
Abstract
Objective
To determine acupuncture-related treatments’ effects and duration on improving cognitive function, physical function, and quality of life in patients with Alzheimer's disease.
Data sources
Eight electronic databases were searched for eligible randomized controlled trials from database inception to January 2021, including Medline, PubMed, EBSCO, Embase, Cochrane, Airiti Library, China National Knowledge Infrastructure, and China Journal Full-text Database.
Review methods
A systematic review and meta-analysis were conducted on acupuncture types, cognitive function, activity of daily life, muscle strength and quality of life.
Results
Sixty-six studies in total with 4191 participants, the overall risk of bias was classified 60% as low and 24% as high. Acupuncture-related treatments for cognitive function and self-care ability revealed a moderate effect size, with a significant difference in noninvasive and invasive remedies (p < 0.001). Cognitive function showed significant differences in 6, 8, 12, and 24 weeks while self-care ability in the latter two weeks (p < 0.001). Meta-regression analysis showed cognitive function increased by 0.05 points (p = 0.002) and self-care ability decreased by 0.02 points (p = 0.04) after weekly treatment. There was a significant difference in muscle strength (p = 0.0003).
Conclusion
Acupuncture-related treatments effectively improved cognitive function with the treatment lasted 6 weeks at least, but self-care ability started showing effects after 12 weeks of treatment. The improvement of muscle strength was also confirmed. Acupuncture-related treatments, particularly noninvasive ones, have few complications and high safety, perhaps providing patients and caregivers diversified choices and clinical care guidelines for reference.
Introduction
Alzheimer's disease is a degenerative neurological illness, and its risk increase with age; it is the most common causes of dementia and elderly disability, accounting for 60%–80% of cases globally. 1 Alzheimer's disease can develop from mild cognitive impairment and eventually dementia. Cognitive decline affects daily activities and physical function, 2 like daily activities, muscle strength ought to be considered an important physical function. 3 Considering the aging population, dementia is the leading challenge for healthcare systems and the foremost public health concern. However, medication for Alzheimer's disease has been shown to slow the cognitive decline but not modify the disease's course. 4 Non-pharmacological interventions are crucial options for treating Alzheimer's disease.
Among these non-pharmacological interventions, acupuncture-related treatments were opted by 78% of patients with dementia and yielded delayed cognitive decline and improved quality of life. 5 Acupuncture-related treatments are accomplished at specific acupoints located on meridians or collaterals, which belong to ancient Chinese medicine and have been used regularly in clinics for thousands of years. 6 These treatments have gained increased interests worldwide in recent years,7,8 and been applied with safety and efficacy in clinical practice following the empirical research. 9 However, different acupuncture-related treatments yield different results.
The present study therefore aimed to determine whether these different acupuncture-related treatments hold promise in improving cognitive function, physical function and quality of life.
Methods
A systematic review and meta-analysis of randomized controlled trials was conducted for eligible studies published from database inception to September 30, 2021. The study protocol was registered in the International Prospective Register of Systematic Reviews (ID: CRD42020196741). The review was reported following the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidance. The participants, intervention, comparison, outcome, and study design (PICOS) form was used to compose key questions. Alzheimer's patient (P) were treated with acupuncture-related treatments (I), usual care, medication, and sham acupoint stimulation (C) to evaluate the effect of acupuncture-related treatments on cognitive function, self-care ability, muscle strength or quality of life (O).
Eight electric databases were searched for the present study, namely MEDLINE in Ovid, PubMed, EBSCO (CINAHL, SportDiscus and MEDLINE with full text), Embase, Cochrane Library, AiritiLibrary, China National Knowledge Infrastructure, and China Journal full-text Database. Text words and medical subject headings (MeSH) terms were used to search. The following search strategy were applied: P (‘Alzheimer*’OR ‘dement*’ OR ‘cognit* impair*’, I (‘acupoint’ OR ‘acupuncture’ OR ‘electro-acupuncture’ OR ‘scalp-acupuncture’ OR ‘acupressure’ ‘auricular acupoint’ OR ‘moxibustion’ OR ‘transcutaneous electrical acupoint stimulation’), O (‘cognit* function’ OR ‘physical activit*’ OR ‘activities of daily living’ OR ‘quality of life’), and S (‘controlled trial’ OR ‘controlled study’ OR ‘controlled design’). For more detailed information search strategy, see the appendix. Titles and abstracts were screened according to the eligibility criteria. Afterwards, the full-text of the studies meeting the selection criteria was further reviewed for inclusion in the systematic review. In additional to electronic database searching, handsearching was performed, which checked reference lists for locating studies in systematic reviews and included studies for relevant studies.
Participants types. The present study included participants diagnosed as having Alzheimer's disease, irrespective of sex, age or disease duration with early to mid-stage cognitive impairment. Individuals cognitive impairments due to other factors (such as vascular dementia, dementia with Lewy bodies, frontotemporal dementia, parkinsonism disease dementia, and pre-senile dementia), or other mental disorders (such as schizophrenia and depression) were excluded.
Intervention types. Acupuncture-related treatments provided to individuals in the present study were a priori differentiated into seven types, namely needle-acupuncture, electro-acupuncture, scalp-acupuncture, body acupressure, auricular acupressure, moxibustion and transcutaneous electrical acupoint stimulation. Broadly, acupuncture includes various techniques of acupoint stimulation.
Comparison types. The included interventions were compared with usual care or medicine. Usual care was defined as ordinary participation in activities offered. Western medication was defined as treatment of symptoms and diseases by using drugs provided by medical doctors and other health care professionals such as nurses, pharmacists, and therapists.
Outcome measures types. The primary outcome was cognitive function as measured using validated assessment tools, including the mini-mental state examination, Hasegawa's dementia scale, and Montreal cognitive assessment. The secondary outcomes of physical function were self-care ability measured using the activities of daily living and the Barthel Index, and muscle strength measured using the timed up and go test Quality of life was measured using the quality of life in Alzheimer's disease scale and the World Health Organization quality of life instrument-older adult module.
Studies types. The criteria for inclusion were randomized controlled trials with no limits on publication date. Papers written in English or Chinese were considered.
After the titles and abstracts from the search results on the electronic databases were browsed, the full-texts of all potentially eligible studies were downloaded and analyzed. Relevant data, including the title, first author, publication year, study design, intervention for each group, outcomes, and dropouts, were independently extracted and confirmed by the research team (C.L, Y.C. and D., M., T.Y., respectively) based on the inclusion criteria. A research team obtained information from the included studies. Doubts and discrepancies were resolved through discussion. The quality of all included studies in this review was independently evaluated by the research team by using the Cochrane collaboration tool for assessing risk of bias 2.0. 10 This instrument consists of six domains: bias risk arising from the randomization process, bias risk due to deviations from the intended interventions (effect of adhering to intervention), risk of missing outcome data, bias risk in measurement of the outcome, bias risk in selecting of the reported result, and overall risk of bias. The tool ranks the research studies as having high (definitely yes), low (definitely no), and unclear (probably yes or probably no) bias levels. Each study was assessed by research team reviewers independently. Any disagreement was resolved through discussion.
