
Abstract
Objective
To determine if home-based exercise programmes for older adults after hospitalisation are effective at improving physical activity, quality of life, activities of daily living (ADL) and mobility compared to no intervention, standard care or centre-based exercise.
Methods
Databases were searched from inception to March 2022. Randomised controlled trials which included home-based exercise in older adults recently discharged from hospital were included. The primary outcome was physical activity. Secondary outcomes were quality of life, ADL performance, mobility, adverse events and hospital readmissions. Two reviewers independently selected relevant studies and extracted data. Quantitative synthesis with meta-analyses using a random-effects model and qualitative synthesis were performed.
Results
Ten trials (PEDro score 6-8) were included. Three trials reported on physical activity but meta-analysis was not possible due to heterogeneity. Home-based exercise was more effective than no intervention at improving ADL performance (SMD 0.60, 95% CI 0.03 to 1.17); and standard care at improving quality of life (SMD 0.30, 95% CI 0.11 to 0.49) and mobility (SMD 0.23, 95% CI 0.00 to 0.45). Few and minor adverse events were associated with home-based exercise.
Conclusion
Based on individual trials, home-based exercise has the potential to improve physical activity compared to no intervention or standard care. Meta-analyses indicate that home-based exercise is more effective than no intervention at improving activities of daily living performance, and standard care at improving mobility and quality of life. It is unclear if home-based exercise is more effective than centre-based exercise at improving these outcomes.
Introduction
Older adults engage in low levels of physical activity, particularly during and after periods of hospitalisation.1–4 Moreover, the combined effects of illness and inactivity during and after hospitalisation put older adults at a heightened risk of physical and functional decline.5–7 Many older adults who have been discharged from hospital fail to return to their previous level of function and are susceptible to hospital readmission.6–10 Facilitating regular physical activity through exercise during and after hospitalisation, particularly on return home, may be crucial to maintain and improve the long-term health outcomes of older adults.11,12 Exercise interventions targeting older people after hospitalisation may increase physical activity, improve function and quality of life, and can reduce falls.13–15 One method by which older adults could engage in exercise and therefore increase physical activity after hospitalisation is through home-based programmes. Multiple reviews have been conducted to investigate the effectiveness of home-based exercise in various population groups, but not in the period immediately after hospitalisation when individuals return home.16–25 It is not known if home-based exercise programmes provided in older people following discharge from hospital are effective at increasing physical activity and improving health outcomes, or if they are a safe modality.
Therefore, this review seeks to describe home-based exercise programmes that have been utilised for older adults after hospitalisation and investigate their effectiveness for increasing physical activity and improving health outcomes. It will also review the safety of such programmes, an important aspect to consider when delivering any exercise intervention. To our knowledge, this will be the first review to assess the effectiveness of home-based exercise provided in older adults immediately after a period of hospitalisation for the purposes of promoting physical activity and improving function. This review will provide important information which can help to inform practice and allow clinicians to understand the effect of intervening at a critical time point in an older adult's health journey.
The primary review question to be addressed is:
Are home-based exercise programs for older adults after hospitalisation effective at increasing physical activity compared to no intervention, standard care or centre-based exercise? Are home-based exercise programs for older adults after hospitalisation effective at improving quality of life, performance of activities of daily living (ADL) or mobility compared to no intervention, standard care or centre-based exercise? Are home-based exercise programs for older adults after hospitalisation safe in terms of adverse events and hospital readmissions?
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement guided the reporting of this review. 26 The study was registered at the International Prospective Register of Systematic Reviews (PROSPERO) (CRD42020213938).
Eligibility criteria
Randomised controlled trials with full text articles available in English were eligible to be included in this review if participants were community-dwelling older adults (aged 60 years or over) who were recently discharged from a hospital setting. The interventions must have tested home-based exercise (strength, balance or mobility training, aerobic exercise, or education) prescribed by a physiotherapist or healthcare professional with skills in exercise prescription (exercise physiologist or exercise scientist). The intervention timeframe was crucial and the interventions must have commenced shortly before (within one week) or after (within four weeks) of hospital discharge. The comparator conditions of interest were no intervention, standard care or centre-based exercise. Intervention and comparison conditions were categorised to form these distinct comparisons (Appendix 2). Trials were included if they included one or more of the outcome measures of interest – the primary outcome of physical activity measured objectively or by self-report and/or any of the secondary outcomes of quality of life, performance of ADL, mobility, adverse events and hospital readmissions.
Literature search
Electronic searches were conducted from inception to February 2021 in the following databases: MEDLINE, EMBASE, Cochrane Central Register of Controlled Trials, PEDro, CINAHL, Scopus. Papers published in English were included. No restrictions for the publication period were placed on the search. The search terms related to ‘exercise’ or ‘physical activity’ and ‘older adults’ and ‘hospital discharge’ and ‘randomised controlled trial’ were combined. The search strategy was developed for MEDLINE and adapted for the other databases (Appendix 1). Database search alerts were set to identify new articles that were suitable for inclusion up until the final analyses (October 2021). Ongoing reviews of database search alerts were conducted from the final analyses to manuscript submission (March 2022).
Study selection
Two reviewers independently screened articles by title and abstract to identify potentially relevant trials. Disparities were discussed and resolved between the two reviewers and, when necessary, two additional reviewers were consulted. Articles not meeting the eligibility criteria were excluded.
