
Abstract
Objective
To determine the effect of interventions on physical activity levels of patients awaiting abdominal resection surgery using self-reported as well as device-measured outcome measures.
Data source
PubMed and EMBASE databases were searched on the 18th of April 2023 up to April 2023 for studies on interventions to promote physical activity during the preoperative phase.
Review methods
Studies were included if pre- and post-intervention physical activity was measured between diagnosis and abdominal surgery. Risk of bias was assessed by the Physiotherapy Evidence Database (PEDro) assessment tool for trials. Meta-analyses were performed to assess the effect of the pre-surgery activity promoting interventions on self-reported and device-measured physical activity.
Results
Seventeen studies were included in the analysis with 452 subjects in the intervention groups. The random-effect meta-analysis showed a moderate improvement in intervention groups measures in pre-surgery physical activity levels compared to the baseline (SMD = 0.67, [CI = 0.30;1.03], I2 = 79%). The self-reported subgroup meta-analysis showed the largest increase in performed physical activity, (SMD = 0.78, [CI = 0.4;1.15], I2 = 79%) whilst non-significant increase was shown in the device-measured subgroup (SMD = 0.16, [CI = −0.64;0.97], I2 = 58%).
Conclusion
Increasing physical activity in the preoperative phase is feasible. Self-reported physical activity outcome measures show larger effects compared to device-measured outcome measures. More high-quality research should be performed utilizing objective measures.
Introduction
Abdominal resection surgery is indicated for the cure or palliation of numerous cancer types. 1 The surgery itself represents a stress event with an increased risk for adverse effects unrelated to the treatment goals. These adverse effects have a profound negative impact on a person's ability to perform daily activities and may negatively impact postoperative quality of life.2–6 To help cope with the stressors involved with surgery, surgeons recommend patients to avoid inactivity and progress towards reaching at least 150 min of moderate to vigorous intensity physical activity and 2 to 3 moderate intensity resistance exercise sessions per week. 7
The role of physical activity for health is well recognized, with recent publications by the World Cancer Research Fund/American Institute for Cancer Research and the 2020 guidelines by the World Health Organization. 8 These guidelines indicate that more physical activity contributes to optimal health outcomes in both the general population and specific subgroups like elderly and subjects suffering from chronic diseases. 8 Due to its positive effect, there is a high interest in the role of preoperative physical activity to improve postoperative recovery. Evidence shows that a patient's physical activity level during the preoperative phase influences surgery outcomes by altering a person's ability to cope with the stressors of surgery. 9 Namely, lower levels of preoperative physical activity compromise postoperative recovery, leading to an increase in postoperative complication rates10–13 and length of hospital stay,9,14,15 and a decrease in health-related quality of life. 16
Although there are many different methods used to assess physical activity, namely self-monitored physical activity by questionnaire or diary log, or via device measured by motion sensors, reliability of the measurement instruments remains an important field of research. 17 Because of low concurrent validity between the self-reported and the device measured methods, determining the best method is of importance.18,19 The cheapest way of measuring physical activity is the administration of physical activity questionnaires, which can assess all types of physical activity. However, very few physical activity questionnaires show acceptable reliability and validity across age groups,20,21 partly because answers may be distorted due to social desirability or recall bias. 22 Motion sensors, such as pedometers or accelerometers are increasingly implemented as a measure of physical activity in a free-living environment. Accelerometers are small electronic devices that record acceleration associated with bodily movement and provide an objective estimate of duration and intensity of locomotion. 23
An increasing number of preoperative intervention studies, also known as prehabilitation, are performed aiming to increase the physical activity level of patients awaiting an abdominal operation amongst others.24–26 A wide variety of interventions are used, ranging from behavioral strategies to prescribed exercise interventions to increase physical activity. Nevertheless, most studies lack the sample size and homogeneity to establish whether physical activity interventions findings are consistent and can be generalized across patient groups, and treatment variations, or whether findings vary significantly. Therefore, the current meta-analysis aims to determine the effect of physical activity interventions in patients awaiting abdominal resection surgery. Furthermore, our secondary objective is to determine whether self-reported and device measured physical activity outcome measures result in similar outcomes.
Methods
This systematic review is reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement. 27
The databases PubMed and EMBASE were searched for relevant studies (Supplementary material S1). The search strategy used blocks of search terms related to preoperative physical activity amongst major abdominal surgery patients. Terms were added for intervention studies aimed at altering physical activity levels including pre and post intervention measurements. The search was conducted on April 18, 2023 ranging from January 2000 to April 2023. Reference lists of eligible studies were hand-searched as a method to supplement electronic searching.
Results of the searches were combined, whereafter duplicates were removed. All unique records were screened for potential relevance using the title, abstract or descriptors, or both. Hereafter, the corresponding studies were screened on compliance with the eligibility criteria based on the full text of the articles. If not compliant, studies were excluded and reasons for exclusion based on its full text were recorded. Study selection and risk of bias assessment were performed by two reviewers (J.K. and C.M.).
Studies that measured pre- and post-intervention physical activity during the period between diagnosis and abdominal resection surgery were included, all physical activity outcome measures were considered eligible. Furthermore, additional criteria were: written in the English language, clinical trial study designs, and case–control studies. Exclusion criteria were: physical activity requirements in sample selection, conference proceedings, non-peer reviewed papers, opinion pieces, letters to the editor, commentaries, abstracts. Furthermore, studies including cosmetic-, bariatric surgery procedures or nonelective surgery were excluded.
A standardized form was used to extract data from eligible studies for assessment of the study quality and evidence synthesis. Information regarding the following was extracted: participant characteristics (age, gender, body mass index, surgery type or site, American Society of Anaesthesiologists classification, (neo)adjuvant therapy and baseline fitness), and study characteristics (sample size, design). All physical activity measurements were extracted. The method of measuring physical activity was extracted to determine the effect self-monitored versus device physical activity measures. Furthermore, measurements during the last week of an intervention were considered post-intervention measurement. To determine the effect of the interventions, pre- and post-intervention physical activity measurements, time between baseline measurement and post intervention measurement, and time until surgery was extracted. The extracted characteristics of the intervention were content, type, and duration. Since supervised interventions are reported to be more effective in persons with low habitual physical activity levels, interventions were categorized into supervised prescribed interventions and/or behavioral interventions aimed to increase daily living physical activity. 28
The Physiotherapy Evidence Database scale was used to determine the risk of bias of all included studies. 29 This tool is deemed a valid measure of the methodological quality of (randomized) clinical trials. 30 Each study was graded using 11 criteria (a score of one was awarded if the response was ‘Yes’ and zero if the response was ‘No’. A total Physiotherapy Evidence Database scale score of 0–3 is considered ‘poor’, 4–5 ‘fair’, 6–8 ‘good’, and 9–10 ‘excellent’.
