
Abstract
Objective
This systematic review and meta-analysis aimed to analyze the published randomized controlled trials (RCTs) that investigated the effects of exercise interventions on functioning and health-related quality of life following hospital discharge for recovery from critical illness.
Design
Systematic review and meta-analysis of RCTs.
Data sources
We searched PubMed/MEDLINE, Cochrane Central Register of Controlled Trials, PEDro data base, and SciELO (from the earliest date available to January 2023) for RCTs that evaluated the effects of physical rehabilitation interventions following hospital discharge for recovery from critical illness.
Review methods
Study quality was evaluated using the PEDro Scale. Mean differences (MDs), standard MDs (SMD), and 95% confidence intervals (CIs) were calculated.
Results
Fourteen studies met the study criteria, including 1259 patients. Exercise interventions improved aerobic capacity SMD 0.2 (95% CI: 0.03–0.3, I2 = 0% N = 880, nine studies, high-quality evidence), and physical component score of health-related quality of life MD 3.3 (95% CI: 1.0–5.6, I2 = 57%, six studies N = 669, moderate-quality evidence). In addition, a significant reduction in depression was observed MD −1.4 (95% CI: −2.7 to −0.1, I2 = 0% N = 148, three studies, moderate-quality evidence). No serious adverse events were reported.
Conclusion
Exercise intervention was associated with improvement of aerobic capacity, depression, and physical component score of health-related quality of life after hospital discharge for survivors of critical illness.
Background
With the improved survival of critical care patients, the prevalence of impairment and disability among survivors of critical illness has significantly increased. 1 Skeletal muscle wasting and weakness and impaired physical functioning are key disabilities, which impact on a social participation and patient's return to work. 2 In addition, these muscle impairments are major complications of critical illness and underlie the profound physical and functional disabilities experienced by survivors after discharge. 3 Thus, these survivors frequently have substantial morbidity after hospital discharge, including physical, cognitive, and mental health impairments.2–5 In this context, these patients often require treatments following hospital discharge.
Physical rehabilitation is the cornerstone of management of post critical illness morbidity, and exercise rehabilitation interventions are advocated to target physical and functional disability.3,4 Physical rehabilitation interventions performed in ICU also aims to primarily ameliorate the effects of muscle weakness and physical function deficits in survivors of critical illness following ICU discharge. 6 While several studies have examined physical rehabilitation interventions as exercise-based active or passive mobilization delivered to critically ill patients in the ICU,5,7 some have evaluated the effects of interventions initiated after ICU discharge, and other after hospital discharge. 8
Recent studies in exercise interventions post ICU discharge and other have investigated it effects performed in ward and are continued after hospital discharge. 8 Exercise-based active or passive mobilization delivered to critically ill patients has been shown to result in significant improvement in muscle strength, physical function, length ICU stay, and duration of mechanical ventilation.5,7 Although there are data to support the use of exercise interventions to address physical and functional disabilities within the ICU 7 and after transfer to the ward8,9 the clinical benefit beyond hospital discharge is controversial, and therefore, the delivery of such a service has been inconsistent. 10 In addition, there remains limited evidence to support rehabilitation following discharge from hospital for patients who survive critical illness. Moreover, as far as we know, there is no published meta-analysis on the effects of exercise Interventions following hospital discharge for recovery from critical illness.
The aim of this systematic review with meta-analysis was to analyze the published randomized controlled trials (RCTs) that investigated the effects of exercise interventions on functioning and health-related quality of life following hospital discharge for recovery from critical illness.
Methods
This systematic review (PROSPERO: CRD42022300724) was reported in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 11
Eligibility criteria
This systematic review included RCTs that studied the effects of exercise Interventions following hospital discharge for recovery from critical illness. According to previous systematic review, 10 we consider critical illness as patients admitted to the ICU, irrespective of causal diagnosis but requiring invasive mechanical ventilation and multiorgan support. For this systematic review, exercise Interventions was defined as exercise and/or passive or active mobility program, use of cycle ergometers involving upper or lower limb pedaling at set levels of intensity, or the application of external adjuncts to enable activation of the muscle in patients unable to actively participate in rehabilitation. 10
Studies were eligible for this systematic review if they met the following criteria: (a) included adult patients (aged ≥18 years) following hospital discharge for recovery from critical illness; (b) a RCT trial design; (c) Exercise Interventions controlled by placebo, no exercise, or other interventions; (d) The outcomes of interest were classified in two health outcomes, namely, functioning (muscle strength, aerobic capacity, balance, mobility, and gait) according to The International Classification of Functioning, Disability and Health, anxiety and depression, and health-related quality of life. Studies with post COVID-19 patients were excluded.