The full text articles of potentially relevant trials were then retrieved and reviewed independently by the same reviewers. An Excel spreadsheet detailing the eligibility criteria was used by both reviewers in this process. Disparities were discussed and resolved between the two reviewers and, when necessary, two additional reviewers were consulted. Trial authors were contacted if additional information was required in order to determine eligibility.
Quality assessment
The PEDro score was used to assess methodological quality of included trials. 27 Searches were conducted in the PEDro database to identify the PEDro score for each trial and two reviewers confirmed the PEDro score where available. Where a trial was not listed on the PEDro database, both reviewers independently rated the trial using the PEDro score. Based on the total PEDro score which ranges from 0 to 10, methodological quality was considered to be poor (0–3), fair (4–5), good (6–8) or excellent (9–10). 28
Data analysis
Data were extracted by two reviewers independently. Publication details, participant characteristics, details of intervention and control groups, and outcome data for the participants analysed in each trial (means, standard deviations, 95% confidence intervals or medians, interquartile ranges at each timepoint) were extracted. Disparities were discussed and resolved between the reviewers and, when necessary, two additional reviewers were consulted. If studies included more than one measure to reflect the outcome, predetermined data rules were applied (Appendix 2). In the case of missing or incomplete data, study authors were contacted in order to obtain further information. Where study authors provided raw data, analyses on IBM SPSS Statistics for Windows, Version 27 (IBM Corp, Armonk, NY) was completed to obtain the necessary data.
