
Abstract
Objective
To explore post-stroke body image experience and enhance understanding of its impacts on wellbeing and recovery.
Design
Cross-sectional qualitative semi-structured interview study with an interpretative phenomenological approach.
Setting
Interviews conducted in participants’ homes, using video-calls, telephone or in-person.
Participants
People treated for acute stroke at two UK hospitals were identified at six months post-stroke and purposively sampled for diversity. Participants were 22 adults (55% male), on average 6.3 months post-stroke and aged 48 to 82 years (median 66 years).
Results
Two main themes were identified: (1) ‘Body now perceived as an ‘obstacle’ to normality’, comprising three subthemes around altered trust in the body, outward presentation of body image and the likening of body image to that of an older person and; (2) ‘Responses to a new body image experience’, comprising five subthemes around the importance of body image, societal pressures, acceptance/adjustment to a changed body image and positivity through experiencing improvements towards a perceived ‘normal’ body image.
Conclusions
Regaining perceived pre-stroke ‘normal’ body image and ability to adjust to a new one is reported as important in recovery. We have demonstrated negative changes in body image experience, and it is possible this is a normal part of post-stroke adjustment. Further research is required to determine whether body image experience can be positively influenced by brief interventions such as guided self-help or psychological support to ensure that they do not persist long term.
Introduction
The body can be viewed as the vehicle through which we experience the world. 1 Temporary or permanent bodily changes caused by stroke can change how body image is experienced.2–3 Body image can be defined as an individual's perceptions, thoughts and cognitions, feelings and affect, and behaviour in relation to the body's appearance, functions and capabilities.4–5 Body image is subjective and hence complex and difficult to define, resulting in a lack of consensus around its definition and how it is experienced after stroke. 6 Its impact on adjusting and recovering after stroke is rarely considered. 2
Perceiving negative post-stroke body image changes can: be linked to depression, reduce self-confidence/esteem, create concerns about the opinions of others, and lead to embarrassment and social withdrawal.3,6–8 This may limit engagement in social relationships, return to paid work and caregiving. 6 Therefore, negative post-stroke changes in body image experience could have implications for life after stroke and may require long-term psychological support. 6 We aimed to explore subjective experiences of post-stroke body image and their perceived impact on recovery.
Methods
In this cross-sectional qualitative study, we used the lens of Phenomenology and an Interpretative Phenomenological Analysis (IPA) approach to provide insights into how people make sense of their personal lived experiences.9,10 We explored the experiences of each participant, before using cross-participant analysis to derive the themes and subthemes from the data. In this respect, phenomenology was used as a touchstone, influencing the interpretation of the data, but not as the only approach. A cognitive behavioural perspective was used for data interpretation,4–5 as the approach lent itself to providing a structure to help interpret and explain participant's experiences. For example, aspects of the approach including cultural socialisation, interpersonal experiences, and physical characteristics were identified during analysis as best explaining participant's experiences.
We recruited participants from two National Health Service (NHS) sites in Northwest England. A purposive sampling strategy was used to monitor under-represented demographics (including people from different ethnic backgrounds and of different ages) and stroke-related characteristics (including stroke severity). Participants were recruited between June 2021 and March 2022. Ethical approval was granted by the Wales Research Ethics Committee 4 Wrexham on 30 November 2020 (REC Reference: 20/WA/0305). Written and verbal informed consent was provided by all participants.
Participants were adults with ischaemic or haemorrhagic stroke; who had recently attended their six-month post-stroke review; and were able to provide informed consent. People with communication impairment were not excluded if they were able to provide consent and participate with supportive communication strategies. People with subarachnoid haemorrhage were excluded due to subarachnoid haemorrhage having a different aetiology, prognosis, and management to other types of stroke. 11 People with a life-threatening/terminal illness were also excluded. Site staff completed screening logs to ascertain numbers of those people who were eligible, and who declined to participate, and reasons for ineligibility. Recruitment was closed when data saturation was reached.
CD conducted all interviews. CD is a female early career researcher, trained in qualitative interview techniques, with a background in psychology and with specific interest in the social experiences of body image. Prior to the interviews, CD and participants were not known to each other. CD collected demographic and stroke-related information, and details about current function (modified Rankin Scale, 12 modified Barthel Index 13 ) and mood (Patient Health Questionnaire PHQ-9, 14 and Generalised Anxiety Disorder GAD-7 13 ) in a separate session ahead of the interview.
