
Abstract
Objective
To examine to what extent the Bern Ambulatory Interprofessional Rehabilitation results in statistically significant and clinically meaningful changes in self-rated quality of and satisfaction with occupational performance, health-related quality of life, pain intensity, and burden of suffering of persons with chronic pain.
Design
Registry-based longitudinal cohort study.
Setting
Department of Rheumatology and Immunology at the Bern University Hospital, Switzerland.
Participants
A total of 172 participants with chronic musculoskeletal pain.
Intervention
The Bern Ambulatory Interprofessional Rehabilitation is a biopsychosocial intervention for persons with chronic pain.
Main measures
Canadian Occupational Performance Measure, Pictorial Representation of Illness and Self Measure, European Quality of Life and Health Measure Visual Analogue Scale, and Visual Analogue Scale for pain intensity.
Results
Changes over time were statistically significant and clinically meaningful for quality of occupational performance (post-treatment p ≤ 0.001, 95% confidence interval (CI) [1.62–2.31], d = 0.8; follow-up p ≤ 0.001, 95% CI [1.23–2.20], d = 0.70), satisfaction with occupational performance (post-treatment p ≤ 0.001, 95% CI [2.35–3.22], d = 0.95; follow-up p ≤ 0.001, 95% CI [1.95–3.14], d = 0.87), burden of suffering (post-treatment p ≤ 0.001, 95% CI [0.25 to −0.42], d = 0.61; follow-up p ≤ 0.001, 95% CI [0.20–0.40], d = 0.55), and health-related quality of life (post-treatment p ≤ 0.001, 95% CI [6.30–15.66], d = 0.43; follow-up p ≤ 0.001, 95% CI [3.08–15.28], d = 0.36). Changes for pain intensity were not statistically significant nor clinically meaningful (post-treatment p = 0.676, 95% CI [−3.85 to 5.45], d = 0.03; follow-up p = 0.243, 95% CI [−8.91 to 1.72], d = −0.09).
Conclusions
This study confirms the short- and mid-term effectiveness of the Bern Ambulatory Interprofessional Rehabilitation on occupational performance, burden of suffering, and health-related quality of life of persons with chronic pain.
Keywords
Introduction
Chronic pain significantly contributes to the global burden of disease. 1 In Europe, the prevalence of chronic pain in the adult population is 27% and is associated with high population costs. 2 Researchers empathize the need to prioritize chronic pain in healthcare and policy.1,2 In the International Classification of Diseases 11th Revision (ICD-11) chronic pain is now recognized as a disease in its own right and is defined as ‘persistent or recurrent pain lasting longer than 3 months’ 2 (p.1004) and acknowledges its biopsychosocial dimensions. 3
Chronic pain is associated with significant emotional distress and functional disability, 4 and reduced health-related quality of life.5,6 Persons with chronic pain experience limitations in occupational performance,6,7 along with difficulties in performing activities of daily living. 8 Serious problems in performing usual activities are associated with lower self-reported health in persons with chronic pain. 6 Further, persons with chronic pain have difficulties in their participation in work, society, and family. 5
Interprofessional multimodal interventions are recommended for chronic pain treatment.9,10 These best practice interventions focus on goals regarding pain management, participation, and increasing quality of life and well-being, rather than solely addressing pain reduction.9,11 A systematic review showed that interprofessional multimodal programmes significantly improved well-being. 9 A Cochrane review of interprofessional biopsychosocial programmes confirmed positive effects on disability and return to work. 12 Several studies reported improvements in occupational performance following pain management programmes.13,14 However, the findings concerning the effect on pain intensity remains inconstant, with some studies showing no effect,11,15,16 while the Cochrane review reported significant reduction of pain intensity. 12
The Bern Ambulatory Interprofessional Rehabilitation (BAI-Rehabilitation) was developed according to evidence-based practice and international guidelines. Research supports its effectiveness on self-perceived health status, return to work, functional capacity, observed task performance in activities of daily living, self-rated occupational performance, and burden of suffering.11,17,18 Previous studies on the BAI-Rehabilitation investigated rather small samples and missed the focus on occupational performance as the main outcome. Thus, this study aims to examine to what extent the BAI-Rehabilitation results in statistically significant and clinically meaningful changes in self-rated quality and satisfaction with occupational performance, health-related quality of life, burden of suffering, and pain intensity in persons with chronic musculoskeletal pain. We hypothesized that participants show improvements in quality and satisfaction with occupational performance, health-related quality of life, and burden of suffering after participating in the BAI-Rehabilitation.
Method
Study design and setting
This is a registry-based longitudinal cohort study with a quantitative design. The Ethics Review Board Bern, Switzerland gave ethical approval for the research project of the Clinic of Rheumatology and Immunology (Project-ID: 2018-01583). Participants of the study agreed either to a general informed consent of the University Hospital of Bern, allowing the use of data for research purposes, or to a specific consent for research projects concerning the registry.
The study took place in Switzerland at the Department of Rheumatology and Immunology at the University Hospital of Bern. The clinic provides inpatient and outpatient medical and rehabilitation services for persons with rheumatic diagnoses, including chronic musculoskeletal pain. The interprofessional team consisting of occupational therapists, physiotherapists, psychologists, social workers, nurses, and physicians assessed and treated the participants. In total, approximately 620% full-time equivalents of the above-mentioned health professionals work for the BAI-Rehabilitation, with an additional 70% full-time equivalents dedicated to its research. Following the approval of cost coverage by the health insurance of the participant, the expenses for each component of the intervention are reimbursed according to the official local tariffs. The BAI-Rehabilitation programme offers groups of three to seven participants approximately 10 times per year.
Participants and sample
Participants of this study took part in the BAI-Rehabilitation. The above-described interprofessional team interviewed and assessed participants for suitability during a 3-day inpatient setting. Diagnosis criterion for inclusion is a chronic musculoskeletal pain syndrome according to ICD-10 diagnosis criteria 19 with indicators of significant impairment in psychosocial functions; participants with a primary mental disorder were excluded. Further inclusion criteria were age over 18 years, consensus for participation among the entire team and the participant, and prior participation in a mono-professional intervention with insufficient effects. Exclusion criteria were insufficient physical or psychological capacity, limited skills to participate in group discussions in German, and ongoing legal investigation about health insurance benefits.
Data collection
Data collection took place between May 2018 and the end of 2022. Data were collected at three measurement points and recorded in the registry. Baseline data collection took place during the 3-day assessment before the start of the BAI-Rehabilitation. Post-treatment data collection took place in the last week of the Rehabilitation programme after 3 months. Follow-up data collection took place 12 months after the baseline. For baseline and post-treatment, occupational therapists treating participants in the BAI-Rehabilitation assessed the Canadian Occupational Performance Measure (COPM) and Pictorial Representation of Illness and Self Measure (PRISM) through an interview and entered it into the registry. For the 12-month follow-up participants completed a questionnaire for the COPM and PRISM by mail. Participants entered the data for the visual analogue scale (VAS) for pain intensity and European Quality of Life visual analogue scale (EQ-VAS) directly into the registry through an electronic questionnaire at all measurement points. Data were extracted from the registry anonymously following the guidelines of the registry.