For pooled analyses when two or more studies were available in a comparison, mean post-intervention scores and standard deviations were extracted where possible. Change scores were used only if all studies in the comparison reported it as such. Results presented as median and interquartile range were converted to mean and standard deviation. 29 In a few instances (adverse events and rehospitalisation outcomes), data were converted to frequencies from information in the text or provided by study authors. For the majority of the outcome measures, a higher score indicated a better outcome. Where lower scores indicated a better outcome, negative signs were applied to mean scores so that results were in the same direction. The review statistician (PG) checked extracted data for accuracy prior to analyses.
R statistical software with the meta package was used for all analyses. 30 For continuous outcomes, data were pooled and reported as mean difference with a 95% confidence interval (CI) if all outcomes were the same and Hedges’ g bias corrected standardised mean difference (SMD) with a 95% CI if outcomes were different. A random-effects model using an inverse variance method was employed in which restricted maximum likelihood method was used to estimate the between study variability. Dichotomous outcomes were pooled to produce an odds ratio; a random-effects model using the Mantel-Haenszel method was employed. Heterogeneity between trials was assessed using the I2 statistic. I2 values of 25, 50 and 75% indicate low, moderate and high heterogeneity respectively. 31 Results were not pooled if I2 was greater than 75%. The magnitude of the SMD may be interpreted using the guideline provided by Cohen whereby an SMD of 0.2 is considered a small effect, 0.5 a moderate effect and 0.8 a large effect. 32
Where there were insufficient studies to pool results for a particular comparison or data were not from continuous distributions or excessive heterogeneity was indicated by the I2 statistic (I2 > 75%), data are reported in narrative form.
Results
Flow of studies through the review
The electronic search strategy identified 4674 papers, 2576 papers after duplicates were removed. The titles and abstracts of these papers were screened, and 51 full text articles were retrieved. From these full text papers, thirteen papers (10 trials) met the inclusion criteria and were included in this review. Eleven papers (10 trials) were included in the meta-analyses. The flow of studies through the review is presented in Figure 1. Duplicate reports for the same trial were managed using guidance from the Cochrane Handbook of systematic reviews. 