To align with the IPA approach, CD used a piloted semi-structured interview. 15 All interviews but one (which was conducted in-person) were conducted via telephone or video call and audio recorded. CD completed a reflective diary immediately after completion of each interview. Recordings were transcribed verbatim and anonymised.
CD inductively derived themes using hand-coding and NVivo (version 1.5.1). CD analysed transcripts individually (case-by-case analysis) looking for personal experiential themes, before merging codes for final analysis to explore convergence and divergence across participants. 16 A second researcher (LL) independently interpreted the data once a first iteration of themes and subthemes had been developed. Codes and themes/subthemes were discussed and modified until CD and LL reached agreement. We did not return transcripts to participants to seek their feedback on analysis (respondent validation), to prevent possible emotional distress from them re-reading potentially upsetting conversations without the opportunity for debriefing. Bracketing CD's personal perspectives and existing knowledge of the topic area was not attempted during the analysis process; a reflective diary was used to appraise CD's subjectivity within the research process. This is fully acknowledged for transparency.
Results
Figure 1 shows the recruitment flow diagrams, with reasons for non-participation. Interviews lasted between 27 and 135 minutes. Three male participants had a family member present during the interview: one to support their understanding of the questions; one to facilitate translation as English was an additional language; and one to clarify details of his experience. Baseline demographic and stroke information is presented in Table 1. The 22 participants (55% male) were aged between 48 and 83 years (median age 66 years). Time since stroke ranged between 5.0–9.9 months (median = 5.9). Most (68%) perceived that their stroke had been mild and 64% had experienced their first stroke. At the time of assessment, participants reported low severity of disability or handicap (mRS median = 2, IQR = 1–2.3), and were physically able to manage everyday tasks (mBI median = 20, IQR = 19–20). Only