
Abstract
Objective
To examine the efficacy and safety of aquatic exercise for people with knee osteoarthritis.
Data sources
PubMed, Web of Science, Embase, CENTRAL, CNKI and WanFang databases were searched from 1966 to September 2022.
Review methods
Randomized controlled trials evaluating aquatic exercise for people with knee osteoarthritis compared with no exercise and land-based exercise were included. The Grading of Recommendations Assessment, Development and Evaluation system was used to evaluate the certainty of evidence.
Results
Twenty-two studies with 1394 participants were included. Compared with no exercise (13 trials with 746 participants), low-to high-certainty evidence revealed that aquatic exercise yielded significant improvements in patient-reported pain (SMD −0.58, 95% CI −0.82 to −0.33), stiffness (SMD −0.57, 95% CI −1.03 to −0.11) and physical function (SMD −0.35, 95% CI −0.52 to −0.18) immediately postintervention. A sustained effect was observed only for pain at three months postintervention (SMD −0.48, 95% CI −0.91 to −0.06). The confidence intervals demonstrated that the pooled results do not exclude the minimal clinically important differences. There were no significant differences between the effects of aquatic exercise and land-based exercise (13 trials with 648 participants) on pain (SMD −0.12, 95% CI −0.29 to 0.04), stiffness (SMD −0.17, 95% CI −0.49 to 0.16) or physical function (SMD −0.13, 95% CI −0.28 to 0.02). No study reported a serious adverse event in relation to aquatic exercise.
Conclusion
Aquatic exercise provides a short-term clinical benefit that is sustained for at least three months postintervention in terms of pain in people with knee osteoarthritis.
Introduction
Osteoarthritis (OA) is the most prevalent chronic joint disease and is associated with painful symptoms, joint stiffness and functional limitations of daily living. 1 Globally, knee OA is the main cause of disability in terms of years lived with disability. 2 A recent report on the Global Burden of Disease emphasized that knee OA accounts for approximately 85% of the burden of OA, and the prevalence of knee OA substantially increased by 32.7% from 2005 to 2015. 3 Nearly 8.1% of people aged 45 years or older in China have symptomatic knee OA according to the China Health and Retirement Longitudinal study, 4 and the prevalence will continue to rise with population ageing, leading to an increased strain on individuals effected and health-care systems. Therefore, facilitating and developing effective management strategies for knee OA has been flagged as a public health priority. 5
In the array of nonpharmacological interventions, land-based exercise has been shown to alleviate pain and improve function in people with knee OA. 6 Evidence from a Cochrane review concluded that land-based exercise has beneficial effects on pain, physical function and quality of life in people with knee OA. 7 However, these types of exercise may aggravate mechanical loading on the affected joint and reduce treatment adherence, and they cannot be performed in people with severe clinical symptoms. In contrast, aquatic exercise can offer benefits over land-based exercise for people with knee OA because it provides the joint off-loading and assisted movement due to buoyancy.8–10
Despite the increasing number of randomized controlled trials (RCTs) examining these interventions, the most recent Cochrane review was based on studies published up to April 2015 11 and reported that aquatic exercise has small and short-term effects on pain, function and quality of life for people with knee and/or hip OA. However, the evidence on knee OA alone was poor, 11 since the three included trials that only recruited people with knee OA demonstrated no statistically significant effect. A more recent meta-analysis published in 2019 focused only on postmenopausal women with knee OA. 12 This review included six RCTs and concluded that aquatic exercise has no positive effect on pain, physical function or stiffness compared with the control. Overall, only three to six trials in these reviews11,12 included people with knee OA alone.
Furthermore, the safety of exercise is also a concern, since even in research settings, the rate of regular exercise participation has been low. 13 Specifically, people with knee OA who dropped out generally had a worse health condition and higher levels of exercise-induced pain than those who retained the program. 14 Therefore, this review aimed to evaluate the effectiveness and safety of aquatic exercise. In addition, minimal clinically important differences (MCIDs) are important considerations in clinical decisions and are discussed in this review.
Methods
This systematic review and meta-analysis was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Statement. 15 The study was registered in the International Prospective Register of Systematic Review (PROSPERO; Registration No. CRD42020219223).
PubMed, Cochrane Central Register of Controlled Trials (CENTRAL), Web of Science, Embase, China National Knowledge Infrastructure (CNKI) and WanFang databases were searched from 1966 to 20 September 2022. RCTs investigating the role of aquatic exercise in people with knee OA were included. The following search strategy was developed: (aquatic exercise OR aquatic training OR water rehabilitation OR hydrotherapy) AND (osteoarthritis OR knee osteoarthritis). The reference lists from the included trials and relevant systematic reviews were also manually searched. The language of publication was restricted to English and Chinese.
The inclusion criteria were as follows: (i) the study design was an RCT; (ii) participants had to be diagnosed with knee OA using accepted diagnostic criteria; (iii) the intervention was aquatic exercise; (iv) the comparisons included no exercise control (e.g. education, usual care) and land-based exercise; and (v) outcomes of interest were patients’ self reported pain, stiffness, physical function and safety assessment, including study withdrawals and adverse events related to aquatic exercise. The exclusion criteria were as follows: (i) participants who suffered from any other disease that may affect joints or had knee arthroplasty within 6 months; and (ii) other passive hydrotherapy methods, such as balneotherapy and spa therapy.
Two reviewers independently screened the titles and abstracts of potentially relevant articles after removing duplicates. All full-text articles were then assessed for eligibility. Any disagreement was resolved by discussion between the two reviewers and by the decision of a third reviewer. Reviewers independently extracted the data using a standardized form. The following information from the included studies was extracted: (i) study characteristics (e.g. first author, year of publication); (ii) population characteristics (e.g. number of participants, age, sex, Kellgren and Lawrence (KL) grading); (iii) intervention characteristics (e.g. exercise components, duration, frequency); and (iv) outcome data for both postintervention and follow-up points.