Statistical analyses were performed using Cochrane Review Manager 5.3 and Comprehensive Meta-Analysis. The mean difference (MD) or standardized mean difference (SMD) and 95% confidence interval (CI) were used to represent results. A random-effects model was used to pool each treatment effect due to the clinically diverse nature of included studies. A forest plot was used to summarize intervention effects, heterogeneity was examined using the χ2 test with the Cochrane's Q and I2 statistics. A potential publication bias was qualitatively evaluated using Egger's test Furthermore, the meta-regression analysis was used to analyze the effect between the interventions and duration. A p value of <0.05 was considered statistically significant.
Results
Figure. 1 shows the flow diagram of the study selection process. In the initial search, 2420studies met the search criteria. Of these, 1093 were eliminated as duplicates and 972 were eliminated due to poor fit with the topic. After the titles and abstracts of the remaining 121 articles were review, 22 more studies were eliminated because they used other interventions and 19 were eliminated because they used other research designs. The reviewers read the entire texts of the remaining articles and used the inclusion criteria to identify 69 studies.11−77
PRISMA flow diagram for systematic reviews and meta-analysis of acupuncture-related interventions in Alzheimer's disease.
Table 1 shows the characteristics of included studies on acupuncture-related treatments in Alzheimer's disease, consisting of 4273 participants in total. The average dropout rate of participants was 10.34% (n = 442), four studies reported a rate in excess of 20%.19,22,29,37 The participants consisted of 45.1% (n = 1929) men and 43.4% (n = 1854) women. The age ranged from 60 years to 88 years, with an average of 64.70 years which were similar in the experimental and control groups. Disease duration ranged from 3 months to 8.20 years, with an average of 3.57 years. Treatment duration ranged from 10 days to 52 weeks. In total, 13, 18, 23, and 15 studies had lasted interventions for 2-6, 7-8, 9-12, 13-52 weeks, respectively. The control group were mostly provided usual care such as medication, cognitive training, and sham point stimulation. The evaluated outcomes were cognitive function using at least one measure in 45 studies, self-care ability 31 studies, and muscle strength 7 studies. Only two studies evaluated quality of life, which was not enough for meta-analysis.
Characteristics of nstudies reporting on acupuncture-related interventions in dementia.
Note: d: day; wk: week; mon: month; y: year; HDS: Hasegawa's dementia scale; MMSE: mini-mental state examination; CDR: clinical dementia rating; TENS: transcutaneous electrical nerve stimulation; *invasive acupuncture-related treatments; **noninvasive acupuncture-related treatments.
Figure 2 showed the result of the assessment of risk of bias. For the randomization process, 60% of included studies were classified as low risk bias. For the deviations from the intended interventions, 35% were rated as low risk bias and 65% unclear. For the missing outcome data, 55% were classified as unclear. There 90% and 89% were classified as low risk bias for measurement of the outcome and selection of the reported result, respectively. The overall risk of bias of 69 studies was classified 70% as low and 24% as high.
Risk of bias graph of included randomized controlled trials.
Acupuncture-related treatments to improve cognitive function
Figure 3 shows the forest plots of acupuncture-related treatments for improving cognitive function outcomes, with a significant difference (p < 0.001). Publication bias was not observed in pooled studies by the Egger's test (p = 0.40). The heterogeneity among studies was considered, followed by subgroup analysis under the type and duration of acupuncture-related treatments. Acupuncture- related treatments were invasive in 30 studies and noninvasive in 11 studies. Figure 4 shows both noninvasive and invasive acupuncture-related treatments significantly improved cognitive function (p < 0.001). Figure 5 shows treatment durations were classified as 6, 8,12, and 24 weeks and significant elevations in cognitive function were observed between each treatment duration (p < 0.001). Figure 6 shows the results of meta-regression analyses showed cognitive function scores on the interventions interval per week showed a positive and significant relation slightly (β = 0.05, p = 0.001).
The effect of acupuncture-related treatments on cognitive function.
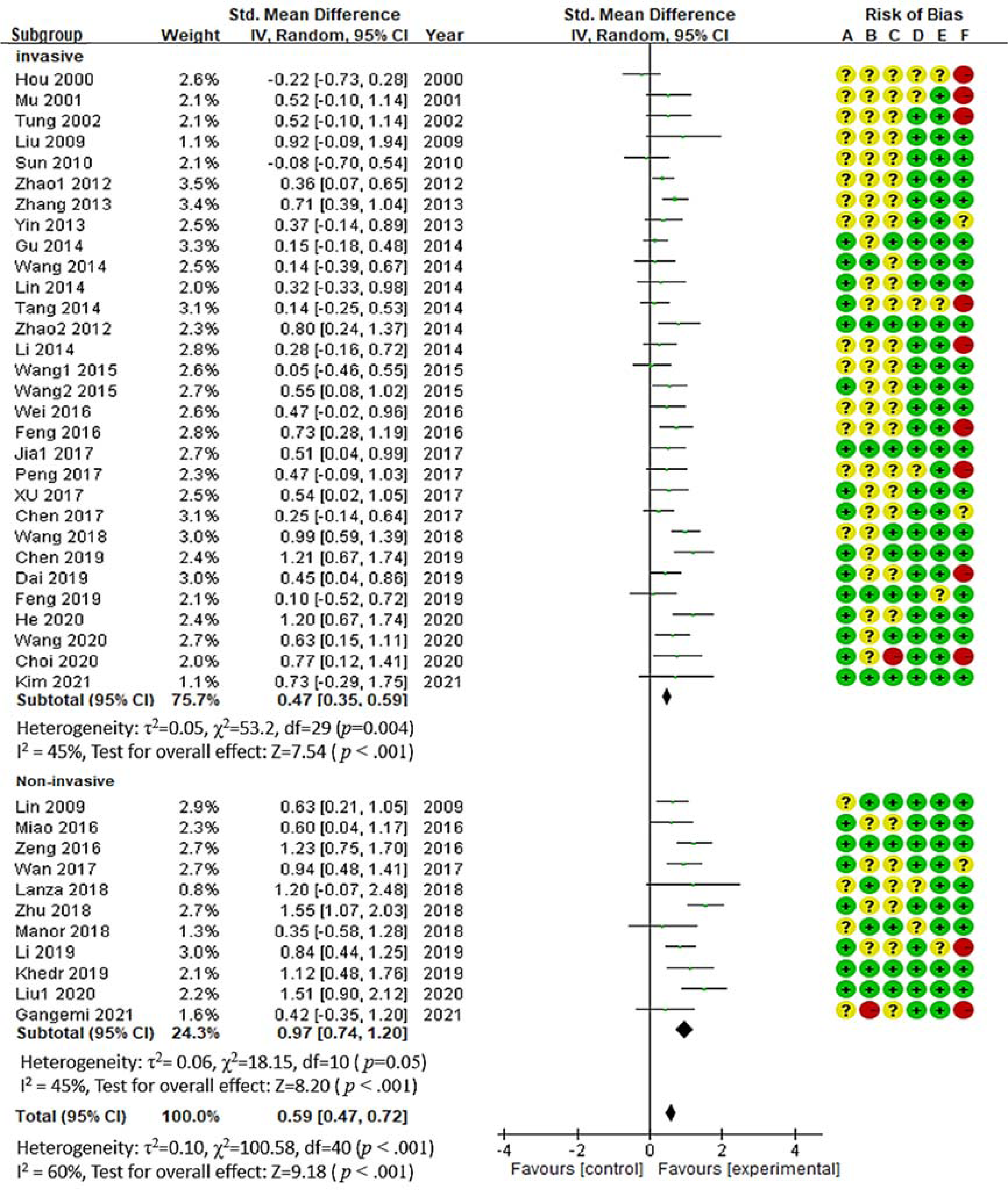
The effect of acupuncture-related treatments by treatment types on cognitive function.
