
Abstract
Objective
Loss of proprioception and balance disorders are commonly observed in patients with knee osteoarthritis. In this study, we aimed to investigate the effects of balance and proprioception exercises in patients with knee osteoarthritis.
Design
A single-center randomized trial with three parallel arms.
Setting
A tertiary health care facility in Turkey.
Participants
Female patients with knee osteoarthritis aged 40–70 years.
Interventions
Ten-week exercise program in Biodex training, classical balance training and isometric strengthening groups.
Main measures
Dynamic balance (overall stability index and the modified Clinical Test of Sensory Interaction and Balance), pain (visual analogue scale), physical function (30-s chair stand test and 40-meter fast-paced walk test) and quality of life (Knee Injury and Osteoarthritis Outcome Score).
Results
Eighty-nine patients enrolled in the study. The Biodex training group, the classical training group, and the control group had overall stability index values of 1.0 ± 0.07, 1.4 ± 0.07 and 1.4 ± 0.07, and the Modified Clinical Test of Sensory Interaction and Balance – Condition-3 values of 0.7 ± 0.04, 0.9 ± 0.04 and 0.9 ± 0.04 respectively, at the end of treatment. In terms of pain scores on movement, each group showed significant improvement compared to their baseline, and the classical balance training group had better scores than the control group. No other significant difference was found between the groups. Physical function and quality of life outcomes showed significant main effects only in the time factor.
Conclusions
Balance and proprioception exercises may have positive effects on dynamic balance and pain. The effects on physical function and quality of life should be investigated in further studies with larger sample.
Introduction
Symptomatic knee osteoarthritis is the most common joint disease in adults aged 45 years and older and is more common in women.1,2 The pain and loss of physical function caused by knee osteoarthritis significantly disrupt activities of daily living and have been extensively studied in the literature.3,4
It is also known that knee osteoarthritis leads to decrease in proprioception, impairs balance5–8 and increases the risk of falls. 7 The incidence of falls in symptomatic knee osteoarthritis has been reported to be 26.5%, 9 and a recent study reported that the risk of recurrent falls increases 1.5-fold in patients with clinical knee osteoarthritis. 10 Falls due to balance disorders often occur during dynamic activities such as walking and stair climbing. 11 Correction of balance disorders is of great importance to prevent falls and associated fractures in the elderly population, in which knee osteoarthritis is common. In addition, loss of proprioception is also known to contribute progression of activity limitations in knee osteoarthritis.12,13 In this regard, improving proprioception may reduce the risk of falls while slowing the progression of activity limitation.
Exercise therapy has been shown to be effective in patients with knee osteoarthritis and is recommended in several guidelines.14,15 Strengthening exercises are the most studied and proven in their efficacy in the treatment of osteoarthritis.3,16,17 In addition to improving pain and physical function, muscle strengthening exercises also have a positive effect on balance by increasing muscle strength and joint stability. However, home exercise programs in particular, which are among the most commonly used and feasible strengthening programs, may not be sufficient to improve proprioception. 18 Proprioception exercises may help improve proprioception by stimulating muscle spindles and cortical reorganization19,20 and may be more effective than strengthening exercises. 21 There are few studies in the literature investigating the effects of balance and proprioception exercises on balance in knee osteoarthritis. 22
Although many clinical tests exist to assess balance, the results of these tests are subjective, exhibit scale attenuation effects, and are generally not responsive enough to measure small progress or deteriorations in a subject's balance ability. 23 However, quantitative assessment instruments provide objective data, have less variability in test performance, do not have a subjective scoring system as in clinical tests, and are sensitive to small changes. 23 In addition, it is possible to detect disorders that do not yet have clinically significant effects by quantitative assessment. The Biodex Balance System™ SD (Biodex Medical Systems, Inc., Shirley, NY, USA) is a reliable and valid quantitative balance assessment tool24–26 and has been used in several studies.27,28
This study aimed to investigate the effects of balance and proprioception exercises using two different methods (classical balance training and Biodex Balance System) in addition to home-based strengthening exercises on dynamic balance, pain, functional status and quality of life in patients with knee osteoarthritis.
Methods
This study was planned to compare the effects of isometric strengthening exercises plus balance and proprioception exercises performed by two different methods (intervention groups) with isometric strengthening exercises (control group) alone. This was a single-center randomized trial with three parallel arms; Biodex training (BT), classical balance training (CT) and control groups.
Patients admitted to our tertiary outpatient clinic with a diagnosis of knee osteoarthritis were recruited. The study was conducted with female patients aged between 40 and 70 years to exclude age-related musculoskeletal problems and gender differences in outcome measures as confounding variables. The purpose and method of the study were explained to eligible patients, and written informed consent was obtained from those who agreed to participate. Patients were included if they had a knee osteoarthritis diagnosis according to the American College of Rheumatology (ACR) diagnostic criteria, 1 had suffered from knee pain for at least six months (chronic knee osteoarthritis), 21 had radiologically verified bilateral definite knee osteoarthritis (grade II or grater) according to the Kellgren–Lawrence classification 29 and had not previously participated in a regular exercise program. Patients who had undergone knee surgery, who had received hyaluronic acid or corticosteroid injections into the knee within six months, patients with extreme degenerative changes (grade 4)21,30,31 and patients with diseases that might affect balance were excluded because of possible confounding effects. The study protocol was approved (Number: 28012014/2) by the institutional review board of Izmir Bozyaka Training and Research Hospital and was conducted in accordance with the principles of the Declaration of Helsinki. The study was registered on the ClinicalTrials website under the ID of NCT05287802. Patients were randomized into three groups using a table of random numbers via the random permuted blocks method. Patients enrolled in the study were referred to the outcome assessor for baseline assessment. The assessor then wrote the name and number ID for each patient on the next sealed, sequentially numbered opaque envelope and referred the patient to the physician supervising the exercises. The supervising physician opened the envelopes and assigned the patients to the Biodex training group, the classical balance training group, and the control group. The patients, the outcome assessor, care provider physicians, and the statistician were blinded to allocation. The supervising physician was not blinded.