The quality of the included studies was evaluated by two reviewers using the Physiotherapy Evidence Database (PEDro). 16 All RCTs were examined for 11 items of methodologic quality with a total score ranging from 0 to 10 because the first item was not scored (eligibility criteria). Studies that obtain a score of ≥ 6 points are rated as high quality, whereas those with a score of < 6 points are rated as low quality. 17 Two reviewers independently evaluated the certainty of evidence in pooled analyses using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) system. 18 Evidence from RCTs began with high certainty of evidence and was downgraded for risk of bias, indirectness, inconsistency, imprecision, or publication bias. Disagreements regarding the quality of the included studies or GRADE assessment were resolved through consensus.
All analyses were carried out using the DerSimonian and Laird random-effects model, 19 with Stata 16.0 software to calculate (i) the relative risk (RR) for dichotomous outcomes and (ii) the standardized mean difference (SMD) for continuous outcomes, which was a unitless measure to combine effect estimates obtained from different scales, 20 all with 95% confidence intervals (CIs). Scale directions were aligned by adding negative values when needed, and a negative value corresponded to improvement of outcomes. The effect size threshold values for SMD were classified as 0.2 for small, 0.5 for medium and 0.8 for large. 21 Significance was set at P < 0.05. Heterogeneity between the trials was assessed using the chi-squared test (P < 0.1 indicates important heterogeneity) and the I2 statistic (a value of 50% or greater was considered substantial heterogeneity). 22 Sensitivity analysis was performed to exclude studies of low methodological quality (PEDro score < 6) to avoid distortion of findings. Egger's test was employed to investigate small-study effects when 10 or more studies were included.
In this study, the effect sizes pooled using SMD were transformed to absolute mean differences with pain, stiffness and function measures by multiplying by representative standard deviation (SD). For pain, we used the WOMAC pain scale (SD 19.6 on a 0 to 100 scale); for stiffness, we used the WOMAC stiffness scale (SD 23.4 on a 0 to 100 scale); and for physical function, we used the WOMAC function scale (SD 18.5 on a 0 to 100 scale).23,24 Pooled SDs of these measures were derived from large population-based observational studies in people with knee OA. According to evidence-based reports, 25 the MCID was defined as 9.7 for WOMAC pain, 10 for WOMAC stiffness and 9.3 for WOMAC physical function based on a 0- to 100-point scale (0 being the best and 100 being the worst).
Results
The flow diagram of each screening process is shown in Figure 1. The initial literature search identified 1095 articles, with 22 studies (n = 1394) included in this review (Figure 1).26–47 The mean age of the included participants was 63 years (range 53–71 years). More than 77% of the participants were female (n = 1077). Seven studies26,27,32,34,38,42 restricted participants with radiographic assessment of Kellgren and Lawrence Grade III or less, whereas six studies29,31,35,36,45,47 included participants with radiographic assessment of Kellgren and Lawrence Grade IV.
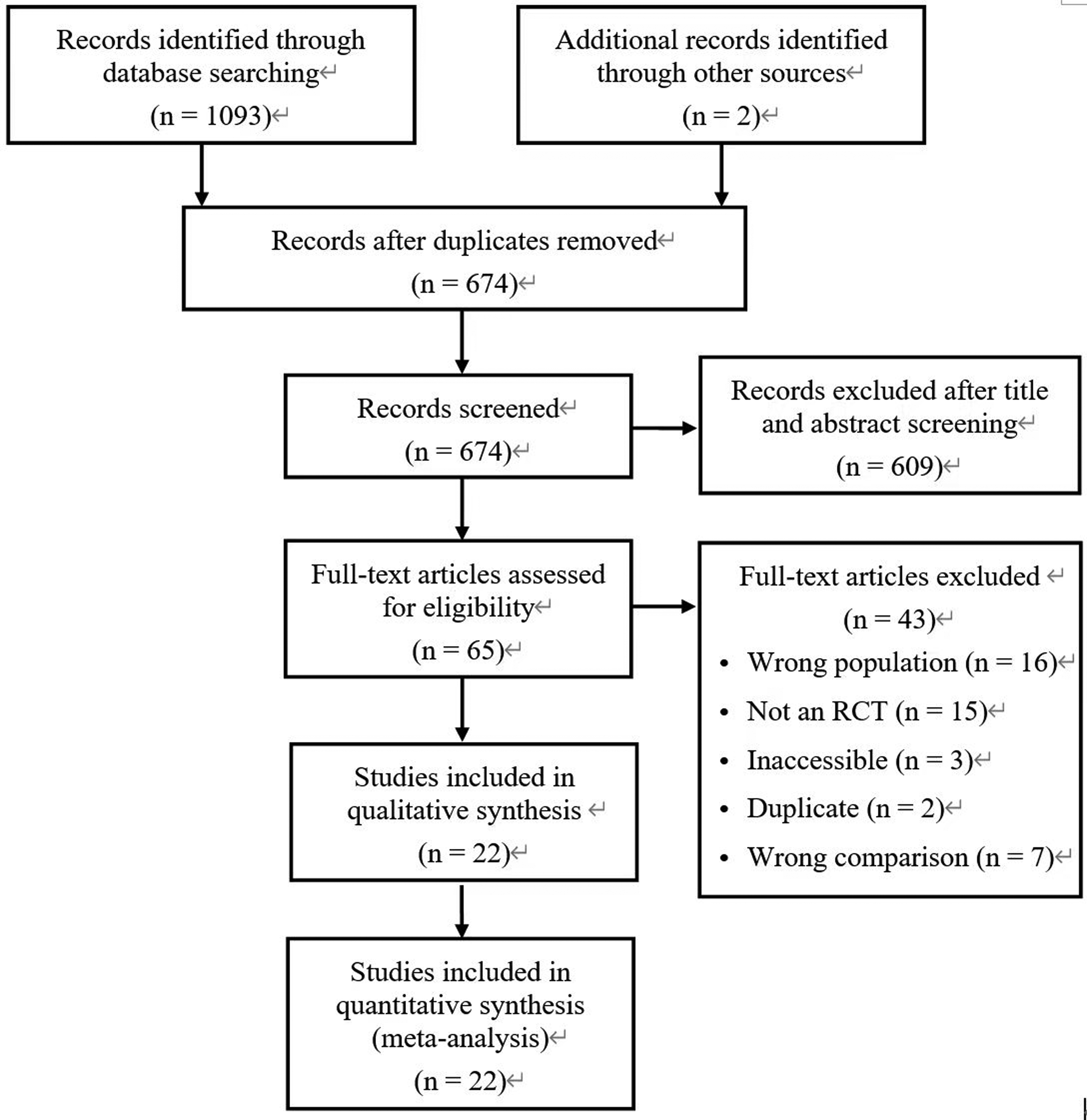
Flow diagram of study selection.