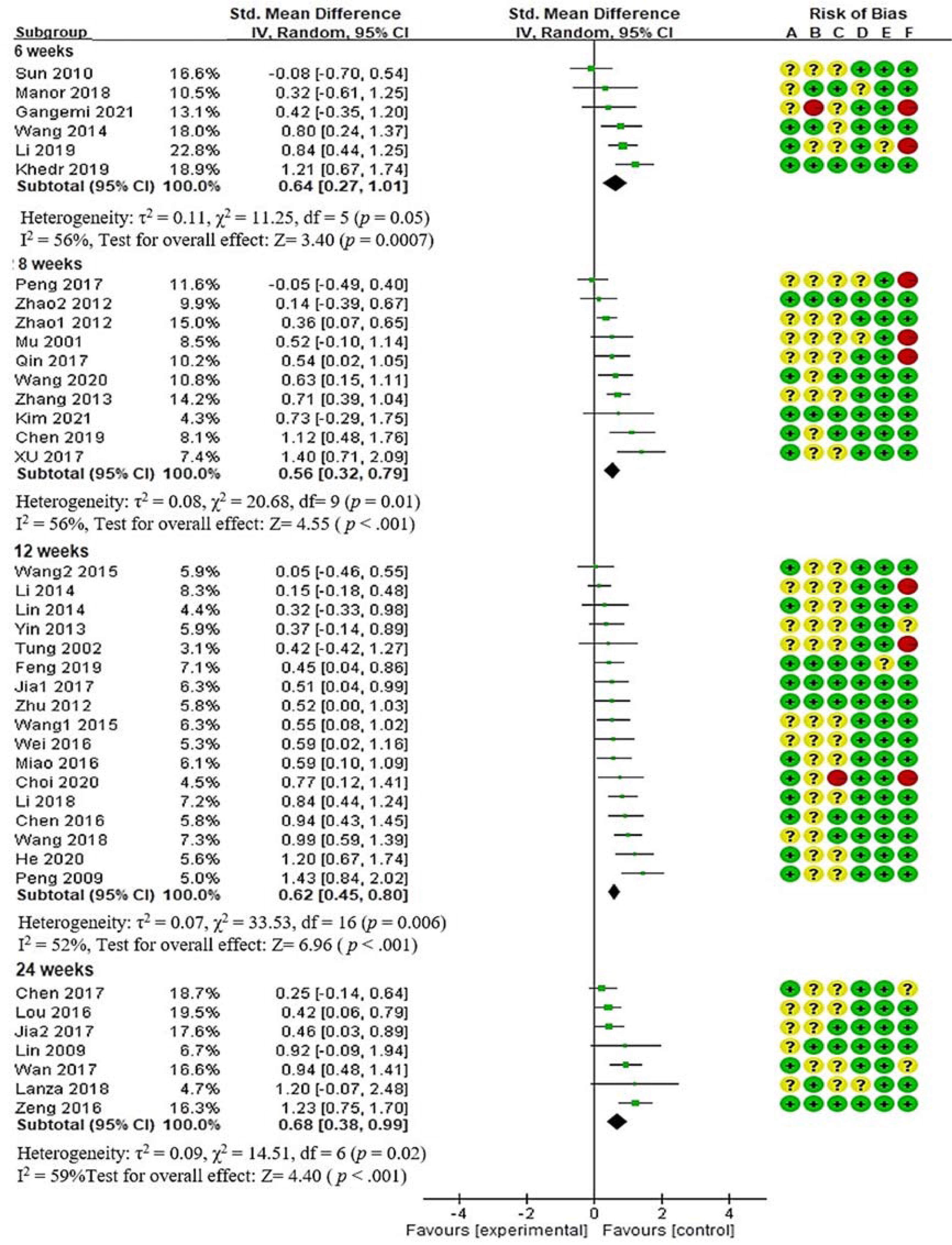
The effect of acupuncture-related treatments by treatment durations on cognitive function.
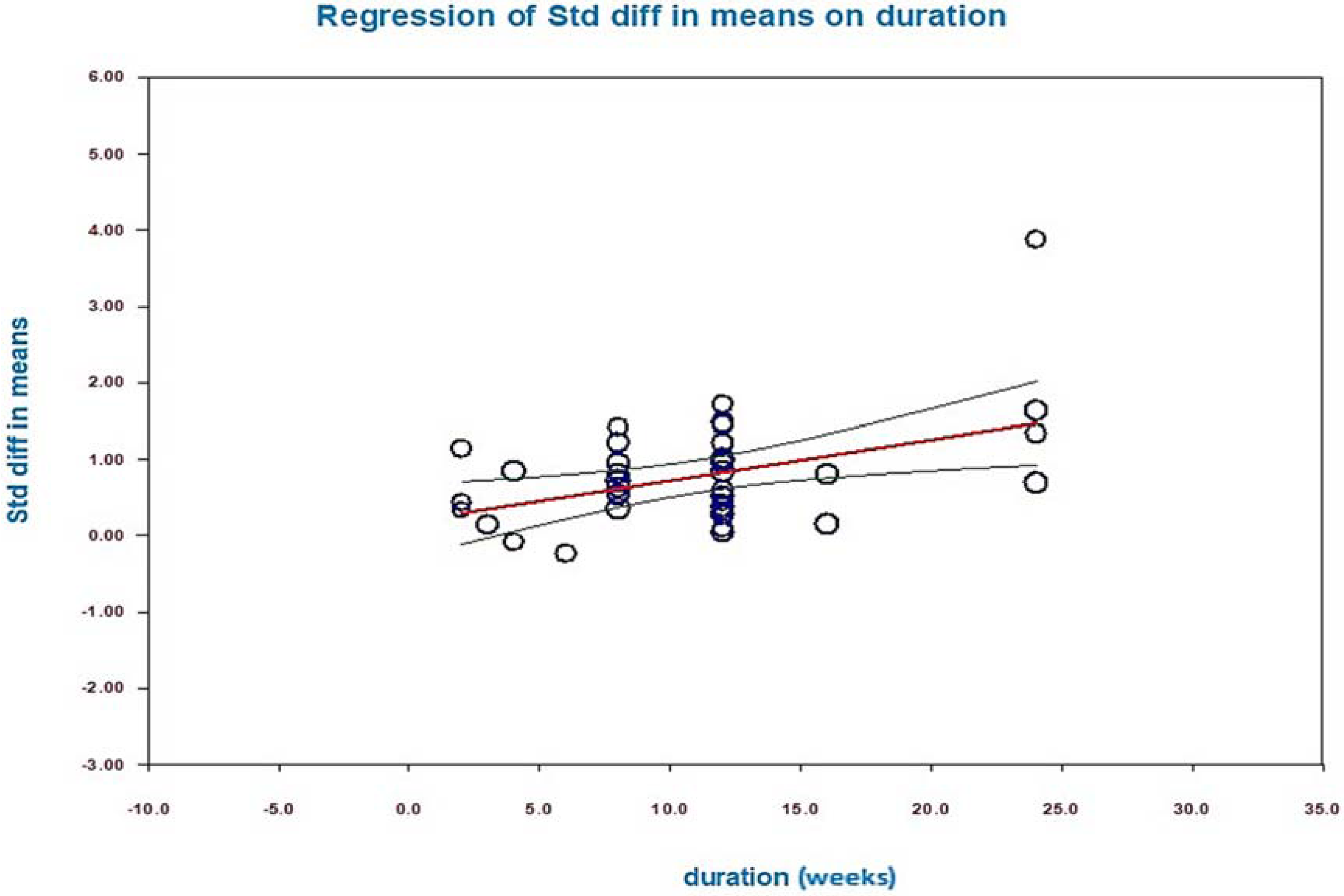
The effect of acupuncture-related treatments of meta-regression analysis on cognitive function.