three people met the threshold for anxiety (score of 10 or above) with none meeting the threshold for depression.14–15 Fourteen participants were married, one had a partner, five were widowed, one was divorced, and one was single. Nine participants were educated to a level of higher education, six had been to high school, six had a vocational qualification and one an apprenticeship. Before their stroke, 11 participants were retired, 10 were employed and one was unemployed.
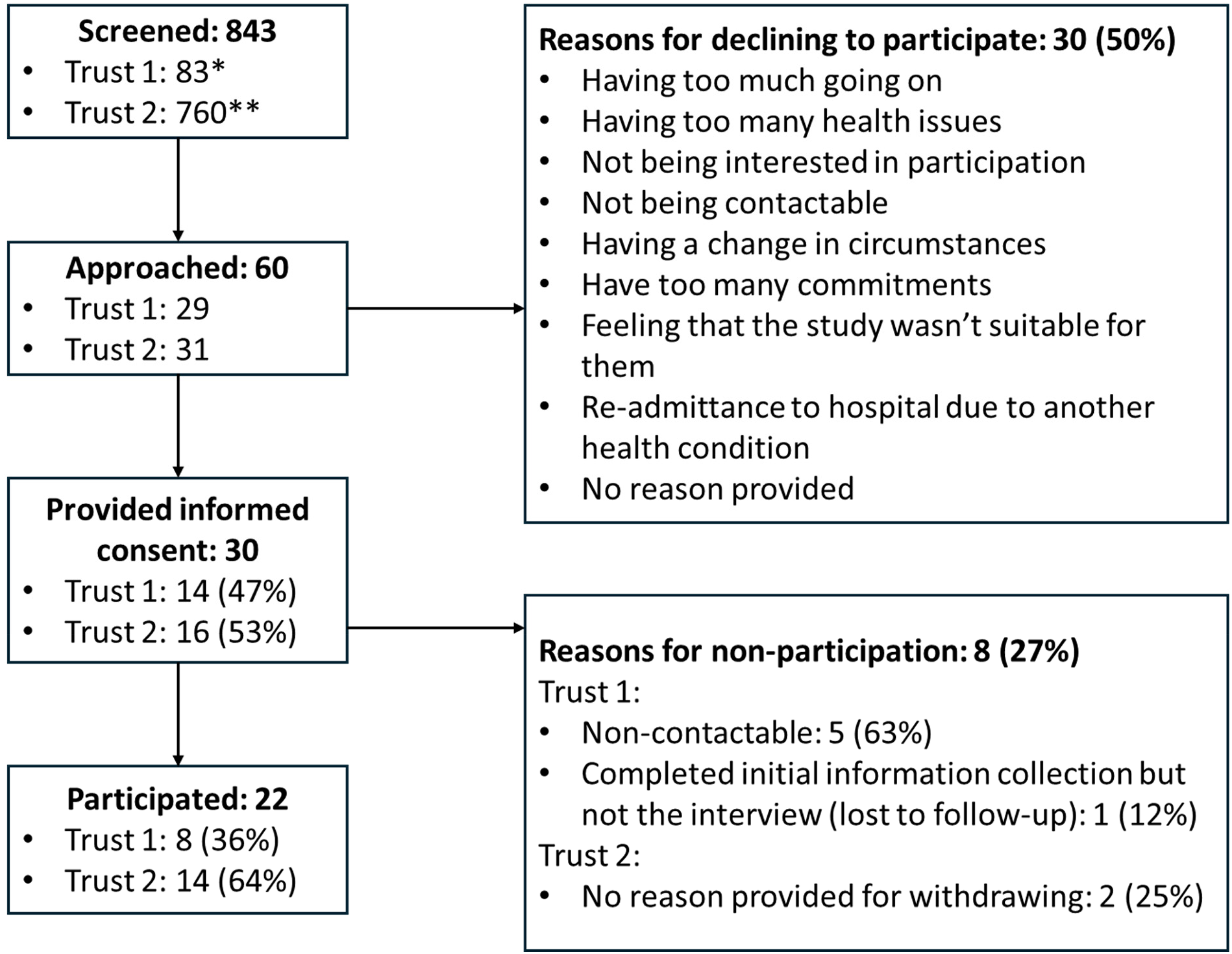
Recruitment flow diagram. *For Trust 1 recruitment logs were incomplete but provided a snapshot of 83 of the patients screened for participation. **Screening logs were maintained, except for June and August, which were manually screened on paper and where the Clinical Research Nurses provided estimates (n = 140). Of these patients, an estimated 129 were ineligible or declined to participate. Of the additional 620 patients confirmed on the screening log, 598 were ineligible and 13 were eligible but declined to take part.
Demographic and stroke-related information for each participant interviewed about their post-stroke body image experiences.
