
Abstract
Aim
To establish and clarify the concept of ‘prenatal rehabilitation’ within maternal health management by identifying its defining attributes, antecedents and consequences.
Design
A concept analysis.
Methods
Walker and Avant's concept analysis method was employed to identify the antecedents, attributes and consequences of prenatal rehabilitation.
Data sources
Comprehensive searches were conducted in PubMed, Web of Science, Embase, Medline, CINAHL, CNKI, VIP, WanFang and CBM databases from their inception to November 2024. Dictionary sources, grey literature and manual reference checks were also utilised to capture diverse perspectives related to ‘prenatal rehabilitation’.
Results
A total of 34 studies were included. Five defining attributes of prenatal rehabilitation were identified: (1) dual therapeutic and preventive functions, (2) proactive and dynamic integrated interventions, (3) focus on specific physiological needs during pregnancy, (4) goal-oriented towards functional recovery and birth readiness and (5) foundation and facilitation for postpartum rehabilitation. Antecedents included pregnancy-induced dysfunction and discomfort, individual characteristics and external resources. Consequences were improved maternal outcomes, better neonatal health indicators and decreased utilisation of healthcare resources.
Conclusion
A clarifying definition and conceptual model of prenatal rehabilitation was developed, highlighting its proactive, personalised and multidisciplinary nature in promoting maternal health management. These findings provide a theoretical foundation for clinical practice and future research.
Keywords
Introduction
Pregnancy is a significant transition in a woman's life, often accompanied by physiological and psychological changes that may affect maternal physical function, quality of life and birth outcomes. Prenatal rehabilitation is increasingly recognised as a proactive health strategy to address these challenges by alleviating discomfort, improving functional capacity and enhancing birth preparedness.1–3
The term prenatal rehabilitation is increasingly used in maternal health literature. Numerous studies related to prenatal rehabilitation have primarily focused on targeted interventions for isolated symptoms or single complications during pregnancy, such as stress urinary incontinence, gestational diabetes and hypertension.4–6 Some scholars have proposed broader perspectives, suggesting that prenatal rehabilitation should be understood as a multidisciplinary and comprehensive intervention strategy that enhances physical adaptability, and reduces pregnancy-related complications through systematic training across physiological, psychological and behavioural dimensions.7–9 Despite these developments, a unified and comprehensive definition of prenatal rehabilitation remains absent.
Notably, prenatal rehabilitation shares conceptual similarities with prehabilitation, a strategy focused on the overall health of the person, emphasising the construction of personalised, multi-modal prehabilitation programmes with multidisciplinary collaboration, and reflect the field of rehabilitation medicine has gradually shifted from ‘post-injury treatment’ to ‘preventive intervention’. 10 Pregnancy, similar to surgery, can present considerable physical and emotional challenges, requiring careful management and rehabilitation. While prehabilitation is yet to be fully defined and operationalised in clinical guidelines, a clearly defined conceptual framework is lacking for prenatal rehabilitation.
To date, no formal conceptual analysis of prenatal rehabilitation has been conducted. This absence limits theoretical clarity, complicates clinical translation and weakens the coherence of research in the field. This study addresses this gap by systematically analysing the concept using Walker and Avant's method,11,12 identifying its defining attributes, antecedents and consequences. It is expected that the findings will contribute to the theoretical development of prenatal rehabilitation, provide a conceptual foundation for subsequent empirical studies and offer guidance for evidence-based nursing practice and interdisciplinary intervention design in the field of maternal care.
Methods
Concept analysis method
This study adopted Walker and Avant's concept analysis method to identify the defining attributes, antecedents and consequences of prenatal rehabilitation.13–15 The method includes eight steps: selecting a concept, clarifying the purpose of analysis, exploring all potential usages of the concept, identifying defining attributes, constructing model cases, identifying additional case types, analysing antecedents and consequences, and defining empirical referents.11,12
Data sources
To gain a comprehensive understanding and definition of ‘prenatal rehabilitation’, this study conducted a wide-ranging literature search of dictionaries, academic databases and grey literature. First, dictionary searches were performed in the Oxford Advanced Learner's English-Chinese Dictionary, the Collins Advanced English-Chinese Dictionary, the Merriam-Webster Dictionary, the Miller-Keane Encyclopedia and Dictionary of Medicine, Nursing, and Allied Health. These sources provided baseline definitions and related meanings of the term ‘prenatal rehabilitation’.