Intervention
The BAI-Rehabilitation is an interprofessional outpatient intervention of 12 weeks. Previous studies described the programme and investigated its effectiveness.11,17,18 The programme consists of individual and group therapies, from the above-mentioned healthcare professionals. The overall goals of the programme are the improvement of quality of life and to support the process of returning to work. At the beginning of the programme, the participants define individual goals with the treatment team. Interprofessional meetings and goal meetings together with the participants take place monthly to review goals and adjust the intervention. Table 1 provides details about the content and duration of the interventions of the BAI-Rehabilitation.
Content and duration of the BAI-Rehabilitation.
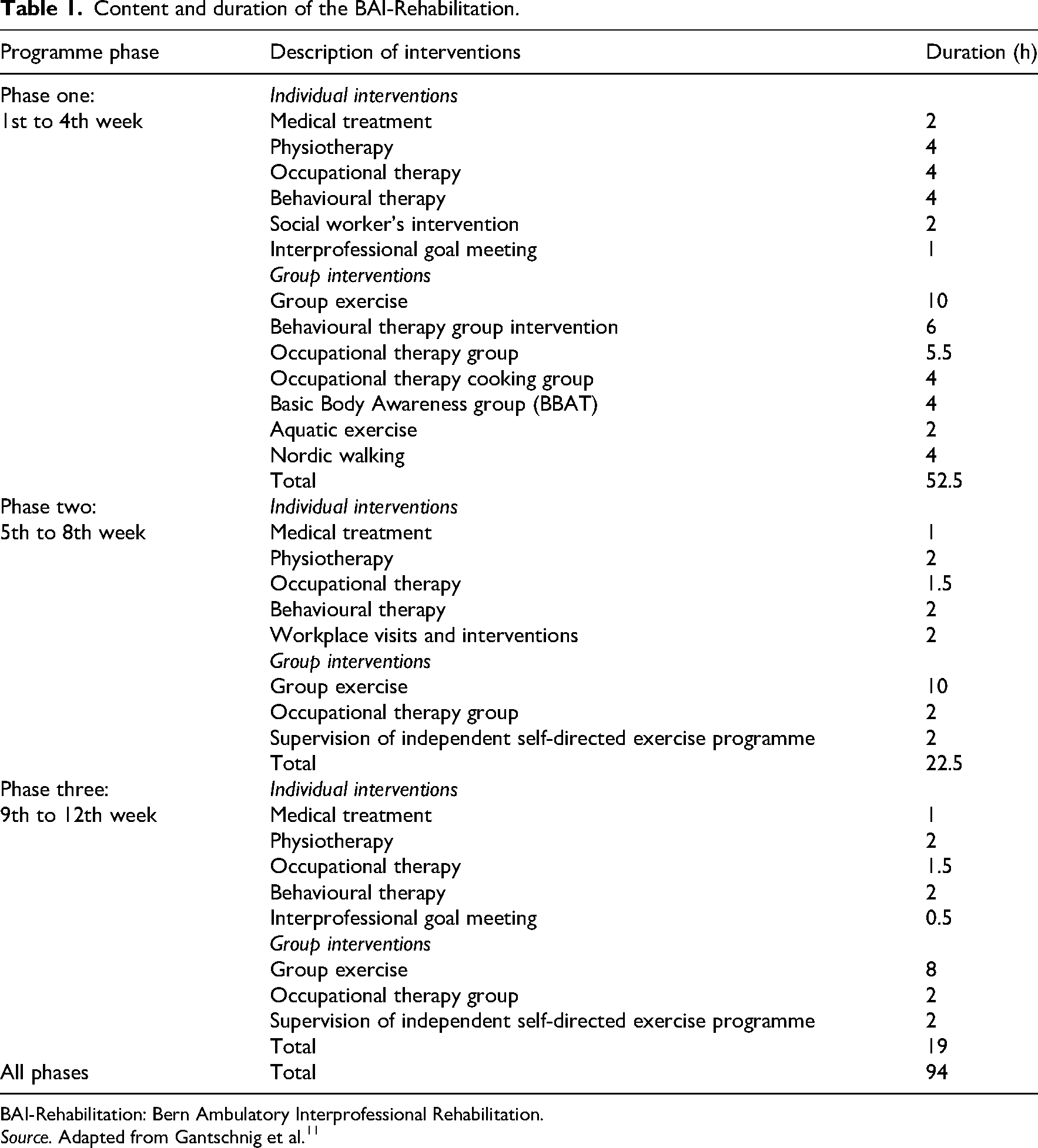
BAI-Rehabilitation: Bern Ambulatory Interprofessional Rehabilitation.
Source. Adapted from Gantschnig et al. 11
The programme is divided into three phases, each lasting 4 weeks. The first phase is the intense phase during which therapy takes place 3 days per week. Phases two and three are characterized by the increasing competence of participants. While the time for the intervention through health professionals decreases, there is more time for independent self-directed exercises (see Figure 1). Usually, participants gradually start to work and are on part-time sick leave. During this period, an occupational therapist assesses the workplace, discusses the re-entry to work with the employer and the participant, and recommends work adaptations for the workplace. Besides therapies, participants are instructed on independent self-directed exercises. During the programme, participants are requested not to participate in other interventions concerning chronic pain.