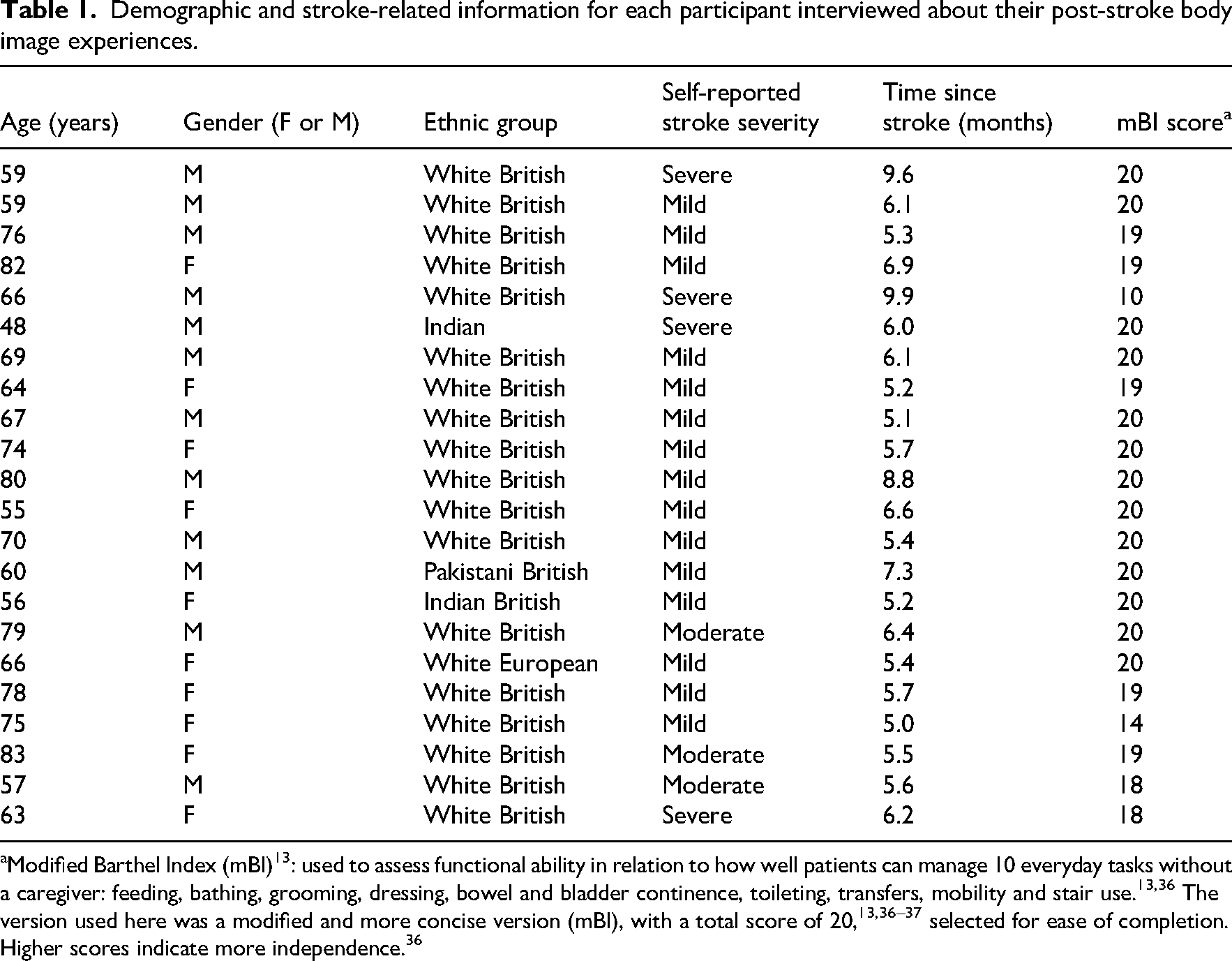
Modified Barthel Index (mBI) 13 : used to assess functional ability in relation to how well patients can manage 10 everyday tasks without a caregiver: feeding, bathing, grooming, dressing, bowel and bladder continence, toileting, transfers, mobility and stair use.13,36 The version used here was a modified and more concise version (mBI), with a total score of 20,13,36–37 selected for ease of completion. Higher scores indicate more independence. 36
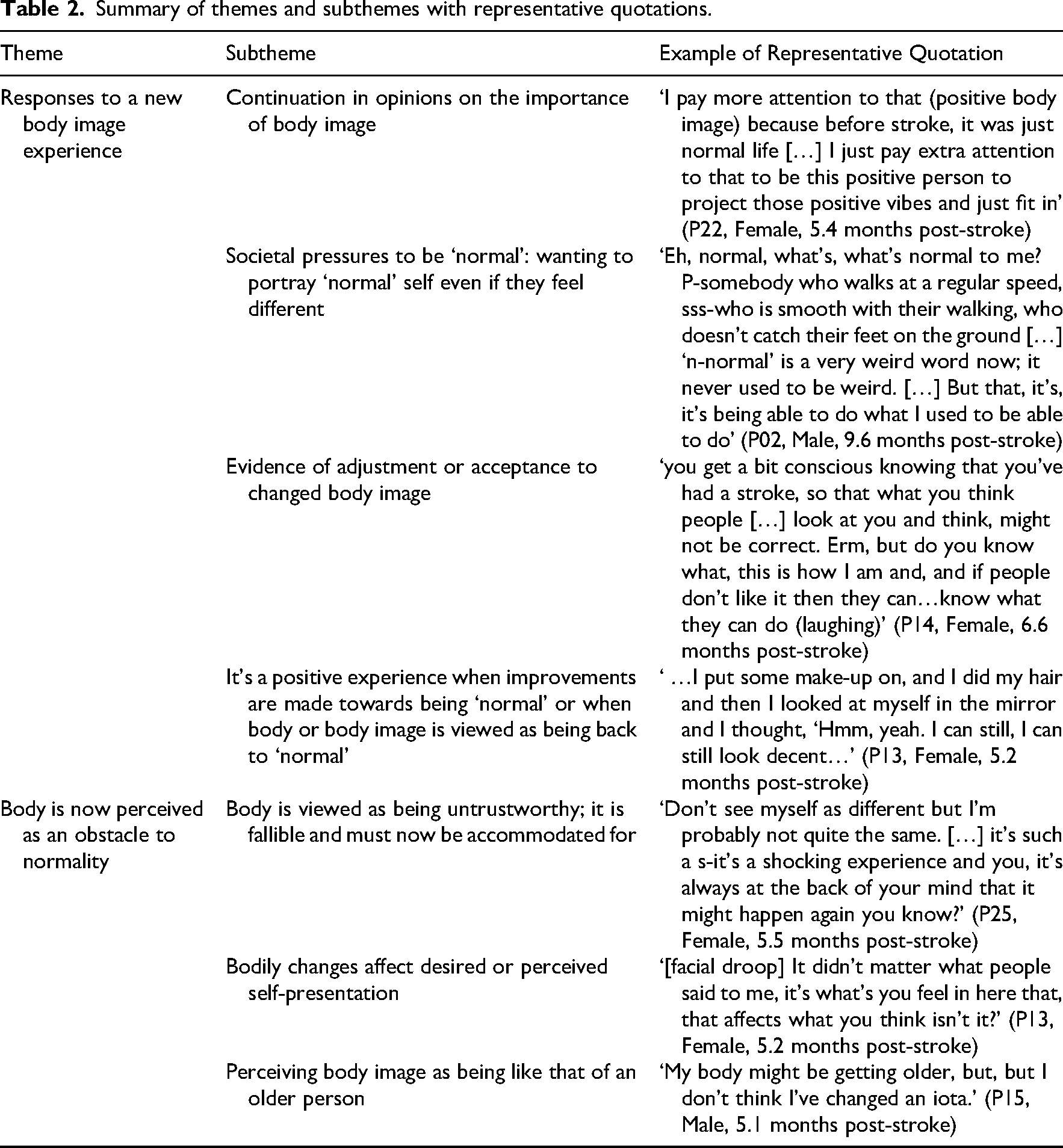
We identified two themes: (1) responses to a new body image experience and (2) body is now perceived as an obstacle to normality. These themes are further subdivided into seven subthemes. Each theme and its subthemes are described in more detail, and the coding tree is provided, in Figure 2. Table 2 shows the themes and subthemes, with an example quotation for each.
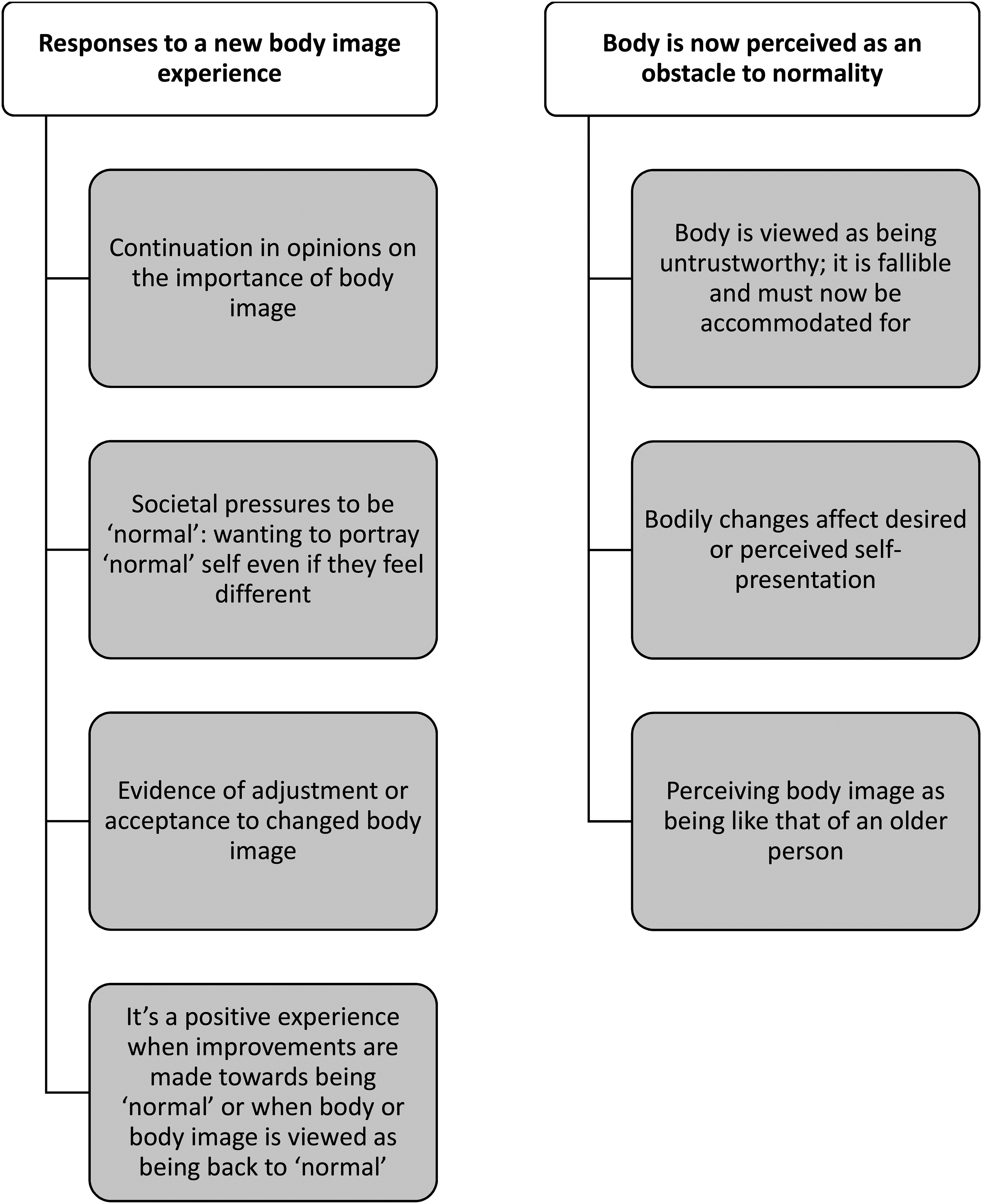
Coding tree showing the relationship between the two main themes and their respective subthemes for people with stroke.