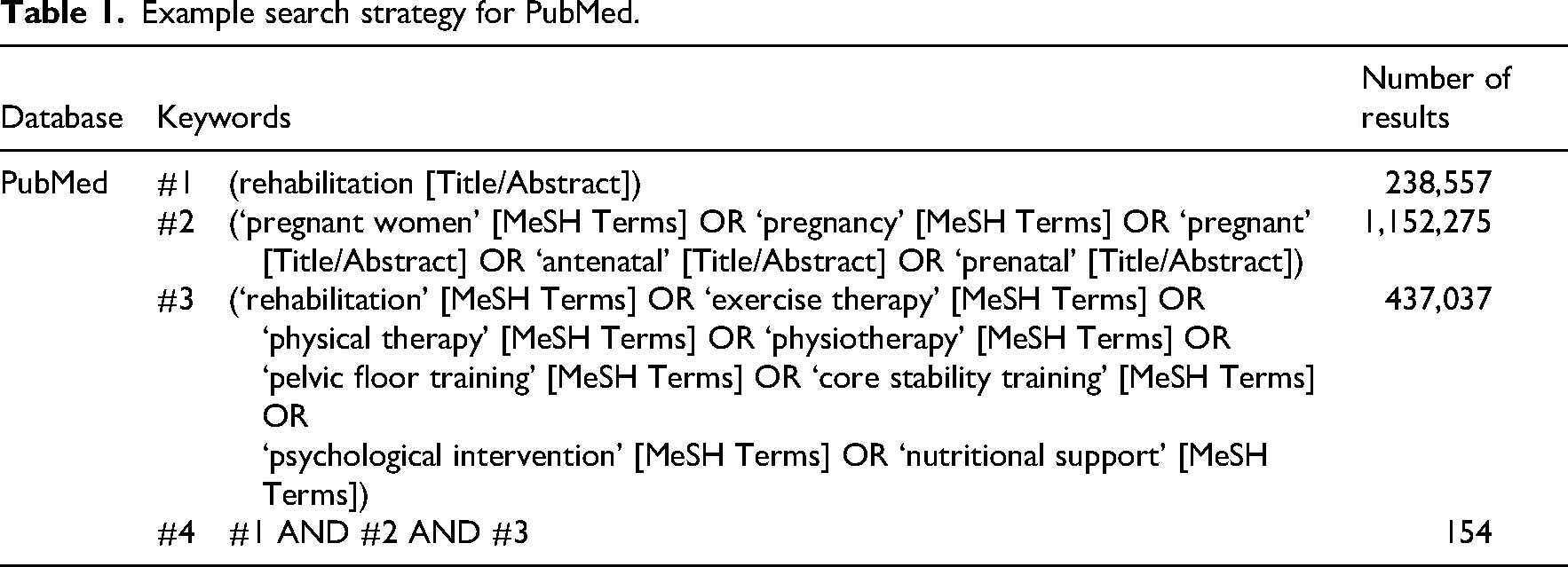
Next, academic database searches were carried out in PubMed, Web of Science, Embase, Medline, CINAHL, CNKI, VIP database, WanFang database and CBM. The search terms were (‘pregnant women’ OR ‘antenatal’ OR ‘prenatal’) AND (‘rehabilitation’ OR ‘exercise therapy’ OR ‘physical therapy’ OR ‘physiotherapy’ OR ‘pelvic floor training’ OR ‘core stability training’ OR ‘psychological intervention’ OR ‘nutritional support’). Literature searches were conducted using a combination of MeSH terms and free words. The search timeframe covered all available records from database inception to November 2024. Reference lists of relevant articles were also reviewed to ensure a broad and in-depth capture of the literature. The detailed search strategy for PubMed is presented in Table 1.
Example search strategy for PubMed.
Additionally, grey literature was explored across multiple key resources, 16 including the British Electronic Theses Online Service, Google Scholar, ProQuest Dissertations & Theses and Open Grey, to retrieve non-commercially published academic and professional documents. This step helped supplement knowledge of and insights into the concept of prenatal rehabilitation, thereby ensuring diversity and completeness in the information sources.
Selection criteria
Documents were included if they discussed any aspect of prenatal rehabilitation, such as definitions, attributes, antecedents, consequences, measurement tools, or example cases. Only Chinese- and English-language documents with accessible full texts were included. Acceptable types were journal articles, books, theses, qualitative or quantitative studies, reviews and grey literature. Editorials, letters and non-peer-reviewed sources were excluded. As the aim of this analysis was conceptual rather than evaluative, no formal quality assessment tools were used; however, each article's relevance to the theme was carefully examined.
Data collection and analysis
Two researchers independently screened all titles and abstracts. Full texts were reviewed when both agreed on eligibility. Zotero (version 7.0) was used to manage records. The selection process is outlined in the PRISMA diagram 17 (Figure 1). Of 1105 initial records, 104 remained after screening titles and abstracts and 34 (10 Chinese, 24 English) were included in the final analysis following full-text review.