33 One trial was identified that met all but one of the inclusion criteria relating to the timeframe between discharge and start of intervention – this trial was included in sensitivity analyses. Two potentially relevant papers were identified from the database search alerts but were ultimately ineligible for this review upon review of the full text.34,35 These two papers reported on the same trial and were ineligible because the active control groups also received home visits and weekly phone calls.34,35
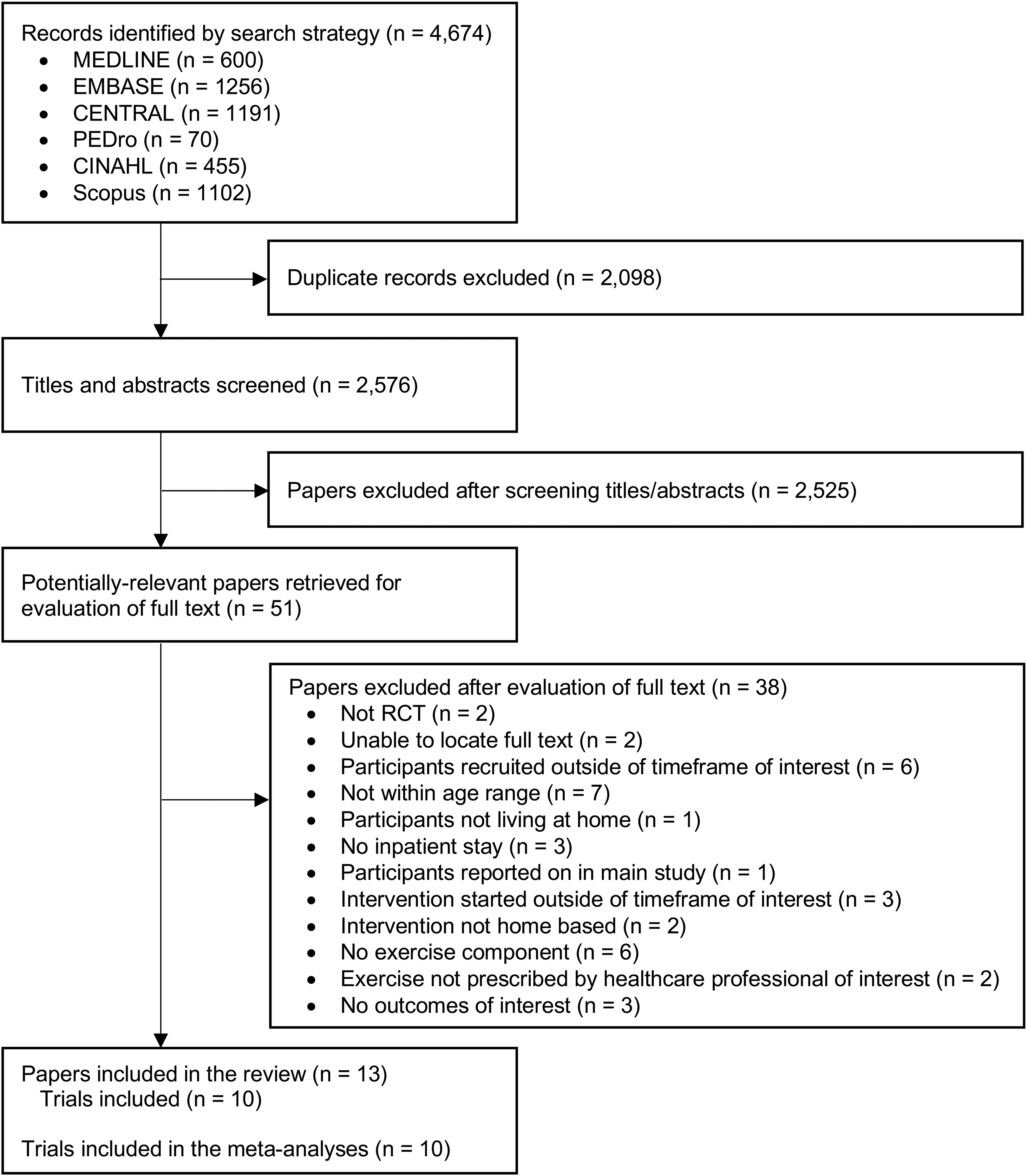
Flow of studies through the review.
Study and participant characteristics
All of the included papers describe randomised controlled trials. Four trials compared home-based exercise with no intervention.36–39 Four trials compared home-based exercise with standard care.40–43 Two trials compared home-based exercise with centre-based exercise.15,44 Characteristics of all included trials are summarised under the three comparison conditions in Table 1 (further details on individual trials are provided in Appendix 3).
Summary of the characteristics of included studies.
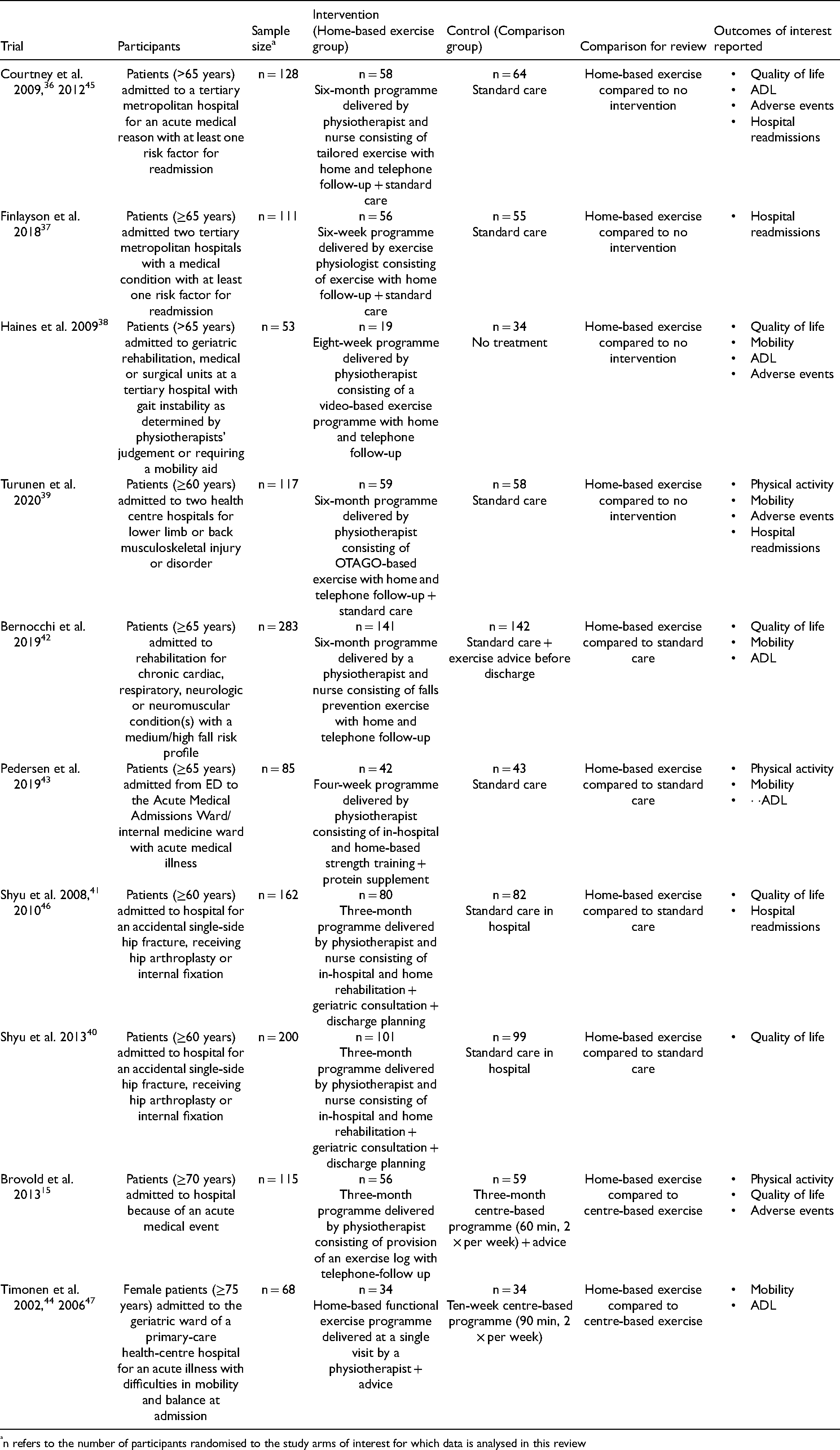
n refers to the number of participants randomised to the study arms of interest for which data is analysed in this review
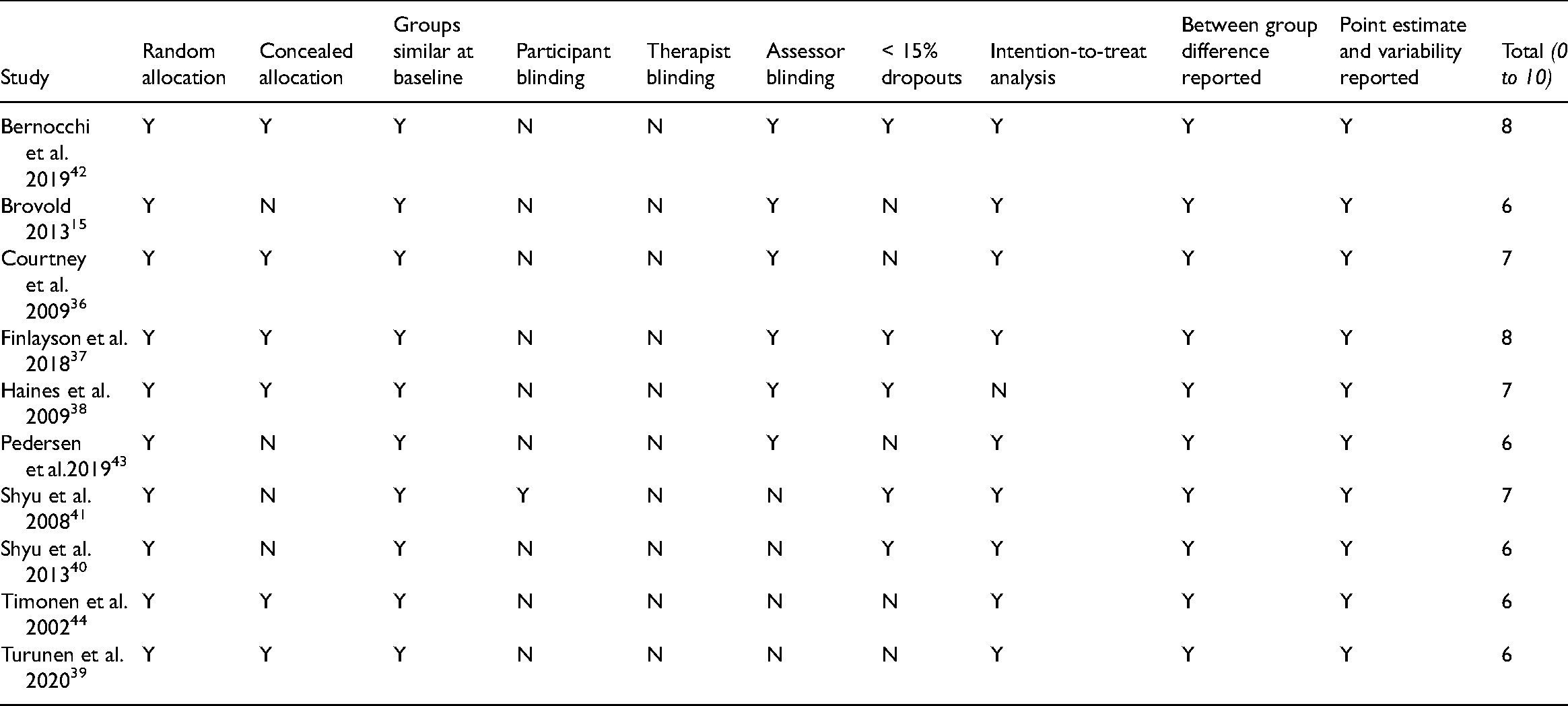
Methodological quality of the included trials ranged from 6 to 8 on the PEDro scale, indicating good methodological quality, with the mean (SD) PEDro score being 7 (1) out of 10 (Table 2). 28 Random allocation was used in all of the included trials. Groups were similar at baseline in all but one trial. 40 Participant and therapist blinding were not possible in any of the included trials. Assessor blinding was not used in four trials (five papers).39,40,44,46,47 Half of the trials (six papers) had greater than 15% dropouts.37,38,40–42,46 Intention-to-treat analysis was used in all but one trial. 39
PEDro scores of included trials.