Search methods for identification of studies
We searched for references on MEDLINE/PubMed, EMBASE, PEDro, SciELO, and The Cochrane Central Register of Controlled Trials (CENTRAL) up to January 2023 without language restrictions. We used a standard protocol for this search and, whenever possible, a controlled vocabulary (Mesh term for PubMed and Cochrane, Emtree for EMBASE). In search strategy, we used three groups of keywords and their synonymous: study design, participants, and interventions.
The strategy developed by Higgins and Green 12 was used for the identification of RCTs in PubMed. To identify the RCTs in EMBASE, a search strategy using similar terms was adopted. To identify the RCTs in other database, we adopted a search strategy using similar terms. We checked the references of the articles included in this systematic review to identify other potentially eligible studies. The search strategy for MEDLINE via PubMed, Cochrane library, and EMBASE are presented in Supplemental Material 1.
Data collection and analysis
Titles and abstracts were independently checked by two reviewers. If at least one of the reviewers considered one reference eligible, the full text was obtained for complete assessment. Then, two reviewers independently assessed the full text of selected articles to verify if they met the criteria for inclusion or exclusion. Two authors independently extracted data from the published reports using standard data extraction forms adapted from Higgins and Green. 12
All studies selected from the databases were exported in an appropriate file. The software EndNote X7.8 (Clarivate, Philadelphia, PA) was used for analysis of eligibility criteria and duplicate analysis. Then, the exported files were also added to the Rayyan Software for evaluation, selection, and data extraction independently by two researchers. Aspects of the study population, intervention performed, follow-up period and rates of missing data, outcome measures, and results were reviewed.
Methodological quality
The quality of RCTs included was scored by two authors using the PEDro scale, which is based on important criteria, such as random allocation, concealed allocation, intention-to-treat analysis, and the point estimates and variability. These characteristics make the PEDro scale a useful tool for assessing the quality of physical rehabilitation RCTs.13,14 Any disagreements in the rating of the studies were resolved by a third reviewer.
Statistical assessment
Pooled-effect estimates were obtained by comparing the least square mean change from baseline to endpoint for each group and were expressed as the weighted mean difference (MD) between groups. Thus, the [post (-) preintervention] changes in the outcomes were extracted from each study and expressed as mean ± standard deviation (SD). Data were reported as MD, standard MDs (SMD), and 95% confidence interval (CI). For continuous variables, results were expressed as the MD in the change in the variable between randomized groups. Conversion of nonparametric data to means and SD was based on recently established methods. 15 When the SD of change was not available, but CI was available, we converted to SD as guidance by Higgins and Green. 12 If the trial was a multiple-arm RCT, all relevant experimental intervention groups had data extracted. In follow-up reports with multiple end points, only data closest to the end of the physical rehabilitation intervention program were included. Heterogeneity among studies was examined with Cochran's Q and I2 statistic, in which values greater than 40% were considered indicative of high heterogeneity. 16 Analyses were performed with Review Manager (Version 5.4). 17
Summary of findings table
The certainty of evidence for the outcomes in meta-analysis was assessed using the GRADE approach. 12 The assessment involved five items: risk of bias, imprecision, inconsistency, indirectness, and publication bias. Decisions to downgrade were justified using footnotes and making comments, where necessary, to aid readers’ understanding of the review. 12
Results
Description of selected studies
The initial search led to the identification of 3269 abstracts, from which 18 studies were considered as potentially relevant and were retrieved for detailed analysis. Fifteen articles18–32 met the eligibility criteria. Of these, two articles18,19 were duplicates (studies that considered the same participants). The study by Turunen et al. 18 used the same participants as the study by Turunen et al. 19 These two articles were considered as a single study. Finally, 14 studies were considered for analysis.19–32 Supplemental Material 2 shows the PRISMA flow diagram of studies in this review. All studies were scored using the PEDro scale. The results of the assessment of the PEDro scale are presented individually in Supplemental Material 3.