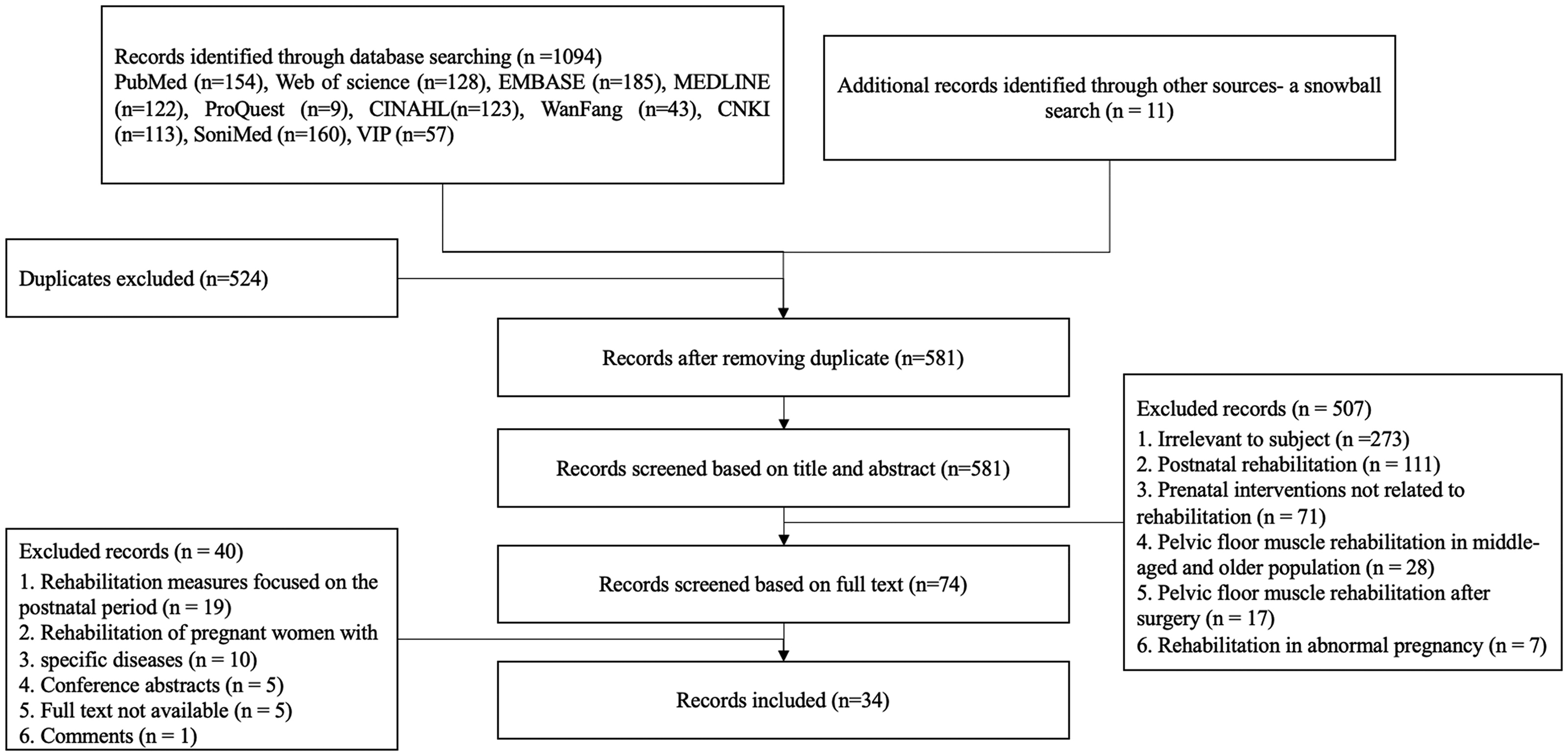
PRISMA flow diagram.
Results
A total of 34 studies focusing on the concept of ‘prenatal rehabilitation’ were included, with participants identified as pregnant or postpartum women. These studies were published between 2002 and 2024 and originated from China (n = 11), the United States (n = 6), Romania (n = 2), Turkey (n = 2), Brazil (n = 2), Pakistan (n = 1), India (n = 2), the Netherlands (n = 1), Japan (n = 1), Canada (n = 1), Lithuania (n = 1), Indonesia (n = 1), France (n = 1), Bangladesh (n = 1) and Hungary (n = 1). The study designs were diverse, consisting of randomised controlled trials (n = 10), review articles (n = 7), cohort studies (n = 6), cross-sectional studies (n = 4), case studies (n = 2), qualitative studies (n = 2), quasi-experimental studies (n = 1), expert consensus (n = 1) and opinion-based studies (n = 1) (see Supplemental Table). A conceptual model of prenatal rehabilitation, including its defining attributes, antecedents, consequences and their theoretical relationships, is presented in Figure 2.
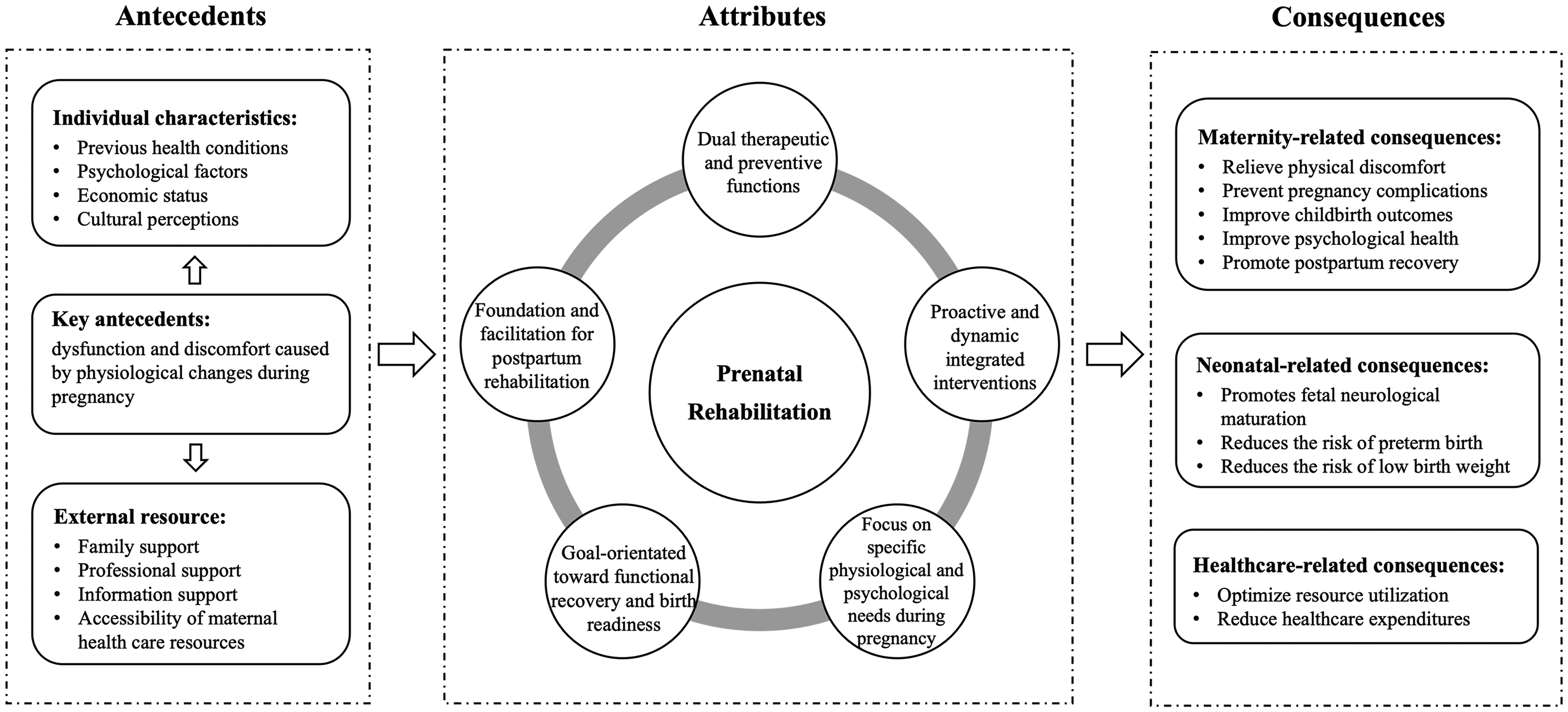
Proposed conceptual model of the prenatal rehabilitation.
Uses of the concept
Uses of the concept in dictionaries
Currently, no mainstream dictionary provides an explicit definition of ‘prenatal rehabilitation’. Accordingly, this study separately searched the terms ‘prenatal’ and ‘rehabilitation’ to deepen the overall understanding of prenatal rehabilitation.
Multiple dictionaries offer similar definitions of ‘prenatal’, referring to events that occur before a baby is born or relating to healthcare during pregnancy. The Oxford Advanced Learner's English-Chinese Dictionary 10th edition defines it as ‘relating to the medical care given to pregnant women’, whereas the Collins Advanced Dictionary states it is ‘used to describe things relating to the medical care of women during pregnancy’. The Merriam-Webster Dictionary describes it as ‘occurring, existing, performed, or used before birth’.
The definition of ‘rehabilitation’ is extensively elaborated in various authoritative sources. The Merriam-Webster Dictionary defines rehabilitation as ‘the action, process, or result of rehabilitating or of being rehabilitated’ The National Library of Medicine describes rehabilitation as ‘restoration of human functions to the maximum degree possible in a person or persons suffering from disease or injury’ Additionally, the Miller-Keane Encyclopedia and Dictionary of Medicine, Nursing and Allied Health define it as ‘a treatment or treatments designed to facilitate the process of recovery from injury, illness, or disease to as normal a condition as possible’. This definition further clarifies that rehabilitation aims to help patients achieve optimal physical and psychological adaptation and regain independence. It also includes vocational training, psychological adjustment and guidance to enable learning and relearning skills essential for daily living.