Acupuncture-related treatments to improve physical function
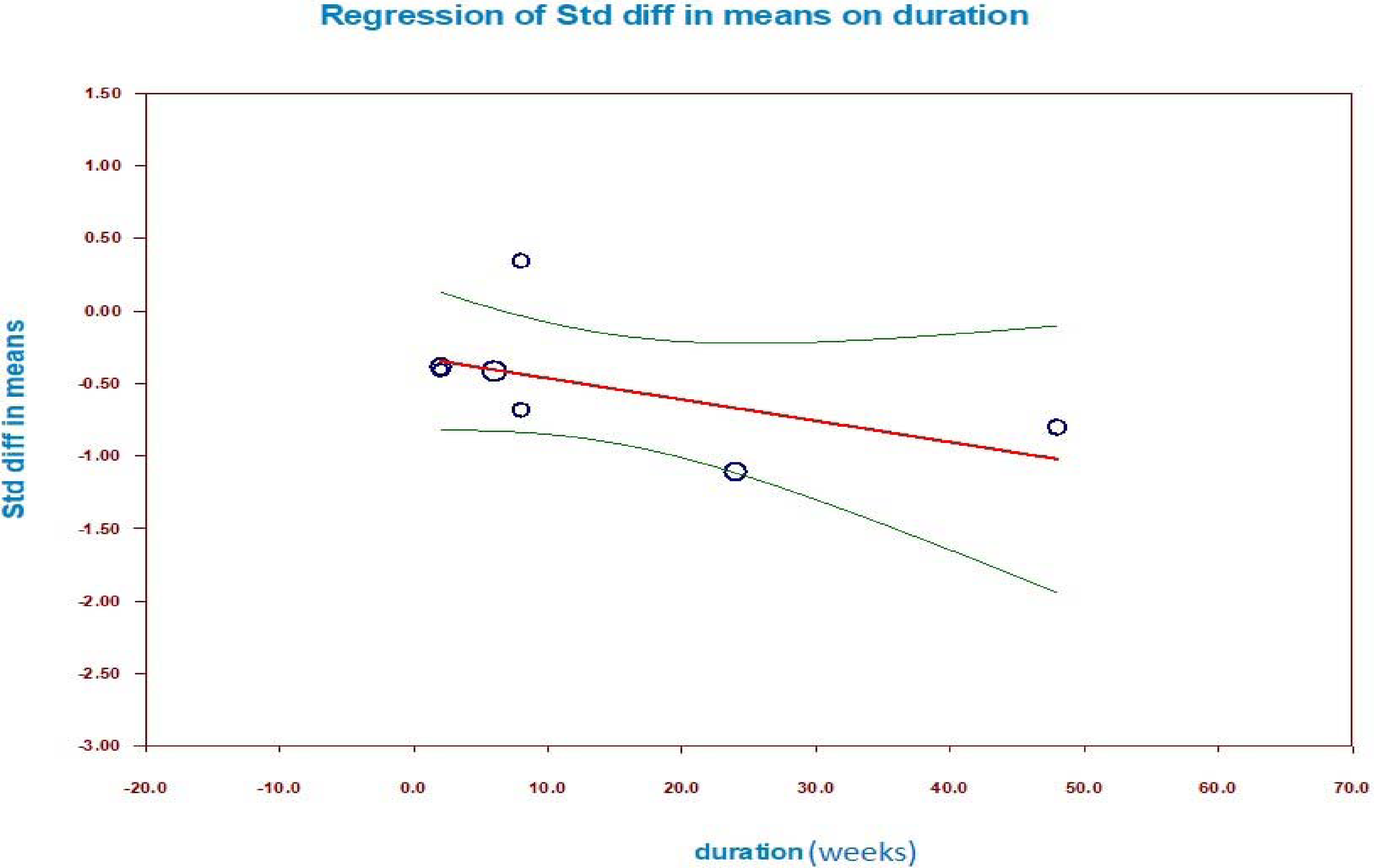
Figure 7 shows forest plots of acupuncture-related treatments for significantly improving physical function, including self-care ability and muscle strength. Regarding self-care ability, data pooling revealed a significant decrease in dysfunction (p = 0.0003). Publication bias was not observed in pooled studies by the Egger's test (p = 0.36). The heterogeneity among studies was considered, followed by subgroup analysis of the type and duration of acupuncture-related treatments. Acupuncture-related treatments were invasive in 16 studies and noninvasive in 6 studies. Figure 8 shows both noninvasive and invasive acupuncture-related treatments significantly improved physical function. Figure 9 shows the different treatment durations were 8, 12, and 24 weeks, revealing a significant increment in 12 and 24 weeks (p < 0.001). Figure 10 shows the results of meta-regression analyses showed physical function scores on the interventions interval per week showed a positive and significant relation (β = −0.02, p = 0.04).