Study characteristics
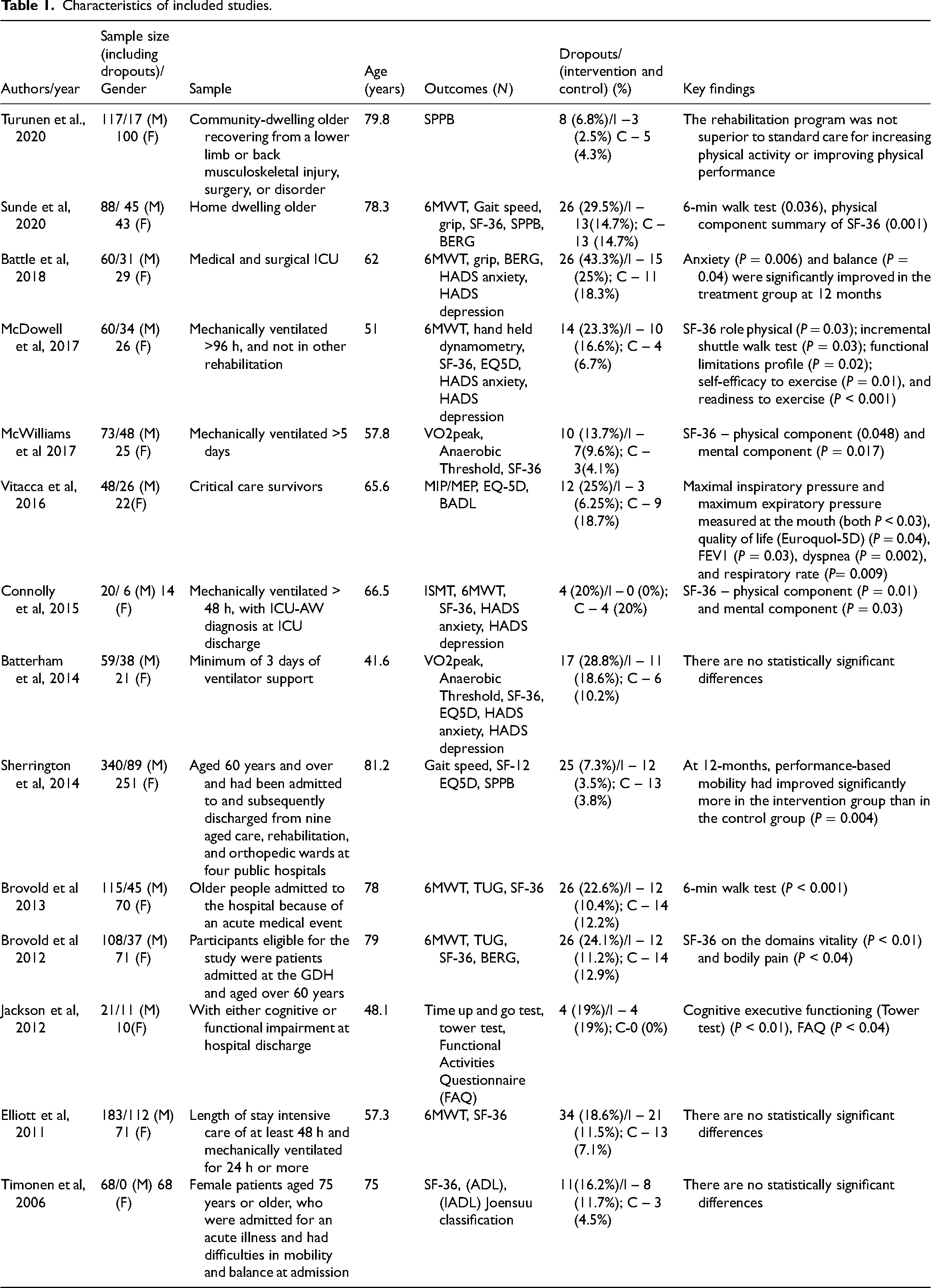
The number of participants randomized ranged from 20 to 312. The mean 12 studies included patients of both genders, one study 32 included only women. Sample size, outcomes, and results of included studies are summarized in Table 1.
Characteristics of included studies.
Characteristics of intervention programs
The characteristics of the exercise interventions have been reported in most studies (Supplemental Material 4).
Aerobic capacity
Nine studies20–23,25–27,29,31 assessed aerobic capacity as outcome. The total number of patients in the exercise group was 394, whereas 399 patients were included in the usual care group. Because of the different instruments used in the measurement of aerobic capacity (6-min walk test, cardiopulmonary exercise testing, and Step Test), a meta-analysis with SMD was used. The meta-analyses showed (Figure 1(a)) a significant difference on aerobic capacity SMD of 0.2 (95% CI: 0.03–0.3, I2 = 0% N = 880, nine studies, high-quality evidence, Table 2) for participants in the exercise group compared with usual care group.
