
Abstract
Objective
To investigate how health professionals working in palliative care services understand rehabilitation related to oncology palliative care in England and Brazil, according to different health system contexts.
Design
Qualitative study.
Setting
Hospices, hospitals, community-based palliative care centre, palliative care units, nursing care homes in different areas of Brazil and England.
Participants
Thirty-six nurses and occupational therapists experienced in providing palliative care interventions from England and Brazil.
Interventions
Individual interviews with open-ended questions.
Main Measures
Individual semi-structured, in-depth interviews, analysed using Braun and Clarke's reflexive thematic analysis.
Results
Professionals in England demonstrated a consolidated and integrated understanding of rehabilitation as part of palliative care, often supported by structured services such as hospices. In contrast, many Brazilian participants expressed uncertainty or perceived rehabilitation as incompatible with end-of-life care, reflecting conceptual misunderstandings, limited training and a lack of service infrastructure. The findings revealed divergence in how rehabilitation in palliative care is conceptualised and implemented in these countries. This divergence is reflected in structural, educational and cultural differences in how palliative care is organised and delivered. However, there is a growing recognition that rehabilitation and palliative care are not separate but complementary approaches.
Conclusions
The findings underscore the urgent need to clarify definitions, develop unified conceptual models and invest in policy and education to ensure that rehabilitation is no longer seen as contradictory to palliative goals, but as a complementary strategy to enhance quality of life in advanced cancer care.
Clinical messages
- A lack of conceptual clarity and national policies addressing rehabilitation in palliative care hinders its implementation, particularly in low- and middle-income countries.
- Clinicians in both palliative and rehabilitation services should adopt a shared, person-centred approach, focusing on autonomy, function and quality of life even at end-of-life stages.
- Interdisciplinary training and national policy support are essential to expand access to rehabilitative palliative care and address professional resistance or misconceptions in oncology settings.
Introduction
Cancer is one of the leading causes of death and an important obstacle to the increase in life expectancy in the world. 1 Palliative care is presented as a humanised form of care that focuses on improving the quality of life for patients and their families.2,3 Its most recent definition of palliative care is an approach that improves the quality of life of adult and child patients and their families facing problems related to life-limiting illnesses and provides a support system to help patients live as actively as possible until death. 4
Rehabilitation is a form of support for people with life-limiting illnesses, traditionally aimed at restoring function to pre-illness levels and maintaining it during treatment and remission.5,6 The World Health Organisation updated the concept of rehabilitation, defining it as interventions that help people with disabilities, or at risk of disabilities, to achieve and maintain optimal functioning in their environment. 7 Rehabilitation and palliative care have different histories and patterns of development, but they are increasingly converging, and the integration of these two approaches offers improved quality of life and meaning for patients, families, carers and service users, as well as for the professionals involved. 8
There is an increasing interest in combining rehabilitation and palliative care.9,10 In 2023 a document was published on the integration of rehabilitation in palliative care with the aim of understanding how the integration of these two approaches can improve the quality, accessibility, effectiveness and cost-effectiveness of health services for people in palliative care. 9 Incorporating a rehabilitative approach into palliative care may reduce suffering and symptoms, and support independence where possible. This improves quality of life for patients and their families until the end of life.10,11
A qualitative study in Australia exploring palliative care physicians’ perceptions of rehabilitation in inpatient units found a lack of consensus on terminology and definitions, highlighting the need for further research to establish agreed frameworks and evidence-based guidelines. 12
Defining the concept and implementing programmes for integrating rehabilitation into palliative care are essential for making it an established intervention accessible to all cancer patients within specialised palliative care. 12 Research on the conceptual integration of these fields is limited, highlighting the need for wider dissemination and understanding of the benefits rehabilitation can offer during disease progression.8,12
The provision of rehabilitation within palliative care remains innovative and controversial in many regions, particularly in developing countries such as Brazil, highlighting substantial gaps in knowledge and research, especially within the Brazilian context. Therefore, the study aimed to investigate how health professionals working in palliative care services understand rehabilitation related to oncology palliative care in England and Brazil, according to different health system contexts.
Methods
Ethical issues
Ethics approval and consent to participate was granted by the University of São Paulo (number 21189919.0.0000.5393) and Kingston University Research Ethics Committee (number 1468) on 5 May 2020. The research project was submitted and approved in all the participants’ institutions in England and in Brazil. All participants gave their written or verbal consent for participation. Transcribed data was anonymised using identity numbers.
Study design
This is a multicentre, cross-sectional, exploratory study employing a qualitative design and a two-country interview study. A constructionist-interpretive approach was adopted, whereby palliative care professionals constructed meaning through their experiences and understanding of rehabilitation. These insights were shaped through their day-to-day interactions with patients and within their work environment. The researchers’ interpretations were also considered in analysing the data. 13 We used individual interviews with open-ended questions to explore and describe the participant's perspectives. 14 The reflexive thematic analysis was used to identify the critical themes grounded in the interviews.15,16 Our study was reported according to the consolidated criteria for reporting qualitative studies – COREQ. 17
Participants
The sample size for this study adhered to guidance from Malterud et al. 18 since ‘information power’ appears more suitable than ‘data saturation’ in the context of reflexive thematic analysis. A pilot interview was conducted, and minor changes to the schedule were made. Demographic information was recorded using a simple questionnaire.
Potential participants were eligible if they were qualified occupational therapists and nurses, working as clinicians or managers and experienced in providing palliative care interventions. Inclusion criteria comprised nurses and occupational therapists who: (a) were permanent employees of the palliative care services, (b) had at least one year of professional experience in health services of caring for patients in palliative care, (c) were able to understand and communicate in English or in Portuguese and (d) were willing to provide informed consent to participate in the study. Thus allowing for a deeper understanding of the discussion on the topic.
Recruitment
Participants were recruited from various settings such as hospices, hospitals, community-based palliative care centre, palliative care units, nursing care homes in different areas of Brazil (Distrito Federal and states of São Paulo, Alagoas, Pará, Minas Gerais, Paraná, Bahia) and England (London and its boroughs).
In order to carry out the collection in the Brazilian field of study, once the potential participants were identified through the snowball sampling technique, the researcher contacted them via e-mail or telephone to invite them to participate, presenting the research objectives.
Regarding the British field of study, the gatekeepers and research lead of each service forwarded information about the research and the invitation to participate to all nurses and occupational therapists who met the inclusion criteria of the study during their team meetings.
All invited participants were informed about the research's aim and agreed to participate in the study. Potential participants were approached via email and offered the opportunity to participate at a time suitable for them. Informed consent was obtained, and all participants were informed about the right to withdrawal.
Data collection
The individual semi-structured, in-depth interviews were conducted by a female researcher trained in qualitative methodology, PhD and occupational therapist (GR), remotely via video conferencing software (Zoom®, Skype®, Google Meet® and Microsoft teams®). The research was carried out between 2020 and 2022. There were difficulties in arranging the interviews due to the pandemic period of the first and second waves of COVID-19 in both countries. All interviews in the British scenario were conducted in English and in Brazil, in Portuguese. A participant information sheet outlined the objectives for doing the study.
The interviews utilised open-ended questions and probes to explore participants’ perceptions of rehabilitation in the palliative care field were recorded with permission and lasted between 20 and 90 minutes. The interview guide for the participants was formulated (see Supplemental materials 1 – Interview Schedule). The questions were based around three main themes: (a) experience of working in oncological palliative care, (b) the meaning and the definition of Rehabilitation in Palliative Care and (c) the specific needs and barriers to providing rehabilitation for oncological palliative care patients.