All included studies were summarized in tables. Normally distributed data were reported by mean and standard deviation (SD). Otherwise, the median and interquartile range or frequency and percentages were provided. Meta-analyses to determine the pooled effect of physical activity interventions were conducted using R-studio, 31 package Meta for outcomes where mean and SD data were available. 32 If multiple physical activity measures were available, total sum of physical activity was preferred over subcategories (e.g., time spend sedentary, moderate to vigorous physical activity or step count). To allow for the comparison between different measures across studies, within group pre-post changes were calculated by standardized mean difference using Hedges’ adjusted g, which includes a correction for sample size bias. 33 Furthermore, prescribed exercise versus behavioral interventions, and device versus self-monitored measured physical activity subset analyses were performed to increase homogeneity. To determine the effect of methodological quality, similar assessment was performed including studies rated ‘fair’, ‘good’ or ‘excellent’. A Standardized mean difference = 0.0 to 0.2 is considered as a ‘small’ effect size, 0.2 to 0.8 represents a ‘medium’ effect size and >0.8 a ‘large’ effect size. Statistical heterogeneity was assessed by the I2 test, 34 which is based upon the percentage of variability across studies beyond what would be expected by chance. I2 values of 25, 50, and 75 serve as limits for low, moderate, and high heterogeneity, respectively.
Results
Selected Studies
We identified 861 potential unique studies published between January 2000 and April 2023. After initial screening, 153 studies were regarded potentially eligible. After reading the full-text, 17 studies passed all inclusion criteria. The final selection consisted of two non-randomized controlled trials, seven randomized controlled trials, and six single arm intervention trials. Furthermore, 12 studies were considered eligible for inclusion in the meta-analysis. A flowchart displaying details of the selection process, including the reasons for exclusion, is presented in Figure 1.
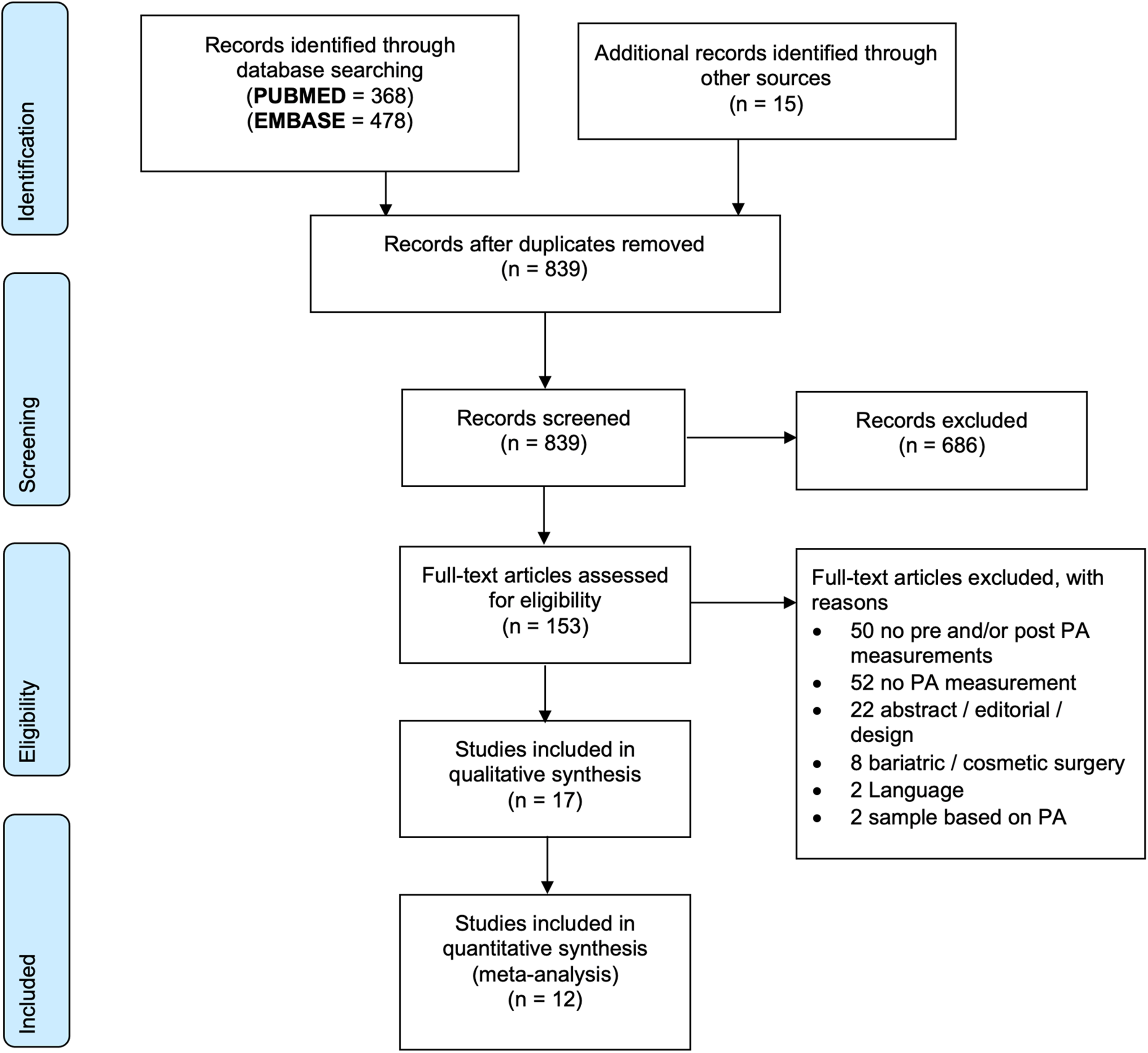
The PRISMA flow diagram displays the selection of studies and reasons for exclusion.