Interventions
Biodex Balance System features a platform that can move simultaneously in the anteroposterior or medio-lateral direction in 12 different levels of stability within a 20-degree range of inclination, as well as a locked position for static environments. For this platform, 1 represents the least stable level and 12 represents the most stable level. This device can be used for testing as well as training. Interactive, game-like training modes are provided with the on-screen grid and score-keeping functions. Patients in the Biodex training group performed exercises with the Biodex Balance System once a day, three days a week for 10 weeks under the physicians’ supervision. The exercises last a total of 30 min, 15 min each, in two different training modes ‘postural stability’ and ‘maze control’. The postural stability training mode is designed to emphasize specific movement strategies by placing markers anywhere on the screen grid. The patient strives to touch the targets with the cursor on the screen during the session. The maze training mode allows the patient to follow a reproducible pattern of movement throughout a maze. The patient strives to hit the targets without touching the boundary lines. Patients completed their training in stability levels six through ten in both exercise modes.
Patients in the classical balance training group completed the exercise program once a day and three days a week during the 10-week period under the physicians’ supervision. The exercises consisted of standing on one leg, tandem walking (heel-to-toe), balance board exercises, Romberg exercise, backward walking, and side-to-side stepping exercises. The total duration of these exercises was 20–30 min.
In addition, closed kinetic chain exercises were included in the training program as an essential part of the exercise treatment for proprioception and balance.22,32 However, the Biodex Balance System was not suitable for large joint movements due to the limited platform area. For this reason, both intervention groups received closed kinetic chain exercises in addition to their own exercise program, which was applied in exactly the same way. The closed kinetic chain exercises were performed in three sets of 10 repetitions with 5 s rest between each exercise. The exercises consisted of mini-squats, wall sits and lunges.
Isometric home exercises, which can be considered the most basic and feasible effective strengthening program, were selected as control. Although the control group performed only isometric exercises, the intervention groups performed both balance and proprioception exercises and isometric exercises. The program consisted of isometric strengthening exercises for the quadriceps and hamstrings performed at home once a day, three days a week for 10 weeks. The exercises were performed as 10 repetitive cycles of 6-s contractions and 2-s rest periods. All patients were given a daily exercise chart to mark the home program, and adherence to the exercises was monitored weekly by telephone call. During the study, pharmacological treatments for all patients were managed by blinded care provider physicians according to current treatment guidelines.
Outcome measures
Dynamic balance was assessed using the Biodex Balance System. The postural stability test, whose reliability to evaluate dynamic balance has been demonstrated, was performed with the following parameters: Duration: 20 s, Stability level: 8, and Stance: two legs. 24 Patients completed three trial repetitions before the test. The value of the overall stability index is obtained by calculating the standard deviations of the degrees of inclination with respect to the zero point (locked position). 33 Higher values indicate poorer equilibrium. However, since this testing protocol uses the device's mobile platform similarly to the device's training modes, it was possible that the results were biased in favor of the Biodex training group. Therefore, a second measurement method was used that has a different operating principle than the device's training modes and is unique for all patients: the modified Clinical Test of Sensory Interaction and Balance (mCTSIB). The mCTSIB test is well-documented in the literature as an effective test for identifying individuals with mild to severe balance problems.5,34 The entire test is performed with the platform in the locked position. The test consists of 4 conditions: Condition-1: eyes open firm surface, Condition-2: eyes closed firm surface, Condition-3: eyes open dynamic (foam) surface, and Condition-4: eyes closed dynamic (foam) surface. 35 Reliability and validity studies have been conducted for this test. 26 Although this test was developed primarily to assess the interaction of the somatosensory, vestibular and visual systems, the firm and dynamic surface tests already assess static and dynamic balance, respectively. The conditions under which visual data are blocked are designed to detect even minor balance disturbances caused by the sensorimotor system. The sway index obtained as a result of the test represents the average position of the patient's center of mass relative to the center of the platform. Higher values indicate poorer balance. Overall stability index, mCTSIB Condition-3 and mCTSIB Condition-4 dynamic balance assessment tests were determined to be the primary outcomes of this study.
Secondary outcome measures were selected in accordance with the Outcome Measures in Rheumatology Clinical Trials (OMERACT)- Osteoarthritis Research Society International (OARSI) core set. 36 Patients’ pain scores at night, at rest, and during movement were measured using visual analogue scale (0–100 mm; 0 indicates no pain and 100 indicates severe pain). Physical function was assessed using the 30-s chair stand test 37 and the 40-meter fast-paced walk test, 38 which are recommended by the Osteoarthritis Research Society International. For the 30-s chair stand test, patients sit in a chair with the knees bent slightly more than 90 degrees and the feet on the floor at an angle behind the knees. Although arms are crossed in front of the chest, patients stand up with lower limbs fully extended and sit back down with full contact to the chair. The movement of standing up and sitting down is counted as one cycle. The number of cycles during the 30-s period is recorded. Increasing values indicate good performance. During the 40-meter fast-paced walk test, two cones are used to mark the start and stop lines of a 10-meter walkway. Patients are asked to walk as fast as they can along with the walkway without running, and then turn around four times, and the total time recorded. Decreasing values indicate good performance. Quality of life of patients was assessed using the quality of life subscale of the Knee Injury and Osteoarthritis Outcome Score (KOOS). 39 The KOOS consists of five subscales assessing pain, other symptoms, activities of daily living, sports and leisure time and quality of life. Each question is scored on a five-point scale ranging from 0 to 4. Scores close to 100 represent good outcomes, while scores close to 0 represent poor outcomes. Outcome assessment was performed at two time points: baseline and the end of the study. In addition to the primary and secondary outcome measures, adverse effects were also recorded.