Considering the participants randomised to the study arms of interest, the trials in this review had between 53 and 283 participants (median 116) with reported mean age ranging from 77 to 83 years.15,36–44 Participants were recruited from hospital settings.15,36–44 All trials identified participants prior to hospital discharge.15,36,37,39–44 One trial also recruited participants within one week of discharge. 38
The home-based exercise component of all included trials involved tailored exercise in the form of falls prevention exercises, strengthening exercises, balance exercises, functional exercises, mobility and education/advice. The active intervention period ranged from 4 weeks to 6 months.15,36–43 The comparator condition was standard care for all but three trials.15,38,44 For two trials, the comparator condition was centre-based exercise which involved structured exercise sessions of a certain dose15,44 For one trial, the comparator condition was no treatment. 38
Three trials measured physical activity with three different measures used.15,39,43 Six trials measured quality of life with validated instruments.15,36,38,40,42,46 Six trials assessed mobility with various measures used.15,38,39,42–44 Four trials assessed performance of ADL and used various indexes.36,38,42,43 Four trials reported the number of adverse events related to the intervention.36,37,39,41 Four trials reported data on the number of people requiring unplanned readmission to hospital.36,37,39,41
Comparison 1: effect of home-based exercise compared to no intervention
One trial compared the effect of home-based exercise to no intervention on physical activity. 39 The mean difference between groups was 3.4 (95% CI −20.3 to 27.1) minutes per day of total physical activity in favour of the home-based exercise group.
Two trials compared the effect of home-based exercise to no intervention on quality of life but data were not pooled in a meta-analysis due to substantial between-trial heterogeneity (I2 = 96%).36,38 In one trial which measured quality of life using the SF-12 Physical Component Summary score, the mean difference between groups was 17.8 (95% CI 14.1 to 21.5) which favoured home-based exercise. 36 In the other trial which measured quality of life using the EuroQol-5 Dimension Visual Analogue Scale (EQ-5D VAS), the mean difference between groups was 1.1 (95% CI −8.9 to 11.1) which favoured no intervention. 38
Two trials compared the effect of home-based exercise to no intervention on mobility (Figure 2(a)).38,39 The SMD was 0.2 (95% CI −0.2 to 0.5, I2 = 0%) indicating a small effect which favoured home-based exercise.
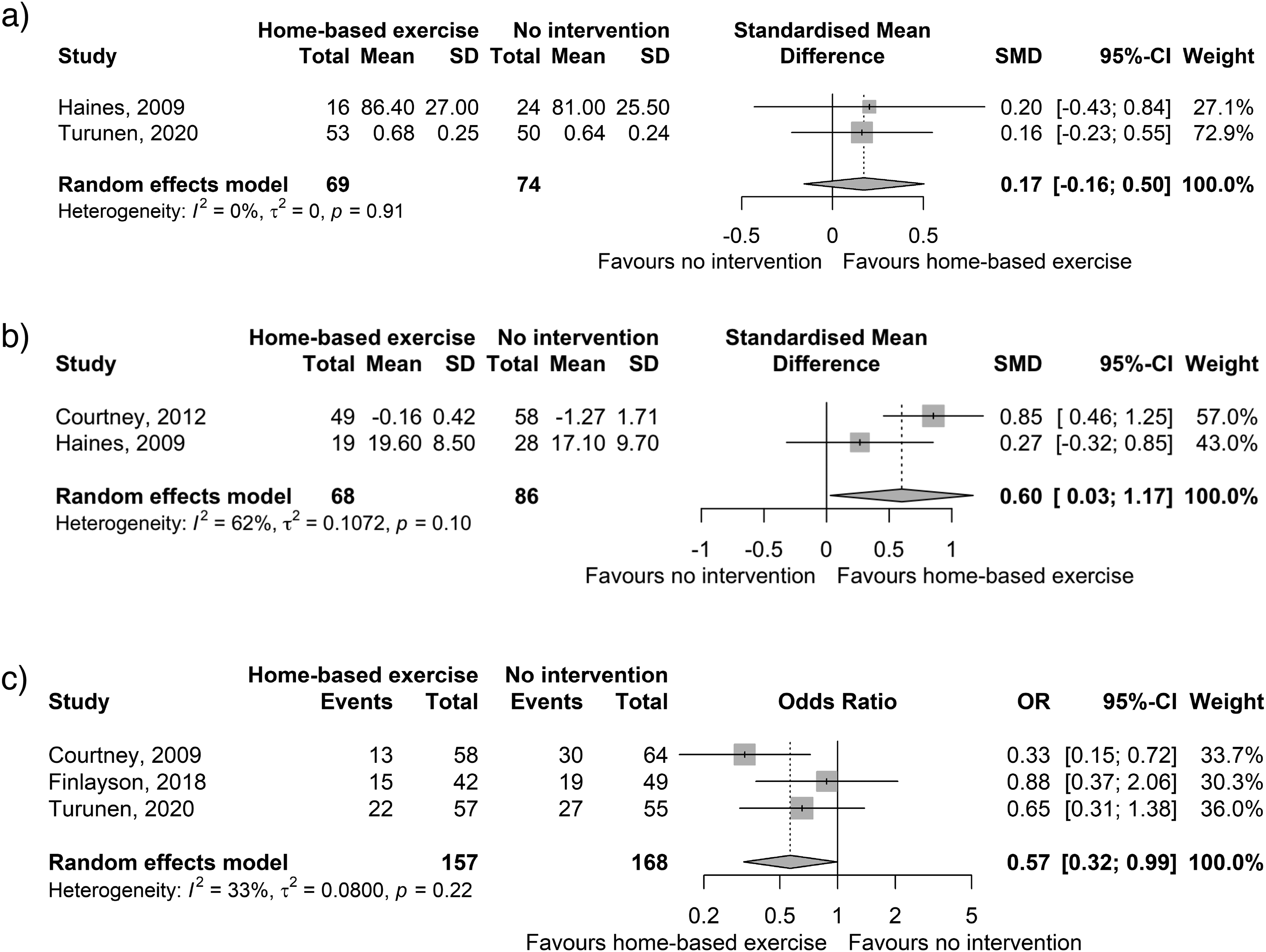
Standardised mean difference (95% CI) of the effect of home-based exercise versus no intervention on a) mobility; b) performance of activities of daily living; and c) Odds ratio (95% CI) for home-based exercise versus no intervention on rehospitalisation.