Nine studies26–29,34,38–40,44 compared aquatic exercise with no exercise control; nine studies30,32,35,41–43,45–47 compared aquatic exercise with land-based exercise; and four studies31,33,36,37 included both no exercise control and land-based exercise comparisons. Seven studies29,37–40,46,47 recorded the follow-up period of outcomes, ranging from 3 to 12 months. One study described three exercise allocations, including underwater treadmill, land-based treadmill and land-based cycle, and the mean effects of two land-based allocations were combined and compared with those of the underwater treadmill group. 45 One study allocated participants to two different forms of aquatic exercise, and the combined effect was compared with that of the control group. 34 The types of exercise in the aquatic intervention program varied among the included studies; however, it commonly included stretching, strength and aerobic exercises. The intervention duration ranged from 3 to 24 weeks, the frequency ranged from 2 to 5 sessions per week and the length ranged from 30 to 65 min per session. The exercise intensity of included studies were applied at 3–4 rating of perceived exertion (RPE), 33 and 4–6 RPE40,45 on Borg 1–10 scale; and 11–13 RPE, 38 13–14 RPE 44 and 13.7 ± 1.0 to 15 ± 1.5 RPE 39 on Borg 6–20 scale. Two studies using 65% and 70% to 85% maximal heart rate, respectively.35,36 Two studies described the intensity as “moderate” with no detail provided.26,37 The mean adherence rate was 87% (SD 5.8%). The water temperature was 30–34 °C, and the pool depth was 115–140 cm. The characteristics of the included studies are summarized in Table 1.
Characteristics of included studies.
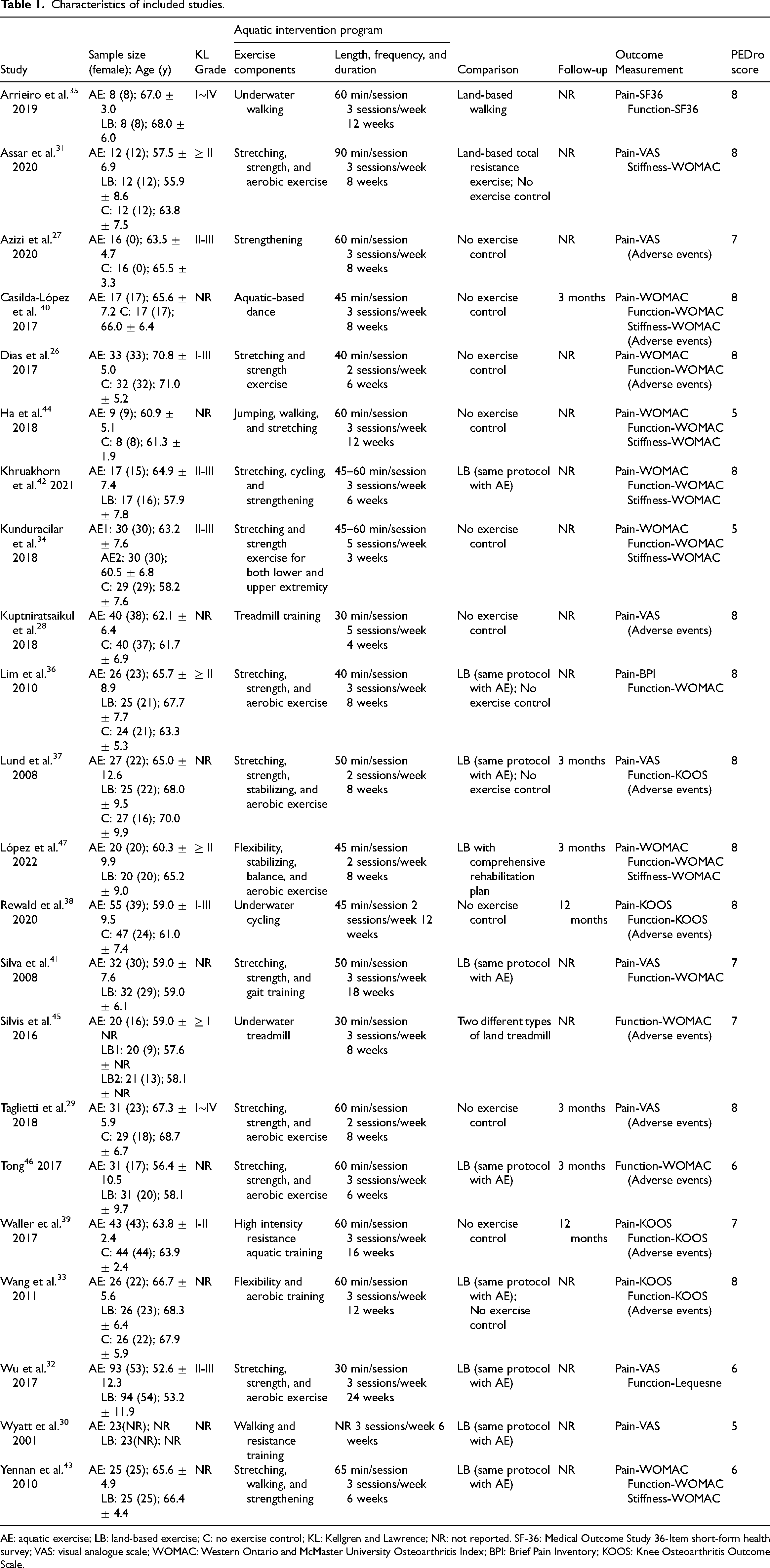
AE: aquatic exercise; LB: land-based exercise; C: no exercise control; KL: Kellgren and Lawrence; NR: not reported. SF-36: Medical Outcome Study 36-Item short-form health survey; VAS: visual analogue scale; WOMAC: Western Ontario and McMaster University Osteoarthritis Index; BPI: Brief Pain Inventory; KOOS: Knee Osteoarthritis Outcome Scale.