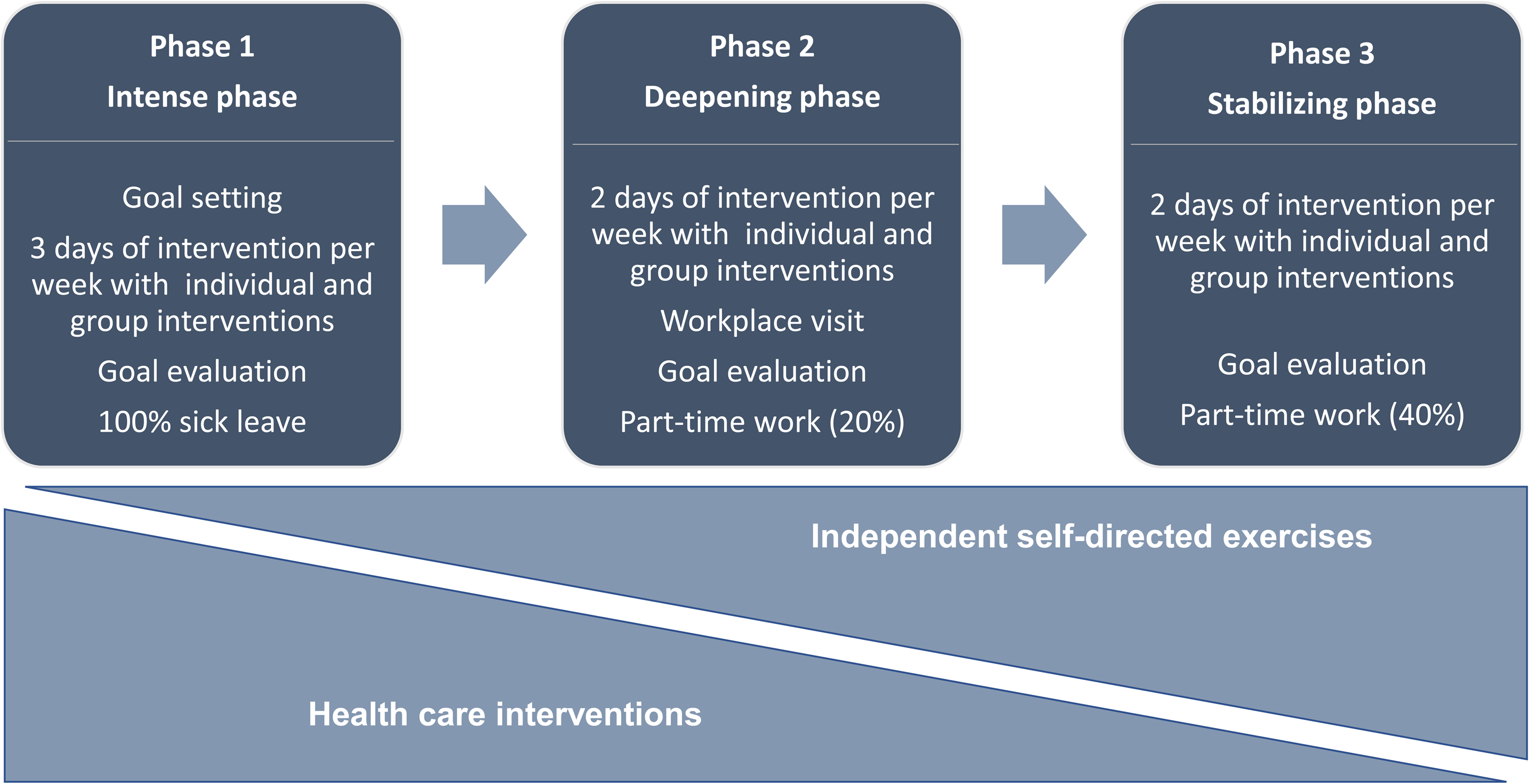
The procedure of the BAI-Rehabilitation. BAI-Rehabilitation: Bern Ambulatory Inter professional Rehabilitation.
Outcome measurements
Individuals’ perspectives on diseases, their impact on daily life, and their treatments become more important in clinical practice and research. 20 Person-reported outcomes are crucial to investigate the effectiveness of interventions for pain. 20 Persons with chronic pain report a wide range of problems in their occupations. 7 The COPM acts as a useful tool to identify relevant problems and is a person-centred outcome measure to evaluate the performance of those occupations that are the most important to the individual. 7 Therefore, the main outcome of this study is occupational performance. Secondary outcomes are the burden of suffering, health-related quality of life, and pain intensity, reflecting goals of the intervention programme.
Primary outcomes
The COPM is a person-centred assessment that is used to identify, prioritize, and evaluate individual problems in important occupations. 21 It focuses on self-rated occupational performance in all areas of life, including self-care, leisure, and productivity. The self-rated assessment is used to evaluate participants’ perception of the quality and satisfaction of occupational performance over time. 21 The COPM is divided into two sub-scale scores: quality of performance (COPM-P) and satisfaction with performance (COPM-S). 21 In the semi-structured interview conducted by an occupational therapist, up to five problems are selected as the most important. 21 Then, the person rates each problem using a 10-point Likert scale. 21 One means that the person is not able to do the occupation or not satisfied with the performance at all; 10 means that the person can do it extremely well or is extremely satisfied with the performance. 21
Studies underlined the validity of the use of the COPM in the context of persons with pain. 7 The COPM showed high sensitivity to change after an interprofessional pain management programme.7,22 Suggested thresholds for the determination of a relevant change are 1.37 for quality of occupational performance, and 1.90 for satisfaction with occupational performance. 22
Secondary outcomes
The PRISM is an instrument for visualizing and measuring the self-perceived burden of suffering due to illness. 23 In this study, occupational therapists used the assessment to measure the burden of suffering due to chronic pain. The distance between the Self and the Pain measured in centimetres provides the quantitative measure of the burden of suffering and is called the ‘Self-Illness Separation’. The smaller the distance, the higher the burden of suffering. 23 The PRISM is validated for measuring the burden of suffering in persons with chronic non-cancer pain and evidence supports the use of the instrument as an outcome measure of interventions. 24 Studies confirmed a high validity and reliability of the PRISM.23,24
The EuroQoL (European Quality of Life measure) is a standardized outcome measure for self-perceived health status. 25 The EuroQoL includes a short questionnaire with an index with five items (EQ-5D) and a visual analogue scale (EQ-VAS). 26 The EQ-VAS is more sensitive to detect mild impairments in the self-perceived health status in comparison with the EQ-5D. 27 Consequently, for this study, the EQ-VAS was used as the outcome measure for health-related quality of life. The EQ-VAS measures the individual's perception of their overall health. 26 The EQ-VAS is a 20 cm-long vertical scale with 100 points. 27 Individuals record their current self-perceived health status, 0 points mean the ‘worst imaginable health status’, and 100 points stand for the ‘best imaginable health status’. 26 Evidence supports the validity of the EuroQoL for chronic low back pain. 25 Research suggests to interpret a difference in scores between 7 and 10 points as a clinically meaningful change. 28
We used a 0–100 VAS to assess pain intensity. Participants rated their pain intensity by making a mark on a 100 mm line corresponding to their pain intensity; 0 mm stands for ‘no pain’; and 100 mm stands for the ‘most intense pain imaginable’.29,30 In this study, participants rated their pain of today. Previous research reported low-quality evidence for the content validity of the VAS and therefore critically question the use of the VAS to measure pain intensity. 29 However, in the core outcome domain set to assessing the effectiveness of interprofessional pain therapy the use of a measure to detect pain intensity is recommended. 30 Literature suggests 20 mm as minimal clinically meaningful change for persons with chronic low back pain. 30
Bias
The first author of this study was partly involved in the intervention of the BAI-Rehabilitation, as an occupational therapist, in data collection, and in controlling the data in the registry. Thereby, we include both a clinical and theoretical perspective in this research project. The first author of this study is aware of this position and possible bias, reflected, and addressed this topic in each step of the research process with her co-authors. Through data tracking in software Redcap, access and change in the data in the registry are documented.