Two trials compared the effect of home-based exercise to no intervention on performance of ADL (Figure 2(b)).38,45 The SMD was 0.6 (95% CI 0.0 to 1.2, I2 = 62%) indicating a moderately sized effect in favour of home-based exercise.
Three trials reported on the number of adverse events. Two trials reported no adverse events related to the home-based exercise intervention.36,39 One trial reported five adverse events related to the home-based intervention. 38 These were minor and involved muscle soreness in the first week of the programme only.
Three trials compared the effect of home-based exercise to no intervention on rates of rehospitalisation (Figure 2(c)).36,37,39 The odds of rehospitalisation was 43% lower for the home-based exercise group compared to no intervention (OR 0.6, 95% CI 0.3 to 1.0, I2 = 33%).
Sensitivity analyses
One additional trial (PEDro score = 8, 340 participants) met all but one aspect of the inclusion criteria relating to the time between hospital discharge and the baseline assessment. 48 It was deemed by three reviewers (IL, KS, JG) as being significant to this review. Therefore this trial was included in a sensitivity analyses for three outcomes. The sensitivity analyses did not reveal important changes in mean differences to the primary outcome of physical activity or the secondary outcomes of quality of life or mobility when this study was added to the analysis.
Comparison 2: effect of home-based exercise compared to standard care
One trial compared home-based exercise with standard care and measured physical activity as steps per day. 43 Mean difference between groups was 999 (95% CI −24 to 2022) steps favouring the home-based exercise group.
Three trials compared the effect of home-based exercise to standard care on quality of life (Figure 3(a)).15,42,46 The SMD was 0.3 (95% CI 0.1 to 0.5, I2 = 22%) which showed a small effect in favour of home-based exercise.
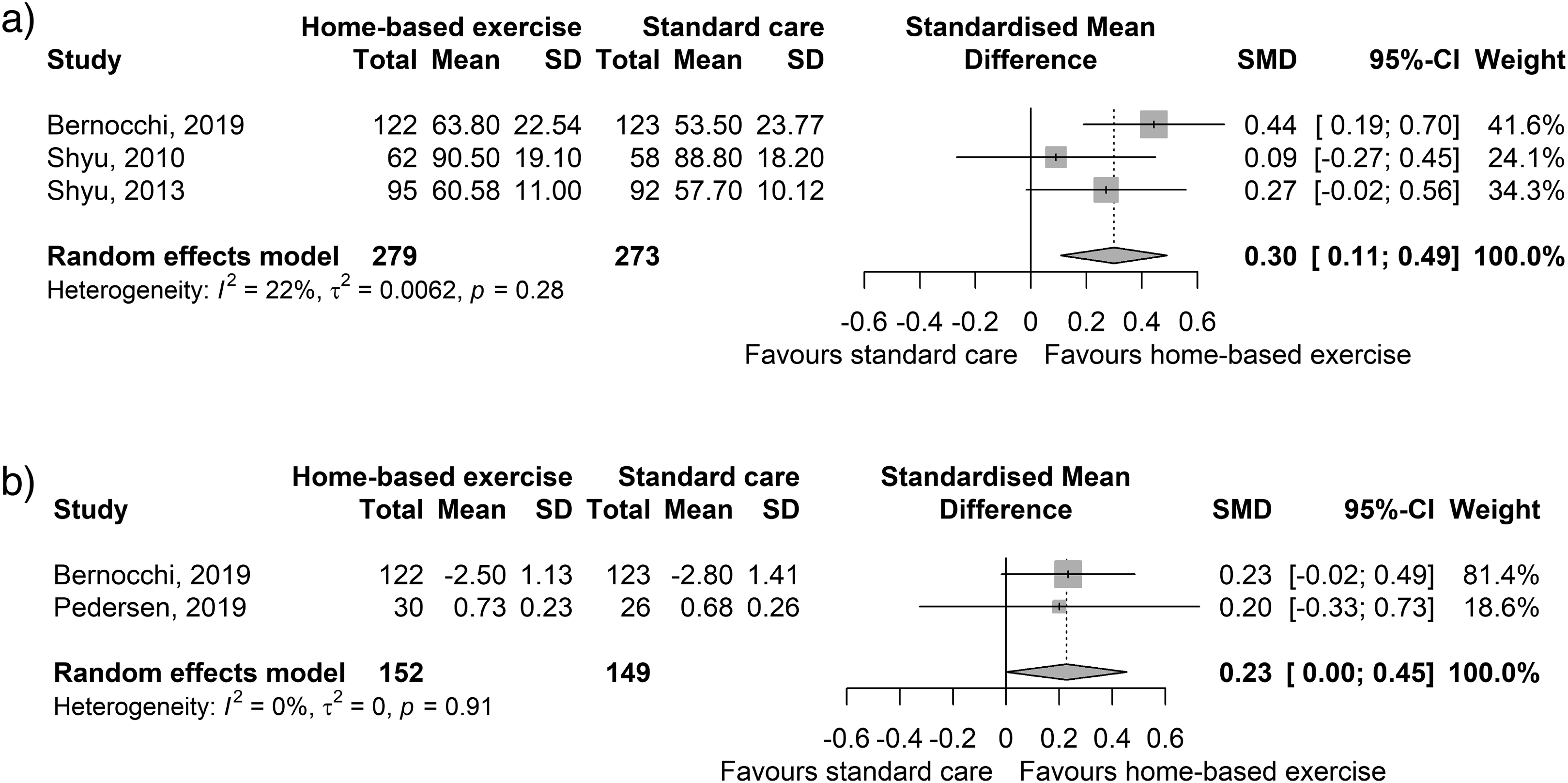
Standardised mean difference (95% CI) of the effect of home-based exercise versus standard care on a) quality of life; and b) mobility.