Summary of themes and subthemes with representative quotations.
Theme 1: Responses to a new body image experience
Participants responded in different ways to a changed body image after stroke, which seemed dependent on (a) continuation in opinions on the importance of body image. There was evidence of (b) societal pressures to be ‘normal’ and wanting to portray a ‘normal’ self even if they felt different. Participants also demonstrated (c) evidence of adjustment or acceptance to a changed body image. It was also (d) a positive experience when improvements were made towards being ‘normal’.
Continuation in opinions on the importance of body image
After their stroke, participants maintained their pre-stroke views on the importance of body image. Body image gained greater importance post-stroke for people to whom it was important pre-stroke, evident through descriptions of paying greater attention to self-presentation and to projecting a positive body image: I pay more attention to that (positive body image) because before stroke, it was just normal life […] I just pay extra attention to that to be this positive person to project those positive vibes and just fit in (P22, Female, 5.4 months post-stroke) If there are other people around then I want to look, erm, acceptable […] I prefer to be tidy so that I erm, would not put people off by my appearance. However, I’m me erm, I don’t have to be determined by what I think other people would view me like (P29, Male, 5.6 months post-stroke)
Societal pressures to be ‘normal’: wanting to portray ‘normal’ self even if they feel different
During adjustment to their changed body, participants wanted to be ‘normal’, where normal was who they were pre-stroke: Eh, normal, what's, what's normal to me? P-somebody who walks at a regular speed, sss-who is smooth with their walking, who doesn’t catch their feet on the ground […] ‘n-normal’ is a very weird word now; it never used to be weird. […] But that, it's, it's being able to do what I used to be able to do (P02, Male, 9.6 months post-stroke)
People also felt self-conscious when they perceived their body looked different after their stroke (P02, P13, P14), even if it was something not perceived as noticeable to others (P02). This is evident in this example where one lady did not want her photograph to be taken: And I kept sort of just, “I’ll just nip to the loo.”, or (laughing). But in the end, I just gave in and let them take one. And actually, looking at it, was really good for me because I realised that it wasn’t that noticeable […] But it was good for this self-consciousness ‘cause it made me feel a lot better about it. (P13, Female, 5.2 months post-stroke)
Participants were most concerned with presenting a ‘normal’ appearance when they were going to be seen by others (e.g., P08, P27). They felt embarrassed when out in public and their body would not function how they wanted it to, linking to feelings of the body being out of their control (e.g., P02).
Evidence of adjustment or acceptance to changed body image
Some participants were adjusting to or accepting of their post-stroke body. This could be due to a general positive approach to their body image coupled with minimal stroke impacts (P15). For others with greater stroke impacts, bodily changes were difficult to cope with, although they tried not to let it affect them. Social context was important, with most participants referencing the adjustment or acceptance of other people when reasoning their own personal adjustment or acceptance: you get a bit conscious knowing that you’ve had a stroke, so that what you think people […] look at you and think, might not be correct. Erm, but do you know what, this is how I am and, and if people don’t like it then they can…know what they can do (laughing) (P14, Female, 6.6 months post-stroke)
Worries about other people's thoughts seemed to decrease with time (P02), although this could also be due to functional improvement and fewer personal body image concerns. For some people, part of coping was a sense of feeling lucky when thinking about how much worse the impacts of their stroke could have been on their body, and subsequently their body image (e.g., P14). Comparatively, other people were not concerned about what others thought at all (P24). These different outlooks on the perspectives of other people emphasises individual differences in body image experience.