The effect of acupuncture-related treatments on self-care ability
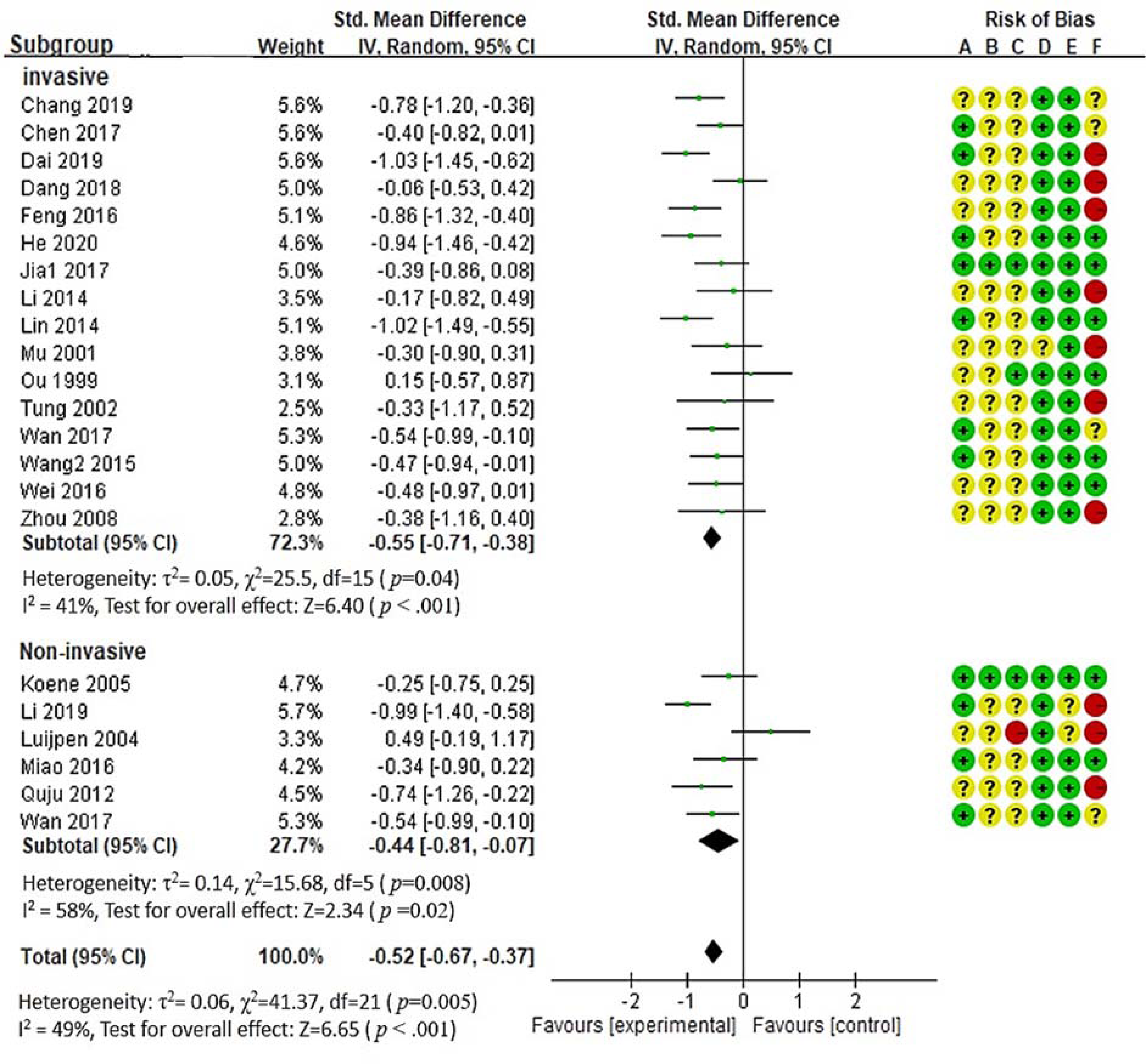
The effect of acupuncture-related treatments by treatment types on self-care ability
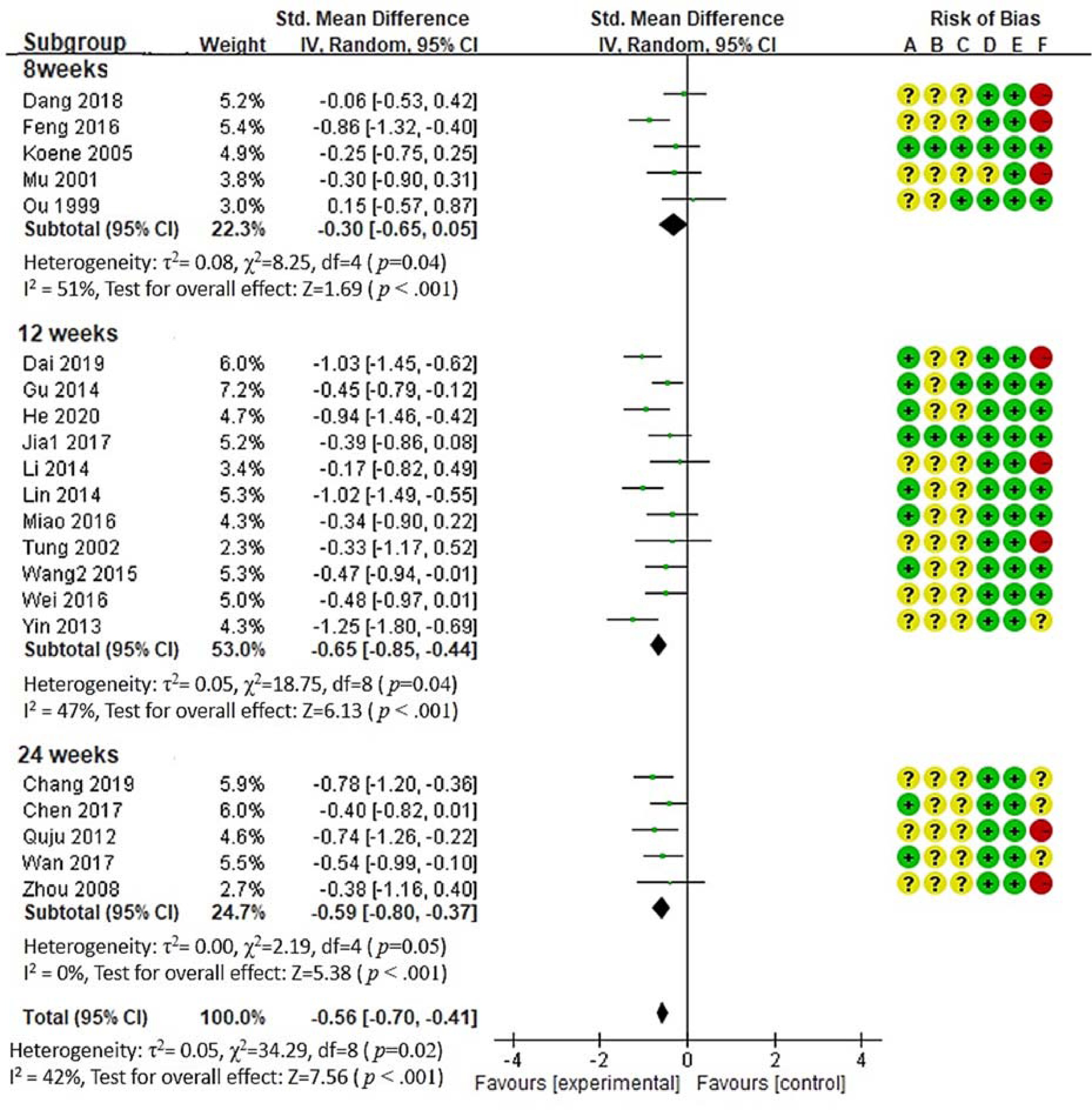
The effect of acupuncture-related treatments by treatment duration on self-care ability
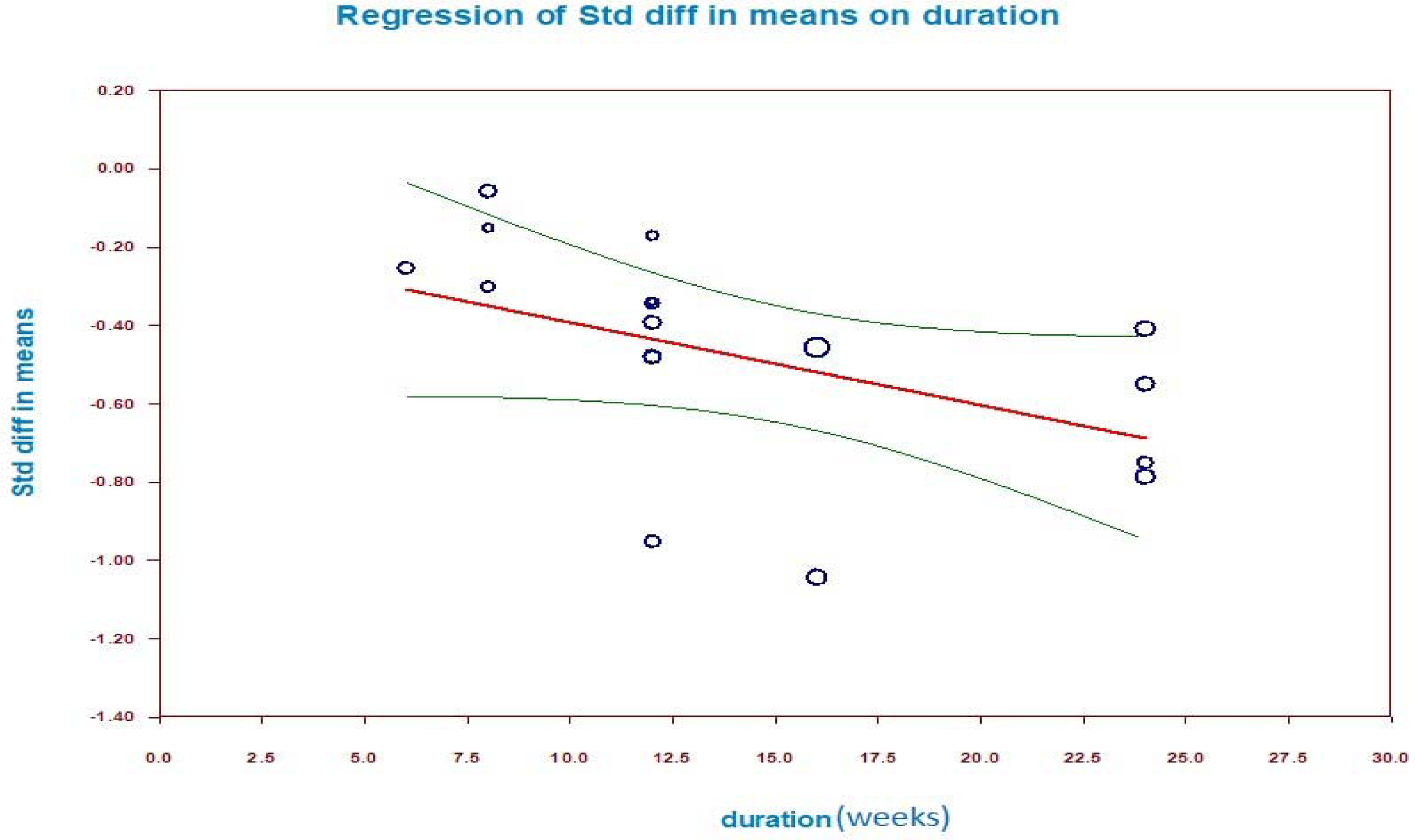
