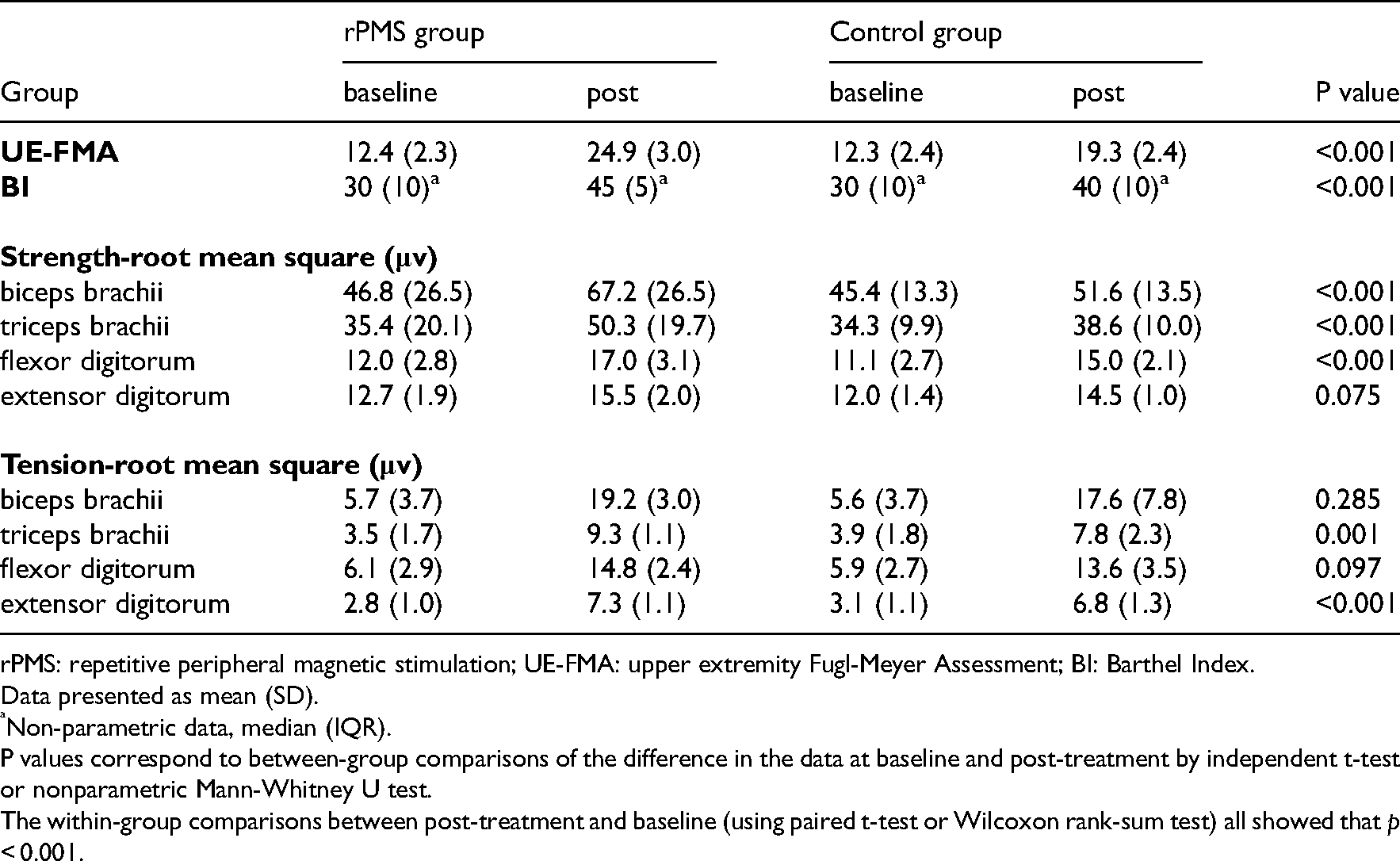
rPMS: repetitive peripheral magnetic stimulation; UE-FMA: upper extremity Fugl-Meyer Assessment; BI: Barthel Index.