Sample size
In our pilot study of 15 patients (five patients in each group), the effect size of the group*time interaction for the overall stability index was 0.37 (partial eta squared). G*Power ® (Version 3.1.9.6) program, ‘ANOVA: Repeated measures, within-between interaction’ test was used to calculate the sample size. To detect a difference of this magnitude with a mixed analysis of variance with a power of 80% and a significance level of 0.05%, the total number of samples required was calculated as 78. Considering the 10% dropout rate the total sample size was set at 90.
Statistical analysis
The main effects and group-time interactions were tested via type 3 mixed design analysis of variance using single within subject (time) and single between subject (group) factors with baseline values as covariates. 40 When a significant effect was detected, post hoc tests were performed for pairwise comparisons. Because the study had three primary outcomes Bonferroni correction was applied, taking into account multiplicity. As a result, a P value of 0.016 or less for the primary outcomes and 0.05 or less for the remaining outcomes was set as the threshold for statistical significance. Intention-to-treat analysis included all randomized patients. Missing data were imputed using the expectation-maximization method with regression analysis. All outcome variables were included in the model.
Results
Eighty-nine of 172 recruited patients enrolled in the study. Of the randomized patients, 14 did not complete the study. The flowchart is shown in Figure 1. There was no statistically significant difference between the groups at baseline, except for radiological stages. The number of patients with stage 3 was higher in the Biodex training group than in the other two groups (P = 0.025). The descriptive characteristics and baseline findings of the patients are provided in Table 1. None of the patients reported any adverse effects.
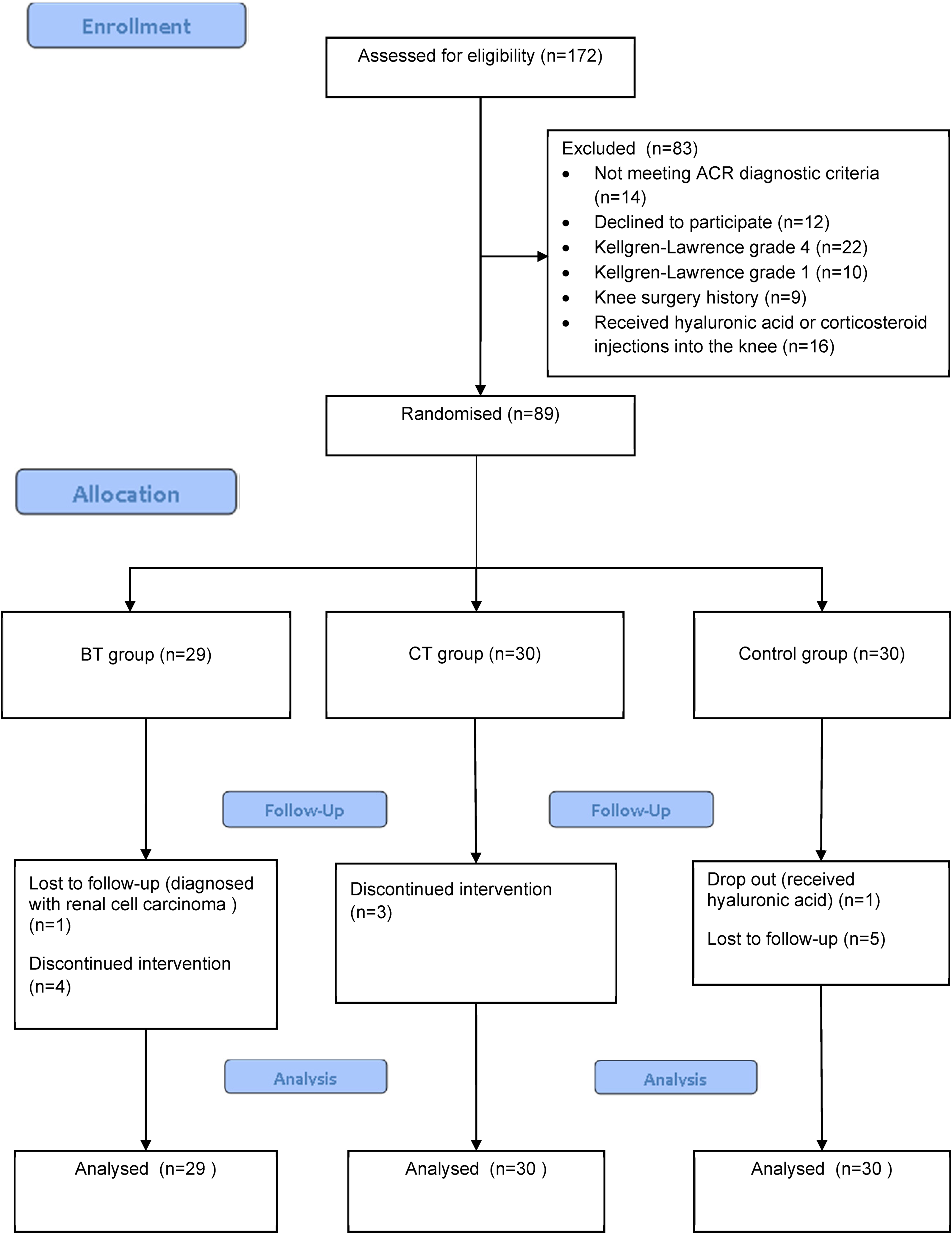
Flowchart of study.