Two trials compared the effect of home-based exercise to standard care on mobility (Figure 3(b)).42,43 The SMD was 0.2 (95% CI 0.0 to 0.5, I2 = 0%) indicating a small effect in favour of home-based exercise.
Two trials compared the effect of home-based exercise to standard care on performance of ADL.42,43 Data for one trial which used the Barthel Index 20 was reported as ordinal categories rather than change scores, thus the data were not able to be pooled in a meta-analysis. 43 The between-group mean difference in change score was −0.1 (95% CI −0.8 to 0.7) which did not provide clear evidence in favour of either intervention. The other trial used the Barthel Index. 42 The mean difference between groups was 8.4 (95% CI 3.5 to 13.4) which favoured the home-based exercise group.
No trials compared the effect of home-based exercise with standard care on number of adverse events.
One trial compared the effect of home-based exercise to standard care on rates of rehospitalisation. 41 A slightly greater percentage of participants from the home-based exercise group experienced rehospitalisation compared to the standard care group (11 of 71 participants (15%) compared to 7 of 76 participants (9%) respectively, chi-squared test p-value 0.36).
Comparison 3: effect of home-based exercise compared to centre-based exercise
One trial compared the effect of home-based exercise with centre-based exercise on physical activity. 15 Physical activity as measured on the PASE increased in both the home-based exercise and centre-based exercise groups after the intervention period. The mean difference between groups was 6.2 (95% CI −10.2 to 27) in favour of centre-based exercise.
One trial compared the effect of home-based exercise with centre-based exercise on quality of life. 15 Mean difference between groups in SF-36 physical functioning subscale scores was 0.5 (95% CI −4.1 to 5.1), showing negligible difference between groups.
Two trials compared the effect of home-based exercise with centre-based exercise on mobility (Figure 4).15,44 The SMD was −0.4 (95% CI −0.8 to 0.1, I2 = 38%) which indicated a small to moderate effect in favour of centre-based exercise.
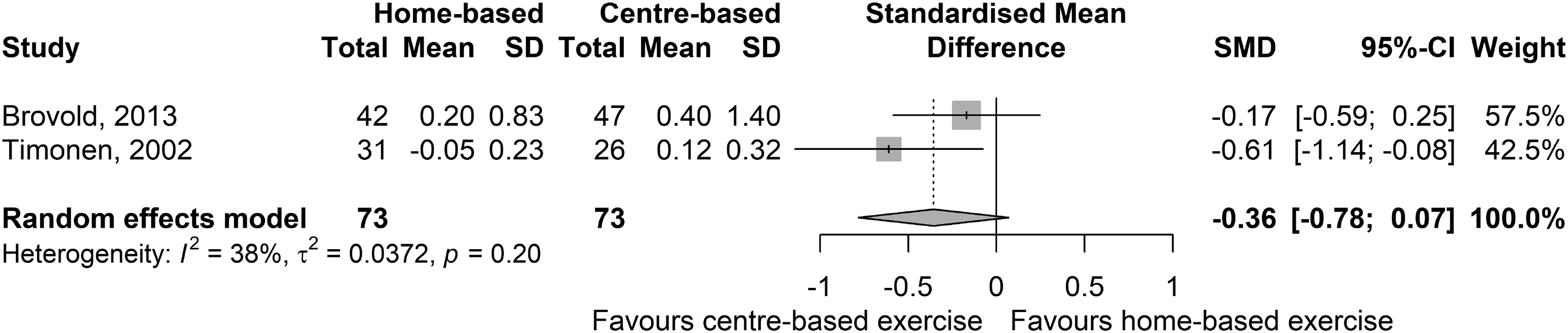
Standardised mean difference (95% CI) of the effect of home-based exercise versus centre-based exercise on mobility.
One trial compared the effect of home-based exercise with centre-based exercise on performance of ADL. 47 This was measured as the number of participants requiring assistance for eating, bathing, dressing or toileting. The results were similar between groups (38% of the participants in the centre-based exercise group required assistance compared to 42% in the home-based exercise group).