Data analysis
Notes from the interviews were documented during or immediately following the interview. Firstly, transcripts were separately read by two researchers (GR and GMXS) to identify any broad themes and have an initial understanding of the contents. Then, for the systematic coding of data, generation of themes, refinement and naming, the software MAXQDA (Computer Aided Qualitative Data Analysis Software) Analytics Pro Student 2020® was used. The context of the participant's responses was considered in creating codes, and when discrepancies between the two researchers occurred, a third author was consulted (MMRPDC). Researchers condensed codes into higher-order categories, and a final coding framework was developed, capturing themes and sub-themes grounded in the transcripts in a satisfactory way concerning the research objectives, according to the six-phase guide in reflexive thematic analysis by Braun and Clarke.15,16 We used an inductive approach, where themes are progressively refined based on codes identified in the data. Connections between themes and sub-themes were established, and comparisons within and across transcripts performed cycles of inductive elaboration on themes. The analysis was conducted on the original transcription in English and Portuguese (GR, IB and MMRPDC). Illustrative quotations have been translated and are presented throughout the findings section to increase the findings’ trustworthiness. The translation is not a straightforward process as it might be challenging to match the English translation to the Portuguese verbal content. This is due to differences in syntax, expressions and word order. Therefore, when translating the quotations into English, the intention has been to convey the participants’ narrative as brought forward in the interviews. Edits were made to the quotes to correct grammar and omit extraneous words.
Regarding improving the reliability and credibility of the research process, the researchers used triangulation, peer review and reflexivity. Triangulation involved three analysts during the data analysis to ensure the accuracy of the data analysis and interpretation. Peer review consisted of a second researcher reviewing 100% of the transcripts and debriefing the analysis with the principal investigator. Reflexivity was carried out throughout the development of the project, by the research team holding reflexive meetings to help identify and challenge assumptions in the interpretation of the themes.
Results
A total of 36 palliative care professionals, 18 occupational therapists and 18 nurses were involved in this study. None of the participants dropped out of the study. Table 1 shows participant demographic information.
Demographic data of the participants.
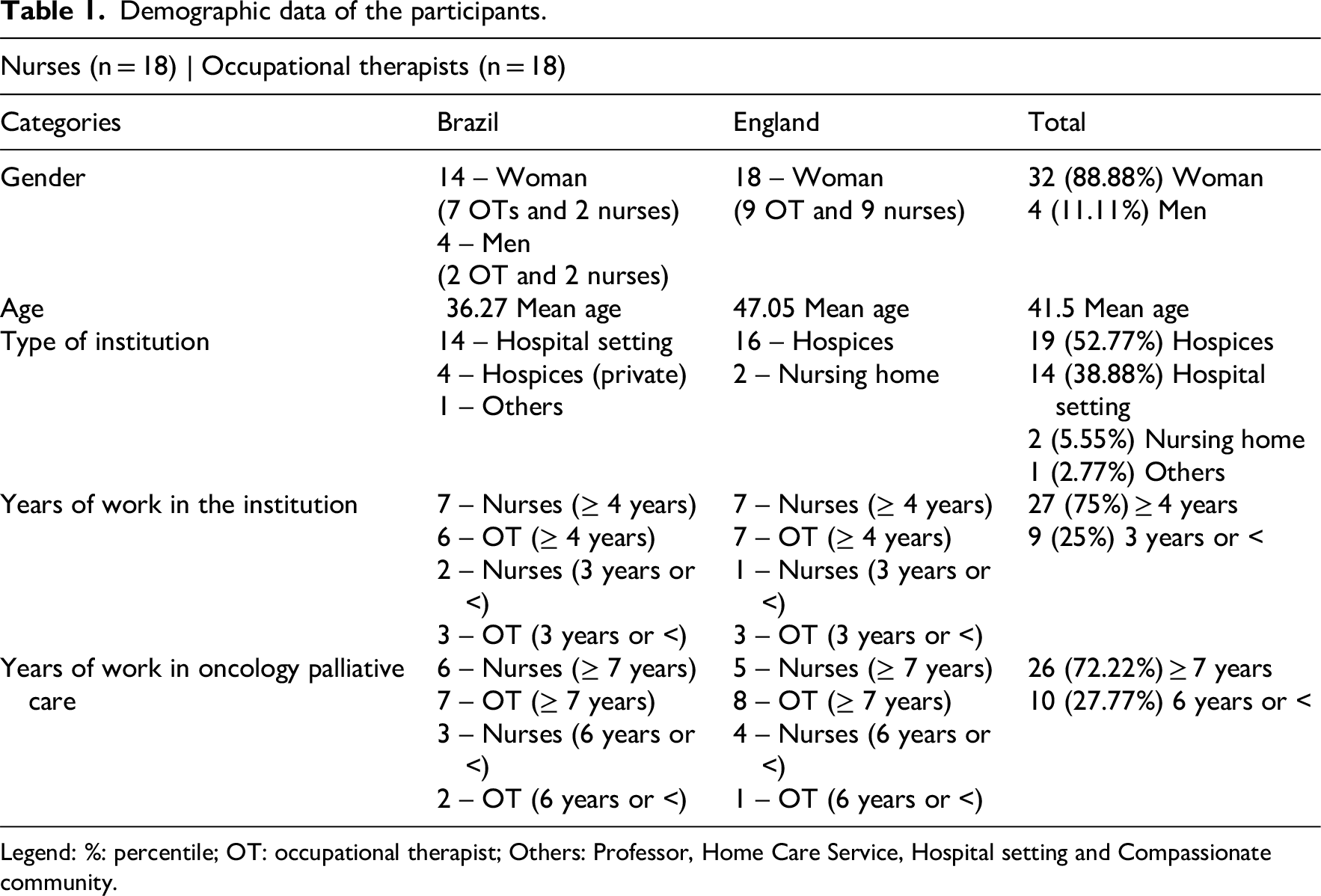
Legend: %: percentile; OT: occupational therapist; Others: Professor, Home Care Service, Hospital setting and Compassionate community.
The participants were recruited working in different parts of Brazil and England, as shown in Graph 1.