Demographic characteristics and baseline findings of patients.
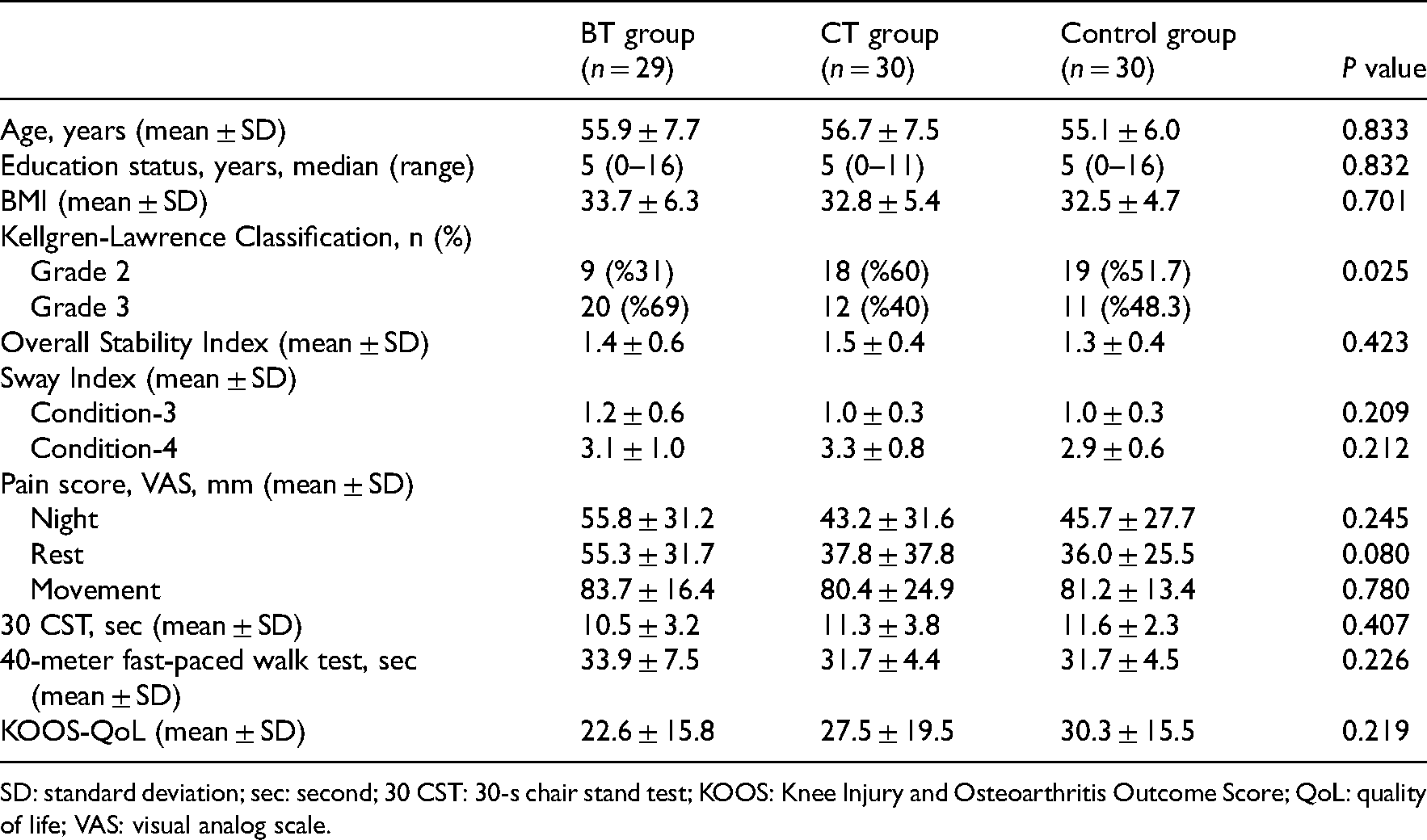
SD: standard deviation; sec: second; 30 CST: 30-s chair stand test; KOOS: Knee Injury and Osteoarthritis Outcome Score; QoL: quality of life; VAS: visual analog scale.
Analysis of variance revealed significant interactions between group and time and main effects of time. A significant interaction was found only for the overall stability index (F2,85 = 8.365, P < 0.01), Condition-3 sway index (F2,85 = 7.927, P = 0.001), and pain scores on movement (F2,85 = 4.259, P = 0.017). Pairwise comparisons of post-treatment scores are shown in Table 2. At the end of treatment, only the Biodex training group showed significant improvement in overall stability scores compared to baseline and had better scores than the classical balance training group (P = 0.002) and the control group (P = 0.002) (Figure 2). For Condition-3 sway index scores, each group showed significant improvement at the end of treatment compared to their baseline values. In addition, the Biodex training group had better scores than the classical balance training group (P = 0.001) and control (P = 0.005) group (Figure 3). For pain scores on movement, each group showed significant improvement compared to their baseline and the classical balance training group had better scores than the control group at the end of treatment (P = 0.015) (Figure 4). No other significant difference was found between the groups in the other pairwise comparisons (Table 2).