It's a positive experience when improvements are made towards being ‘normal’ or when body or body image is viewed as being back to ‘normal’
Participants seemed to feel better when they perceived that their body image was similar or the same as before their stroke, or when they saw improvements: …I put some make-up on, and I did my hair and then I looked at myself in the mirror and I thought, “Hmm, yeah. I can still, I can still look decent…” (P13, Female, 5.2 months post-stroke)
Theme 2: Body now perceived as an obstacle to normality
After their stroke, participants viewed their body as an obstacle preventing them from experiencing their pre-stroke normality. It was now (a) untrustworthy, fallible and needed to be accommodated and (b) bodily changes affected desired or perceived self-presentation. Body image was now (c) perceived as being like that of an older person.
Body is viewed as being untrustworthy; it is fallible and must now be accommodated for
After their stroke, the function and capability aspects of body image experience were now magnified for participants. Physical aspects of their body which had been impaired by the stroke were untrustworthy, resulting in a lack of confidence in their own body. This included feeling unbalanced and uncertain about walking. Distrust and doubt in their body was also experienced in relation to fear of stroke recurrence, which made people fearful of strenuous activities. Some felt more content to stay at home.
Even when people did not perceive any post-stroke bodily changes, their outlook and body image experience was affected: Don’t see myself as different but I’m probably not quite the same. […] it's such a s-it's a shocking experience and you, it's always at the back of your mind that it might happen again you know? (P25, Female, 5.5 months post-stroke) […] when you go to cut something up, it actually requires thought, whereas you do it almost without thought. (P13, Female, 5.2 months post-stroke)
Overall, it was evident that the body and its negative change in perceived trustworthiness was experienced as being central to daily experiences.
Bodily changes affect desired or perceived self-presentation
It was participants' own personal perceptions and thoughts about their appearance which were the most salient to how they felt, even if other people did not notice any changes (e.g., P04): [facial droop] It didn’t matter what people said to me, it's what's you feel in here that, that affects what you think isn’t it? (P13, Female, 5.2 months post-stroke) And after stroke, it definitely takes like more focus, more devotion, more determination to do everything to get back to normal and sometimes it's hard (P22, Female, 5.4 months post-stroke)
Perceiving body image as being like that of an older person
Participants commonly referenced their age or getting older as a concern when discussing their body image or bodily perceptions. They now likened their body image to that of an older person, which they sometimes wanted to minimise, even if they had minor stroke impairments. They associated taking medication with older relatives (P04). Perceptions of premature ageing were also related to physical bodily changes. Descriptions were used that were associated with being older, including describing walking as ‘old man shuffles’ (P06), or having a ‘slightly quavery voice’ as seen in older people (P13).
People felt that others saw them differently, including as being ‘slightly more frail’ than they felt (P12). Emphasising this disconnect between what other people think and how internal body image is perceived, people perceived their ‘self’ as being the same, despite the body physically ageing: My body might be getting older, but, but I don’t think I’ve changed an iota. (P15, Male, 5.1 months post-stroke)
Discussion
The findings of this study show that body image after stroke is a broad, complex and unique experience which is socially constructed; it impacts, and is impacted by, social experiences. Body image can be interpreted in different ways by different people across different social contexts at different times, and needing to feel ‘normal’ in social settings is reinforced by social factors. 17 This aligns with sociocultural perspectives of body image; whereby perceived norms are perpetuated by society. 18 Based on Cash's cognitive behavioural explanation of body image, both cultural socialisation and physical characteristics impact body image experience.4–5 The need to feel ‘normal’ is compounded by any visible differences experienced due to stroke, causing people after stroke to feel further away from their understandings of societal and functional norms.