Statistical analysis
Descriptive statistics provided demographic information about the sample of participants. We tested data for normal distribution for each dependent variable for all time points. Data of the outcome variable PRISM were not normally distributed, and where transformed by applying a log transformation to achieve a normal distribution. The level of the data of the outcome variables is not equivalent to an interval scale due to the limitations of the self-rated Likert scale and the unequal distances between the values. However, data from Likert scales can be analysed as interval data if they are normally distributed. 31 Furthermore, several previous studies treated data from the COPM as interval scaled for their analysis.14,32
The structure of the data led to the choice of a linear mixed-effects model for the analysis. We pre-defined two primary and three secondary outcomes. Cases with missing data due to incomplete measures or missing a measurement time point were maintained in the dataset for the analysis due to the assumption of missing at random. 33 Therefore, a larger sample could be analysed, which leads to increased precision of the estimates and statistical power. 33
To fit the linear mixed model, we compared different models with Akaike's information criterion. Graphical procedures and statistical tests proved the assumptions underlying the model (i.e. linearity, homoscedasticity, normality of residuals, absence of multicollinearity, normality of the random slope, and constant). 33 The final model included measurement points as a repeated effect, a constant and time as fixed effects, and a constant, subject and time as random effects.
We used IBM Statistical Package for Social Sciences (SPSS) version 25.0 software to analyse the data. To determine statistical significance a level of α = 0.05 was assumed. 34 We did not adjust for multiple testing, and we report all p-values unadjusted. The size of the effect d was interpreted as small (d = 0.2), medium (d = 0.5), or large (d ≥ 0.8). 35 To interpret clinical meaningfulness a threshold for each outcome measure was previously defined according to the literature. No study about clinically meaningful change for the PRISM was found.
Results
The analysis for this study included data from 172 participants with a chronic pain diagnosis. Recruitment for the registry took place from May 2018 to September 2022. Figure 2 presents the flowchart of participant inclusion and process. Participants reported the socio-demographic data at baseline, summarized in Table 2. The age of participants ranges between 19 and 77 years (mean 43.40, standard deviation (SD) 11.01).
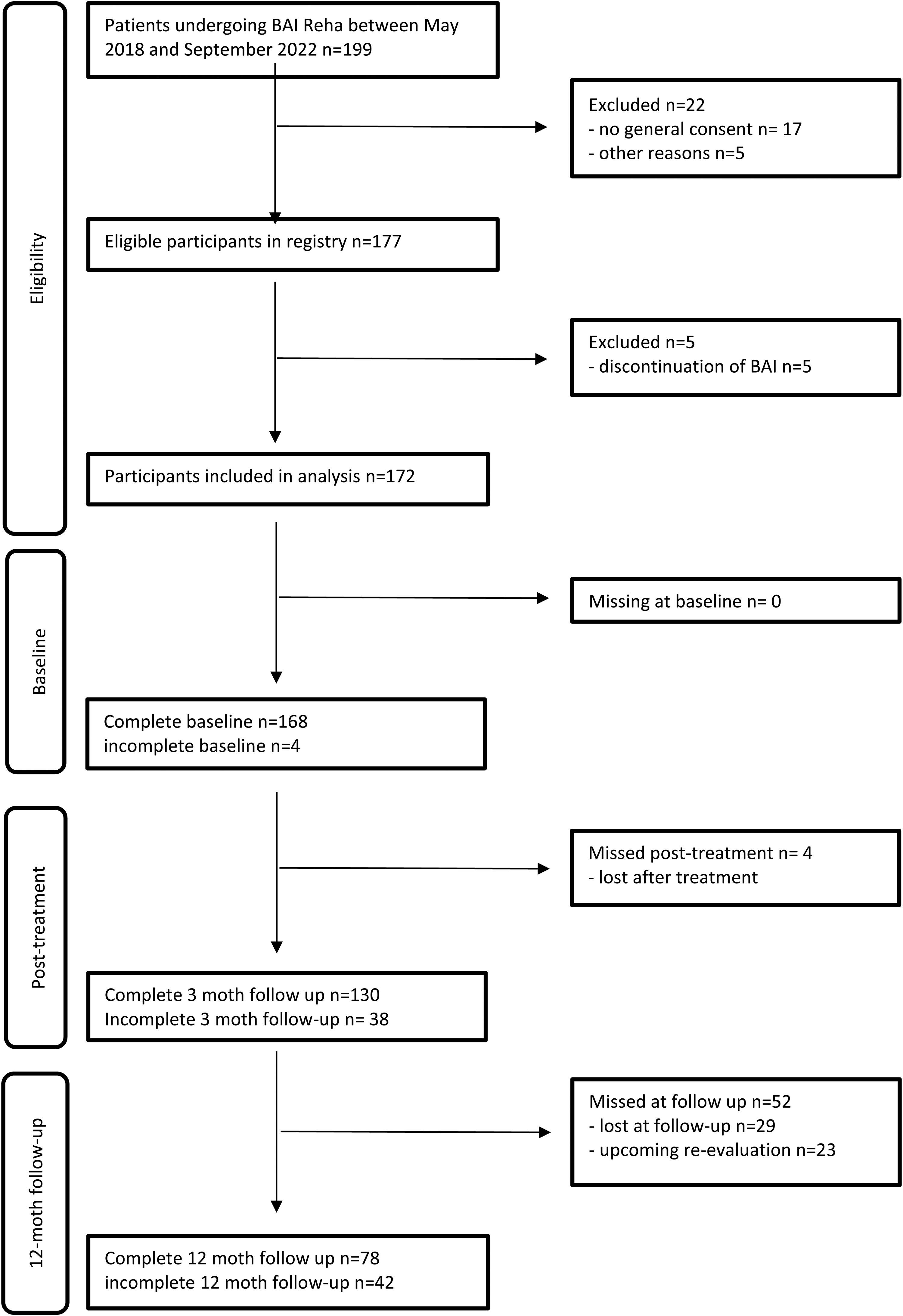
Flowchart of participants.
Sociodemographic characteristics of participants at baseline.