Methodological Quality Assessment
Quality of the included studies varied, and none of the studies fulfilled all eleven quality criteria. An excellent quality score was observed in one study, seven studies received a ‘good’ score, and four studies received a score ‘fair’, and five studies received a ‘poor’ score. On average, randomized controlled trials received higher scores compared to non-randomized trials with 7.1 and 4.4 points, respectively. Due to the nature of the intervention, no study included blinding of participants and allocation concealment for participants. Table 1 provides a detailed overview of the methodological quality of the included studies based on the Physiotherapy Evidence Database scale.
Methodological quality of included studies based on PEDro scale.
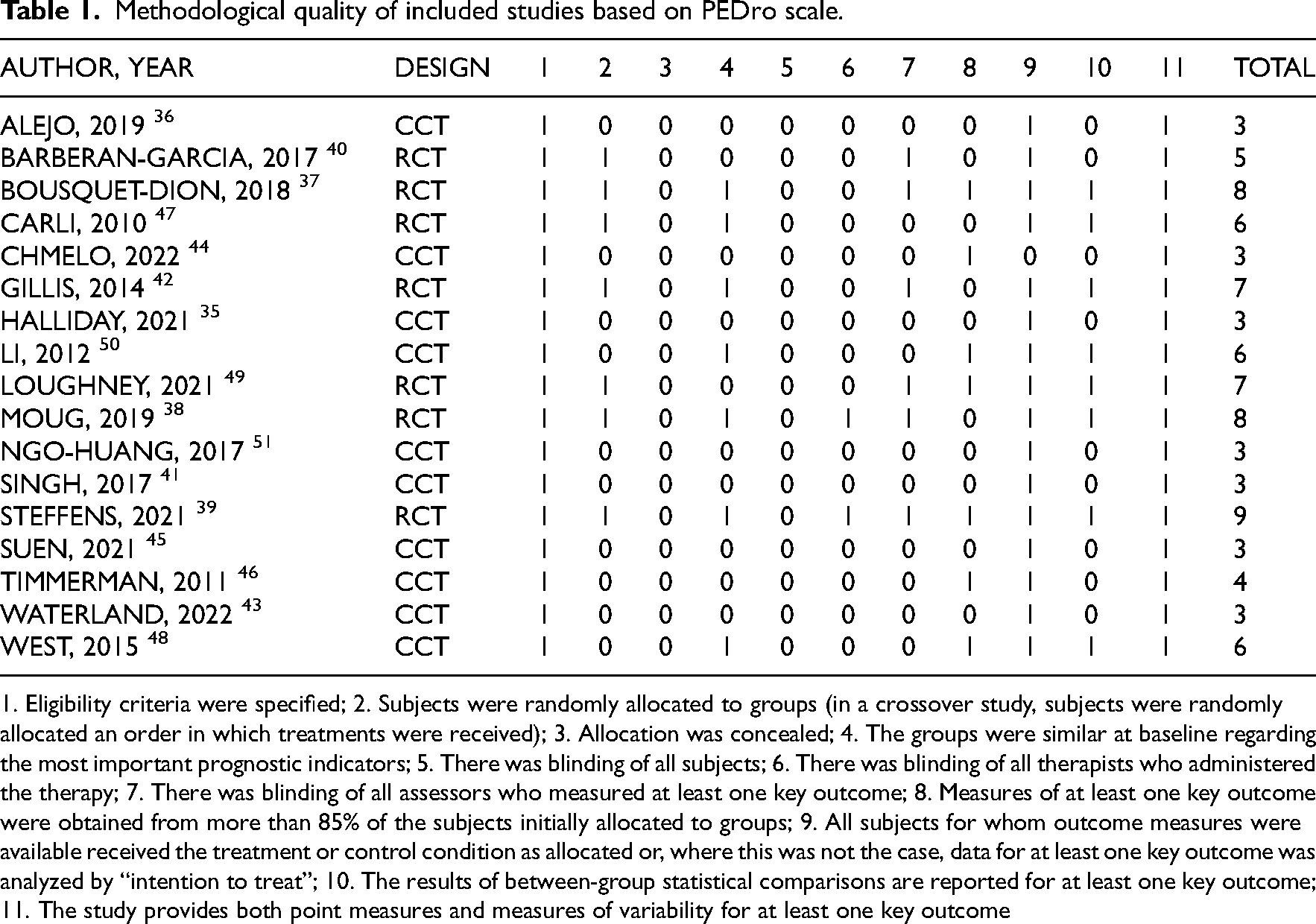
1. Eligibility criteria were specified; 2. Subjects were randomly allocated to groups (in a crossover study, subjects were randomly allocated an order in which treatments were received); 3. Allocation was concealed; 4. The groups were similar at baseline regarding the most important prognostic indicators; 5. There was blinding of all subjects; 6. There was blinding of all therapists who administered the therapy; 7. There was blinding of all assessors who measured at least one key outcome; 8. Measures of at least one key outcome were obtained from more than 85% of the subjects initially allocated to groups; 9. All subjects for whom outcome measures were available received the treatment or control condition as allocated or, where this was not the case, data for at least one key outcome was analyzed by “intention to treat”; 10. The results of between-group statistical comparisons are reported for at least one key outcome; 11. The study provides both point measures and measures of variability for at least one key outcome
Study Characeteristics
Table 2 displays the overall study characteristics. The 17 included studies assessed 856, 261 (30%) female and 513 (60%) male subjects in total, of which were 452 (164 females, 302 males) in intervention and 315 (97 females, 211 males) in control groups. One study did not report the sex distribution. 35 Mean and median age of included subjects ranged between 54.4 and 74 years. Subjects received neoadjuvant chemo- and/or radiotherapy during the intervention in ten studies (58.8%), before the intervention in two studies (11.8%) and no neoadjuvant therapy in five studies (29.4%).
Overall study characteristics.