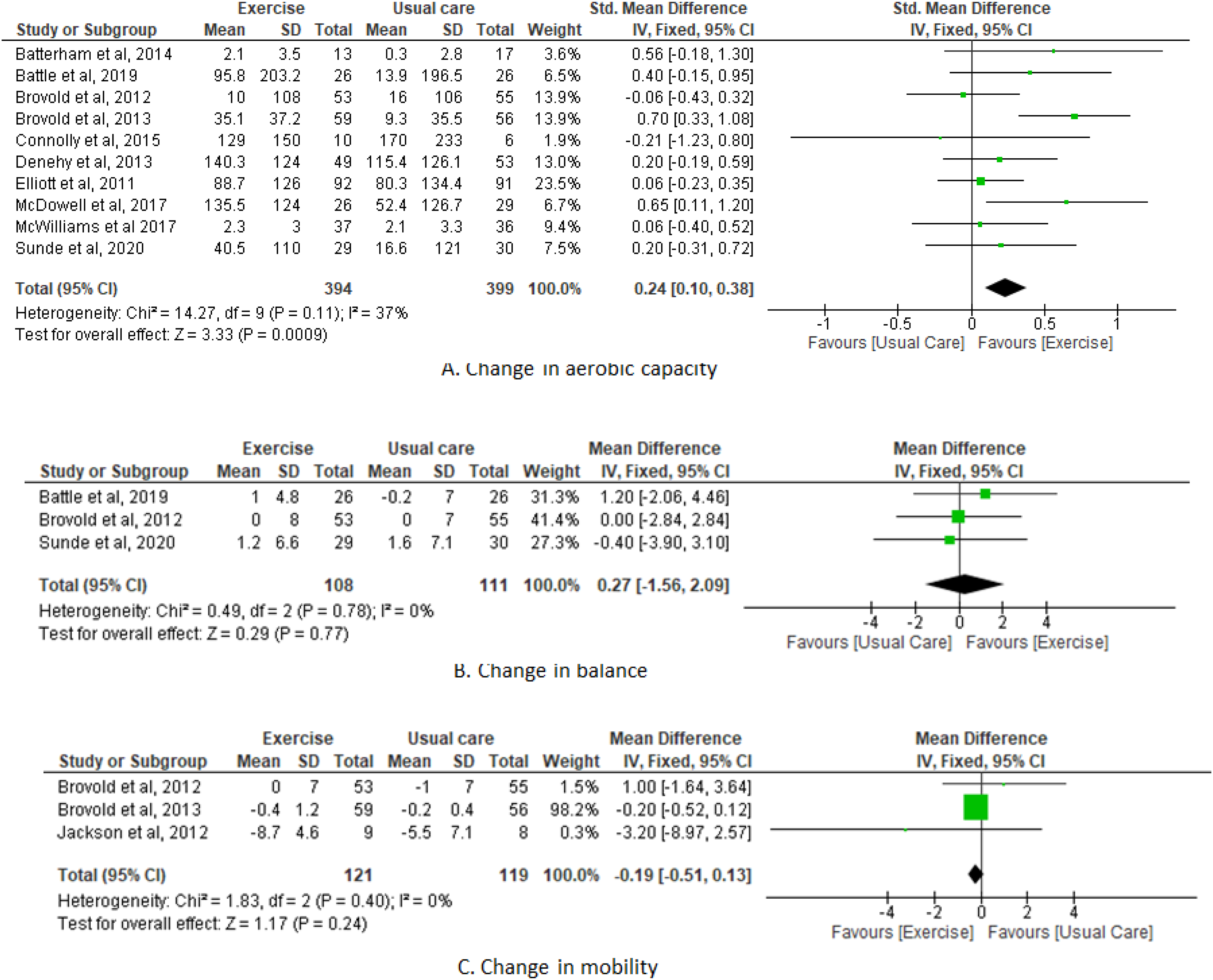
Exercise interventions versus control.
Exercise compared to UC for [hospital discharge].