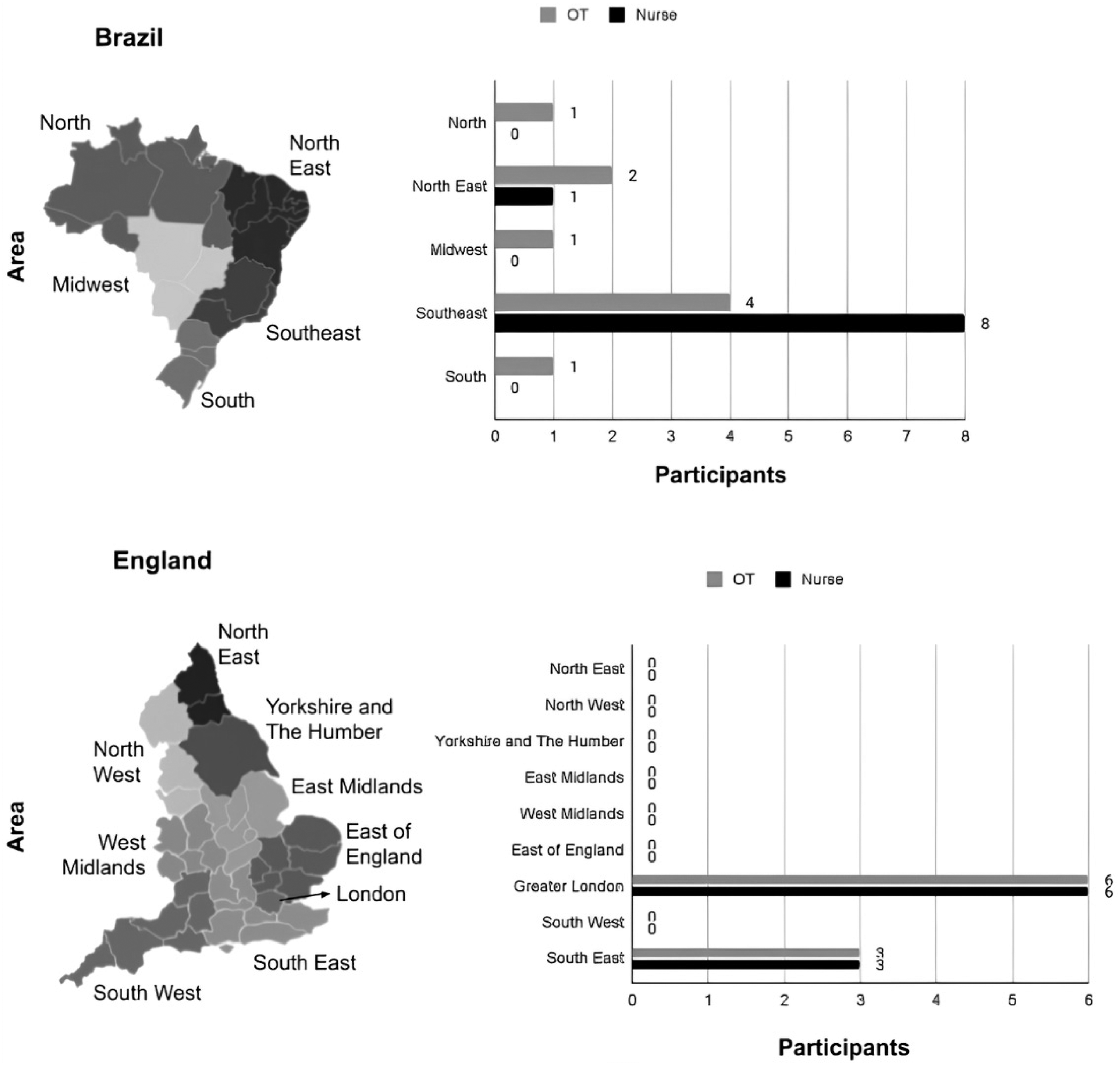
Geographical location of the participants per workplace.
The average age of participants was 41.5 years. The majority of participants were women, had worked in hospices in the United Kingdom and hospitals in Brazil for 4 or more years, and had worked in oncology palliative care for 7 or more years.
Thematic analysis
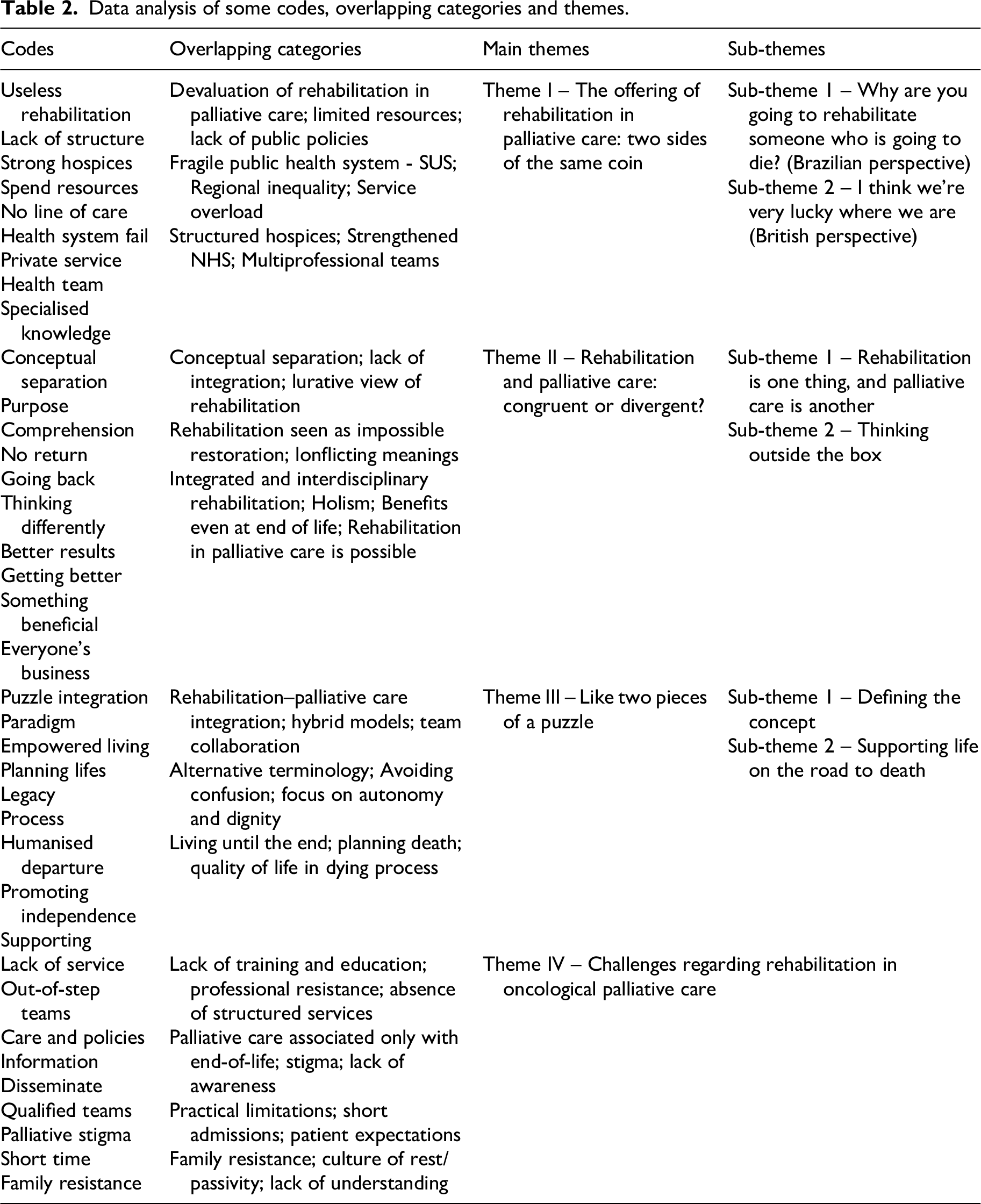
Initially, codes were identified from a thorough reading of the transcripts, representing meaningful units of meaning extracted from the empirical material. The codes were then compared and grouped into overlapping categories, which consider the convergences and divergences of meanings identified in the reports. This process allows for the construction of main themes, which express central patterns related to the phenomenon under investigation, and their sub-themes, which detail specific and complementary aspects, enabling a deeper understanding of the experience studied (Table 2).
Data analysis of some codes, overlapping categories and themes.
Four themes emerged from the qualitative analysis of participants’ responses regarding their experiences and perceptions of rehabilitation within the context of oncological palliative care (see Figure 1).