Data presented as mean (SD).
Non-parametric data, median (IQR).
P values correspond to between-group comparisons of the difference in the data at baseline and post-treatment by independent t-test or nonparametric Mann-Whitney U test.
The within-group comparisons between post-treatment and baseline (using paired t-test or Wilcoxon rank-sum test) all showed that p < 0.001.
In the surface electromyography-based evaluation, a paired t-test showed a significant increase in strength-root mean square and tension-root mean square for all the four tested-muscles posttreatment compared with baseline in both groups (p < 0.001). The independent-sample t-test showed that the increases in strength-root mean square values of biceps brachii, triceps brachii, and flexor digitorum (p < 0.001) after treatment in the rPMS group were more significant than those in the control group (Table 2). The rPMS group presented a much higher rate of rise in strength-root mean square compared with control group (biceps brachii: 43.8% vs. 13.7%; triceps brachii: 42.1% vs. 12.5%; flexor digitorum :42.5% vs. 36.0%). The increases in tension-root mean square values of triceps brachii (5.8μv (2.2μv) vs. 4.0μv (1.2μv), p = 0.001) and extensor digitorum (4.5μv (0.7|μv) vs. 3.6μv (0.2μv), p < 0.001) after treatment in the rPMS group were more significant than those in the control group. Meanwhile, the modified Ashworth scale values of triceps brachii and extensor digitorum of the participants in the rPMS group did not exceed grade 1.
The six patients in the rPMS group whose modified Ashworth scale was 1 after treatment were given paraffin wax therapy, one kind of heat therapy that has been in use for spasticity due to stroke, 20 for 20 min a day to relieve muscle tension and continued routine rehabilitation therapy. One week later, the spasticity of triceps brachii disappeared (modified Ashworth scale was 0) and tension-root mean square values were all less than ten µv.
Discussion
The main findings of this randomized controlled study are that rPMS of the extensor muscles of the affected upper extremity significantly improves upper extremity function (upper extremity Fugl-Meyer Assessment score from 12.4 to 24.9 points) and daily living (Barthel Index score from 30 to 45 points) in patients with no functional arm movements (a Brunnstrom Stage of 1 to 2) during the early subacute phase of stroke. Employing surface electromyography, we also found the combination of rPMS of upper limb extensors and routine rehabilitation could promote the recovery of muscle strength for grip and elbow flexion and extension more than standard rehabilitation. It is necessary to conduct a long-term follow-up study to prove the efficacy of rPMS further, providing evidence to support the use of rPMS as a routine adjunct treatment for hemiplegia.
We summarize the studies on rPMS effects on hemiplegic upper limbs that can be found in the Pubmed database.10–14 There's only one RCT study conducted by Krewer et al. demonstrated that the two weeks of rPMS could improve sensory function, not spasticity and motor function, 12 which may be due to the extensive range of disease course of the included patients, two weeks to 9 years. The brain plasticity is the strongest in the subacute stage after stroke, and the sensitivity to treatment response decreases in the chronic and sequelae stage. 21 A recent case-control study on acute stroke showed that the progress rate of upper extremity Fugl-Meyer Assessment adjusted by treatment duration was more significant for rPMS plus standard care than standard care, which was consistent with the results of this study. 11 Similarly, a recent self-control study suggests that rPMS could improve upper limb function and shoulder pain. 10 Strupler et al. found that a single rPMS treatment on the extensor muscle of the finger and hand could alleviate the spasm of the flexor muscle of the finger and improve the finger activity in a case series.13,14 It is improper to compare their experiment with this study because the included patients have different degrees of spasticity (Ashworth scale 3–4 vs. below 3) and differences between single and multiple treatments. Quantitative evaluation of the impact of several rPMS on muscle strength and muscle tension is critical to guide clinical application.