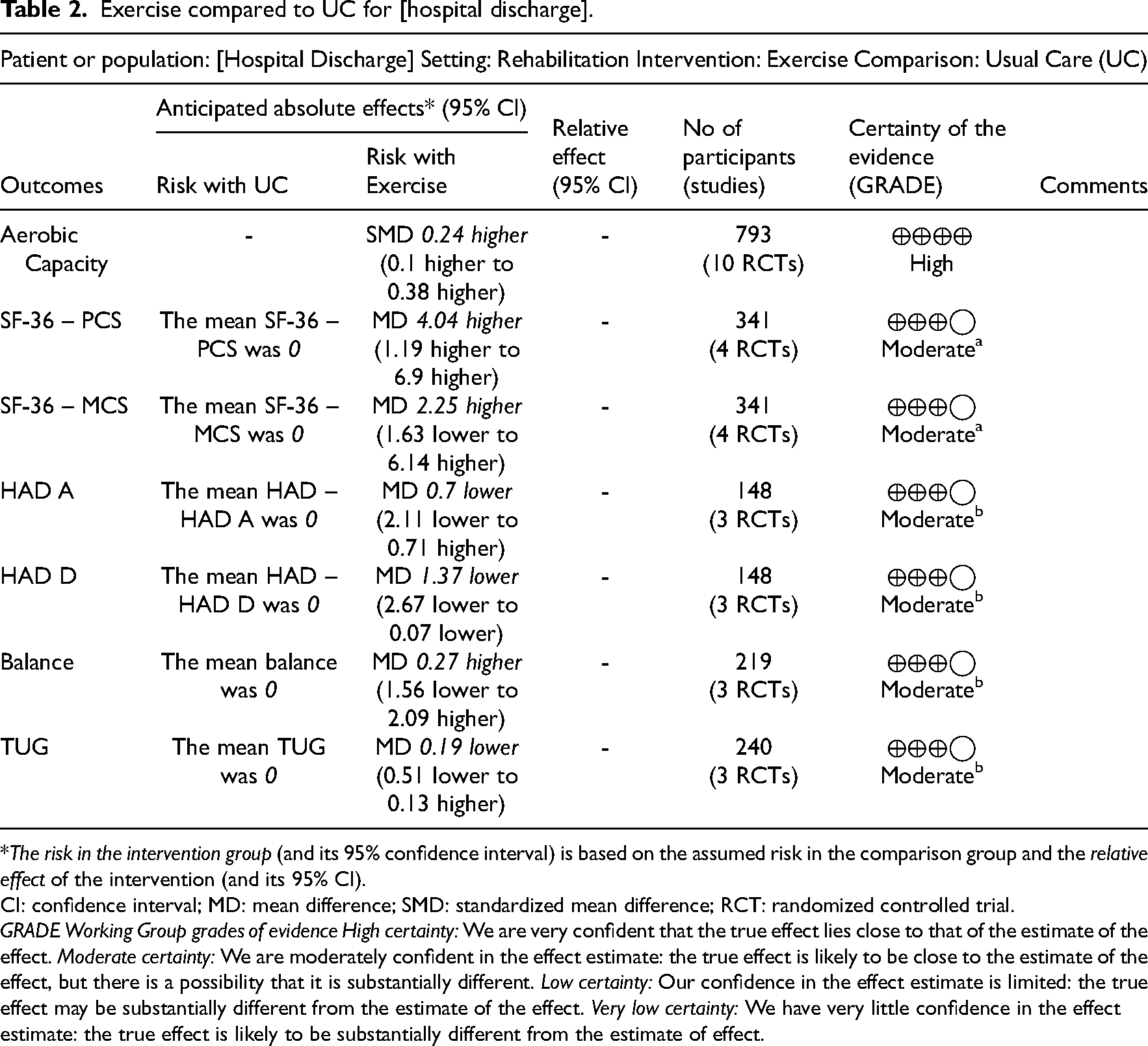
*The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).
CI: confidence interval; MD: mean difference; SMD: standardized mean difference; RCT: randomized controlled trial.
GRADE Working Group grades of evidence High certainty: We are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: We are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: Our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low certainty: We have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect.
Balance
Three studies20,21,29 assessed balance as outcome. The total number of patients in the exercise group was 108, whereas 111 patients were included in the usual care group. Balance was assessed through Berg Balance Scale. The meta-analyses showed (Figure 1(b)) a nonsignificant difference on balance MD of 0.3 (95% CI: −1.6 to 2.1, I2 = 0% N = 219, three studies, moderate-quality evidence, downgraded for imprecision, Table 2) for participants in the exercise group compared with usual care group.
Mobility
Three studies28–30 evaluated mobility. Mobility was assessed through Timed Up and Go Test. The total number of patients in the exercise group was 62, whereas 63 patients were included in the usual care group. The meta-analyses showed (Figure 1(c)) a nonsignificant difference on mobility MD of −0.2 (95% CI: −0.5 to 0.1, I2 = 0% N = 240, two studies, moderate-quality evidence, downgraded for imprecision, Table 2) for participants in the exercise group compared with usual care group.