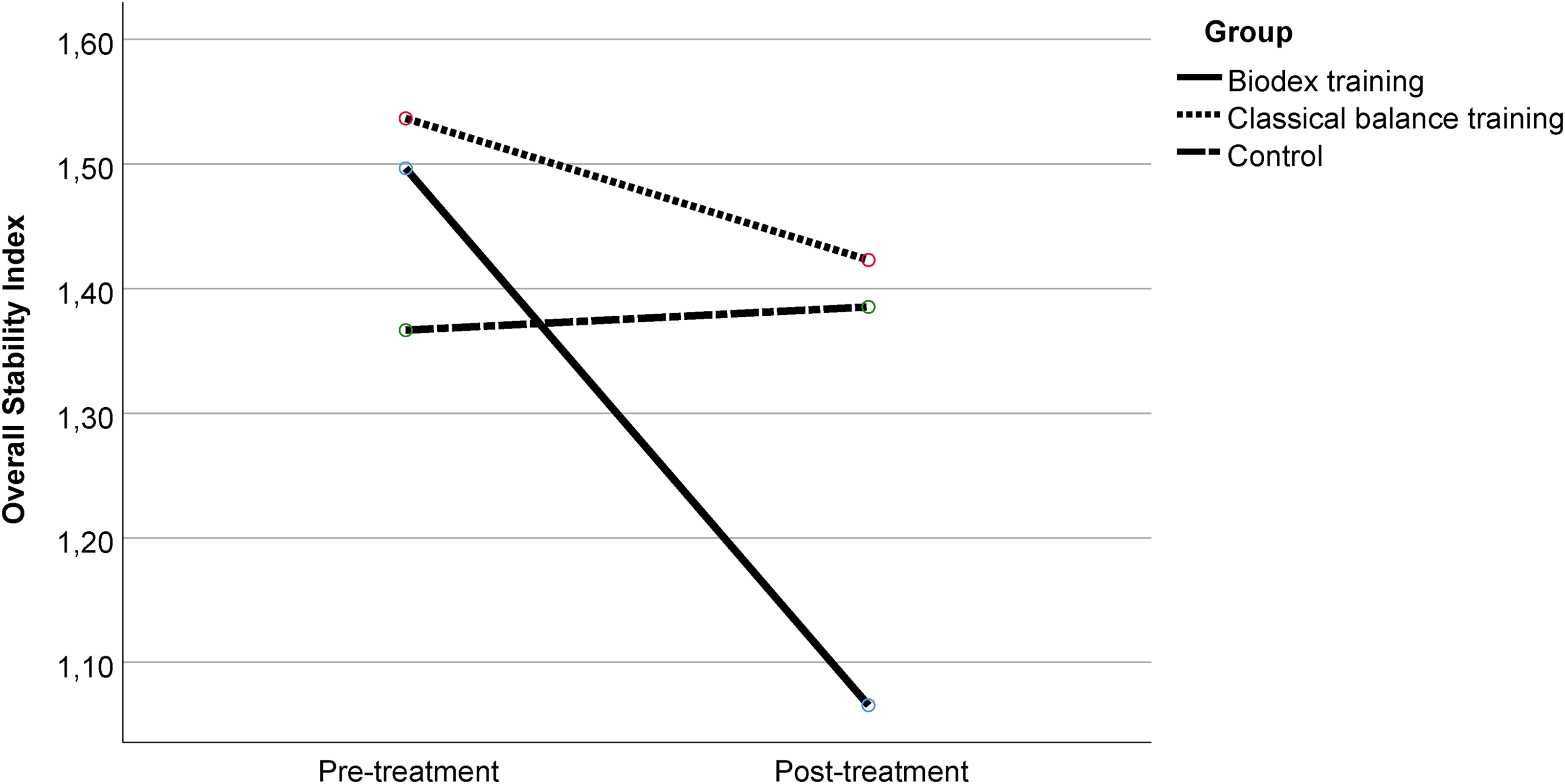
Comparison of overall stability index scores at baseline and at the end of the study. Only the Biodex training group showed significant improvement in overall stability scores compared to baseline (P < 0.01) and had better scores than the classical balance training group (P = 0.002) and the control group (P = 0.002) at the end of treatment. Data are mean (95% CI).