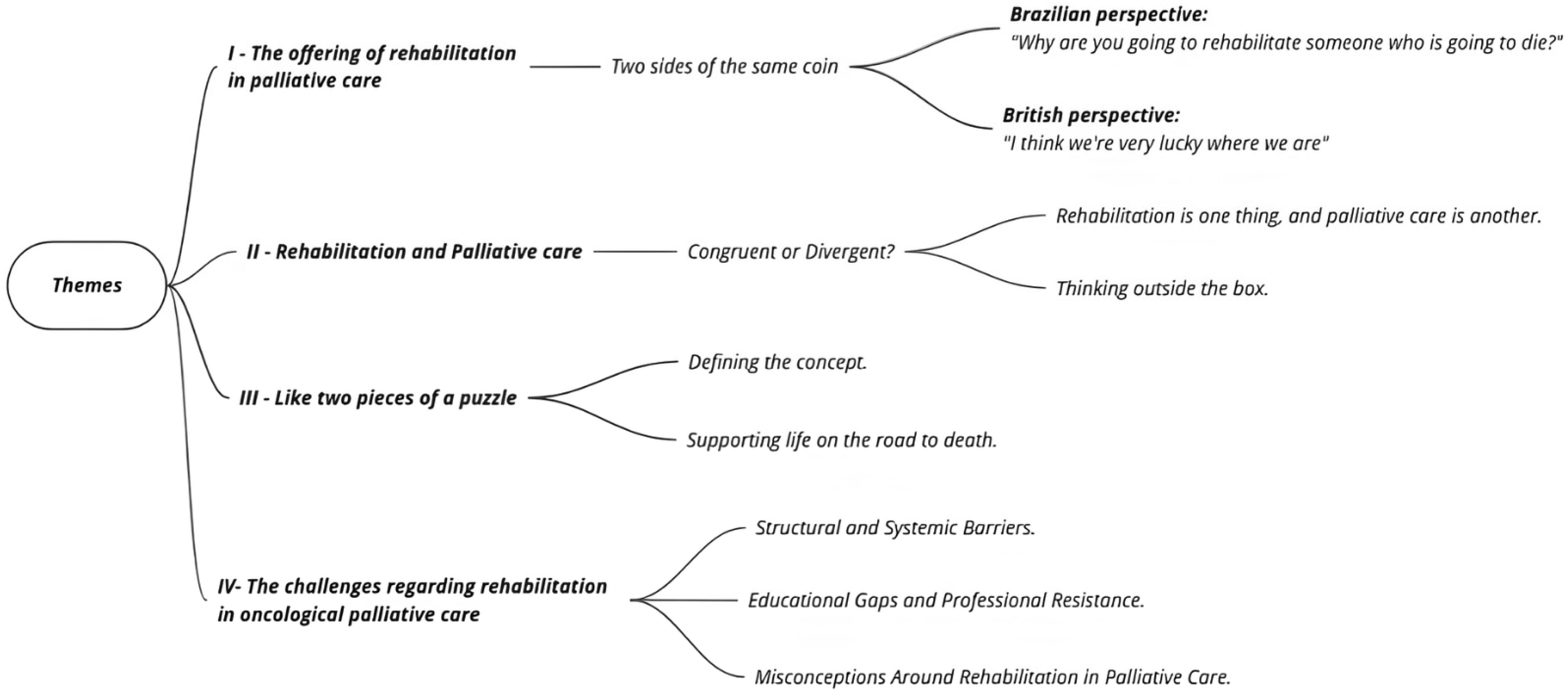
Themes emerged from the qualitative analysis.
The findings indicate a predominantly favourable perception of palliative rehabilitation, particularly in the United Kingdom, where services are more structured and awareness of the topic is higher. However, there was considerable variation in participants’ familiarity with the concept, depth of understanding, and professional experiences. In the Brazilian context, notable challenges were observed due to structural limitations in providing rehabilitation services for patients in palliative care, especially in cancer. Despite the barriers and challenges to integrating rehabilitation and palliative approaches, participants emphasised the importance of implementing these services to enhance the quality of life for cancer patients, even in the advanced stages of illness and end-of-life care.
Theme I: The offering of rehabilitation in palliative care: Two sides of the same coin
This theme captures a notable discrepancy in the accessibility and quality of palliative rehabilitation services between Brazil and the United Kingdom. The provision of palliative care in the United Kingdom and Brazil demonstrates significant contrasts, with systemic differences impacting the recognition and delivery of rehabilitation within the palliative context.
Why are you going to rehabilitate someone who is going to die? (Brazilian perspective)
Brazil is confronted with significant challenges in providing palliative care, largely due to structural weaknesses within its healthcare system. “Why are you going to rehabilitate someone who is going to die? The managers would say to you, what are you going to spend resources on?” (Nurse8-BR)
Participants identified a deficient provision of palliative care, constrained funding, and inadequate training of professionals as crucial impediments. These challenges are further compounded by the lack of prioritisation of palliative care within national health policies, which frequently results in inadequate investment. Consequently, palliative care, which is already under-recognised in the broader healthcare context, becomes challenging to consider as a viable component of the rehabilitation process. “I think we have a hard time thinking about oncological patients, because there is no line of care here, so the patient comes in and where is he going to be sent? There's no care, there's no outpatient care, there's no hospice, the primary care network is extremely weakened, the home care service is extremely overloaded and there are smaller cities where this happens much less.” (OT4-BR) “We don't even have the basis of palliative care. The Ministry of Health says that palliative care is part of it, but rehabilitation in palliative care is one of the last components and shouldn't be.” (Nurse9-BR)
The provision and availability of palliative care services is precarious in many countries, especially in Brazil, where this type of care is still only offered at the end of life, contradicting what is recommended in the definitions of palliative care. The inclusion of rehabilitation in this context is even more precarious. “The issue of palliative care is only introduced at the end of the patient's life, with very, very aggravated symptoms and with great damage to quality of life.” (Nurse3-BR)
Brazil faces significant structural challenges, both in terms of human resources and service organisation, which expose the weaknesses of the Brazilian health system and the deficiencies of public policies related to palliative care. In addition, the vast geographical size of the country exacerbates disparities in the structure and delivery of services. These inequalities are particularly evident when comparing the private health sector and the supplementary healthcare system with the public Unified Health System (SUS). In addition, there are significant regional differences in the availability and quality of services in different parts of the country, further highlighting inequalities within the system. “It's a different reality here [north-east of Brazil]. I have a lot of illiterate patients, there's a lack of primary health care assistance. To give you an idea of what the health context is like here, primary care, there's no occupational therapist in palliative care here, it's very complicated.” (OT2-BR)
“I think our system [SUS - Unified Health System] doesn't really help, maybe it would be more functional in a private service.” (Nurse5-BR)
In contrast, the United Kingdom demonstrates a distinct model of palliative care, emphasising the importance of hospice structures and their associated benefits. This distinction is evident through the perspectives shared by British participants, who highlighted the role of hospices in delivering comprehensive, patient-centred care that addresses the multifaceted needs of individuals receiving palliative care.