Anxiety and depression
Four studies21,22,25,26 evaluated anxiety and depression. Anxiety and depression were assessed through Hospital Anxiety and Depression Scale.
Anxiety
The total number of patients in the exercise group was 80, whereas 84 patients were included in the usual care group. The meta-analyses showed (Figure 2) a nonsignificant difference on anxiety of −0.7 (95% CI: −2.1 to 0.7, I2 = 0% N = 164, four studies, moderate-quality evidence, downgraded for imprecision, Table 2) for participants in the exercise group compared with usual care group.
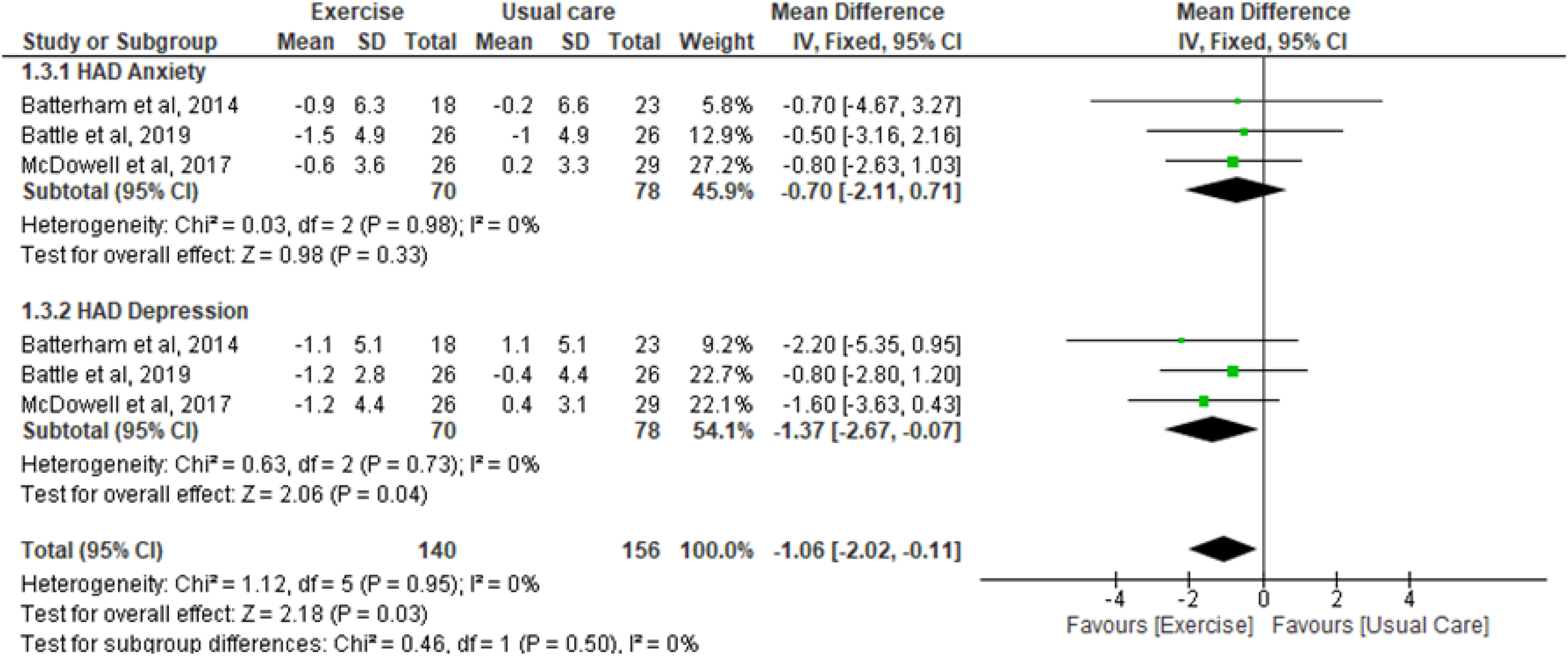
Change in anxiety and depression–exercise interventions versus control.
Depression
The total number of patients in the exercise group was 70, whereas 78 patients were included in the usual care group. The meta-analyses showed (Figure 2) a significant difference on depression of −1.4 (95% CI: −2.7 to −0.1, I2 = 0% N = 148, three studies, moderate-quality evidence, downgraded for imprecision, Table 2) for participants in the exercise group compared with usual care group.