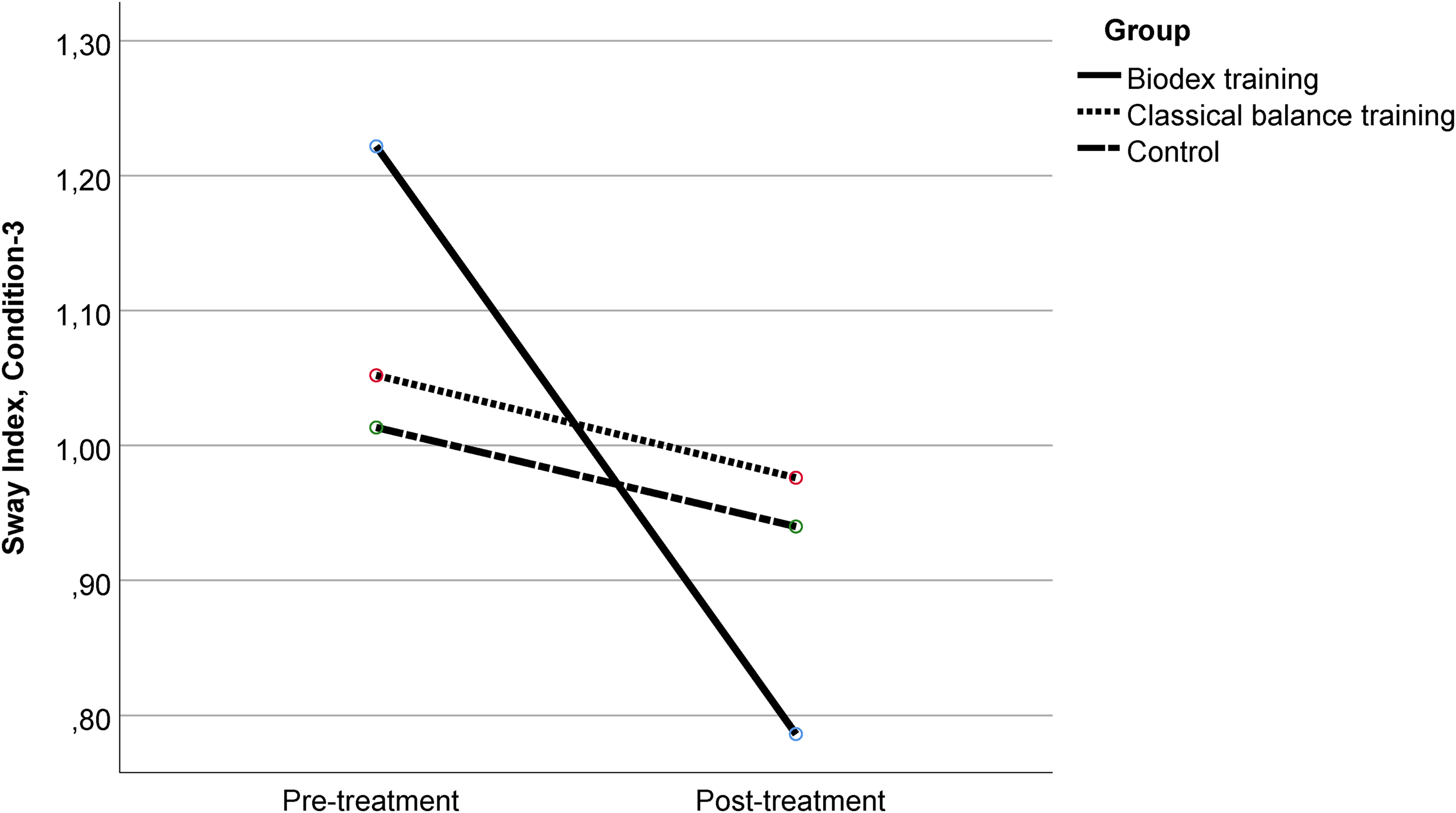
Comparison of Condition-3 sway index scores at baseline and at the end of the study. At the end of the treatment, the Biodex training, classical balance training and control groups showed significant improvements compared to their baseline; P < 0.01, P = 0.025 and P = 0.006, respectively. In addition, the Biodex training group had better scores than the classical balance training group (P = 0.001) and the control group (P = 0.005). Data are mean (95% CI).
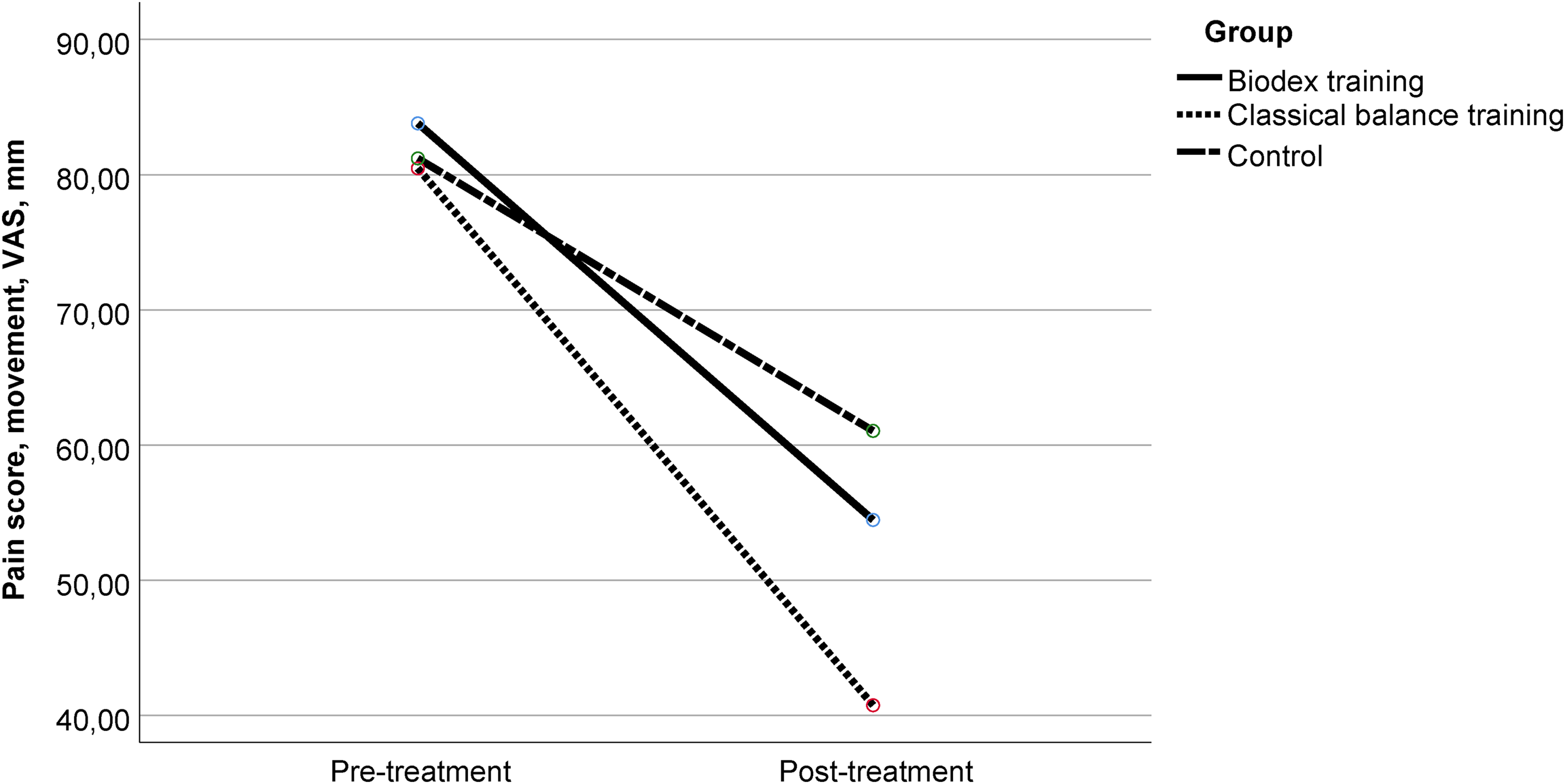