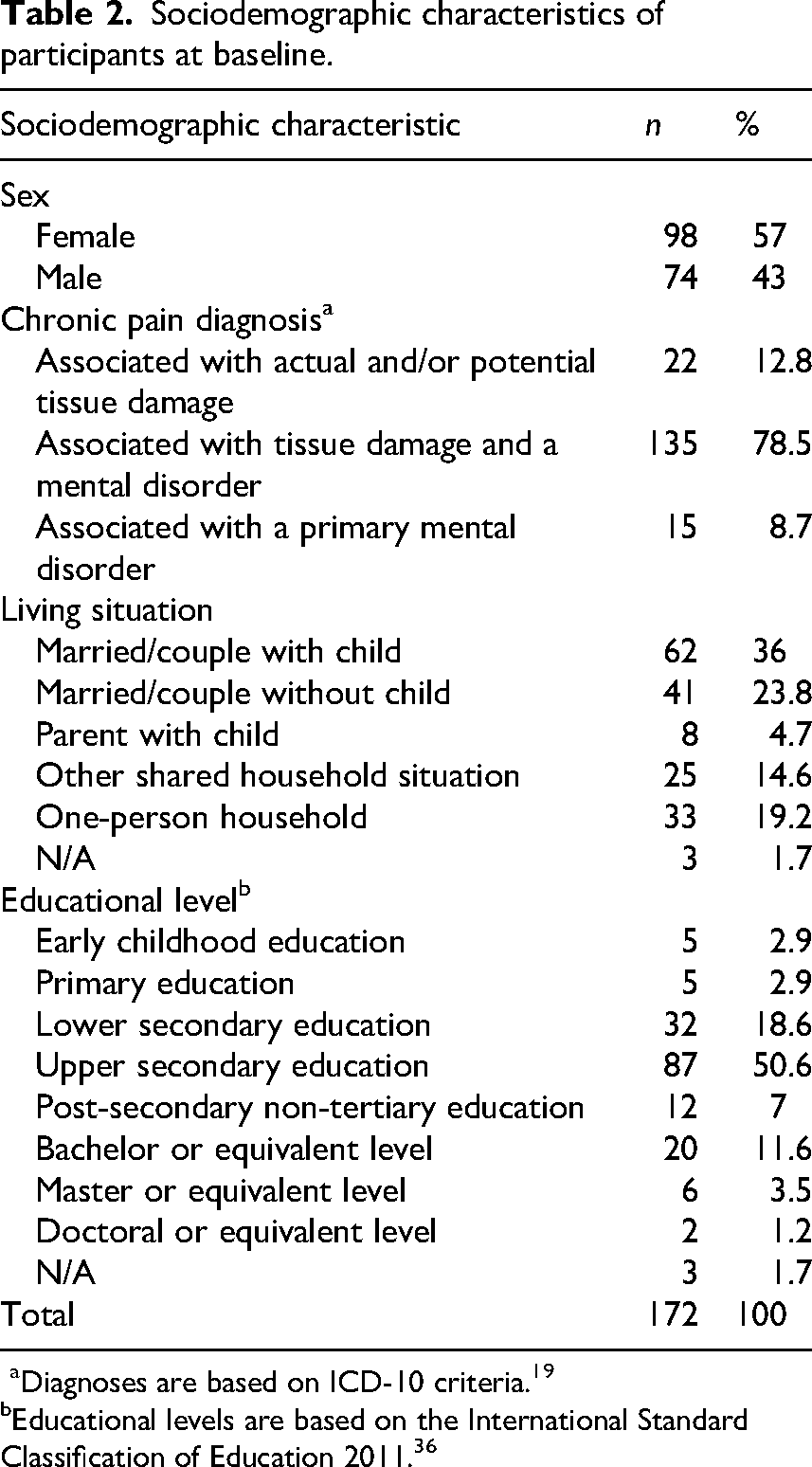
aDiagnoses are based on ICD-10 criteria. 19
Educational levels are based on the International Standard Classification of Education 2011. 36
Primary outcomes
The linear mixed model analysis showed a significant change over time in the primary outcome variables quality of occupational performance and satisfaction with performance post-treatment (p ≤ 0.001) and at 12-month follow-up (COPM-P p ≤ 0.001; COPM-S p ≤ 0.001). We found a clinically meaningful change after the BAI-Rehabilitation in the quality of occupational performance and satisfaction with performance post-treatment (mean change COPM-P 1.96; COPM-S 2.78) and after 12 months (mean change COPM-P 1.71; COPM-S 2.54). The effect size for COPM-P showed a large effect post-treatment (d = 0.8) and a medium effect after 12 months (d = 0.7). The effect in the COPM-S was large post-treatment (d = 0.95) and after 12 months (d = 0.87). Table 3 presents the detailed results for both primary and secondary outcomes. Change over time is graphically shown in Figures 3 to 5.
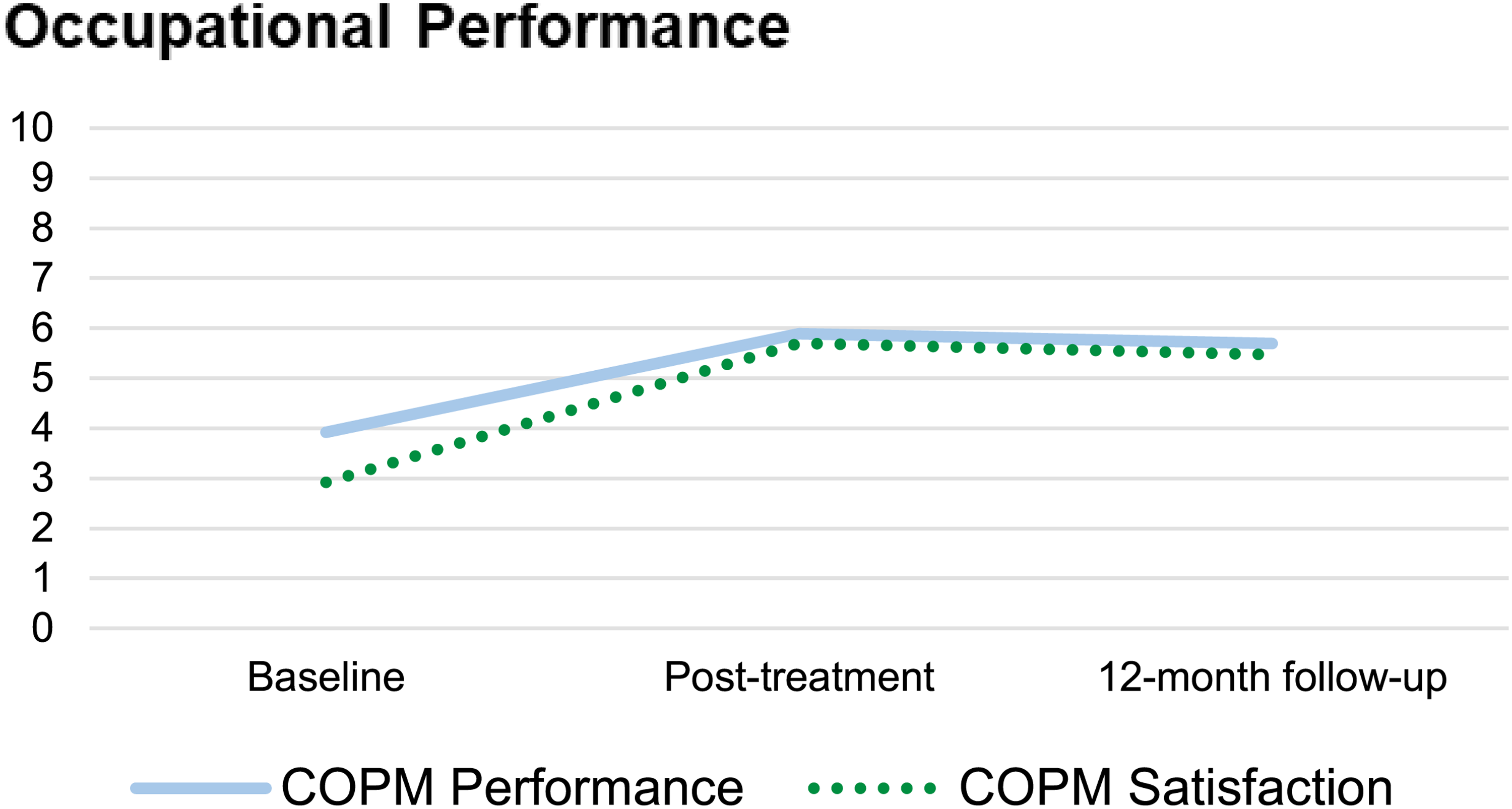
Change of the mean value over time for the occupational performance. Note. N = 172. Error bars represent 95% confidence intervals. COPM: Canadian Occupational Performance Measure.