The effect of acupuncture-related treatment of meta-regression analysis on self-care ability.
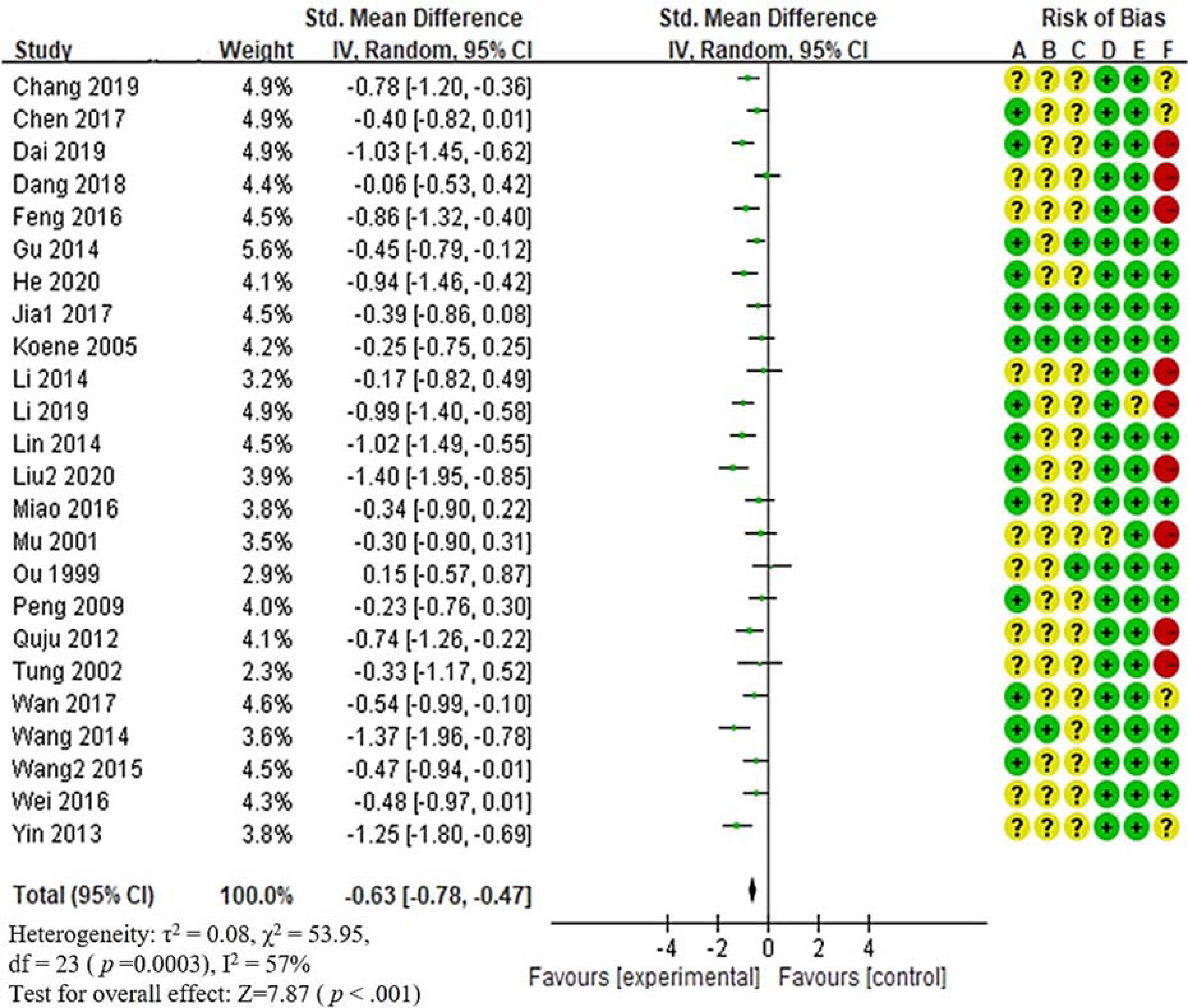
As seen in Figure 11, the data pooling for muscle strength revealed a significant increase in physical function (p = 0.0003). The heterogeneity among differences of studies were not significant (χ2 = 6.68, p = 0.35, I2 = 10%). Publication bias was not observed in the pooled studies by the Egger's test (p = 0.70).