Health-related quality of life
Six studies20,22,23,25,27,31 assessed health-related quality of life. Five studies assessed by Medical Outcome Study Short Form-36 questionnaire, and one study assessed by SF-12 Version 2. 27 Results are represented as a physical component score (PCS) and a mental component score (MCS). The total number of patients in the exercise group was 331, whereas 338 patients were included in the usual care group for both components.
Physical Component Score
The meta-analyses showed (Figure 3) a significant difference in PCS of 3.3 (95% CI: 1.0–5.6, I2 = 57%, six studies N = 669, moderate-quality evidence, downgraded for consistency of effect, Table 2) for participants in the exercise group compared with usual care group.
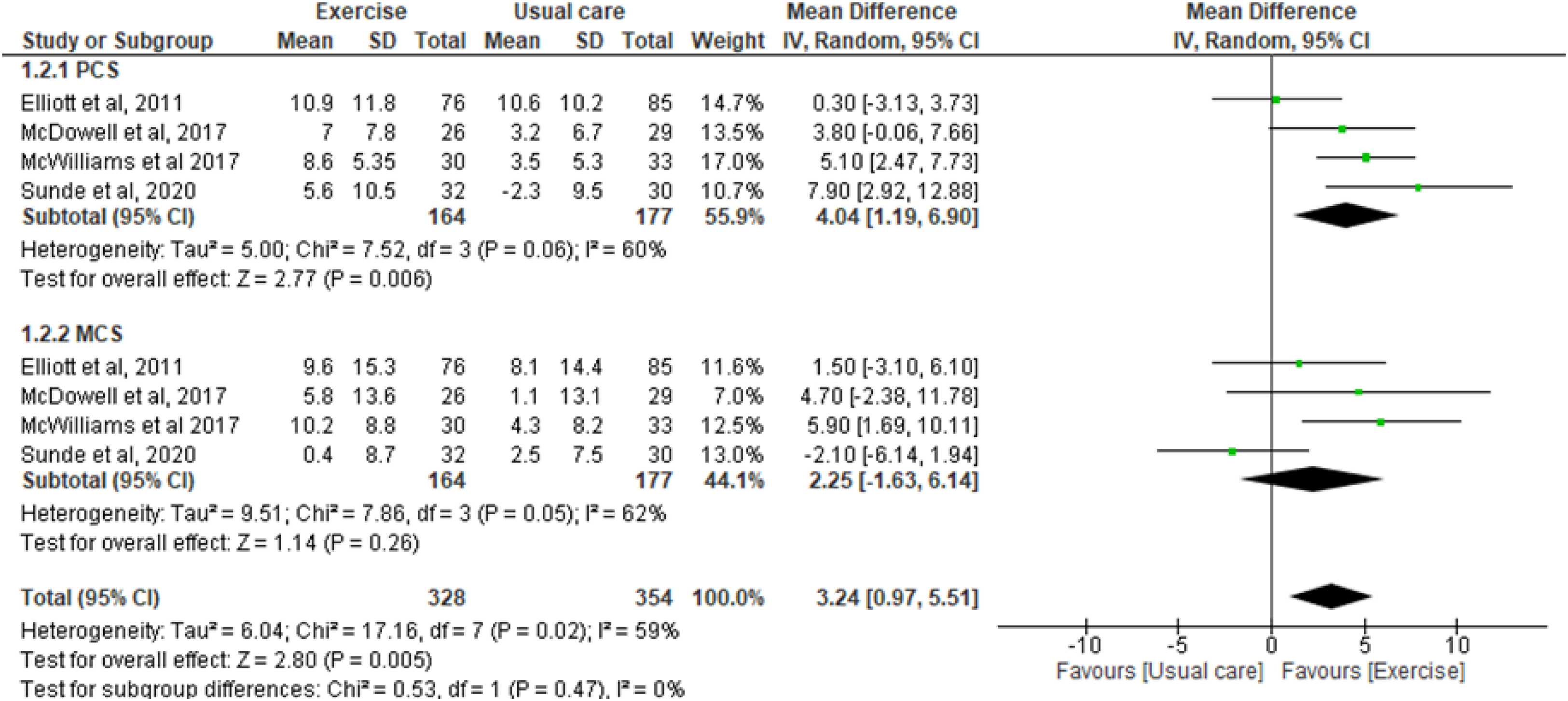
Change in health-related quality of life–exercise interventions versus control.
Mental Component Score
The meta-analyses showed (Figure 3) a nonsignificant difference in MCS of 2.4 (95% CI: −1.3 to 6.1, I2 = 47%, six studies N = 669, moderate-quality evidence, downgraded for consistency of effect, Table 2) for participants in the exercise group compared with usual care group.