I think we're very lucky where we are (British perspective)
In the United Kingdom, palliative care is offered within a well-established and structured healthcare system which facilitates the integration of palliative care as a recognised component of comprehensive rehabilitation approach in cancer care. “It's that they can live longer with a better quality of life for longer just with our contributions, I think things like that are really forgotten by people who don't really know what hospices are, or what rehabilitative palliative care is. I think we're very lucky where we are. I'm not sure what it's like in Brazil, or your health system, but we're so lucky in England, sometimes when we complain about the National Health System [NHS] you think it's joking.” (Nurse6-UK) “I came from a hospital setting, so it's very important that people are discharged quickly. But when you come to a hospice it's quite different (…) And I didn't really realise that people can come here and they can actually get better or their condition can stabilise and they can go home and they can still lead a reasonable life and some people come just to rest.” (OT7-UK)
The United Kingdom participants described a system whereby multidisciplinary teams are trained to address patients’ holistic care needs. This enables the incorporation of rehabilitation into palliative care pathways, thereby enhancing patients’ quality of life even during advanced stages of illness. “Our team is amazing, we go to people's homes, we do all the complex symptom control, but I like to think that all hospices are like a cake. We enable people to have quality of life, we're all just the ingredients. They need all of us to make the cake, you have all the ingredients here to make a cake full of quality for these patients. And it's about the patient coming and choosing which ingredients they want and deciding which piece they want for their quality. And hospices can literally make a big difference to these people's lives, not just this hospice. Every hospice I've worked in has all these services.” (Nurse5-UK) “I think I'm very spoiled, we have hospice because they're just amazing. You just see the patients and how they just relax when they get to the hospice, knowing that they're actually being looked after and with that specialised knowledge.” (OT4-UK)
Thus, United Kingdom participants highlighted the presence of well-organised frameworks that support palliative care, while Brazilian participants often described systemic barriers, such as insufficient funding, a shortage of trained professionals, and inadequate infrastructure for both palliative care and cancer rehabilitation.
These contrasting perspectives underscore the profound influence of systemic structures on the recognition and implementation of palliative care and rehabilitation. While the United Kingdom benefits from a cohesive and well-resourced framework that enables integrated care, Brazil's systemic challenges highlight the urgent need for investment in infrastructure, workforce development and policy reform. Addressing these gaps is critical to ensuring equitable access to palliative care and rehabilitation for patients with advanced cancer, regardless of geographic or economic disparities.
Theme II: Rehabilitation and palliative care: Congruent or divergent?
Rehabilitation remains a widely misunderstood concept among healthcare professionals when considered in the context of life-limiting illnesses, particularly in oncology. This misconception is particularly evident in Brazil, where some participants considered rehabilitation to be neither feasible nor appropriate within palliative care, reflecting broader systemic and cultural challenges that impact on the understanding and implementation of rehabilitation in this context.
Rehabilitation is one Thing, and Palliative Care is Another
For participants, (all from Brazil) rehabilitation was often associated exclusively with curative or restorative goals, which they perceived as incongruent with the aims of palliative care. These two concepts are perceived as fundamentally different, with minimal overlap in their goals or practical application, as reflected in the participants’ perspectives: “I wouldn't put palliative care within rehabilitation (…) so I couldn't find a denominator because I think rehabilitation is one thing and palliative care is another.” (Nurse7-BR) “Rehabilitation in palliative care I didn't see it that way. When you talk to me about rehabilitation, I think of the patient who is going to rehabilitate their functionality and in palliative care, we're going to try to give comfort to this patient, not necessarily that they're going to be able to gain functionality.” (Nurse4-BR)
This perspective highlights the conceptual challenges that arise when attempting to integrate rehabilitation into a palliative care framework. For some Brazilian participants, rehabilitation is seen as separate from palliative care. Such a perception reflects a more compartmentalised understanding of healthcare, where interventions are categorised into discrete domains rather than viewed through a holistic, integrative prism. “My vision isn't for that, for me it doesn't fit into palliative care. Rehabilitation is a term that isn't part of my practice, so for me rehabilitation, there is no returning to what once was.” (OT3-BR)
This participant's statement reflects a perception that rehabilitation is linked to restoring individuals to a previous state of health or functionality, which contrasts with the goals of palliative care. ‘Rehabilitation’ implies an expectation of recovery that is incompatible with caring for patients with life-limiting illnesses. The expression ‘there is no returning to what once was’ is highlighted, as it encapsulates the participant's belief that rehabilitation in its traditional sense is not applicable in the context of palliative care. This view reinforces a fundamental conceptual tension in which rehabilitation is often understood as the goal of physical recovery.
The internal conflict experienced by some professionals in aligning rehabilitation with palliative care is exemplified by the following participant's perspective: “I have great difficulty defining rehabilitation. I understand this differentiation of rehabilitation within the context of palliative care, I know that today there is the term, the concept and the intervention of palliative rehabilitation, but I argue a lot with myself about what that means, honestly I still can't tell you conceptually what that would be, to close off palliative rehabilitation is to limit myself, it's to punish myself. It doesn't make sense to me today.” (OT6-BR)
Despite the recognition of the existence of a formalised concept – palliative rehabilitation – there is a simultaneous resistance to defining it in rigid terms, perceiving such boundaries as limiting and even contrary to the holistic ethos of palliative care. This perspective challenges traditional notions of rehabilitation, which often focus on tangible and measurable outcomes. Therefore, these perspectives may be influenced by systemic and cultural factors, particularly in contexts where palliative care is still developing, such as Brazil. The lack of integration between rehabilitation and palliative care in many health systems reinforces this dichotomy, leading professionals to view these two approaches as separate and sometimes incompatible.
Thinking outside the box
On the other hand, British and some Brazilian participants described a more integrated understanding of rehabilitation within palliative care. Rehabilitation was described as a means of improving patients’ physical, emotional and social wellbeing, which is closely aligned with the holistic goals of palliative care. “I think it's thinking outside the box, being open-minded to the idea that rehabilitation can be really beneficial even for people who are living with serious illnesses and even for people whose general problems are getting worse.” (Nurse9-UK)
For some participants, rehabilitation was seen as an opportunity to support patients in achieving the best possible level of independence, functionality and wellbeing, despite the limitations imposed by their illnesses, including an interdisciplinary perspective: “Everyone with a palliative diagnosis can be rehabilitated in some way. So I think it's very difficult to convey this concept even to some members of our multidisciplinary team, but I think we're lucky here.” (OT4-UK) “Rehabilitation certainly gives better results even for people at the end of life, so I think it's essential for me. Rehabilitative palliative care is not just the domain of physiotherapists and occupational therapists, it must be integrated, it must be everyone's business.” (Nurse3-UK)
Participants acknowledged the challenges of conveying this concept, particularly within multidisciplinary teams. This challenge points to a potential gap in education and awareness about the role of rehabilitation within palliative care frameworks. Despite these difficulties, the participant underscores the rehabilitation within palliative care is perceived as impactful even in the final stages of life, where the focus shifts from recovery to maintaining dignity, comfort, and quality of life and the need for an interdisciplinary approach, through coordinated teamwork. “When I saw the concept of health, which is a Preventive, Curative, Rehabilitative and Palliative process, you can't dissociate one from the other. Within palliative care, I can have preventive, curative and rehabilitative care. Within rehabilitation, I can have curative, palliative and preventative. I think they're inseparable, prevention, curative, the search for a cure, because it doesn't have to be a cure for everything, but curing a symptom, for example, is a cure.” (Nurse1-BR)
Participants provided a holistic perspective on healthcare, supporting an integrated model in which each process complements and reinforces the others. Within this framework, rehabilitation extends beyond physical restoration, merging with efforts to alleviate symptoms and improve overall wellbeing. This expanded interpretation aligns with the goals of palliative care, which emphasise symptom management as a means to enhance patients’ quality of life.
Consequently, participants suggested that healthcare professionals should look beyond traditional notions of rehabilitation, embracing the idea that meaningful interventions remain possible, even in the context of progressive illness. “Palliative rehabilitation can scare people a lot, because rehabilitation means getting back, going back to the beginning and then you're not going back, it's going to be from where they are, from where they started. It's going to be strange, different if I wasn't a palliativist and didn't see that. There is life as long as the person is living, but you have to be detached to do that.” (Nurse8-BR)
It is possible to observe the potential discomfort or resistance among professionals who are not as familiar with palliative care principles. The idea that ‘there is life as long as the person is living’ reflects the fundamental philosophy of palliative care, emphasising that rehabilitation is not about reversing decline but about enhancing life in the present moment. These findings suggest that integrating rehabilitation into palliative care requires not only redefining its goals and practices but also fostering a cultural shift among healthcare professionals.