In addition to these dictionary and clinical definitions, many publications have discussed the meaning of rehabilitation. A terminological analysis comparing definitions used by consumers, major stakeholders and researchers showed considerable variation in the words and concepts used and proposed a synthesis of key elements of rehabilitation. 43 An editorial has also argued for an internationally shared rehabilitation definition for clinical research purposes and described the rationale for the global initiative led by Cochrane Rehabilitation. 44 These works indicate that rehabilitation is a complex concept with multiple definitions across settings. Acknowledging this, the present analysis does not aim to redefine rehabilitation in general, but focuses on clarifying how ‘prenatal rehabilitation’ should be understood within this broader field.
Uses of the concept in literature
There was no uniform definition of ‘prenatal rehabilitation’ in the current literature, and there was some variation in its field of application. It is worth noting that ‘prenatal’ was expressed in different ways in related studies, including ‘prenatal’, ‘pregnancy’, ‘antenatal’, etc. In this study, all of them were regarded as applications of the term ‘prenatal rehabilitation’ in the literature.
In 2011, Beyaz et al. 18 proposed the concept of pregnancy rehabilitation, focusing on the role of exercise rehabilitation in improving musculoskeletal function during pregnancy, suggesting that stretching, core stabilisation, respiratory conditioning and relaxation training could be used to reduce pain and discomfort during pregnancy. Subsequently, researchers have continued to expand the connotation of prenatal rehabilitation, applying it to a variety of areas such as pelvic floor rehabilitation, nutritional management, oral health management and psychological intervention.
Acharya et al. 3 showed that pelvic floor muscle rehabilitation during pregnancy was effective in strengthening the pelvic floor muscles and reducing the risk of postpartum urinary incontinence and pelvic organ prolapse, and Yıldırım et al. 1 and Perjés 34 investigated the effects of Pilates and dance rehabilitation on the alleviation of low-back pain during pregnancy and the promotion of foetal neurodevelopment, respectively. Choedon et al. 20 found that personalised dietary interventions and nutritional education could improve maternal nutritional status and addressing risk factors for pregnancy complications. Calin et al. 45 and Yang et al. 29 proposed the concept of ‘prenatal oral rehabilitation’, which emphasises the promotion of the overall health of mothers and infants through oral care, gingival health management and caries prevention.