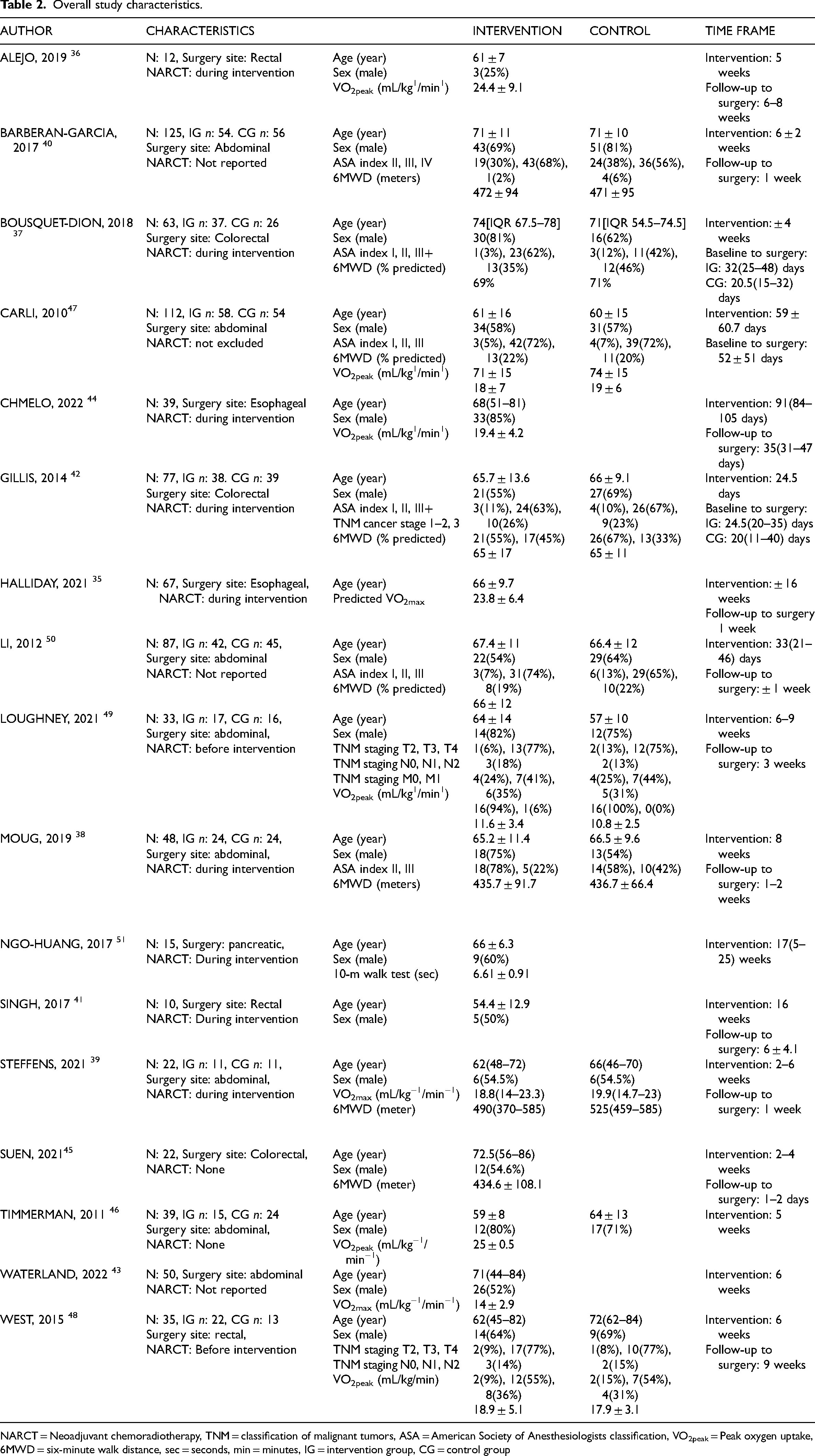
NARCT = Neoadjuvant chemoradiotherapy, TNM = classification of malignant tumors, ASA = American Society of Anesthesiologists classification, VO2peak = Peak oxygen uptake, 6MWD = six-minute walk distance, sec = seconds, min = minutes, IG = intervention group, CG = control group
Intervention
Characteristics of the interventions are reported in Table 3. Six studies used behavioral interventions aimed to increase physical activity.36–41 These interventions consist of a pedometer or a time goal to be physical active, a motivational interview to maintain and/or increase physical activity, or education on the importance of physical activity. All studies used a prescribed exercise scheme to be performed either in hospital-based or home-based intervention to increase physical activity.35–47 Four studies performed solely supervised hospital-based exercise sessions,46,48–50 most studies combined home-based and hospital-based sessions or did not include a statement about the location. The frequency of the exercise sessions ranged from 0.5 to 5 sessions per week and lasted between 10 and 120 min per session. The duration of the interventions ranged from 2 to 16 weeks.
Intervention description.