Overall, the findings highlight the potential of fostering an open-minded and innovative perspective among healthcare professionals to advance the integration of rehabilitation into palliative care frameworks. By reimagining rehabilitation as a flexible and holistic intervention, it may be redefined as a vital component of comprehensive care, significantly enhancing the quality of life for individuals with life-limiting illnesses at all stages. Achieving this vision, however, requires overcoming conceptual barriers, fostering interdisciplinary collaboration, and promoting a unified understanding of rehabilitation as an integral part of palliative care.
Theme III: Like two pieces of a puzzle
The integration of rehabilitation and palliative care was seen as a dynamic and evolving approach aimed at optimising quality of life for individuals with life-limiting illnesses. Although traditionally viewed as distinct areas of care, rehabilitation and palliative care are increasingly recognised as complementary, working together like two pieces of a puzzle. This theme explores how rehabilitation is conceptualised within palliative care, examining the different terminologies and frameworks used by healthcare professionals to define its role.
Defining the concept
The participants reported the diverse approaches to understanding and articulating rehabilitation within palliative care. The participants’ definitions of rehabilitation within palliative care reflected a diverse and evolving understanding, which was influenced by their professional backgrounds, experiences and healthcare contexts. While the terminology used varied, including palliative rehabilitation, rehabilitative palliative care, rehabilitation in palliative care, reablement rehabilitation approach, and even empowered living, there was a shared recognition that rehabilitation in palliative care is not about reversing decline but about optimising quality of life, preserving dignity, and promoting autonomy within the constraints of progressive illness.
A significant proportion of participants conceptualised rehabilitation within palliative care as a process of adaptation, aimed at assisting patients in adjusting to changing functional abilities. This process fosters self-management, compensation strategies, and family awareness. The paradigm of rehabilitative palliative care was described as an approach that empowers individuals to maintain as much independence as possible while recognising and accepting disease progression: “It's within this paradigm of rehabilitative palliative care, it's about reframing roles, looking to support the person to recognise that there is a change, because of the progression of the disease, and an acceptance of it. So when you think about rehabilitative care, the rehabilitation paradigm involves empowerment, compensation, self-management and self-care. It's about supporting the person to recognise that there is a change in their function, because of the progression of the disease, and it's also an acceptance of the change, it's also about bringing the family some awareness that actually they may not recover, they're not going to go back to who they were before, and it's about getting to that level of acceptance.” (OT5-UK)
Similarly, the reablement/rehabilitation approach was described as a coordinated and flexible strategy that evolves according to patients’ changing priorities: “The reablement/rehabilitation approach is about the importance of promoting someone's independence to do the tasks as much as they can do them or achieve their personal goals, interests, and their priorities. The whole team works collaboratively with the patient, family and other carers to support them to achieve personal goals in a coordinated way, and their priorities can change as they get progressively worse. I also think it's about working holistically, so I think it's really about finding out what's really important. But it's also about enabling that person to be as independent as possible and also about optimising their function. Rehabilitation has to be careful and flexible, and you have to be able to adapt very quickly as well.” (OT7-UK)
These perspectives highlight rehabilitation as an interdisciplinary, patient-centred approach, in which professionals collaborate to establish achievable, personalised goals that undergo modification as the illness progresses.
Beyond considerations of functionality, the concept of rehabilitation was also described as an instrument for preserving dignity, alleviating suffering and promoting comfort. One participant defined palliative rehabilitation as: “There's palliative rehabilitation, so it's making life as comfortable and dignified as possible. So comfort, dignity, respect, not condemnation and sadness. It's exactly the opposite.” (OT1-UK)
This is consistent with the holistic philosophy underpinning palliative care, illustrating that rehabilitation encompasses not only physical function but also social, emotional and existential dimensions of wellbeing.
Despite the shared goals of rehabilitation in palliative care, terminology itself was identified as a barrier to understanding and acceptance. Some participants pointed out that the word rehabilitation often implies recovery or restoration, which can lead to misunderstandings among patients, families, and even healthcare professionals: “People hear the word rehabilitation, and they can get very confused about it. It needs to be achievable, it needs to be realistic, and it needs to be in line with what the patient really wants. I like the phrase ‘empowered living’, about empowering people. And I like the team that calls itself the ‘empowered living team’, because I think that sounds better than rehabilitation and I don't think it gives people the wrong idea. It can't make them independent, but what you can do is empower them a bit more. It's very sensitive. It doesn't sound so much like hard labour, this ‘empowered life’ sounds like something much gentler. So I think people can expect more than rehabilitation.” (Nurse5-UK)
This participant suggested alternative language such as ‘empowered living’ with a view to providing a more appropriate frame of reference for rehabilitation that would resonate more effectively with patients and that would avoid any potential misconceptions.
Others argued that it is important to explicitly recognise rehabilitation within palliative care, ensuring that it is seen as an integrated, essential component rather than an add-on: “I would say rehabilitation in palliative care, I think it defines it very well, because it's rehabilitation, so I have to use it, I think it's important that I use the term and it's in palliative care. It's being able to look at the patient, the family and find the best that they want and that they want in terms of their body, their image, and from there be able to draw up a plan and help them with that.” (Nurse5-BR)
These statements emphasise the necessity for greater awareness and more effective communication regarding the role of rehabilitation in palliative care. This is both within healthcare teams and in interactions with patients and their families.
Thus, participants described this integration using different terms, reflecting the evolving nature of the concept across healthcare contexts: ‘Palliative rehabilitation’; ‘Rehabilitative palliative care’; ‘Rehabilitation in palliative care’; ‘The reablement/rehabilitation approach’; ‘Empowered living.
The participants’ perceptions indicated that, despite the utilisation of disparate terminology to describe rehabilitation in palliative care, their definitions exhibited common elements. Rehabilitation is about adaptation, empowerment and self-management, collaboration among healthcare teams, patients and families to define and achieve meaningful goals, and extends beyond physical function. The findings indicate that language and terminology can influence perceptions, and that clearer communication is required to ensure that rehabilitation is understood as an integral part of palliative care.
Supporting life on the road to death
The participants described rehabilitation as a means of preserving function, dignity and autonomy, ensuring that individuals experience comfort, control and quality of life in their final days. This sub-theme explores how rehabilitation supports individuals in engaging with life while preparing for death, highlighting the importance of planning, person-centred care and a shift in societal attitudes toward dying.