In the general population, appearance is the most important aspect of body image experience. 19 Comparatively, function holds a magnified role within post-stroke body image.19–21 Changes in function affect confidence. Increasing confidence after stroke relates to re-building skills and activities and re-engaging with life roles, which establishes positive self-belief and motivation. 22 Achieving or aiming to re-build or re-engage with previously enjoyed (‘normal’, pre-stroke) activities could therefore act as part of this motivation. In this respect, people with stroke may use their pre-stroke ‘normal’ as a comparator, and therefore as motivation, for their desired body image. This reflects the importance of historical factors (e.g., pre-stroke physical characteristics) and self-evaluations (e.g., satisfaction or dissatisfaction) as recognised by cognitive behavioural perspectives of body image.23–25
Acknowledging these roles of historical factors and self-evaluations in post-stroke body image experience has implications for post-stroke support. Aligning with positive psychology perspectives, encouraging bodily appreciation could facilitate a more positive view of the current body and prevent negative feelings from making comparisons to the previous self. 26
The continued importance of body image after stroke suggests body image is a personality trait which remains stable across different contexts.27–28 This links to the life-thread perspective, 29 whereby post-stroke experiences are made sense of by people combining their personal stories of their past, present and future. 17 However, what appeared most crucial to body image experience in the current study, was the fluctuation of body image experience across different situational contexts and times (state body image).3,23–25,27–28 This aligns with Merleau-Ponty's perspectives of embodiment in that the body is central to experience.30–31 Therefore, the current findings appear best explained through both trait (stable) and state (situational) components. 28
Other researchers have explored different aspects of post-stroke body image, including altered body perceptions and comfort in people experiencing motor, sensory, proprioceptive, or attentional issues due to stroke,9,31 or on the role of exercise in self-perceptions post-stroke. 3 Comparatively, we considered body image experiences from a broader phenomenological perspective. Although similarities are evident in the findings, existing work does not explore the importance of social context in bodily experiences, nor reference pre-stroke bodily opinions.
In our study, there were limitations affecting transferability of the findings. Not all patients were systematically screened potentially leading to selection bias. Use of a sampling frame aimed to encourage diversity in participant characteristics. However, the participants were younger than the average age for stroke in the UK (77 years, IQR = 67–85) 32 and had low levels of self-reported disability. Also, while the majority of participants were White British, which is comparable with the English and Welsh population (86%) 33 not all ethnic groups in the UK were represented. However, we achieved a representative sample in terms of socio-economic status. 34
Given the possible breadth of experiences, to further enhance our understanding, and to ensure findings and recommendations are as inclusive and as meaningful as possible across different societal contexts and constructs, post-stroke body image should be explored further with a broader participant demographic and stroke severity.
Overall, this research provides evidence for the personal impacts of stroke caused by altered body image. As such, it highlights body image experience as a potential area for support post-stroke. This contributes towards the evidence base of a top priority for the Stroke Priority Partnership, which is addressing the mental and emotional (psychological) problems caused by stroke.
35
However, there are no well-validated tools to identify issues with body image post-stroke. Given that body image experience has the potential to impact wellbeing after stroke, further research is therefore required in this area.
Perceiving a negative change in body image experience after stroke can impact on wellbeing and recovery. Key factors in how post-stroke body image is experienced include how important body image was pre-stroke, perceived deviations from pre-stroke ‘normal’ and social context. We have demonstrated negative changes in body image experience which could be a normal part of post-stroke adjustment. Further research is required to determine whether body image experience can be positively influenced by brief interventions such as guided self-help or psychological support to ensure they do not persist long-term.Clinical messages
Footnotes
Acknowledgments
Thank you to the National Institute for Health Research Applied Research Collaboration North West Coast (NIHR ARC NWC) for funding the research and to my supervisors and co-authors for their support. Thank you also to the participants who gave up their time to speak to me about their experiences, and without whom this study would not have been possible.
Ethical approval and informed consent statements
Ethical approval was granted by the Wales Research Ethics Committee 4 Wrexham on 30th November 2020 (REC Reference: 20/WA/0305). Written and verbal informed consent was provided by all participants.
Consent to participate
Written and verbal informed consent was provided by all participants.
Consent for publication
The consent process included asking participants to consent to their anonymised data being used as part of dissemination of the research.
Author contributions
Lead author, Catherine Davidson (CD), conducted the research as part of a doctoral research project. The thesis is available for access online (![]() ). Liz Lightbody (LL) was her main supervisor, with Caroline Watkins, Clare Gordon and Maree Hackett as additional supervisors. All supervisors contributed to the planning of the study, with LL also being involved in the analysis process. CD wrote this article, with all other authors reviewing and providing feedback.
). Liz Lightbody (LL) was her main supervisor, with Caroline Watkins, Clare Gordon and Maree Hackett as additional supervisors. All supervisors contributed to the planning of the study, with LL also being involved in the analysis process. CD wrote this article, with all other authors reviewing and providing feedback.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the National Institute for Health Research Applied Research Collaboration North West Coast. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: This study was part of a doctoral research project, funded by the National Institute for Health Research Applied Research Collaboration North West Coast (NIHR ARC NWC).
Data availability
In line with ethical approvals, anonymised data from this study may be requested for sharing within the same research theme. Written proposals and requests are to be directed to CD (lead author).