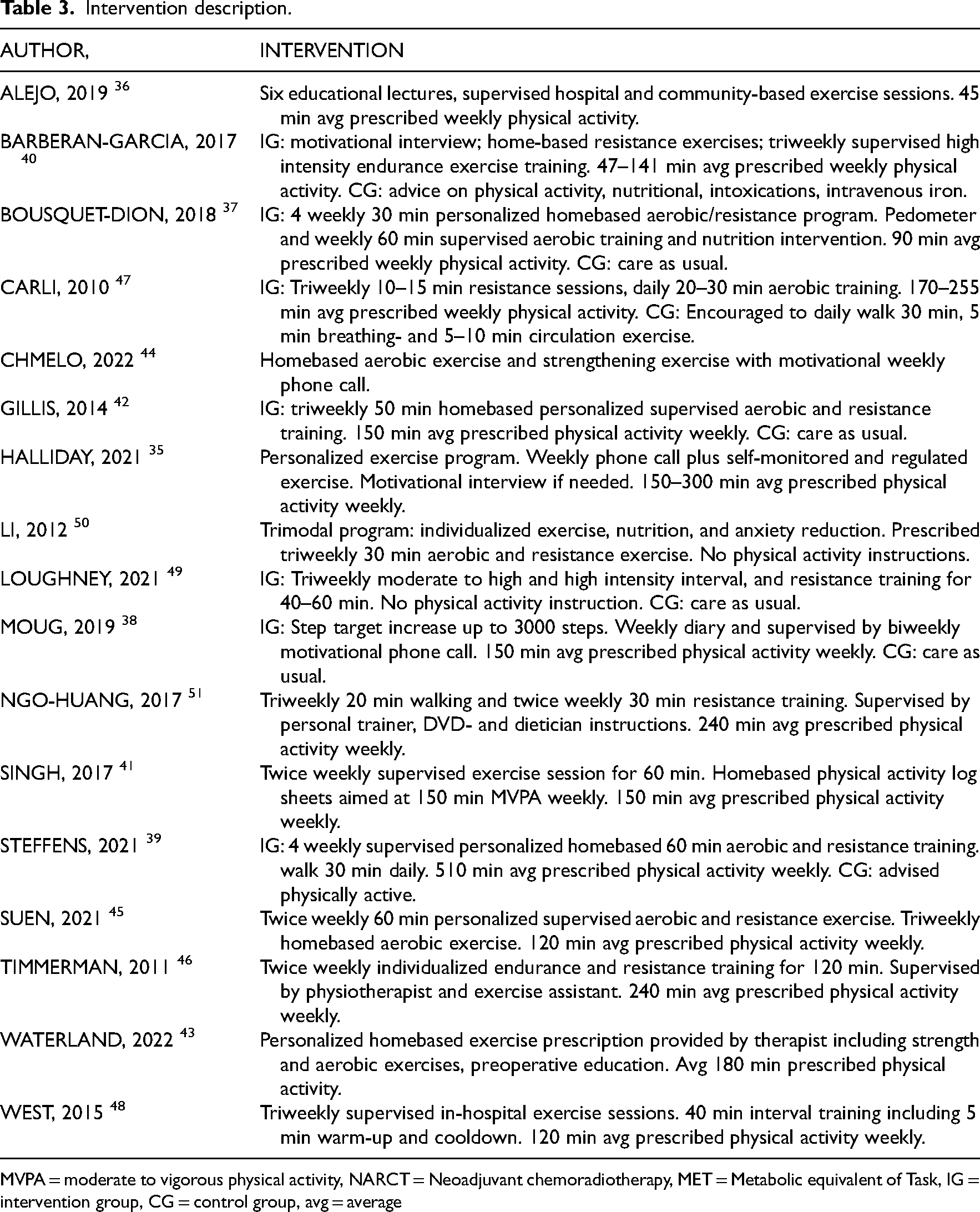
MVPA = moderate to vigorous physical activity, NARCT = Neoadjuvant chemoradiotherapy, MET = Metabolic equivalent of Task, IG = intervention group, CG = control group, avg = average
Physical Activity
Table 4 shows the baseline and pre-operative physical activity measures. Performed physical activity increased in ten out of the thirteen and four out of seven studies for the intervention and control groups, respectively. The random-effect meta-analysis, depicted in Figure 2, showed a moderate improvement in intervention groups compared to the baseline measures; however, high heterogeneity was detected (SMD = 0.67, [CI = 0.30; 1.03], I2 = 79%). Excluding studies of ‘poor’ quality showed no significant increase with an SMD of 0.56 ([CI = −0.11; 1.24] I2: 89%). When comparing baseline and pre-operative physical activity behavior in control groups, see Figure 2, no changes (SMD = 0.03 [CI = −0.18; 0.24] I2 = 0%) were found without heterogeneity.
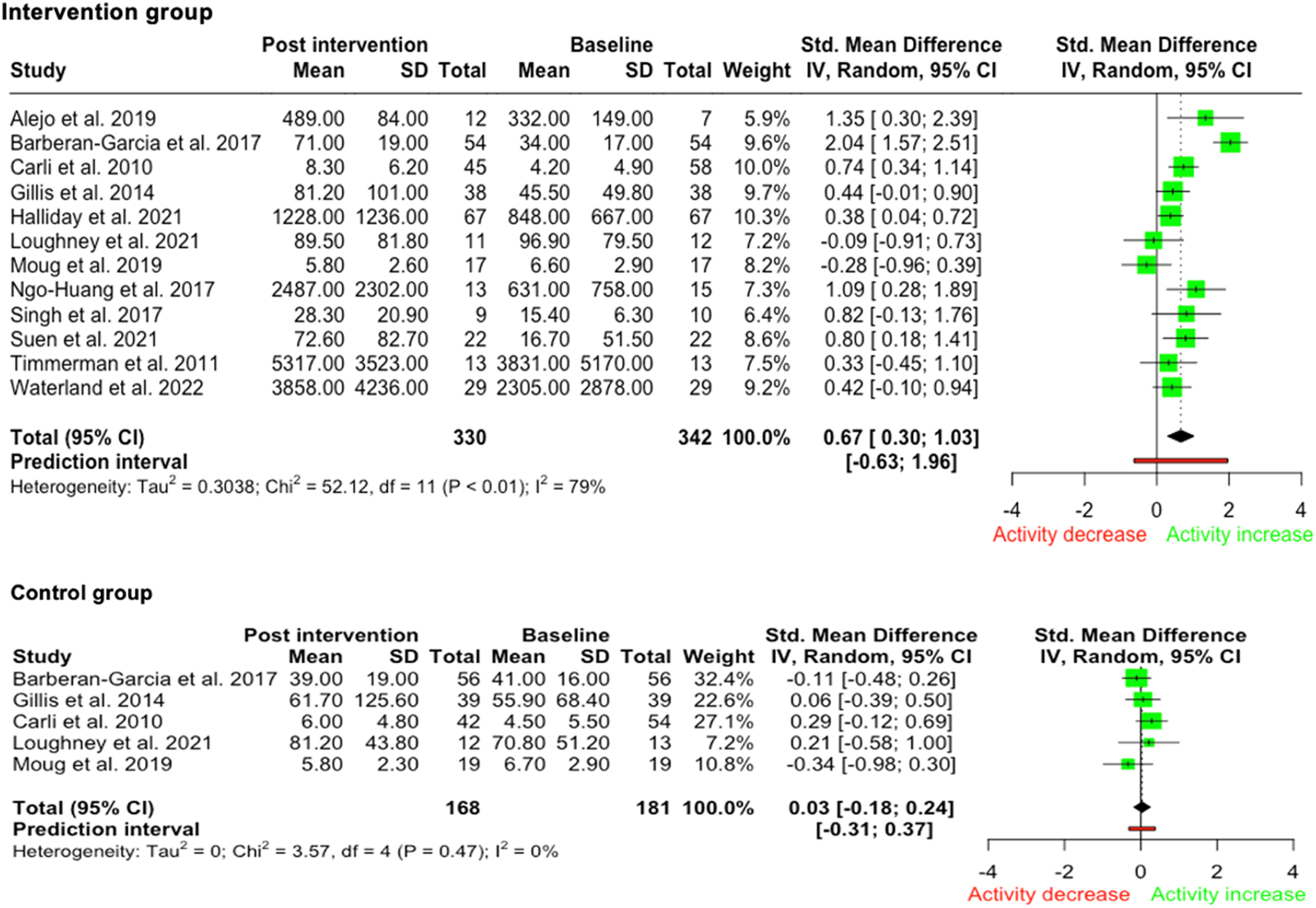
Meta-analysis of baseline and post-intervention physical activity in the intervention and control group. Meta-analysis and forest plot of random effect baseline and post-intervention physical activity in the intervention and control group.