The participants reported the notion that death should be humanised to the same extent as birth, requiring care, intention and support for the individual and their loved ones. One participant described the satisfaction of being able to support individuals in maintaining their sense of functionality and wellbeing until the end of their lives. “When I realise that there's something I can do to make the person feel functional until the moment they die, when that's possible and I feel very good about being able to do it, being able to be a person who contributes to that person's quality of life. We have to have a humanised birth, but we also have to have a humanised departure.” (Nurse1-BR)
The lack of preparation and conversation around death was emphasised, with the view that rehabilitation plays a crucial role in helping individuals and families plan for the end of life. One participant emphasised the necessity to conceive of death as an integral component of life, requiring the same consideration and care as birth. “We come from a place where we don't talk about death. We don't plan. Death is like a taboo. So if you're planning your life, you'd better plan your death. So rehabilitation is very important and it's still important until the person dies, because you still have to make sure that they get the best out of life while they're dying, make it as comfortable and pain-free as possible at the end of their lives.” (Nurse1-UK)
Another participant compared how much attention is given to birth planning versus the lack of planning for death, arguing that a similar level of preparation should be devoted to how individuals leave this world: “We spend a lot of time and energy on how people come into this world. You know we have birth plans, we spend nine months talking to women and men about how you want and where your baby will be born. What music you want, what doctor you want, and all that. We don't put half that energy into how we want to leave this world. And we should, because it's the last thing we'll do for ourselves and our loved ones, it's how people go, and it's important for those left behind, because people shouldn't be left clinging to bad experiences, and we can make a difference.” (Nurse5-UK)
A significant shift in perspective among the participants was the recognition that palliative rehabilitation is not focused on death, but rather on supporting individuals to live well until the death.One participant highlighted the misconception that palliative care is inherently depressing, explaining that it is instead about helping people experience a good death and leave behind a meaningful legacy: “I think people are always a bit surprised, they don't know about palliative care. They say: ‘Oh, it must be very depressing’. But it's not depressing. I could be sad sometimes, but it's not depressing, it's a different thing. I love how, even before working in palliative care, I always worried about how people would get to the end of their lives, and how they would die. And I read a lot of Cicely Saunders’ work before and you know, how important it is to die well, so that you leave that legacy for your family, a life and a death well done.” (OT9-UK)
Another participant reinforced the idea that palliative rehabilitation is not merely about dying, but rather about optimising life. “I think I like the fact that strangely enough we've improved the quality of life and probably improved life expectancy. So it's not all gloomy, in fact, it's very little about dying, it's more about living well.” (Nurse3-UK) “Supporting people to live when and while they're dying. (…) Encouraging people to live until they die, whatever that means. Yes, that's the broad meaning of palliative rehabilitation, I think, is to make it easier for someone to live while they're dying, and for them to identify the key things that are important to them, to allow that life process to continue.” (OT6-UK)
The findings reinforces the core philosophy of palliative rehabilitation, which is not about resisting or denying death, but rather about enabling individuals to live fully, in accordance with their values and priorities, supporting life on the road to death.
Theme IV: The challenges regarding rehabilitation in oncological palliative care
The provision of palliative rehabilitation for cancer patients is accompanied by several challenges, which are especially pronounced in developing countries such as Brazil. The barriers to providing adequate care are multifactorial but include limited government funding for healthcare and an insufficient number of healthcare professionals with the necessary skills and training in palliative and oncological rehabilitation. Despite the growing recognition of the value of rehabilitation within palliative care, participants highlighted significant challenges in its implementation across both the Brazilian and United Kingdom healthcare contexts.
In Brazil, the absence of structured services and formalised policies for palliative rehabilitation emerged as a major limitation. One participant emphasised the lack of a comprehensive and integrated approach, stating: “The service isn't structured for such care. We need to have a very broad context of the word team, which has to be integrated, try to talk about the same idea and develop actions”. (Nurse2-BR)
Additionally, the absence of a specific public policy recognising palliative rehabilitation as part of palliative care further exacerbates the challenge. Another participant reflected on how policy recognition could not only improve patient outcomes but also lead to economic benefits: “The lack of a specific public policy on palliative care that includes all possible professionals who can work in some way to maintain quality of life and value this issue of rehabilitation, in other words, to show in the form of a project, in the form of experiences, so that management understands that in addition to bringing quality of life to the patients being cared for, it can increase the economy”. (Nurse1-BR)
In contrast, participants from the United Kingdom did not emphasise policy gaps as a primary barrier. Instead, time constraints and limitations in service availability were more frequently cited, particularly when patients were admitted for short periods: “Sometimes time can be a barrier, especially if they're here for a short period of time, that can be a bit of a challenge. But it can also be the person's expectations, so you kind of have to adapt the programme or the information you're giving them”. (OT7-UK)
It is evident that there are issues related to access and the lack of palliative care services in Brazil, coupled with a shortage of specialists, insufficient patient education and a lack of resources dedicated to this speciality, makes it difficult to provide adequate care, a scenario that differs from the British context.
A lack of education and training in palliative rehabilitation was frequently mentioned by Brazilian participants as a central challenge. Professionals and families often lacked a clear understanding of its role within palliative care, leading to resistance and misconceptions. One participant outlined the foundational steps required before palliative rehabilitation could be widely implemented: “We still have some difficulty, sometimes we hear that rehabilitation in palliative care isn't necessary, it's not the main thing, or, look, it's palliative care, are you going to rehabilitate? or, look, rehabilitation is no longer necessary here (…) we don't have a palliative rehabilitation service, we would need to have a palliative rehabilitation service. But in order to have a palliative rehabilitation service, we first need to start talking about palliative rehabilitation, publishing about palliative rehabilitation, so that maybe we have a team that's open to it, in other words, I miss the basics”. (OT1-BR)
This challenge is further enhanced by the limited incorporation of palliative care in healthcare education, as highlighted by another participant: “I think the main barrier is still the term palliative care itself, it's still something that's been around here in Brazil for some time, but it's still not disseminated in hospitals, it's still not disseminated in undergraduate courses and often what I see as a difficulty is that people don't understand palliative care itself, perhaps rehabilitation, because people think that this patient has nothing to be rehabilitated ‘this patient is going to die’ or people think that the definition is in the concept ‘at the end of life’”. (Nurse5-BR)
Moreover, professional resistance to interdisciplinary work was reported as an additional challenge, as healthcare providers were often reluctant to adopt collaborative models of care: “We need education first, we need funding so that we have a service, we need professionals to be trained and the family needs to understand what rehabilitation in palliative care is, sometimes they don't understand what palliative care is. Professionals are resistant to interdisciplinary work, because they're not used to it”. (Nurse9-BR)
A central barrier identified in both contexts was the perception of rehabilitation as a curative intervention, conflicting with the palliative care philosophy. In the United Kingdom, one participant pointed out that even the term “rehabilitation” itself can create confusion or resistance among professionals and patients: “I think part of that is the word rehabilitation”. (Nurse5-UK)
Similarly, another UK participant reflected on how patients’ fears and expectations about hospice and palliative care can act as a barrier to engagement with rehabilitation services: “There are those patients who, when they hear the word hospice, or palliative care, think it's the end of their life, so they don't want to be empowered themselves, I think they want to be looked after, or they've reached a point where they're actually totally fed up, they don't want to be independent any more”. (OT5-UK)
This underscores an important cultural challenge, whereby patients and families may not always be receptive to rehabilitation efforts, particularly if they align palliative care with end-of-life care rather than quality-of-life enhancement.
Similar misconceptions were evident in Brazil, with families sometimes actively discouraging rehabilitation efforts in favour of complete rest and dependency: “I think the biggest barrier is when the family doesn't allow us to work completely, when they really believe that the best thing for the patient is to be doing for him, to leave him without work, to leave him just resting”. (OT5-BR)
This reflects a fundamental gap in understanding rehabilitation's role in maintaining dignity and autonomy, rather than contradicting the palliative approach.
The findings highlight several key challenges in implementing palliative rehabilitation across both the Brazilian and UK contexts. In Brazil, structural and policy limitations, a lack of education and training, and resistance from professionals and families were the predominant barriers. In the United Kingdom, while services were more established, challenges arose from time constraints, misconceptions around the word ‘rehabilitation’, and patients’ reluctance to engage with rehabilitative interventions.