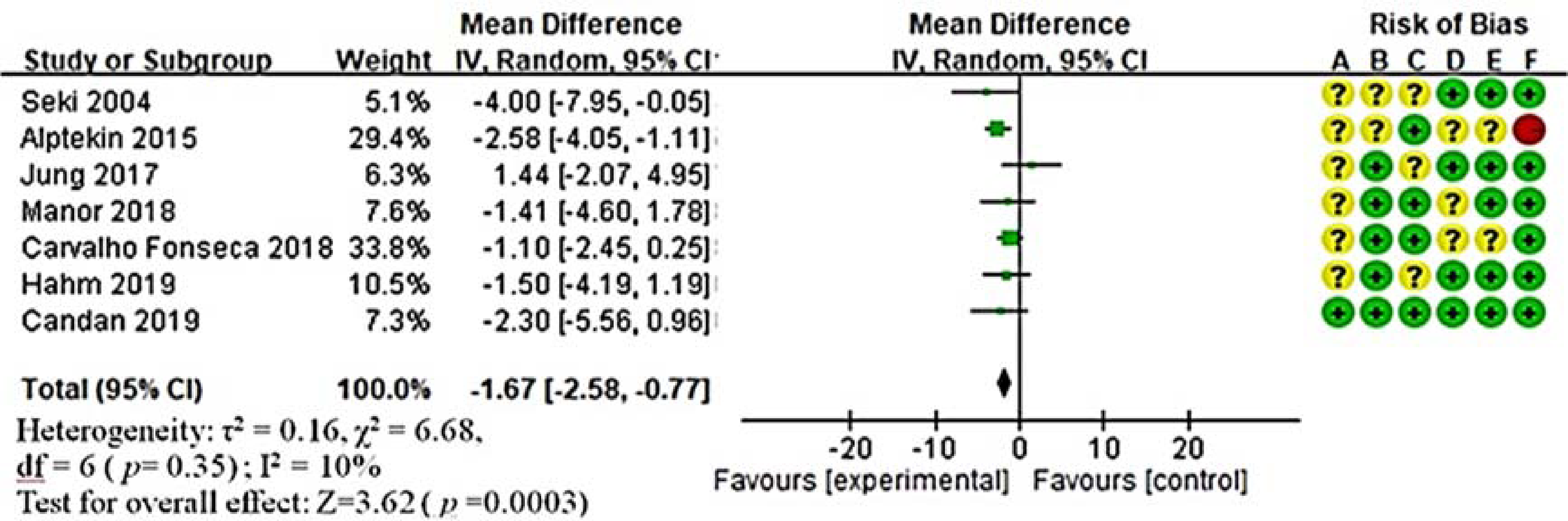
The effect of acupuncture-related treatments on muscle strength
The effect of acupuncture-related treatments of meta-regression analysis on muscle strength.
Discussion
This systematic review and meta-analysis study was based on 66 studies, confirmed noninvasive and invasive acupuncture-related treatments providing evidence supporting the benefits of these treatments on the cognitive and physical functions of older people with Alzheimer's disease. Regarding cognitive function, this finding is in line with previous studies that have suggested that acupuncture-related treatments effectively improved cognitive function.5,78–80 The present study found that noninvasive acupuncture-related treatments provided moderate-scale improvement compared with invasive ones. The noninvasive acupuncture-related treatments included acupressure, acupressure, moxibustion and transcutaneous electrical acupoint stimulation in the present study; they were effective. These may balance blood circulation and energy through specific acupuncture acupoint on the meridians; that is similar to acupuncture where the needle is applied to acupoints. 6
Rather than noninvasive techniques, most systematic reviews and meta-analyses on acupuncture-related treatments in dementia have mainly included invasive techniques such as acupuncture,5,78and electro-acupuncture.79,80 The present study provides a more comprehensive analysis of the effects of acupuncture-related treatments on Alzheimer's disease by building on previous reviews. This cognitive function was improved effectively through acupuncture-related treatments starting from the 6-week duration. Noted that participants in the present study aged 79 years and 72 years, and had been diagnosed Alzheimer's disease for 5.5 years and 3.6 years in the noninvasive and invasive acupuncture-related treatments, respectively. The former was older and severer than the latter. Among aging-related diseases, Alzheimer's disease is a common neurodegenerative disease of the central nervous system and mostly affects those more than 65 years old. 81 Age is the main risk factor for cognitive impairment. 82
The present study confirms that noninvasive and invasive acupuncture-related treatments improve self-care ability of physical function. This finding is in line with some systematic reviews that suggested that acupuncture-related treatments plus medication effectively improve self-care ability compared with medication alone. 5 The present finding is inconsistent with other systematic reviews that compared the effects of acupuncture-related treatments with medication on self-care ability.80,81 Limited ability to self-care, however, would increase the disease burden on patients and their families. 83 Furthermore, the present study identified that noninvasive acupuncture-related treatments are more effective than invasive ones in terms of self-care ability. Noninvasive acupuncture-related treatments have a favorable effect on cognitive function and then reduce the care burden of patients and caregivers. Despite these benefits, the present study concluded the intervention duration has to maintain at least 12 weeks to bring about self-care effect.