Comparison of pain on movement scores at baseline and at the end of the study. At the end of treatment, each group showed significant improvement compared to their baseline (P < 0.01), and the classical balance training group had better scores than control group (P = 0.015). Data are mean (95% CI).
Post-treatment scores and pairwise comparisons.a
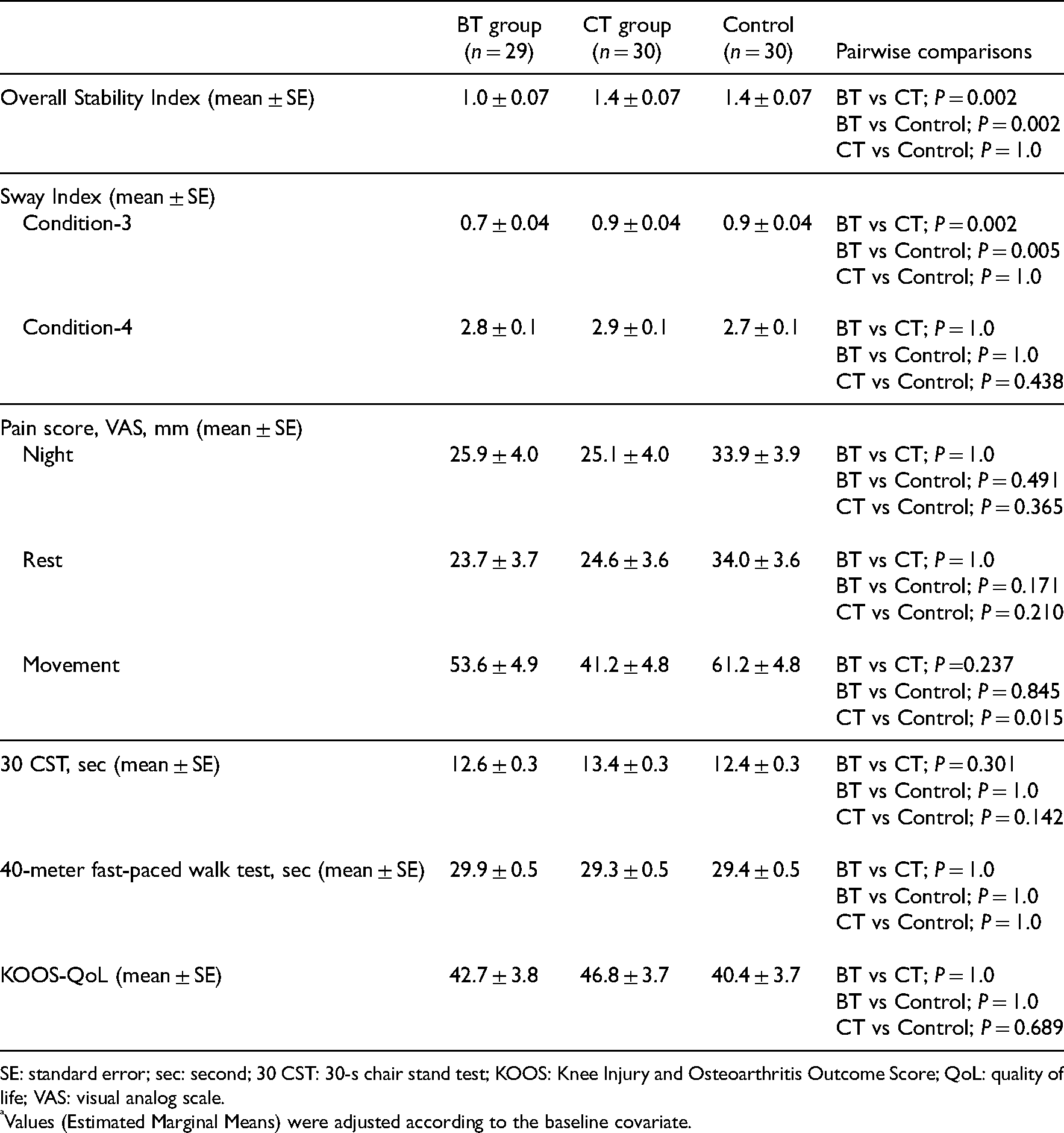
SE: standard error; sec: second; 30 CST: 30-s chair stand test; KOOS: Knee Injury and Osteoarthritis Outcome Score; QoL: quality of life; VAS: visual analog scale.