Discussion
Our systematic review showed that exercise interventions was associated with improvement of aerobic capacity, and PCS of health-related quality of life after hospital discharge for survivors of critical illness. In addition, a significant reduction in depression was observed. Rehabilitation for survivors of critical illness is increasingly recognized as a vital component in the management of post intensive care syndrome. Exercise-based interventions target the physical functional impairment evident in these patients, which persists long after ICU discharge.8,10
The strength of this systematic review is the comprehensive search developed by a multidisciplinary team and adherence to best practice methodological guidance. Of note, these results of the meta-analyses were based on evidence that can be considered, on average, of high quality (i.e., PEDro score ≥ 6 for all meta-analyzed outcomes). Moreover, the outcomes included considered in our analysis are related to prognosis chronic disease and hospitalized patients. Another novelty of this systematic review is the addition of anxiety, depression, and health-related quality of life as important outcomes.
One of the main consequences of critical illness is skeletal muscle loss and wasting, which is the cause and underlie the profound physical and functional impairments experienced by survivors after discharge from the ICU. 3 Physical rehabilitation during ICU stays has been extensively studied, with evidence in favor of its use in clinical practice. 10 However, its effectiveness when started after hospital discharge is little studied and applied in clinical practice. Therefore, this systematic review presents the available evidence regarding the use of exercises interventions applied after hospital discharge. In this way, we identified the studies that tested their efficacy and observed a positive effect on physical dysfunction, suggesting that their use may be a therapeutic option to restore or maximize physical dysfunction in these patients.
McPeake et al. 33 published a study with the aim of understand the impact of a critical care admission on long-term outcomes, compared to other hospitalized patients without a critical care encounter. They found a significant difference in emotional and social outcomes for critical care and noncritical care hospitalized participants. Patients exposed to critical care were more likely to experience mental health issues such as depression and social isolation following discharge from hospital. Further, it has shown that physical, social, and emotional problems are interrelated. Patients exposed to critical care were more likely to experience mental health issues such as depression and social isolation following discharge from hospital. Further, it has shown that physical, social, and emotional problems are interrelated. 33 In this way, our findings also suggest a reduction in depression, which could favor recovery.
Studies have shown significant and long-lasting physical, psychological, and socioeconomic problems in survivors of critical illness, all of which contribute to a reduced health-related quality of life.23,34 In addition, hospitalization is followed by a frequently irreversible decline in functional status and health-related quality of life.35–37 Another important aspect to note is that the hospitalization demonstrably exacerbates patients’ emotions and increases feelings of depression and anxiety. 37 Our meta-analysis showed additional improvement in the PCS associated with the quality of life. The eligibility of quality of life as the outcome in this systematic review is important because it is an essential component in a rehabilitation program and is an important outcome in studies involving exercise training.
Despite the findings, the result of this systematic review is limited by variance in exercise protocols (variable intensities and different durations of the exercise programs). Moreover, given that this evidence is from moderate-quality evidence, the interpretation should be analyzed with caution. In addition, patients and therapists were not blinded in any of the included studies. Thus, our results should be viewed considering the considerable variation in the exercise program, and of the small number of included studies, although this ultimately reflects the body of evidence about the effects of exercise interventions on functioning and health-related quality of life following hospital discharge for recovery from critical illness.
Taking in account the available studies, this systematic review with meta-analysis showed that exercise interventions performed after hospital discharge for survivors of critical illness was associated with improvement of aerobic capacity, depression, and PCS of health-related quality and should be considered as a component of care of survivors of critical illness after hospital discharge.
Exercise interventions improve aerobic capacity, and physical component score of health-related quality of life of survivors of critical illness. Exercise interventions should be considered as a component of care after hospital discharge.Clinical messages
Supplemental Material
sj-docx-1-cre-10.1177_02692155241241665 - Supplemental material for Effects of exercise interventions on functioning and health-related quality of life following hospital discharge for recovery from critical illness: A systematic review and meta-analysis of randomized trials
Supplemental material, sj-docx-1-cre-10.1177_02692155241241665 for Effects of exercise interventions on functioning and health-related quality of life following hospital discharge for recovery from critical illness: A systematic review and meta-analysis of randomized trials by Bianca Bigogno Reis Cazeta, Rodrigo Santos de Queiroz, Tais Silva Nacimento, Beatriz Reis Ferreira, Micheli Bernardone Saquetto, Bruno Prata Martinez, Vitor Oliveira Carvalho and Mansueto Gomes-Neto in Clinical Rehabilitation
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.