The mean score for quality assessment using the PEDro scale was 7.1 with a range of 5–8, indicating that studies were high quality. Low scores corresponded to studies that failed to describe the details of random sequences (14%; n = 3),30,34,44 concealed allocation (45%; n = 10),27,30,32,34,39,41,43–46 blinded the outcome assessor (23%; n = 5),32,34,42,43,46 blinded subjects and therapists (0%). The certainty of evidence ranged from low to high. The reasons for downgrading are shown in Table 2.
GRADE summary of findings.
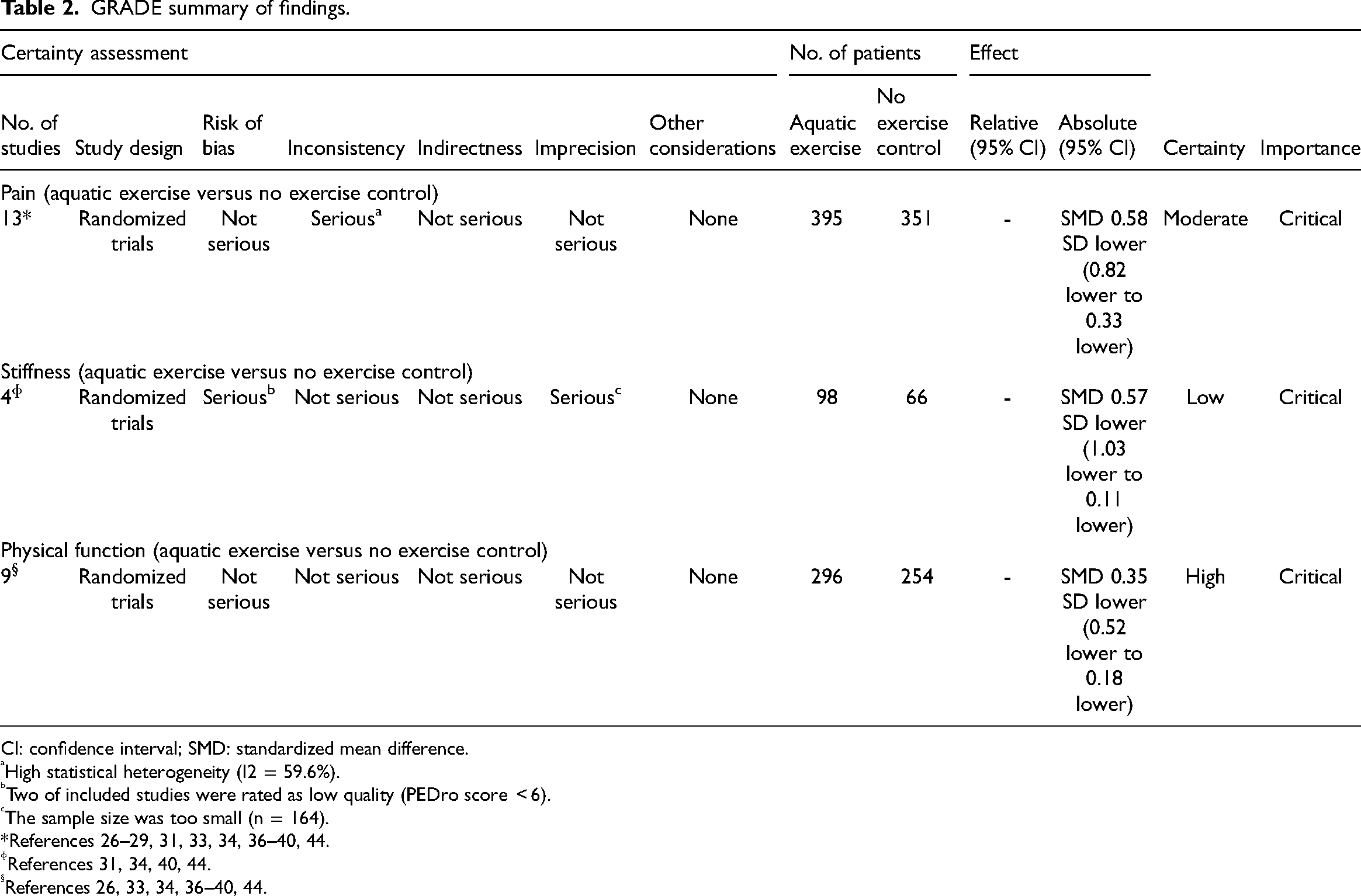
CI: confidence interval; SMD: standardized mean difference.
High statistical heterogeneity (I2 = 59.6%).
Two of included studies were rated as low quality (PEDro score < 6).
The sample size was too small (n = 164).
*References 26–29, 31, 33, 34, 36–40, 44.