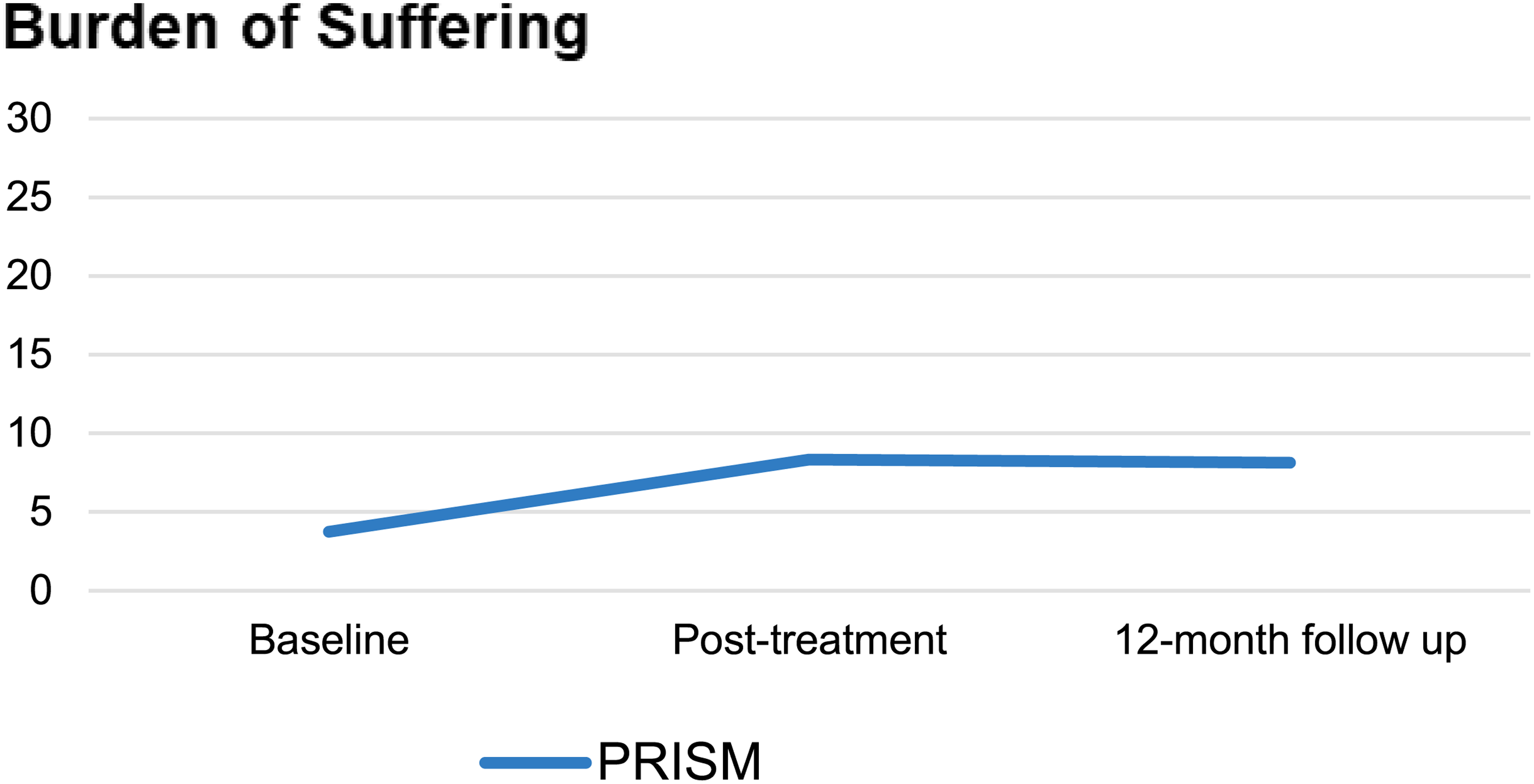
Change of the mean value over time for the burden of suffering. Note. N = 172. Error bars represent 95% confidence intervals. PRISM: Pictorial Representation of Illness and Self Measure.
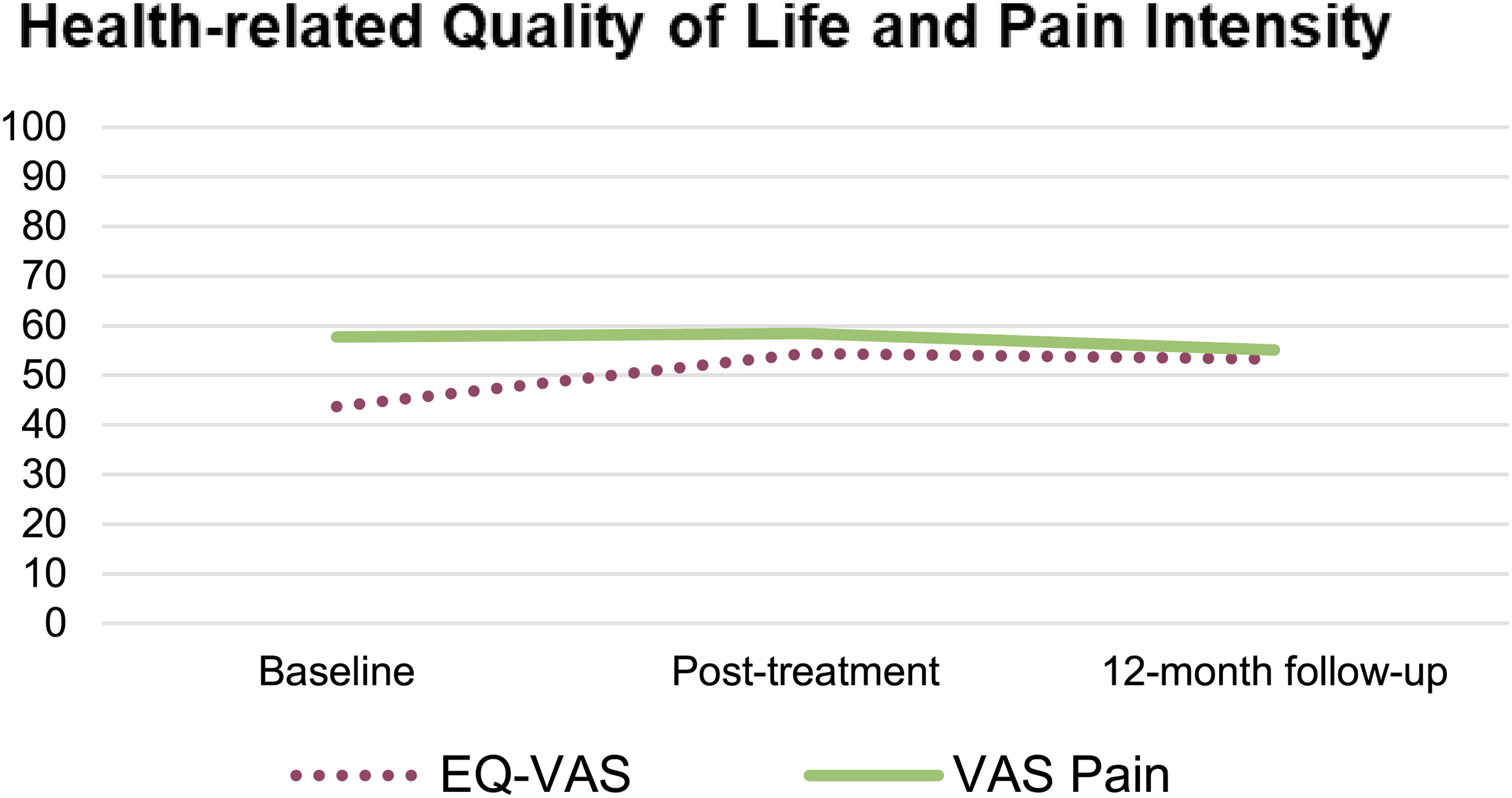
Change of the mean value over time for the health-related quality of life and pain intensity. Note. N = 172. Error bars represent 95% confidence intervals. EQ-VAS: European Quality of Life visual analogue scale; VAS Pain: visual analogue scale pain.