Discussion
Findings showed a divergence between Brazil and the United Kingdom in how rehabilitation in palliative care is conceptualised and implemented in these countries. Brazilian participants had limited familiarity with rehabilitation in palliative care and its end-of-life applicability, while professionals in the United Kingdom integrated rehabilitative principles into practice. This reflects structural, educational and cultural differences in service delivery. The importance of integrating rehabilitation into palliative care has gained increasing attention globally.5,6,19–23
From a theoretical perspective, this integration can be conceptualised in terms of the fundamental goals of palliative care and rehabilitation, through a holistic approach that highlights the interdependence of maintaining function, independence, quality of life and control as priorities perceived for patients with life-limiting conditions. 8 This aligns with a constructivist view in which patients’ lived experiences and individual priorities shape the meaning and goals of rehabilitation within palliative care. 13 Despite demonstrated benefits, this integration remains limited and inconsistent. 24 Evidence supports that rehabilitation is compatible with palliative care and that integration represents best practice. 9
The implementation of rehabilitation within palliative care systems differs across countries. In Brazil, the National Palliative Care Policy (PNCP-SUS) was approved in 2024 within the Unified Health System (SUS), aiming to strengthen palliative care services. 25 However, the policy does not mention rehabilitation, indicating a critical gap that may hinder awareness of rehabilitative strategies. 26 In contrast, the United Kingdom has increasingly integrated rehabilitation into palliative care, exemplified by the clinical guideline ‘Rehabilitative Palliative Care: a challenge for the twenty-first century’, marking a step forward in service innovation in the British health system. 10
New palliative rehabilitation services are increasingly developed in the United Kingdom. 27 Hospices are widely implemented as integral models of palliative care, often incorporating rehabilitation to enhance patients’ quality of life. 28 These services provide outpatient and community-based rehabilitation, using trained volunteers to increase patient access, 29 as reflected in British participants’ perspectives. In Brazil, the lack of a structured hospice model limits comprehensive palliative rehabilitation. Most initiatives are concentrated in few regions and are rarely integrated with rehabilitation teams. 30 This reflects broader differences in health system maturity, workforce development, and public health governance. Bridging these gaps will require coordinated action across research, professional education, policy formulation, and service planning to ensure rehabilitation is recognised as an essential dimension of palliative care. 9
The contrast between the United Kingdom and Brazil highlights systemic disparities. While the British model has progressively adopted an interdisciplinary, person-centred model recognising rehabilitation as fundamental to palliative care,10,11 Brazil lacks clear guidelines and infrastructure. 25 Addressing this requires coordinated strategies across education, policy, research and public awareness, ensuring that palliative care encompasses not only symptom control and psychosocial support but also access to rehabilitation, which promotes autonomy, functionality and quality of life until the end of life throughout the end-of-life trajectory. 9
Another important finding concerned the barriers to integrating rehabilitation into palliative care, including structural limitations, professional resistance and misconceptions about its role at the end of life. For some participants, especially in Brazil, promoting rehabilitation and functionality at end-of-life seemed inappropriate. Limited exposure, structural constraints, and lack of training likely shaped these perceptions. Despite these barriers, there was convergence in recognising the potential benefits of integrating rehabilitation and palliative care. Participants consistently highlighted shared professional values: promoting autonomy, dignity, quality of life, symptom management, client-centred care and continuity throughout the illness trajectory. This perspective resonates with literature advocating person-centred models that incorporate rehabilitation into palliative care frameworks, particularly among UK participants.5,6,10,11,20–23
The interface between palliative care and rehabilitation is not a new concept, but its relevance is increasingly recognised. Rehabilitation in oncology, first described by Dietz in 1969, includes preventive, restorative, supportive and palliative models.12,31 Our findings indicate that a lack of conceptual clarity regarding rehabilitation in palliative care may hinder professional engagement, echoing Harding et al.5,6 Furthermore, an observation was made regarding the inconsistency in the terminology employed, with the utilisation of various terms, including ‘palliative rehabilitation’, ‘rehabilitative palliative care’ and ‘rehabilitation in palliative care’. Despite this, all definitions share core principles: supporting life through decline and death, symptom management and enhancing quality of life.5,6,12,32 The absence of a consensus definition and standard terminology remains a key barrier in the field. Further research is required to develop a consensus definition and standardised outcomes, to determine optimal models of palliative rehabilitation, including resources, interventions and appropriate settings, particularly in low- and middle-income countries such as Brazil.5,6,12,24,32–34
Barriers to integrating rehabilitation into palliative care for cancer patients include structural limitations, professional resistance, misconceptions about rehabilitation at the end of life, and cultural differences between Brazil and the United Kingdom. Overcoming these challenges requires a multifaceted approach including policy development, interdisciplinary education and a shift in perceptions to ensure rehabilitation is recognised as a palliative care component.10,12 Education should target both palliative and rehabilitation professionals to foster mutual understanding of each discipline's role and the benefits of integration. These steps are essential to guarantee equitable access to rehabilitation and palliative care, enabling patients to achieve optimal quality of life and dignity. 24
The findings reveal significant conceptual and structural disparities in how rehabilitation is understood and delivered within palliative care across the two countries. This underscores the need to clarify definitions, establish unified conceptual models, and invest in policies and professional training to ensure rehabilitation is viewed not as contradictory, but as complementary to palliative care goals. Rehabilitation and palliative care should be seen as integrated strategies, working together to preserve autonomy, dignity and engagement in life for people with advanced disease.
The study captured healthcare professionals’ perceptions, challenges and barriers, providing insights often overlooked in quantitative research. However, limitations include the focus on nurses and occupational therapists, which may omit perspectives from other disciplines involved in palliative care and rehabilitation. The qualitative design does not allow generalisation but offers in-depth understanding of meanings and practices. Future research should investigate the development, implementation and evaluation of evidence-based palliative rehabilitation models, particularly in low- and middle-income countries, including patient and family perspectives, cost-effectiveness, and clinical outcomes, to support adoption of integrated care approaches.
Supplemental Material
sj-doc-1-cre-10.1177_02692155251387314 - Supplemental material for Rehabilitation in oncological palliative care, does it exist? A qualitative and multicentre study of healthcare professionals’ perceptions
Supplemental material, sj-doc-1-cre-10.1177_02692155251387314 for Rehabilitation in oncological palliative care, does it exist? A qualitative and multicentre study of healthcare professionals’ perceptions by Gabriela Rezende, Gabriel Morais Xavier dos Santos, Ingrid Bacon and Marysia Mara Rodrigues do Prado De-Carlo in Clinical Rehabilitation
Footnotes
Acknowledgements
The authors wish to thank the healthcare assistants who participated in this study. Their contribution was greatly appreciated given the demands on their time. They also would like to express thanks to the clinicians, managers and research staff who facilitated recruitment to the study.
ORCID iDs
Ethical approval
Ethics approval and consent to participate approval was granted by the University of São Paulo (number 21189919.0.0000.5393) and Kingston University Research Ethics Committee (number 1468) on 5 May 2020.
Informed consent
Verbal and written consent was provided by participants.
Consent for publication
Participants provided consent to be quoted in publications.
Author contributions
GR conceived the original idea of the project, organisation of sources and analysis, elaboration of the text, correction and final revision. GMXS was involved in organisation of sources and analyses, elaboration of the text. IB contributed to the design of the study, analyses and final revision. MMRPDC conceived the original idea of the project and obtained funding, correction of the text and final revision. All authors participated in the interpretation of the data, revised the manuscript critically for important intellectual content and approved the final version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors disclosed the financial support for the research, by the Brazilian Federal Agency for Support and Evaluation of Graduate Education (CAPES), in the scope of the Program CAPES-PrInt (process number 88887.371124/2019-00).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Availability of data and materials interviews contain personally identifiable information. To access please contact the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.