References 31, 34, 40, 44.
References 26, 33, 34, 36–40, 44.
Outcome measure immediately after intervention
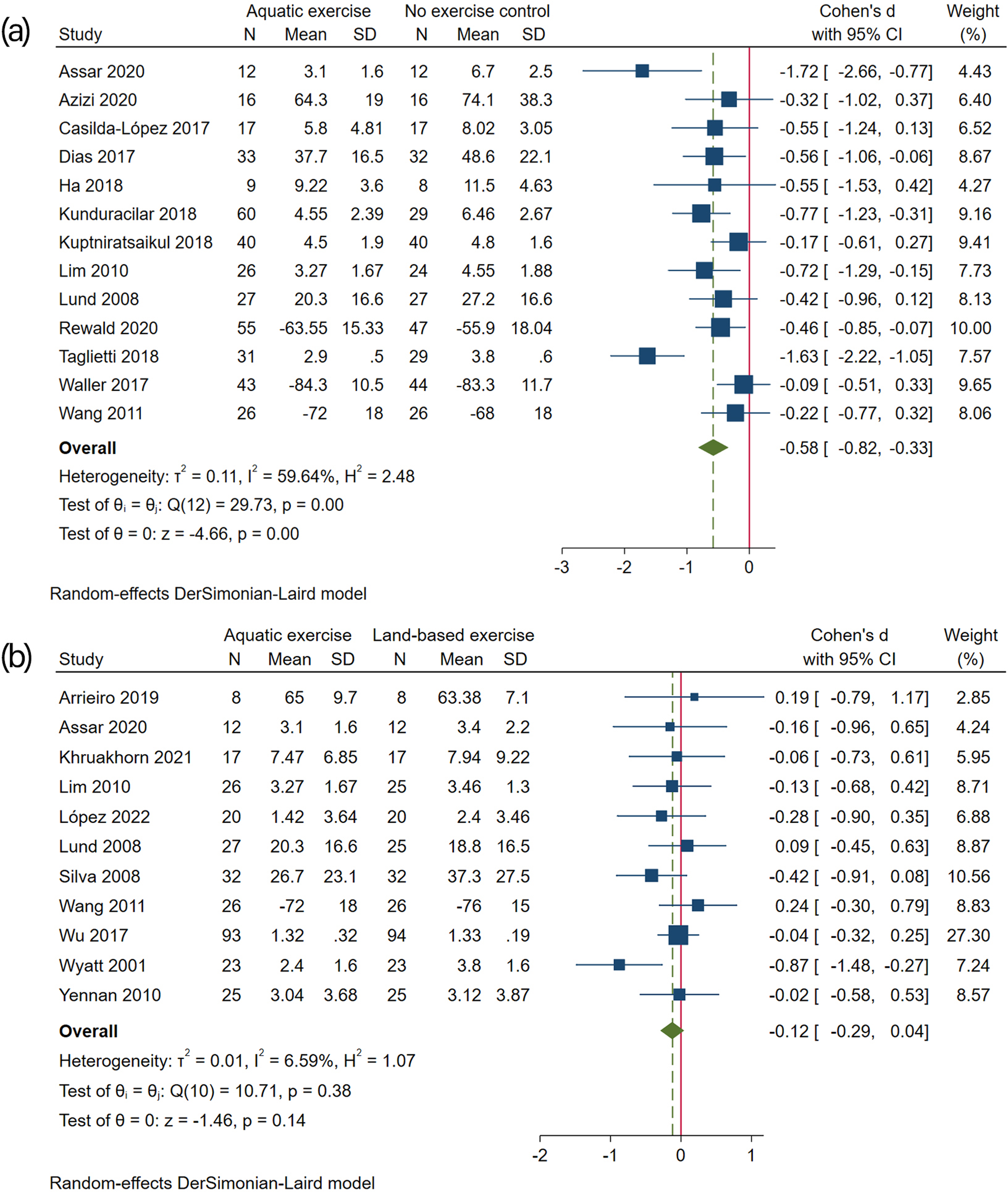
Forest plot for pain: (a) aquatic exercise versus no exercise control, and (b) aquatic exercise versus land-based exercise.
Eleven studies (n = 525)30–33,35–37,41–43,47 were included for aquatic exercise compared with land-based exercise, indicating no statistically significant difference in the management of pain between the two groups, with an effect size of −0.12 (95% CI −0.29 to 0.04; Figure 2(b)). For the sensitivity analysis, the meta-analysis was repeated by removing low-quality studies, 30 and there were no appreciable differences, with an effect size of −0.07 (95% CI −0.23 to 0.10).