Mean and change over time in dependent variables.
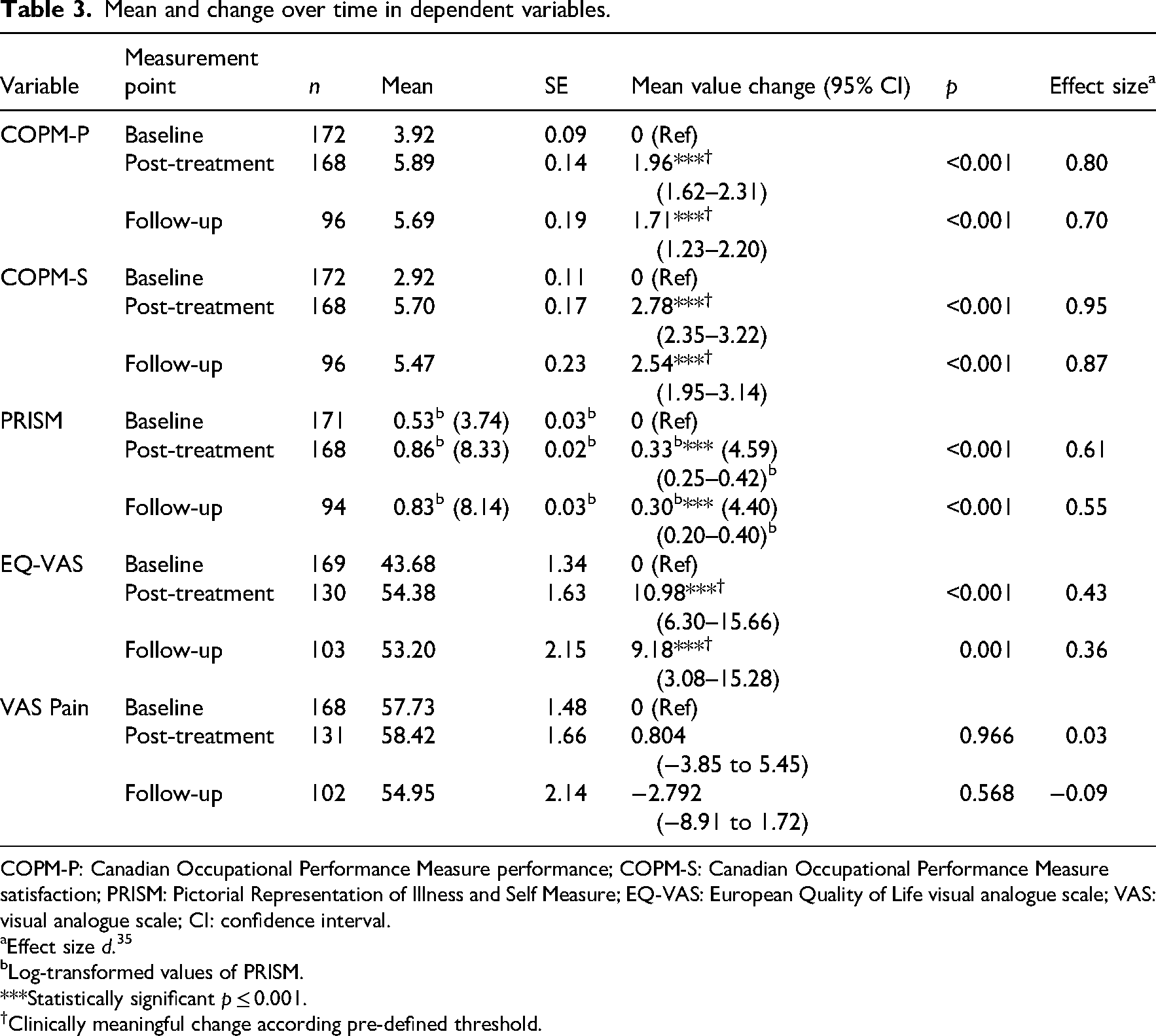
COPM-P: Canadian Occupational Performance Measure performance; COPM-S: Canadian Occupational Performance Measure satisfaction; PRISM: Pictorial Representation of Illness and Self Measure; EQ-VAS: European Quality of Life visual analogue scale; VAS: visual analogue scale; CI: confidence interval.
Effect size d. 35
Log-transformed values of PRISM.
***Statistically significant p ≤ 0.001.
Clinically meaningful change according pre-defined threshold.
Secondary outcomes
The secondary outcome variables PRISM and EQ-VAS showed significant time effects post-treatment (PRISM p ≤ 0.001, EQ-VAS p ≤ 0.001) and at 12-month follow-up (p ≤ 0.001). The PRISM showed a mean change of 4.59 post-treatment (d = 0.61) and 4.40 after 12 months (d = 0.55), which is a medium effect. The effect in the EQ-VAS was small and reached the threshold for a clinically meaningful difference post-treatment (mean change 10.98; d = 0.43) and after 12 months (mean change 9.18; d = 0.36). The pain intensity did not significantly change over time (post-treatment p = 0.676; 12-month follow-up p = 0.243).
Discussion
The results support the short- and mid-term effectiveness of the BAI-Rehabilitation in enhancing quality and satisfaction with occupational performance, reducing the burden of suffering and improving quality of life. These findings are aligned with previous research on the BAI-Rehabilitation.11,17,18 Furthermore, improvements in occupational performance are consistent with results from other studies on pain rehabilitation programmes.14,32 Overall, this study adds to previous findings and confirms the effectiveness of interprofessional rehabilitation in enhancing occupational performance in persons with chronic pain.