In addition, the present study has evidence that was support to ameliorate muscle strength. To the best of our knowledge, this is the first study confirming that acupuncture-related treatments could improve muscle strength for older people with Alzheimer's disease. The result of the present study is consistent with one systematic review on the effect of acupuncture on muscle strength in older patients with stroke. 84 Although acupuncture-related treatments are commonly used for musculoskeletal disorders, 7 their mechanism to improve muscle strength has not been well understood. 85 However, muscle strength is highly associated with self-care ability. 83 Further study to reconfirm this evidence of Alzheimer's disease is suggested.
Irrespective of acupuncture-related treatments in the present study improved cognitive and physical functions in patients with Alzheimer’s disease. This disease characterizes by a gradual loss in cognitive function and leads to a decreased ability to perform activities of daily living. Furthermore, Alzheimer's disease affects both patients’ and their caregivers’ quality of life. Until now, two studies have been conducted regarding the quality of life outcome for Alzheimer's disease in the present study.34,51 And insufficient evidence to support the effect of acupuncture-related treatments on improving quality of life was found. Further research to provide evidence is needed.
Although the mechanism by which acupuncture-related treatments improve cognitive function and physical function remains unestablished, some hypotheses can be considered. First, acupuncture-related treatments may improve cognitive function through neuron-protective effects. 84 They could promote choline acetyltransferase secretion in the hippocampus, reduce the production of glial fibrillary acidic protein, participate in acetylcholine synthesis, and regulate abnormal astrocyte hyperactivity.78,86 In people with Alzheimer's disease, acupuncture-related treatments have significantly improved learning and memorization abilities, by potentially inhibiting excessive β-amyloid production in the brain.78,86 On the basis of these results, these treatments might protect neurons from deterioration and promote axonal regrowth in neurodegenerative diseases. 85 Moreover, a growing body of evidence supports that acupuncture point stimulation exerts apparently regulatory effects on glucose metabolism intake rate because glucose metabolism is enhanced to compensate neuronal dysfunction to prevent and treat neurodegenerative diseases. 84 Therefore, acupuncture-related treatments potentially excite nerve fibers, and improve local blood circulation. They stabilize and accelerates cerebral metabolic responses in brain systems. In addition, acupuncture-related treatments could increase cerebral blood flow and restore long-term potentiation impairments to ameliorate such symptoms.78,86 Finally, acupuncture-related treatments may become a form of perceptual stimulation. Acupuncture-related treatments have shown to improve cognitive and physical functions widely applied by clinicians to treat dementia as a disease-modifying therapy.
The noninvasive acupuncture-related treatments had none of adverse events; however, few complications were reported due to the invasive acupuncture-related treatments in the present study. There 19 participants reported adverse events associated with the invasive acupuncture-related treatments were pain, dizziness, light ecchymosis, and light bleeding.25,29,32,35,45,46,61,68 These events Participants who developed local hematoma were treated with cold compress and they recovered within 3 days. Those who developed headache recovered after taking a rest Neither of these events caused the participants to withdraw from the trials. The present study showed that compared with the controls, acupuncture-related treatments had few complications and higher safety and accessibility, improving relevant domains of patients with Alzheimer's disease namely cognitive function, self-care ability and mobility. Thus, the results of the present study have important implications for clinical practice, which indicated that acupuncture-related treatments could be a recommendation for Alzheimer's patients except for choosing medication. Noninvasive acupuncture-related treatments such as acupressure and transcutaneous electrical acupoint stimulation are not restricted by time or space to provide Alzheimer's patients and their caregivers with choices according to the patients’ preferences. The overall research results can let clinical professionals understand the effect of different acupuncture-related treatments and then provide more objective information and suggestions to Alzheimer's patients.
The present study has some limitations. Firstly, a moderate risk of bias in performance and detection present due to blinding. Blinding bias in the methodology of the included studies was considered because was either not performed or not described in most studies. However, because of the nature of the acupuncture-related treatments, acupoints stimulated with needles or pressure will always be felt by patients and known to practitioners. Notably, if outcome assessors could be blinded, measurement bias would be minimized. Secondly, the meta-analyses showed moderate heterogeneity. This could be considered clinical heterogeneity, which may be attributed to patient characteristics, such as dementia stage and ages. Thirdly, the included studies used different acupuncture-related treatments and acupoints, which may lead to clinical heterogeneity risk in the results. Similarly, previous studies have observed moderate heterogeneity due to the interventions.5,87 The definitions of intervention categories and regrouping were formulated through expert consensus; however, heterogeneity was difficult to avoid because of the nature and complexity of acupuncture-related techniques. Fourthly, because few included studies reported whether adverse events occurred due to the treatment, the relative safety of acupuncture-related treatments requires more research. Lastly, there was a methodological limitation in this systematic review and meta-analysis study, which led to only Chinese and English papers found and included. A language restriction is not avoided.
In conclusion, effective evidence-based non-pharmacologic interventions are available for enhancing the cognitive and physical functions of people with Alzheimer's disease and their caregivers. These acupuncture-related treatments need to be applied at least six weeks for obvious curative effects. Contemporarily, pharmacological therapy in clinical treatments is most commonly used to slow the exacerbation of the Alzheimer’s disease. However, the development of pharmacologic treatment to slow the progression of cognitive deficits is an ongoing process that will likely take years. The drug side-effects are still concerned. Other available option to treat Alzheimer's disease should be open to patients and their caregivers. Acupuncture-related treatments are not only effective for improving cognitive dysfunction but also safe with few complications in the present study, moreover, they have high acceptance among Asians. These findings indicate diverse choices for patient and caregivers, and provide a reference for clinical care guidelines for Alzheimer's disease. The noninvasive acupuncture-related treatments highlight to effect for cognition function and physical function more superior than invasive ones. As noninvasive ones such as auricular acupressure, body acupressure, transcutaneous electrical acupoint stimulation, and moxibustion are applied for patients, the benefits are lessened negative effects, risen accessibility, and increased cooperation. Furthermore, whether significant effects are clinically meaningful and improve daily life must be evaluated. Future research on acupuncture-related treatments involving people with Alzheimer's disease living in long-term care facilities or at home is warranted.
Clinical massage
Acupuncture-related treatments were confirmed to improve cognitive and physical functions for patients with Alzheimer's disease.
The treatment duration is suggested to maintain at least 6 and 12 weeks to generate cognitive function and self-care effects, respectively.
Noninvasive acupuncture-related treatments highlighted to effect for cognition and physical functions superior than invasive ones.
Footnotes
Statement of ethics
The present study is not required because of did not involve individual participants as this was a systematic review and meta-analysis of existing publications, and no primary data were collected. Since no patients are involved, there is no individual privacy concerning problems.
Author contributions
C.L., M.Y., S.W., and Y.C. carried out study design. C.L, M.Y., and Y.C. performed literature search and meta-analyses. C.L, M.Y., and J.C. drafted the manuscript. C.L., M.Y. and J.C. critically revised the manuscript. All authors read and approved the final version of the manuscript.
Conflict of interest
None of the authors have conflicts of interest to declare.
Funding Information
No sources of funding are used to assist in the preparation of this article.
International prospective register of systematic reviews
ID: CRD42020196741
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.