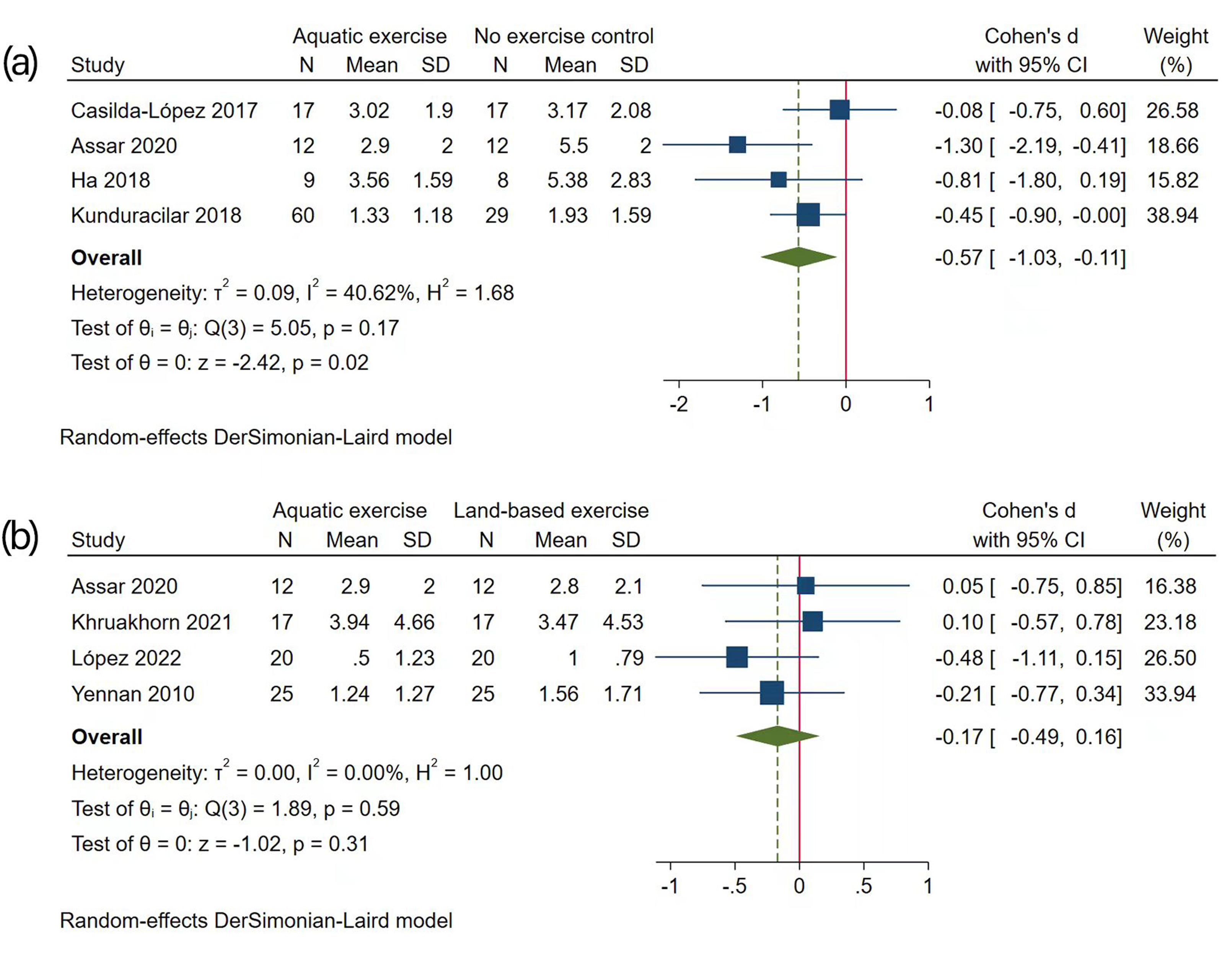
Forest plot for stiffness: (a) aquatic exercise versus no exercise control, and (b) aquatic exercise versus land-based exercise.
Four studies (n = 148)31,42,43,47 were included for aquatic exercise compared with land-based exercise, indicating no statistically significant difference in the management of stiffness between the two groups, with an effect size of −0.17 (95% CI −0.49 to 0.16; Figure 3(b)). Sensitivity analysis was not performed because all four included studies were rated as high quality.
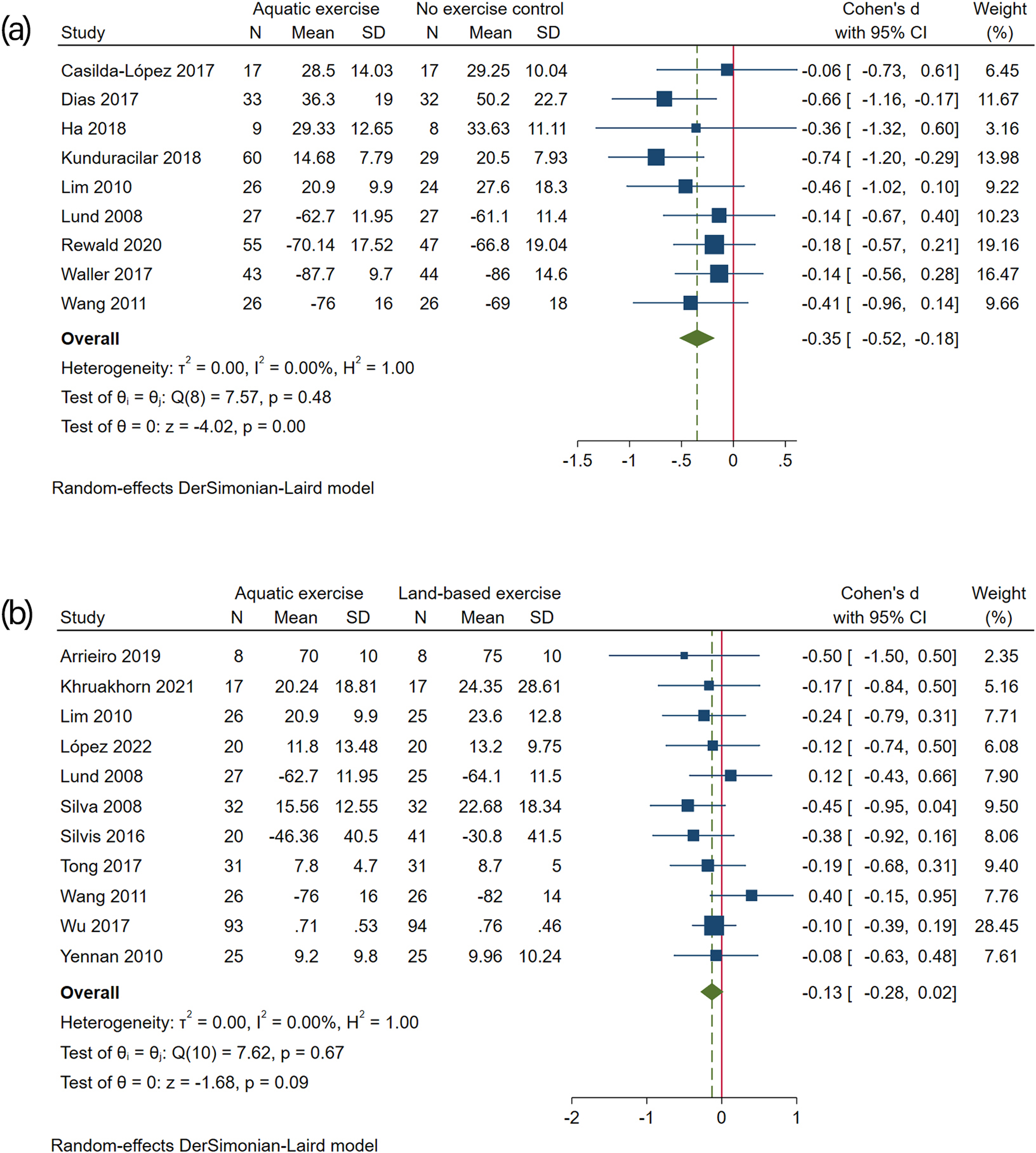
Forest plot for physical function: (a) aquatic exercise versus no exercise control, and (b) aquatic exercise versus land-based exercise.