This study detected differences in the extent of change in the quality of occupational performance and satisfaction with occupational performance. Both scores reached the threshold for a clinically meaningful change, but the satisfaction score maintained a large effect size up to 12 months, while the performance score showed a large effect post-treatment and a medium effect at 12 months. The greater improvement in the satisfaction score compared to the performance score is consistent with previous studies.14,22 There are several possible explanations for this result. These differences might be due to improved adaptation skills, coping strategies, and acceptance of the life situation. 14 This indicates that satisfaction with performance may better address the outcome of pain management programmes, which focus on pain management strategies. However, caution is needed when interpreting satisfaction scores, as it is unclear whether they measure a distinct construct form performance scores.7,22 Performance and satisfaction scores were highly correlated with previous studies,7,14,22 leading to the hypothesis of a potential relationship between the quality of performance and satisfaction with performance. 7
This study showed statistically significant and clinically meaningful improvements in health-related quality of life and burden of suffering after the BAI-Rehabilitation at the 12-month follow-up. These findings indicate an improved overall health status 26 and a reduced burden of suffering 23 for persons with chronic pain. These findings confirm previous research on the BAI-Rehabilitation.11,17,18 Similarly, Elbers et al. 9 showed that that interprofessional multimodal programmes led to long-term improvements in physical and psychological well-being.
In the present study, no significant improvements in pain intensity were found after the BAI-Rehabilitation. Research on pain management programmes reported inconsistent outcomes regarding pain intensity. A previous study on the BAI-Rehabilitation also found no evidence of changes in pain intensity. 11 Other studies on pain management programmes reported similar results.15,16 However, a Cochrane review concluded that biopsychosocial rehabilitation programmes for chronic back pain led to a reduction in pain intensity. 12 Indeed, numerous studies investigating multimodal rehabilitation programmes for chronic back pain reported reductions in pain intensity.37–39 The underlying causes for this discrepancy are unclear. A possible explanation may be differences in inclusion criteria: Kamper et al. 12 focused on chronic back pain, while the present study included participants with any chronic musculoskeletal pain conditions. Morone et al. 39 excluded participants with rheumatological diagnoses and mental health diagnoses. Moreover, some studies reported improvements in pain intensity for both intervention and control groups, but no statistically significant differences between the groups.37–39 Morone et al. 39 attributed pain intensity reduction to analgesic drugs, which were included in both intervention and control treatments. However, in the present study most participants underwent multiple interventions (e.g. treatment from a physician, medication, physiotherapy) before participating in the BAI-Rehabilitation, which is usually required for health insurance coverage. Accordingly, Kamper et al. 12 suggested that multimodal biopsychosocial rehabilitation necessitates careful consideration due to the high costs associated with such interventions. Interprofessional pain rehabilitation programmes are often the last option after the failure of other interventions. 10 Therefore, the absence of improvement in pain intensity in this study might be due to previous interventions focusing on pain intensity before BAI-Rehabilitation. Additionally, the primary goals of the examined intervention include enhancing pain coping and improving quality of life rather than reducing pain intensity.
A strength of this study is the large sample size. The use of the linear mixed model provided a powerful approach to analysing change over time and dealing with missing data. 33 Another strength is the focus on occupational performance as the main outcome measure, aligning with the goals of interprofessional multimodal rehabilitation, specifically the improvement of activity and participation. 11
Several methodological limitations should be considered. Data were extracted from a registry and were affected by missing data. The study lacked a control group, therefore it is not possible to conclude that changes were exclusively due to the BAI-Rehabilitation. However, it is likely that the programme significantly contributed to the changes, as participants did not receive additional interventions besides the programme, and spontaneous recovery is improbable in chronic pain conditions. 14 We did not adjust for multiple testing across the primary and secondary outcomes, which may have inflated the overall type I error; significant findings – particularly for secondary outcomes – should therefore be interpreted with caution. As multiple measures were analysed, some findings may reflect chance rather than true effects. 31 Self-rated outcome measurements might be subject to bias. 31 Bias is also possible through the influence of interviewers on participants, particularly as interviewers were not blinded to measurement points and were usually in the role of treating the participant during the BAI-Rehabilitation. This could lead to biased results, as the therapist–participant relationship may affect the score rating. 31 Further weaknesses are associated with the COPM as the main outcome measure: scoring problems for the COPM were reported in previous studies, incentivizing researchers to speculate that participants might struggle to distinguish between the scores of performance and satisfaction with performance.7,22 The 10-point Likert scale may be subject to varied interpretations among individuals, limiting objectivity and requiring cautious use in research. 22
Overall, this study confirms the short- and mid-term effectiveness of the BAI-Rehabilitation in improving quality and satisfaction with occupational performance, reducing the burden of suffering, and enhancing health-related quality of life in persons with chronic musculoskeletal pain. However, no effect of the BAI-Rehabilitation on pain intensity was observed. These findings confirm previous research on the BAI-Rehabilitation and emphasize the importance of focusing on occupational performance, burden of suffering, and quality of life in multimodal interprofessional interventions. Further research is needed to verify the long-term effectiveness of the examined intervention and to understand better occupational performance as an intervention outcome. Overall, this study contributes to the evidence supporting the effectiveness of outpatient interprofessional rehabilitation for persons with chronic pain. Further studies should include a control group to strengthen conclusions.
Clinical messages
The interprofessional biopsychosocial intervention empowers persons with chronic pain to enhance their occupational performance and quality of life.
The intervention reduced pain related suffering, without changing pain intensity.
The increase in satisfaction with performance may indicate that coping strategies play a key role in the intervention's success.
Footnotes
Acknowledgements
We would like to thank the interprofessional team of the BAI-Rehabilitation for the programme's implementation and development, and for supporting data collection. We would also like to thank Tom Friedli for assistance with the registry, Lukas Bütikofer for statistical consulting, and Franziska Heigl and Anita Zogg for their support. This research was conducted as the final qualification work in the programme of the European Master of Science in Occupational Therapy.
Ethical considerations
The Ethics Review Board Bern, Switzerland gave ethical approval for the research project of the Clinic of Rheumatology and Immunology (Project-ID: 2018-01583). Data were extracted from the registry anonymously following the guidelines of the registry.
Consent to participate
Participants of the study either agreed to a general informed consent of the University Hospital of Bern, allowing the use of data for research purposes, or to a specific consent for research projects concerning the registry. Verbal information about the study was provided, as well as a written consent form and a written information sheet.
Author contributions
This study was designed by Felicia Bertschi, Brigitte E Gantschnig, and Mette Andresen. The data were analysed by Felicia Bertschi and Brigitte E Gantschnig, and the results were critically examined by all authors. Felicia Bertschi had a primary role in preparing the manuscript, which was edited by Brigitte E Gantschnig and Mette Andresen. All authors have approved the final version of the manuscript and agree to be accountable for all aspects of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Department of Rheumatology and Immunology of the University Hospital (Inselspital) Bern funded data collection for this study. The authors received no other financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data in this study was extracted from the internal chronic pain registry from the Department of Rheumatology and Immunology of the University Hospital (Inselspital) Bern. 40 The dataset analysed during the current study is not publicly available but is available from the corresponding author on reasonable request.