Baseline and pre-operative physical activity measures.
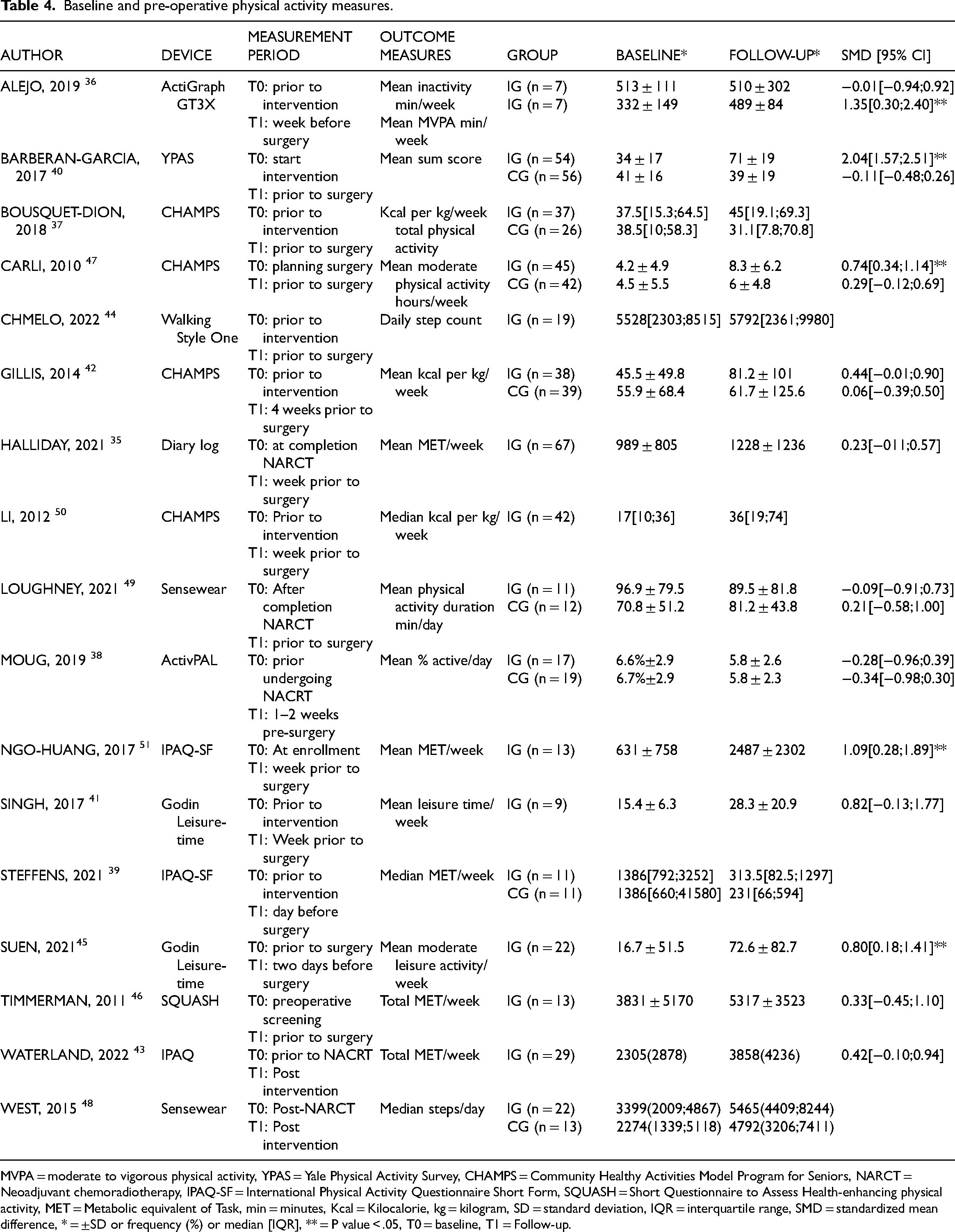
MVPA = moderate to vigorous physical activity, YPAS = Yale Physical Activity Survey, CHAMPS = Community Healthy Activities Model Program for Seniors, NARCT = Neoadjuvant chemoradiotherapy, IPAQ-SF = International Physical Activity Questionnaire Short Form, SQUASH = Short Questionnaire to Assess Health-enhancing physical activity, MET = Metabolic equivalent of Task, min = minutes, Kcal = Kilocalorie, kg = kilogram, SD = standard deviation, IQR = interquartile range, SMD = standardized mean difference, * = ±SD or frequency (%) or median [IQR], ** = P value < .05, T0 = baseline, T1 = Follow-up.