Eleven studies (n = 590)32,33,35–37,41–43,45–47 were included for aquatic exercise compared with land-based exercise, indicating no statistically significant difference in the management of physical function between the two groups, with an effect size of −0.13 (95% CI −0.28 to 0.02; Figure 4(b)). Sensitivity analysis was not performed because all 11 included studies were rated as high quality.
Outcome measure at follow-up
Studies comparing aquatic exercise with no exercise control were included. After excluding one study 29 with extreme outliers, four studies37–40 with 277 participants were included. The pooled results demonstrated a significant benefit for pain management at three months after the end of intervention (SMD −0.48, 95% CI −0.91 to −0.06; Figure 5(a)), which was equivalent to 9.4 points lower (95% CI 1.2 to 17.8); a nonsignificant effect was noted at 12 months post-intervention (SMD −0.28, 95% CI −0.57 to 0.01; Figure 5(a)). There was no statistically significant effect for the management of physical function between aquatic exercise and no exercise control at three months (SMD −0.10, 95% CI −0.52 to 0.31; Figure 5(b)) and 12 months (SMD −0.15, 95% CI −0.43 to 0.14; Figure 5(b)) after intervention. Analysis was not performed since only one study reported on stiffness outcome.
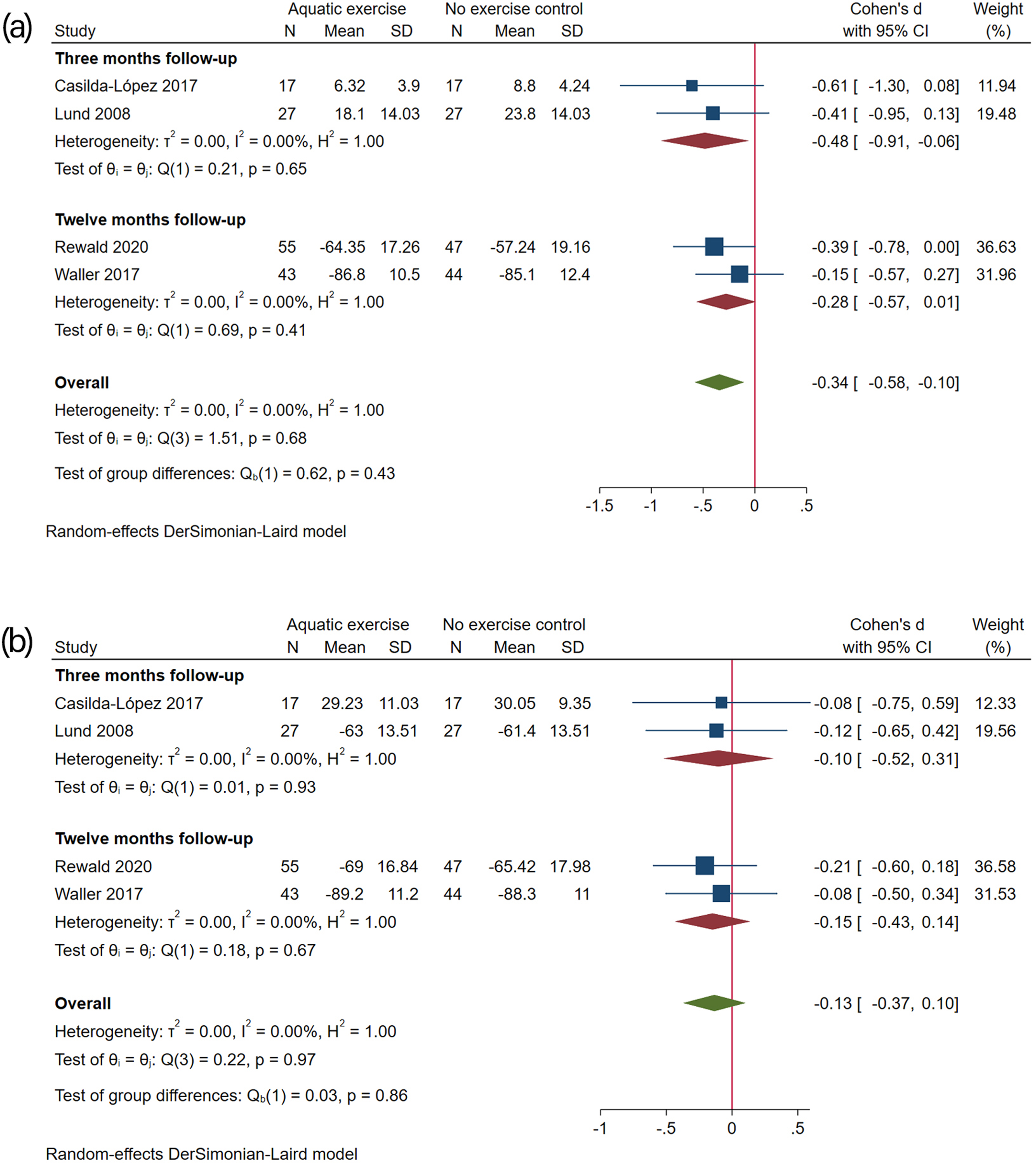
Forest plot comparing aquatic exercise with no exercise control at follow-up: (a) pain, and (b) physical function.