Values (Estimated Marginal Means) were adjusted according to the baseline covariate.
Condition-4 sway index (F1,85 = 45.904, P < 0.01), 30-s chair stand test (F1,85 = 84.891, P < 0.01), 40-meter fast-paced walk test (F1,85 = 38.993, P < 0.01), and the quality-of-life subscale of the KOOS (F1,85 = 57.382, P < 0.01) showed significant main effects only in the time factor indicating an improvement for the whole sample but not differing at the group level at the end of the treatments. No significant main effects or interactions were found for the remaining pain scores.
Discussion
This study features a quantitative assessment of dynamic balance and a comparison of three exercise programs. Our results suggest that all exercise programs seem to be effective and Biodex training and classical training program may be of greater benefit in improving dynamic balance and pain on movement, respectively.
There are very few studies in the literature using Biodex Balance System as an exercise tool in patients with knee osteoarthritis. Jahanjoo et al. compared the effects of physical therapy plus quadriceps strengthening program and Biodex exercises in addition to the former and showed the superiority of the Biodex group in terms of fall risk, mobility and pain. 41 The improvements in fall risk and mobility appear to be compatible with the results we observed in dynamic balance in our study. In his study comparing the effects of strengthening–stretching exercises and a sensorimotor exercise program (classical balance exercise program) in addition to former, Ahmed found that the sensorimotor exercise group scored better than the control group in postural stability measures. 42 However, in our study, we did not find the superiority of the classical balance training group over the control group in terms of dynamic balance. Visual feedback has been shown to provide additional sensory input that contributes to a better perception of body position and the development of a better balance response. 43 In addition, training with game-like exercises has been shown to improve learning, motivation and sensorimotor integration by increasing dopamine levels and contributing to better dynamic balance.28,44 These features may explain the superiority of the Biodex training group over the other groups in the overall stability index and Condition-3 tests. However, we did not find the superiority of the Biodex group in Condition-4 test. Studies evaluating the efficacy of exercise treatments in knee osteoarthritis with mCTSIB are very rare and present conflicting results on the Condition-4 test in the literature.45,46 The variation of visual compensation among patients may have caused this situation. Nevertheless, although Condition-4 is a compelling test to detect subtle deficiencies, Condition-3 is more in line with real conditions. In conclusion, the results of our study together with the literature suggest that exercises performed with the Biodex Balance System may be beneficial for dynamic balance.
Many studies have shown that both hamstring and quadriceps strengthening and balance-proprioception exercises improve pain in patients with knee osteoarthritis.3,4,16,17,22,47 In our study, we found that classical balance exercises in addition to home exercises lead to better improvement in movement pain. This finding is similar to the results of Lin et al. 28 The limited platform area of the Biodex device or the greater increase in muscle strength with classical exercises may be responsible for this difference. In his study using classical balance exercises, Ahmed found better quadriceps torque values in the study group than in the control group, which performed only strengthening and stretching exercises. 42 In this regard, it would be appropriate to measure muscle strength as an outcome to compare the Biodex training group and the classical balance training group in further studies.
There are conflicting results on Biodex training regarding patient-reported assessment of physical function.41,48 Also Lin et al. showed that active video games performed better than a traditional exercise program on performance-based assessments of physical function (10-m walking time and stairs ascent time) but not on patient self-administered assessments (Western Ontario and McMaster Universities Osteoarthritis Index). 28 In addition, the classical balance exercise program and exercises with visual feedback have been shown to improve quality of life better than a traditional exercise program.28,42 In our study, we did not find an improvement in physical function or quality of life in either group, but we did find an improvement in the main effect of time in both assessments. These findings suggest that exercise therapy may have a positive effect on physical function and quality of life, but the contribution of balance and proprioception exercises is subtle and needs further investigation.
Although our study has a larger sample size than other studies in the literature, the fact that the significant changes observed in the main effect of time were not observed in the interaction of group and time suggests the need for studies with larger sample sizes.
In conclusion, balance and proprioception exercises may have additional beneficial effects in patients with knee osteoarthritis. However, the relationship between these improvements, detected by sensitive methods, and clinical results is not yet clear, and given the ease of application of isometric exercises and the limited accessibility of the device, it may be beneficial to perform balance and proprioception exercises in selected patients. Patients with balance impairments identified by quantitative or clinical methods and patients with poor adherence to the exercise program due to motivational problems may be candidates for this treatment. The effects of balance and proprioception exercises on physical function and quality of life should be investigated in further studies with larger sample size.
Clinical messages
Falls occur frequently during dynamic activities in patients with knee osteoarthritis.
It is only possible to monitor the effects of treatment with quantitative methods.
Visual biofeedback may be an effective method to improve balance in patients with knee osteoarthritis.
Classical balance exercises can contribute to strengthening exercises for pain.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.