The root mean square value of surface electromyography can represent muscle strength and tension more quantitatively and precisely than clinical grading, hand-held dynamometer, and joint movement angle.22–25 Through the surface electromyography examination, we found that rPMS could clearly and rapidly enhance patients’ muscle strength. rPMS increased the muscle strength of stimulated triceps brachii and unstimulated biceps brachii and flexors digitorum more significantly than the control group, indicating the profound penetration effect of rPMS. Deng et al. have studied the half-value depth of the circular coil on the head is 1.0–3.5 cm. 26 The half-value depth represents the penetration depth of the electric field generated by transcranial magnetic stimulation, defined as the radial distance from the cortical surface to the deepest point where the electric field strength is half of its maximum value on the cortical surface. 26 When the circular coil is used for peripheral stimulation of muscle and nerves, a greater penetration depth may be produced because there is no magnetic field attenuation caused by skull thickness. Thus the rPMS acted on the extensors of the upper limb may penetrate to stimulate the flexors. There was no significant difference in strength-root mean square of extensor digitorum between the two groups, which may be due to the slow recovery of distal limb function. Perhaps the combination of rPMS and neuromuscular electrical stimulation will be more effective than single stimulation, which should be further studied in the future.
The specific mechanism of peripheral magnetic stimulation in promoting muscle strength recovery in hemiplegic patients is not clear. Peripheral magnetic stimulation can produce sensory input, including direct activation of sensorimotor nerve fibers and indirect activation of mechanoreceptors during rhythmical contraction and relaxation. 9 Enhancement of sensory input can enhance excitability of the motor cortex and upper limb performance. 27 Stroke patients are already subject to extensive sensory stimulation during standard care, such as exercise therapy and electrical peripheral nerve stimulation, which could facilitate learning by offering intensification of sensory input from the paretic limb. 27 Functional magnetic resonance imaging has proved that certain intensity of neuromuscular electrical stimulation increases excitability of corticomotor pathway, with a significant activations of the sensorimotor network, cerebellum and thalamus. 28 As another kind of peripheral stimulus, rPMS may share these effects, or it may have special mechanism, which still needs to be studied.
At the same time, we found that rPMS tends to induce an increase in muscle tone. The tension-root mean square values of the stimulated extensors in the rPMS group were significantly higher than those in the control group, but the modified Ashworth scale values did not exceed grade 1. In the motor recovery course, the upgrading of Brunnstrom stages is accompanied by increasing and decreasing muscle tone. Increased muscle tone may play a meaningful role in the functional task. The effect of rPMS on muscle spasm is rarely studied, and the reduction of spasticity observed by one treatment could not represent the effect of multiple treatments.13,14 Plenty of randomized controlled studies and systematic reviews shown that neuromuscular electrical stimulation, as an adjunct to rehabilitation therapy, could not affect spasticity.29–31 We ponder that rPMS may increase muscle tension while enhancing muscle strength. In this study, the slightly increased tension of the stimulated muscles could be relieved after 1 week of paraffin wax therapy, providing new ideas for patients with muscle weakness and severe spasticity. In that case, rPMS should combine with paraffin therapy or other antispasmodic therapy to strengthen muscle and avoid the aggravation of spasm.
There are some limitations to this study. The magnetic stimulation was limited to triceps brachii and extensor digitorum. If magnetic stimulus is applied to shoulder muscles such as supraspinatus and deltoid muscles, and upper limb flexors, it may induce more functional movement. Furthermore, this study included patients of early subacute stroke with severe upper limb impairment, but whether rPMS was effective in patients with mild to moderate impairment in the chronic stage still needs to be studied.
In patients with no functional arm movement after stroke, early application of rPMS on the upper extremity extensors increases muscle strength of grip and elbow flexion and extension, decreases the upper limb impairment, and improves daily living ability. rPMS could quickly induce muscle strength recovery, and its effect of increasing muscle tension is controllable. These findings would contribute to the justification for specific treatment parameters to maximize upper limb recovery after stroke.
Clinical messages
rPMS of the extensor muscles of the affected upper extremity significantly improves upper extremity function and daily living in patients with no functional arm movements during the early subacute phase of stroke.
rPMS may increase muscle tension while enhancing muscle strength.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Department of Science and Technology of Liaoning Province (grant number 2013225049). Clinical trial registration number: ChiCTR1800016600.