Discussion
This systematic review and meta-analysis investigating the effects of aquatic exercise on patient-reported outcomes among people with knee OA provides implications for clinical practice. The low-to-high certainty of evidence demonstrated that aquatic exercise resulted in an immediate significant benefit on pain, stiffness and physical function. The pain-relieving effect of aquatic exercise declined at three months after the end of intervention but was still significant; however, this sustained benefit was lost at 12 months postintervention.
Because of variability in the measurements of outcomes, SMDs were used to calculate the effect sizes. Nevertheless, statistically significant differences in SMDs do not fully reflect the clinically important improvements. Hence, pooled SMDs were transformed to absolute mean differences of outcomes to evaluate the clinically important improvements. In this study, the absolute mean differences in both pain and stiffness scores were beyond the cut-off of the MCID, and the 95% CI (3.3 to 9.6) for physical function did not exclude the MCID (9.3), indicating that aquatic exercise provided statistically and clinically important improvements for patient-reported outcomes. To date, only one systematic review 11 has investigated the effect of aquatic exercise for people with knee and/or hip OA, reporting a 5-point reduction in both pain and functional scores after the end of intervention, which is lower than our findings (11.4 and 6.5 points reduction in pain and functional scores, respectively). In contrast, we also noted a 9.4-point reduction in pain score at three months after intervention. This disagreement is certainly related to the number of included studies due to the time of the literature search, but more importantly, it is closely related to the different eligibility criteria of the studies. To limit clinical heterogeneity, we only included people with knee OA, and it is likely that the confounding factors of the included subjects led to the differences between clinical outcomes. In addition, it is also noteworthy that the MCID has obvious limitations, since it varies across baseline disease severity, OA location, underlying health disorder, different populations and studies.48–50 However, the conclusions of Bratels et al. 11 and our study both suggested the potential benefits of aquatic exercise.
With the update of relevant guidelines and the development of clinical practice, which exercise modality is more suitable for people with knee OA has attracted extensive attention. Although there have been two systematic reviews51,52 comparing the effects between aquatic exercise and land-based exercise on knee OA symptoms, these have all identified limitations in the number and quality of included trials when drawing conclusions, highlighting the need for further research. Our findings further supported that the effects of those two exercise modalities were comparable. However, it is worth noting that the risk of adverse events in land-based exercise was much higher than that in aquatic exercise.33,36,37,45 This is an important point when considering what advice is given to health care practitioners, since even slight adverse events may reduce exercise adherence, and it is the low exercise adherence rates that largely explain the decreased long-term effects of exercise for people with knee OA. 53 Thus, exercise intervention programs should focus on achieving higher adherence rather than increasing the intensity or amount of exercise.
Studies included in this review reported that participants have higher compliance and satisfaction with aquatic exercise programs,28,37,43,45 which can be attributed to the advantages of exercising in the aquatic environment. Aquatic pools for rehabilitation are generally heated to above 32 °C to prevent people from getting cold, and the heating effect of warm water may accelerate blood circulation, thereby reducing joint swelling and stiffness. Compared to the same activities on land, joint forces in the knee joint were reduced by 36–55% in the water environment. 54 Additionally, hydrostatic pressure may reduce peripheral oedema and dampen sympathetic nervous activity, leading to pain relief. 55 Another effect of water immersion relates to the enhanced activation in both sensory and motor areas of the cortex, 56 thereby helping those who have been unable to participate in physical activity for a long time to regain sports skills and improve self-efficacy. Overall, all aforementioned beneficial aspects could increase the levels of exercise participation, and lead to higher exercise adherence.
This systematic review and meta-analysis has several strengths, including a preregistered protocol, high quality of included studies and the GRADE assessment of certainty of evidence. However, there are limitations to this study that must be considered. First, we were unable to perform subgroup analyses to quantify the dose-response relationship between symptoms and duration, frequency and intensity of aquatic exercise due to the lack of sufficient information. Second, based on the current findings, the sustained benefit was observed only in pain outcomes with no longer than three months. Considering that a large proportion of people with knee OA are typically inactive and overweight, it is more important to help those people increase their daily physical activity. Additionally, researchers and clinicians should advocate and promote the benefits of exercise or physical activity for every people with OA and might consider the paradigm shift from supervised and prescriptive exercise intervention to lifestyle physical activity as a comprehensive strategy in conjunction with physical therapy and education. In light of the advantages of aquatic exercise, it may be considered the first part of a rehabilitation program for people with knee OA.
Clinical messages
Aquatic exercise demonstrated significant and immediate clinical improvements in patient-reported outcomes for people with knee OA.
The effect on pain was secured for at least 3 months.
The benefits of aquatic exercise and land-based exercise on patient-reported outcomes are comparable.
Footnotes
Acknowledgements
We appreciate great effort of authors who conducted clinical trials included in our study.
Author contributions
ZX developed the protocol, completed the collection of data, formal analysis of data and drafted, reviewed and edited the manuscript; YDW completed the collection of data, formal analysis of data, provided supervision and help to drafting the manuscript; YZ reviewed and edited the manuscript; YFL contributed to the conceptualization of the review; YHW conducted project administration and revised the manuscript.
Declaration of conflicting interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Key Research and Development Program of China (grant no. 2020YFC2006700).