Most of the above studies focused on a single dimension or specific symptoms. As research deepened, multidisciplinary integration was becoming an important development in prenatal rehabilitation. Selman et al. 9 stated that prenatal rehabilitation can integrate multiple interventions, such as exercise rehabilitation, pelvic floor rehabilitation and core stabilisation training in the management of maternal health. Ferreira et al. 8 further emphasised that the integration of multidisciplinary rehabilitation approaches such as physiotherapy, acupuncture, yoga, resistance training and orthopaedic manipulation may be effective in the management of chronic pain during pregnancy. The integration of multidisciplinary rehabilitation approaches is effective in managing chronic pain during pregnancy. Sun et al. 41 also pointed out in their expert consensus that prenatal rehabilitation should not only include a single type of training but should also cover weight management, pelvic floor rehabilitation, mental health support, whole-body muscle training and respiratory training, thus providing a systematic rehabilitation programme for pregnant women.
Defining attributes
To derive the defining attributes, all included studies were read repeatedly and key statements describing the purposes, components and processes of prenatal rehabilitation were extracted. Similar expressions were grouped into preliminary categories, which were then compared and refined through discussion among the researchers. This iterative process led to the identification of five core attributes of the concept.
Dual therapeutic and preventive functions
Prenatal rehabilitation serves both therapeutic and preventive roles. Therapeutically, prenatal rehabilitation may help alleviate common pregnancy-related discomforts such as musculoskeletal pain, urinary incontinence and pelvic floor dysfunction. Some studies suggest that these interventions may be associated with lower risks of gestational diabetes mellitus, gestational hypertension and pelvic floor injuries. 3 Antenatal and postnatal pelvic floor muscle training ‘may reduce the risk of developing urinary incontinence in late pregnancy and postpartum’, 3 and a structured pregnancy rehabilitation programme was reported to be ‘effective for preventing low back pain and excessive weight gain during pregnancy’. 18 Furthermore, strategies including oral rehabilitation and nutritional management have been reported to be associated with fewer pregnancy complications and maternal–infant health risks, potentially contributing to better overall health during pregnancy.20,27,45
Proactive and dynamic integrated interventions
Prenatal rehabilitation is a health management process with dynamic adaptability that needs to be optimised according to the different stages of pregnancy and individual needs. Early pregnancy focuses on adaptation to initial physiological changes and discomfort relief, while mid- and late pregnancy emphasises core stability, muscular endurance and preparation for labour. 9 In the literature, prenatal rehabilitation is described as promoting proactive health management, with programmes that encourage pregnant women to engage in personalised exercise, psychological adjustment and health monitoring. 26 Multidisciplinary teamwork (including rehabilitation therapists, obstetricians and gynaecologists, counsellors and dietitians) is reported to support the development of scientific and individualised interventions. 39 A recent clinical commentary proposed ‘a timeline and suggested progression for exercise participation’ from pregnancy through the postpartum period, highlighting the need for proactive, stage-specific and adjustable rehabilitation plans. 9
Focus on specific physiological and psychological needs during pregnancy
In existing studies, prenatal rehabilitation is described as taking into account the physiological and psychological changes during pregnancy in order to support the safety and appropriateness of interventions. As noted in a clinical study, ‘virtually all women experience some degree of musculoskeletal discomfort during pregnancy’, 18 highlighting the need to tailor rehabilitation to these physiological changes. As hormonal changes during pregnancy may affect pelvic stability, rehabilitation should be combined with core strengthening and postural adjustment to reduce the risk of musculoskeletal problems such as pubic symphysis separation. 23 Some authors note that altered haemodynamics in late pregnancy may increase the risk of venous thrombosis and describe rehabilitation programmes that include strengthened circulatory management to optimise circulatory intervention strategies. 40 In addition, many authors recommend that prenatal exercise programmes avoid high-impact and high-intensity training in order to protect foetal safety. Moreover, the literature highlights the psychological challenges during pregnancy, such as anxiety, mood fluctuations and fear of childbirth, and describes the use of interventions such as cognitive behavioural therapy and mindfulness techniques to support emotional well-being and improve adherence to rehabilitation programmes. 42
Goal-oriented towards functional recovery and birth readiness
The core goal of prenatal rehabilitation is to promote physical functional recovery of the pregnant woman and prepare her adequately for childbirth. Training of core and pelvic floor muscles could reduce the risk of perineal injuries and enhance maternal control of contractions, and improve childbirth efficiency. 36 Systematic rehabilitation also improves muscular endurance and coordination, reduces caesarean section rates and relieves fatigue during labour. 3 A graded pre- and postnatal physical therapy protocol ‘improved symptoms of incontinence, prolapse and pain in the athlete mother’, 5 underscoring the goal of restoring and maintaining functional capacity. Rehabilitation interventions may improve the physiological adaptability of pregnant women before childbirth, thus increasing the success rate of spontaneous delivery and reducing complications during labour.