Outcomes
Physical activity performed during the last four weeks37,42,47,50 or the last week of the intervention was used as the measurement period in the majority of the studies.35,36,39–41,45,46,48,51 Twelve studies employed self-report measures of physical activity; the CHAMPS questionnaire was most frequently used.37,42,47,50 Outcomes were either a sum score,
40
hours and/or minutes of physical activity per week37,41,42,45,47 or metabolic equivalent of task (MET) per week.35,39,43,46,51 The intervention arms of the self-report measurement studies reported an increase in physical activity in ten studies,35,37,40–43,45–47,50,51 while three out of seven studies reported increase in physical activity in control groups.42,47,49 Five studies used device measures of physical activity, namely, one reporting on activity bouts, three reporting step counts, and two studies reporting both step counts and activity bouts.36,38,44,48,49 The self-reported intervention subgroup meta-analysis showed a large increase in performed physical activity, notably high statistical heterogeneity was found (SMD = 0.78, [CI = 0.4; 1.15], I2 = 79%), while no significant changes were shown in the device-measured subgroup (SMD = 0.16, [CI = −0.64; 0.97], I2 = 58%) as seen in Figure 3a. Analysis in ‘fair’ to excellent’ quality studies show a SMD 0.61 ([0.31; 0.91], I2: 0%) in self-reported, and a non-significant SMD −0.2 ([−0.73; 0.32] I2: 0%) in device measured physical activity, respectively. Although studies including behavioral interventions yielded a large improvement with a standardized effect of SMD 0.99 ([CI = −0.03; 2.01], I2 = 90%) compared to solely prescribed exercise, namely SMD 0.51 ([CI = 0.33; 0.69], I2 = 1%), these differences in outcome are not statistically significant. Control groups solely receiving advice to maintain
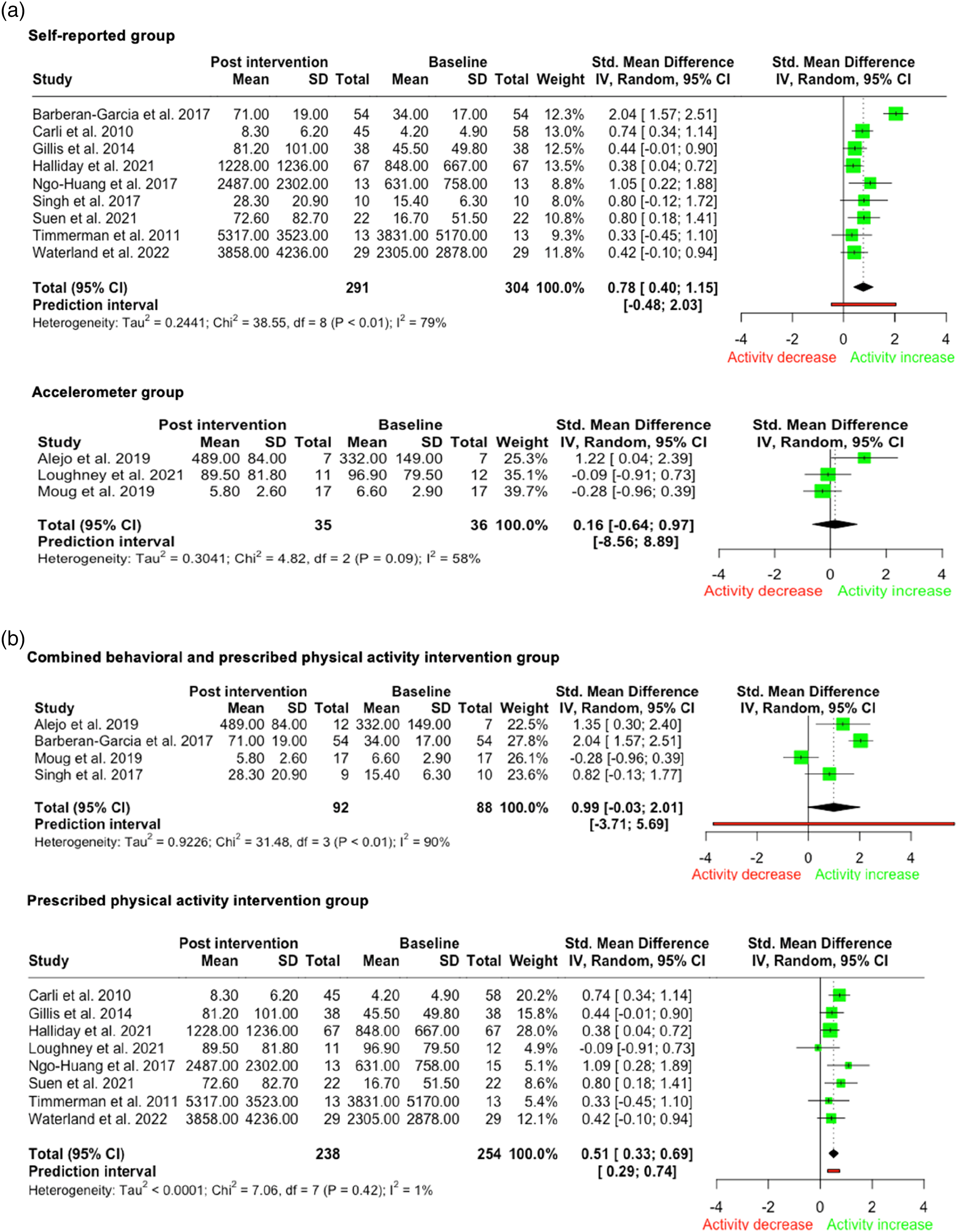
3.a Meta-analysis of effect of measurement method on physical activity. Meta-analysis and forest plot of random effect baseline and post-intervention physical activity in the intervention group measured by self-monitor and accelerometer instruments. Figure 3.b Meta-analysis of effect of intervention type on physical activity. Meta-analysis and forest plot of random effect baseline and post-intervention physical activity in the intervention group receiving behavioral intervention and a prescribed physical activity scheme and the group receiving solely a supervised and/or unsupervised prescribed physical activity scheme.
Discussion
The principal finding of this review was that interventions aimed to increase preoperative physical activity in major abdominal surgery appear to be effective. However, self-reported outcome measures seem to report larger increases in physical activity levels compared to device measures. Nonetheless, too few high-quality studies utilized device measures to determine the effect of measurement instruments. Overall, interventions including a combination of prescribed exercise and behavioral strategies seem to be the most effective way to increase physical activity.