One trial reported on the number of adverse events. 15 The number of participants experiencing adverse events was slightly greater in the home-based exercise (n = 16, 38%) group than the centre-based exercise group (n = 14, 30%).
No trials compared the effect of home-based exercise to centre-based exercise on rates of rehospitalisation.
Discussion
This systematic review found that home based exercise may improve physical activity when compared to no intervention or standard care. Home-based exercise is superior to no intervention at improving ADL performance and standard care at improving quality of life and mobility. However, home-based exercise may not be superior to other interventions, such as centre-based exercise, at improving these outcomes. Furthermore, the findings indicate that home-based exercise is a safe modality which may reduce the risk of rehospitalisation in older adults when compared to no intervention. To our knowledge, this is the first systematic review to assess the effect of home-based exercise on physical activity in older adults at this specific timepoint.
Only three trials reported on physical activity as an outcome with variability in measures used.15,39,43 Heterogeneity in physical activity outcome measures among research trials is not uncommon but limits meaningful comparisons. 49 Physical activity is an important outcome measure as physical activity levels are associated with health and function, particularly in older age. Future studies should use objective methods of measurement, such as accelerometry, to provide more credible and accurate results.
A previous systematic review which evaluated the effectiveness of physical activity interventions among older adults found that home-based interventions can increase physical activity at least in the short term. 50 This is in agreement with the results of the current review where outcomes were not assessed past six months. Strategies which promote long-term maintenance of physical activity should be considered. For example, interventions could target behaviour change and habit formation. Such interventions may integrate exercise into older adults’ daily routines and tend to be less structured, reducing barriers to exercise participation. 51 Additionally, approaches which work on building self-efficacy may improve exercise adherence in older adults and require further investigation.51,52 Future research investigating the utility of home-based exercise for older adults after hospitalisation should adopt these strategies and assess physical activity as an outcome, particularly in the longer-term.
For the secondary outcomes of quality of life, mobility and performance of ADL, the results indicate that home-based exercise may be better than no intervention or standard care but may be similar or inferior to centre-based exercise. This may reflect that having a certain amount of supervision from physiotherapists or other health professionals when exercising may be beneficial in older adults. However, other research evidence suggests that the benefits of home- versus centre-based exercise in older adults may depend on the specific health condition and home-based exercise may result in better long-term adherence. 16 Regardless of this, either exercising at home or at a centre is likely to improve older adults’ health and function. 16 Clinicians could consider home-based execise as a viable alternative to centre-based exercise as it may be less resource intensive or more practical for some clients, for example, if transport options are limited. In addition, only few and minor adverse events were associated with home-based exercise and this modality can reduce hospital readmissions when compared to no intervention. Thus, home-based exercise could be considered a safe modality for older adults after hospitalisation.
It should be noted that there was an inability to pool data from a large number of trials due to the limited number of trials identified based on the inclusion criteria. The absence of much data resulted in large confidence intervals. However, a lack of clinical benefit should not be assumed as the point estimates largely favour home-based exercise. Therefore, further trials in this area of research is warranted. Additionally, a limitation of this review is that the search strategy only included trials published in English, thus reducing the generalisability of results and potentially leading to missing data. In terms of the available literature, there was high variability in outcome measures. This highlights the need for trials to use high quality, standardised outcome measures, and outcome measures which match the content of interventions, from which meaningful data can be produced. 53 Similarly, there is heterogeneity in the patient populations and interventions of included trials. However, this reflects the nature of pragmatic clinical trials investigating exercise interventions and therefore this review provides clinically relevant information.
The strengths of this review are that it explores a novel area and its methods are consistent with a prospectively-registered protocol. Individual trials demonstrated good methodological quality which adds weight to the findings of this review. Furthermore, small to moderate effect sizes were observed for home-based exercise compared to no intervention and standard care on quality of life, mobility and performance of ADL, despite the small number of trials.
In conclusion, home-based exercise has the potential to improve physical activity levels in older adults after hospitalisation. Further, home-based exercise is effective at improving performance of ADL when compared to no intervention, and quality of life and mobility when compared to standard care. It appears to be a safe modality which could be further studied in high quality trials, especially as it may reduce the risk of rehospitalisation compared to no intervention. Therefore, there is scope for physiotherapists and other health professionals to intervene and facilitate physical activity through exercise at this crucial point in an older person's health journey. However, due to limited evidence, the use of home-based exercise for older adults after hospitalisation, specifically as a means to increase physical activity, should be further studied in high quality trials. Future trials of home-based exercise should be designed to specifically intervene at the physical activity level, assess physical activity and use appropriate outcome measures.
Clinical messages
Physical activity is important for healthy ageing and maintenance of function in older adults.
Home-based exercise may increase older adults’ physical activity after hospitalisation and can improve some health-related outcomes.
Future exercise trials in older adults should assess physical activity and use standardised measures to allow for meaningful comparisons.
Footnotes
Acknowledgements
Amitoj Thind assisted with screening articles, reviewing full text articles and data extraction.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Australian Government Research Training Program Scholarship.
Author contributions
Ingrid Lin: Conceptualisation, Methodology, Data curation, Writing – Original Draft; Joanne Glinsky: Methodology, Writing – Review & Editing, Supervision; Catherine Dean: Writing – Review & Editing, Supervision; Petra Graham: Formal analysis; Katharine Scrivener: Conceptualisation, Methodology, Writing – Review & Editing, Supervision.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.