Foundation and facilitation for postpartum rehabilitation
Pelvic floor muscle training and core stability training during pregnancy have been reported to be associated with lower rates of postpartum urinary incontinence, pelvic organ prolapse and rectus abdominis muscle separation in some studies.9,30,38 A recent review on pelvic-floor dysfunction prevention reported a ‘positive effect of pelvic-floor muscle training in prepartum and postpartum periods’ on pelvic-floor dysfunction, particularly urinary incontinence. 40 In addition, measures such as psychological support and weight management may help to reduce the risk of postpartum depression and anxiety and enhance maternal capacity to cope with newborn care. 41 Taken together, these findings suggest that prenatal rehabilitation may provide an important foundation for postnatal recovery and long-term health management.
Model case
According to Walker and Avant, 11 a model case can be derived from real life, literature, or constructed by the researcher based on a practical situation. The model case for this study was constructed based on clinical experience as follows:
Mary, a 28-year-old woman who was 26 weeks pregnant, visited an integrated healthcare center due to sacrococcygeal pain and nocturnal leg cramps. After her assessment, she was recommended to join a multidisciplinary and integrated prenatal rehabilitation programme designed to alleviate discomfort, optimise fitness, manage weight gain and prepare for labour and postnatal recovery.
The physiotherapist advised Mary to perform Kegel exercises, core training, brisk walking and stretching exercises. These activities aimed to relieve pain, improve pelvic floor muscle function and enhance postural stability. Concurrently, the dietitian developed a nutrition plan enriched with calcium, magnesium and potassium to support muscle health, regulate weight and prevent gestational diabetes. In addition, a psychological counsellor introduced cognitive behavioural therapy and positive thinking exercises to help Mary manage her anxiety. She was also trained in breathing techniques for labour. At her 36-week follow-up, Mary reported significant pain relief, improved sleep quality, healthy weight gain and increased confidence regarding childbirth.
Additional cases, including related, borderline and contrary examples, are provided in Supplemental Appendix I for further clarification of the concept's defining attributes.
Antecedents
Key preconditions: Dysfunction and discomfort caused by physiological changes during pregnancy
The key preconditions for prenatal rehabilitation are dysfunction and discomfort caused by physiological changes during pregnancy. As the foetus grows, increasing pressure on the pelvic floor muscles leads to their gradual relaxation, potentially resulting in urinary incontinence and pelvic organ prolapse, which impair daily functioning and quality of life. Hormonal fluctuations during pregnancy further exacerbate pelvic floor weakening, increasing the likelihood of urinary incontinence after childbirth.24,30 In addition, elevated levels of relaxin and other hormones contribute to ligament laxity and decreased pelvic stability, which may cause pubic symphysis separation and pelvic girdle pain – factors that limit mobility and may result in chronic postpartum pain.1,22
As pregnancy progresses, the forward shift in the centre of gravity and intensified lumbar lordosis cause compensatory overuse of the lower back muscles, often leading to persistent low back pain. Such discomfort not only affects mobility but may also continue into the postpartum period, undermining maternal quality of life. 21 Additionally, hormonal changes may disrupt oral micro-ecology, increasing the risk of gingivitis and dental caries, thereby posing further challenges to maternal health during pregnancy.28,29
Individual characteristics
Previous health conditions: Women with health problems such as chronic low back pain, pelvic floor dysfunction, pelvic structural abnormalities, or obesity before pregnancy are more likely to experience dysfunction during pregnancy and may affect the implementation and effectiveness of prenatal rehabilitation.21,22,33
Psychological factors: emotional factors such as anxiety, depression and fear of childbirth may reduce pregnant women's compliance with rehabilitation training. It was found that pregnant women with higher levels of anxiety were more likely to avoid exercise rehabilitation.24,34
Economic status: Economic pressure may make some pregnant women more inclined to reduce non-essential medical interventions, such as prenatal rehabilitation training. Studies have shown that pregnant women with better economic status are more likely to accept personalised rehabilitation programmes and show higher adherence, whereas pregnant women with financial difficulties may miss out on rehabilitation opportunities due to insufficient medical resources.25,33
Cultural perceptions: Misconceptions about exercise during pregnancy in traditional attitudes may affect the rehabilitation participation of pregnant women. In some regions, pregnant women may have limited awareness of the benefits and safety of antenatal rehabilitation exercise, and this view may reduce their willingness to participate in rehabilitation training. 24
External resources
Family support: the attitudes of family members have a direct impact on the willingness of pregnant women to participate in rehabilitation training. Studies have shown that the positive attitudes of spouses, parents and other family members help to increase the execution rate of rehabilitation and promote the psychological health of pregnant women.24,25
Professional support: professional guidance from physiotherapists, obstetricians and rehabilitation therapists is decisive for the effectiveness of rehabilitation training. It was found that pregnant women who received professional rehabilitation guidance achieved better results in pelvic floor function recovery and pain relief. 30
Information support: existing studies describe health education about rehabilitation as an important way to enhance pregnant women's knowledge and compliance with rehabilitation. Information dissemination methods such as medical staff counselling, health lectures and online rehabilitation courses are commonly reported approaches. Some studies suggest that these measures are associated with higher acceptance of rehabilitation training among pregnant women. 25
Accessibility of maternal healthcare resources: Uneven distribution of medical resources, especially in rural areas, may make it difficult for pregnant women to access professional rehabilitation services. Measures such as improving the accessibility of maternal healthcare resources, setting up rehabilitation clinics in medical institutions and promoting distance rehabilitation courses have been proposed as potential ways to address this problem. 7
Consequences
The outcomes of prenatal rehabilitation can be categorised according to their impact on the pregnant woman, the newborn and the healthcare system:
Maternity-related consequences
Prenatal rehabilitation may help relieve low back pain, pubic symphysis separation and pelvic floor dysfunction during pregnancy, and improve the motor ability and quality of life of pregnant women. Rehabilitation interventions targeting the pelvic floor have been reported to strengthen pelvic floor muscles and are associated with lower rates of urinary incontinence and pelvic organ prolapse in some studies.9,39 In addition, some exercise-based rehabilitation programmes have been reported to be associated with shorter labour duration, higher rates of spontaneous delivery and lower caesarean section rates, as well as improvements in psychological health, including reduced anxiety and depressive symptoms, in certain study populations. 31
Neonatal-related consequences
Prenatal rehabilitation may also be linked to favourable neonatal outcomes. Moderate maternal exercise during pregnancy has been reported to be associated with indicators of foetal neurological maturation, such as increased foetal heart rate variability (FHRV), and with a lower risk of intrauterine growth restriction in some studies. Some studies have suggested that pregnant women who participate in prenatal rehabilitation programmes have higher neonatal Apgar scores and a lower risk of preterm birth and low birth weight in their infants.4,34,42
Healthcare-related consequences
Some studies suggest that wider implementation of prenatal rehabilitation may be associated with reduced use of healthcare resources, lower healthcare expenditures and lower rates of postpartum complications and hospitalisation. 25
Empirical referent
In the final stage of the analysis, we identified empirical references for the concept. They are important in practice because they provide healthcare professionals with clear and observable phenomena that enable the identification of the existence of the concept in a given patient.