Moderate-sized improvement in physical activity levels was found in intervention groups compared to the baseline measures. Similarly, interventions aimed at increasing physical activity in the healthy and chronically ill adults’ population have been proven to be moderately effective.52–54 In these populations, larger effects are reported when using individually adapted behavioral interventions.52,53 This method, aimed to have participants incorporate physical activity into their daily routines, are more cost-effective when compared with prescribed physical activity interventions in the general population.55,56 However, the brief preoperative window of opportunity to increase physical activity behavior, and the effects of the stress involved with being enlisted for surgery favors an intensive collaboration between patient and healthcare provider. 57 This assumption is supported in the current meta-analysis, which shows that the largest increase was achieved through intensive collaboration in the form of combined of prescribed exercise and behavioral intervention. However, behavioral changes are time consuming. Although patients are likely to be open for behavioral changes to increase their ability to cope with the stressors of surgery during the preoperative period, the available preoperative time is limited to achieve long lasting behavioral changes. 58
Our meta-analysis suggests that studies utilizing device measurement showed a lower or non-significant increase compared to self-monitored questionnaires. This difference may be due to overestimation in the self-monitored group resulting from recall bias.59,60 Thereby, owning an over optimistic version of performed physical activity, may represent a distorted version of reality. This effect might be enlarged by knowing the potential effect of inactivity on surgery outcomes. This knowledge likely increases when subjects participate in an intervention aimed at improving the patient's ability to cope with the stressors of surgery via increased physical activity. Furthermore, participation in an intervention built around physical activity can result in an increased awareness on performed physical activity, duration neglect, and socially desirable answers to please researchers.61,62 However, device measurement instruments are subject to the researcher's analysis and configuration choices, which can affect the reliability of the data. Therefore, to gather reliable information into performed physical activity, device measures should be used, utilizing standardized configurations.
Since homogeneous results were found in the studies using device measurement instruments, the high heterogeneity between studies found in the analysis of the overall effect and in analysis of the different intervention types, might be caused by the application of different measurement instruments. However, the number of studies using device measurement instruments was low. Furthermore, in general, studies with a high therapeutic validity show homogeneous results towards better postoperative outcomes.63,64 Peer-reviewed studies on prehabilitation schemes for major abdominal elective surgery candidates show heterogeneous designs in terms of measurement instruments, duration, and modalities of the intervention. The design of these interventions depends in part on organizational aspects of healthcare providers, like the interval of time before surgical date, availability of healthcare providers and identifying eligible patients as well as by type of surgical intervention. 63 In the current study, designs varied significantly between studies. Nevertheless, most studies showed an increase in physical activity. Notably, the biggest improvement was observed in the study conducted by Barberan-Garcia et al., this trial performed a personalized program including a motivational interview aimed at increasing physical activity, home-based functional training, and supervised endurance training. 40 However, more studies are needed to confirm the effect of this combined intervention.
PubMed and Embase were the chosen database resources for the current study, based on their well-established reputation for providing comprehensive, diverse, and high-quality biomedical literature. Both databases offer broad coverage, unique content, and accessibility, with their use of different indexing systems providing complementary results. The decision to limit the study to these two databases was a deliberate one, made to ensure a rigorous and comprehensive literature review. However, our analyses are limited by the low number of studies included in the selected subgroups. Therefore, the effect of device versus self-reported measurement for each intervention type could not be determined since only a single study performed both a behavioral intervention combined with device measurement. Furthermore, the discrepancy between the device measured, and self-monitored physical activity outcomes limits the generalizability of the overall intervention effects. However, the current meta-analysis provides an up-to-date overview of the effect of prehabilitation literature incorporating interventions aimed to increase physical activity levels in patients awaiting major abdominal surgery. Prehabilitation is a broad term encompassing various interventions with different theoretical underlying mechanisms that have a common goal to improve a person's ability to cope with the stressors of surgery. The ultimate goal is to improve outcomes after surgery, so this is just the first step of the proof of concept that it is possible. Narrowing the focus to a specific area of prehabilitation, physical activity, provided meaningful analysis of the practicalities of the intervention and a clearer understanding of its effectiveness.
In conclusion, increasing physical activity in the preoperative phase is feasible. Self-reported physical activity outcome measures show larger effects compared to device measured physical activity outcome measures. To gather reliable information about performed physical activity, device measures should be used, utilizing standardized configurations.
Clinical messages
Interventions aimed to increase preoperative physical activity in major abdominal surgery appear to be effective. Interventions including a combination of prescribed exercise and behavioral strategies seem to be the most effective to increase physical activity. There is a discrepancy between self-reported outcome measures compared to device measures, self-reported outcome measures seem to report larger increases in physical activity levels.
Supplemental Material
sj-docx-1-cre-10.1177_02692155231202215 - Supplemental material for Changes in Self-Reported and Device-Measured Physical Activity Before Abdominal Resection Surgery: A Meta-Analysis
Supplemental material, sj-docx-1-cre-10.1177_02692155231202215 for Changes in Self-Reported and Device-Measured Physical Activity Before Abdominal Resection Surgery: A Meta-Analysis by Caspar F Mylius, Yvet Mooiweer and Wim P Krijnen, Tim Takken, Barbara C van Munster, Cees P van der Schans, Joost M Klaase in Clinical Rehabilitation
Footnotes
Acknowledgements
Not applicable.
Authors’ Contributions
CM carried out the design of the study, data collection, analysis and drafted the manuscript. YM performed initial search and draft of the manuscript, WK helped to perform and design statistical analysis and draft of the manuscript. TT helped to design the study and draft the manuscript. BvM reviewed the manuscript. CvdS helped in the design of the study and the draft of the manuscript. JK helped in the design of the study, data analysis, and in the draft of the manuscript. The authors read and approved the final manuscript.
Availability of Data and Materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Consent for publication
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
Not applicable.
Funding
The study was supported by the University Medical Centre Groningen, the Netherlands; Utrecht University, the Netherlands; and the Hanze University of Applied Sciences Groningen, the Netherlands.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.