Currently, the majority of prenatal rehabilitation measurement tools focus primarily on the assessment of rehabilitation outcomes, with relatively little attention paid to the process and quality of rehabilitation implementation. These tools are commonly used to assess improvements in physical functioning, enhanced mental health status and pain reduction in postpartum women. In the field of pelvic floor muscle rehabilitation, commonly used measurement tools include the Modified Oxford Grading System (MOGS), the Pelvic Organ Prolapse Quantification (POP-Q), the Urinary Distress Inventory (UDI-6) and the International Continence Questionnaire-Short Form (ICIQ-SF), which are tools primarily used to assess the effects of rehabilitation on pelvic floor muscle strength, organ prolapse and urinary incontinence improvement.30,32,37,38 In terms of pain management and postural control, commonly used measurement tools include the Québec Back Pain Disability Scale (QBPDS), Roland-Morris Disability Questionnaire (RMDQ), Visual Analogue Score (VAS), McGill Pain Questionnaire and gait analysis and the Force Platform Test, which are tools that can assess low back pain severity, postural control and functional limitations.1,18,22,35
Additionally, tools such as the Anxiety and Depression Inventory and the Maternal Mental Health Inventory are employed to assess improvements in emotional wellbeing, particularly symptoms of anxiety and depression among pregnant women.34,42 Specialised measurement tools have also been developed for specific contexts – for example, the FHRV metric to assess foetal neurodevelopment, and oral health instruments such as the Plaque Index (PI) to evaluate the effectiveness of prenatal oral rehabilitation.27,29,45 However, the common feature of these tools is that they are more focused on the assessment of the effectiveness of rehabilitation rather than reflect the process and qualitative aspects of the rehabilitation intervention.
Notably, a questionnaire instrument for assessing the level of knowledge, attitudes and practices (KAP) of pregnant women in the field of prenatal rehabilitation was constructed in a study by Mahmood et al. 19 The questionnaire covered pregnant women's knowledge of rehabilitation services, attitudes towards prenatal rehabilitation interventions, and behaviours of actual participation in rehabilitation activities. The questionnaire was scientifically pre-tested and administered under the supervision of medical professionals and obstetricians. Although the KAP questionnaire provides valuable information in identifying the implementation of and adherence to rehabilitation behaviours, it still fails to directly measure the quality and strategies of the rehabilitation implementation process.
Future research should focus on developing a system of tools that can comprehensively assess the prenatal rehabilitation, covering multiple dimensions such as the quality of the rehabilitation, implementation process and adherence.
Discussion
Based on Walker and Avant's conceptual analysis, this study systematically analysed the core definitions, attributes, antecedents and consequences of ‘prenatal rehabilitation’. The results of this study indicate that prenatal rehabilitation contains five key attributes: dual therapeutic and preventive functions; proactive and dynamic integrated interventions; focus on the specific physiological needs during pregnancy; goal-oriented towards functional recovery and birth readiness; and foundation and facilitation for postpartum rehabilitation. Meanwhile, this study summarises the multifaceted antecedent of prenatal rehabilitation and explores its positive impact related to maternal and child health and healthcare, providing an important theoretical foundation for future theoretical modelling, clinical pathway optimisation and the development of assessment tools.
This study further proposes an operational definition of ‘prenatal rehabilitation’: prenatal rehabilitation refers to a systematic and proactive health management process conducted during pregnancy grounded in multidisciplinary interventions. The aim is to enhance maternal functional reserves, alleviate pregnancy-related discomforts and prevent complications, thereby laying a foundation for safe delivery and postpartum recovery. This process emphasises early intervention and dynamic adjustment, and it formulates scientifically sound and safe rehabilitation strategies tailored to the physiological and psychological needs unique to pregnancy. By integrating the prevailing understandings found in the literature, this definition provides a theoretical foundation and direction for future research in the field. This operational definition is proposed in line with recent work that compares and clarifies rehabilitation definitions for research purposes,43,44 and is intended to describe how rehabilitation is applied during pregnancy rather than to replace generic definitions used in other contexts.
Notably, the theoretical framework of prenatal rehabilitation aligns closely with the concept of ‘prehabilitation’. As a forward-looking management model embedded in the Enhanced Recovery After Surgery framework, prehabilitation underscores the importance of enhancing an individual's functional reserves through multidimensional interventions – including exercise, nutritional support and psychological counselling – prior to major treatments such as surgery or chemotherapy.10,46 Although pregnancy and childbirth are physiological processes, the dual physical and psychological challenges they present qualify them as a special form of physiological stress. This is especially relevant for women of advanced maternal age, those with underlying conditions, or those at high obstetric risk, who often face pre-delivery functional vulnerabilities similar to those observed in preoperative patients. From this perspective, positioning pregnancy as a critical ‘rehabilitation time point’ and viewing prenatal rehabilitation as an extension of prehabilitation in the context of pregnancy not only highlights its conceptual distinction from conventional obstetric care, but also deepens its theoretical relevance within the framework of contemporary rehabilitation medicine.
The study results also reveal that prenatal rehabilitation is evolving beyond symptom-specific or complication-oriented interventions. It is increasingly being implemented as a structured, multimodal approach, encompassing pelvic floor training, core stability, psychological support, nutritional management and oral health. Such a multifaceted structure suggests that integrated interdisciplinary service models may be more appropriate than isolated interventions in clinical practice.47,48 In future practice, the clarified concept of prenatal rehabilitation may help healthcare providers to consider earlier initiation of rehabilitation, including assessments and personalised interventions from early pregnancy. Multidisciplinary teams – including obstetricians, rehabilitation therapists, psychological counsellors and dietitians – may also facilitate the delivery of more continuous and coordinated rehabilitation services for pregnant women.
Moreover, the study underscores the importance of promoting continuity between prenatal and postpartum rehabilitation. The findings of this study indicate that prenatal interventions may be viewed as a foundational phase of the postpartum recovery trajectory. At the policy level, these results may inform discussions on the institutionalisation and formalisation of prenatal rehabilitation pathways, for example by incorporating relevant elements into routine obstetric service guidelines, clinical pathways and supportive mechanisms such as insurance reimbursement and public health education. 49 Additionally, strengthening professional workforce development and specialised education for obstetric care professionals may represent important steps towards advancing clinical practice in this area.
Several limitations of this study should be acknowledged. First, it only included literature published in Chinese and English, which may have excluded relevant insights from studies published in other languages or cultural contexts. Second, the study focused on concept analysis rather than on in-depth evaluation of specific intervention modalities. Future research could explore the effects of various prenatal rehabilitation models, examine their cultural adaptability and conduct empirical investigations to strengthen evidence-based implementation and interdisciplinary integration.
In conclusion, this study systematically reviewed the definition, attributes, antecedents and consequences of prenatal rehabilitation and developed a conceptual model that clarifies its internal structure and pathways of influence. The proposed model not only helps to unify academic understanding of the concept but also provides a theoretical basis for the development of clinical interventions and integrated service frameworks. In contrast to traditional problem-oriented maternity care, the proposed model reconceptualises prenatal rehabilitation as a proactive and forward-looking health management strategy. The model highlights the potential value of early and targeted multidisciplinary interventions and may support a shift from passive support to more active health promotion. The findings also point to the potential importance of stronger interdisciplinary collaboration and greater continuity in rehabilitation services. Future research should validate this model in diverse populations and cultural contexts, and develop tools to assess the quality and implementation process of prenatal rehabilitation interventions, thus advancing the field from theoretical construction to clinical translation and systems integration.
Clinical messages
This concept analysis clarifies the previously inconsistent use of ‘prenatal rehabilitation’ in maternal health research.
Prenatal rehabilitation combines therapeutic and preventive interventions to support maternal function and preparation for childbirth.
It is characterised by multimodal, multidisciplinary care addressing physical, psychological and behavioural needs across pregnancy.
Supplemental Material
sj-docx-1-cre-10.1177_02692155251415249 - Supplemental material for Prenatal rehabilitation: A concept analysis
Supplemental material, sj-docx-1-cre-10.1177_02692155251415249 for Prenatal rehabilitation: A concept analysis by Yuan Mengmei, Zhang Ke and Zeng Tieying in Clinical Rehabilitation
Supplemental Material
sj-docx-2-cre-10.1177_02692155251415249 - Supplemental material for Prenatal rehabilitation: A concept analysis
Supplemental material, sj-docx-2-cre-10.1177_02692155251415249 for Prenatal rehabilitation: A concept analysis by Yuan Mengmei, Zhang Ke and Zeng Tieying in Clinical Rehabilitation
Footnotes
Acknowledgements
The authors acknowledge the Department of Obstetrics and Gynecology, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology for their help with recruitment.
Author contributions
Yuan Mengmei: visualisation, data curation, formal analysis, writing – original draft preparation, funding acquisition; Zhang Ke: data curation, formal analysis, writing – review & editing; Zeng Tieying: supervision, writing – review & editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the National Natural Science Foundation of China (No. 72304105) and Tongji Hospital Affiliated to Tongji Medical College of Huazhong University of Science and Technology (No. 2025C05). The funding bodies were not involved in the design of the study, data collection, analyses and interpretation of data or in writing of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.