
Abstract
Objective
To explore and describe the components and underpinning theories of nurse-initiated transitional (hospital-to-home) care and to evaluate the effects of interventions on activities of daily living (ADLs), quality of life (QoL), depression, anxiety, self-efficacy, stroke-related knowledge, patient satisfaction and healthcare service utilisation in older stroke survivors and self-efficacy, caregiver burden, QoL and satisfaction with care in caregivers.
Data sources
MEDLINE, CINAHL, Cochrane Library, Health and Medical Collection, Nursing and Allied Health, Web of Science, Health Source: Nursing/Academic Edition and Scopus databases were searched in February 2024 and updated in March 2026.
Review methods
Randomised controlled trials (RCTs) and cluster-RCTs were included. Risk of bias was assessed using the Cochrane Risk of Bias tool, and evidence quality was rated with GRADE. Meta-analysis was undertaken using random-effects models.
Results
Seventeen trials were included. Transitional care interventions were guided by various theoretical frameworks and had multiple components. Interventions improved ADLs at 1 month (standardised mean difference (SMD) 0.54; 95% CI 0.12–0.97, four studies) and 3 months (SMD 0.43; 95% CI 0.12–0.74, seven studies), increased patient satisfaction and reduced hospital readmissions up to 3 months. Interventions may improve the Mental Component Score at 1 month, Role Limitations due to Physical Problems and General Health of QoL at 6 months. The certainty of evidence was low to very low.
Conclusion
Nurse-initiated transitional care can improve ADLs and QoL, while reducing hospital readmissions among older stroke survivors during the hospital-to-home transition. Multicomponent interventions combining home visits and follow-up phone calls may enhance improvements in ADLs. High-quality studies are needed to clarify long-term effects.
PROSPERO ID
CRD42024517619.
Introduction
Stroke is the second leading cause of death, and the third most common cause of disability-adjusted life-years lost among noncommunicable diseases worldwide.1,2 Over 93 million people are currently living with stroke. 2 The global increase in the population aged 60 years and older 3 is expected to result in a growing number of older stroke survivors, thereby placing a greater burden on health care systems worldwide, particularly in low- and middle-income countries.1,2
Older stroke survivors require support from family caregivers to assist with daily activities, functional rehabilitation, medication management, complication prevention, and facilitating social interaction.4–6 Among stroke survivors, older adults face a heightened risk of worsened physical function,7,8 emotional distress, 5 adverse events, complications,9,10 and hospital readmissions after discharge from the hospital to home.10–12 In addition, caregivers also face emotional distress, such as anxiety, fear, and being overwhelmed by the increased responsibility of caring for older stroke survivors at home.5,13,14 These issues have become more pronounced due to shortened hospital stays, rushed discharges, limited involvement in discharge planning, and a lack of post-discharge care support.5,13,14
Transitional care is defined as ‘a set of actions designed to ensure the coordination and continuity of healthcare as patients transfer between different locations or different levels of care within the same location’. 15 (p.556) Transitional care interventions have been widely recognised as essential aspect of care during the transition from hospital to home following stroke, as the interventions have positive effects on activities of daily living,16–19 quality of life16,17 and depression.16,17 Global stroke guidelines recommend that stroke survivors and their families or carers be actively involved in planning their transfer of care before hospital discharge, receive early supported discharge services and be referred to community stroke rehabilitation when needed, delivered through interprofessional care and collaboration across the healthcare system.20–22
Fragmented post-discharge services and a lack of continuing care support after discharge lead to stroke survivors and their caregivers facing challenges such as feeling abandoned in adjusting to their new roles and life journeys. 13 The literature highlights that effective transitional care programs are interventions designed to bridge the care gap between hospital and home transitions, initiated during the hospital stay and continuing into the post-discharge period. 23 Whilst there have been multiple systematic reviews considering transitional care and stroke survivors,16–19 there are none which explicitly consider transitional care initiated during pre- and continuing post-discharge in older stroke survivors, nor the specific role of nurses as the primary providers or coordinators of transitional care interventions. Previous reviews have focused on multidisciplinary rehabilitation professionals17–19; however, nurses are widely recognised as having a key role in transitional care for stroke survivors and their family caregivers as they move from hospital to home, particularly in preparing for and supporting self-management, rehabilitation and recovery.24–28
This review aims to explore and describe the components and underpinning theories of existing nurse-initiated transitional care interventions and to evaluate the effectiveness of the interventions on activities of daily living, quality of life, depression, anxiety, self-efficacy, stroke-related knowledge, satisfaction with care and the utilisation of health care services as older stroke survivors’ outcomes and caregivers’ self-efficacy, burden, quality of life and satisfaction with care.
Methods
The protocol of this review was registered in the International Prospective Register of Systematic Review (PROSPERO) (CRD42024517619), and minor amendments to the protocol can be found in Supplemental Table 1. This systematic review and meta-analysis was reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement guidelines. 29
The search was conducted in February 2024 and last updated in March 2026 in the following databases: MEDLINE, CINAHL, Cochrane Central Register of Controlled Trials, ProQuest Health and Medical Collection, ProQuest Nursing and Allied Health, Web of Science, Health Source: Nursing/Academic Edition and Scopus. Keyword and subject heading (where relevant) were undertaken for the following three terms: stroke, transitional care and nurse, including considering additional keywords, abbreviations and MeSH terms. A Boolean search was conducted by combining keywords, as shown in Supplemental Table 2 (e.g. stroke* OR “acute stroke*” OR “cerebrovascular accident*” OR “cerebrovascular stroke*” OR “cerebral stroke*” OR “stroke survivor*” OR CVA OR “cerebral infarction”) AND (“transition* care*” OR “transition* home” OR “transition* of care” OR “care* transition” OR “transition*” OR “hospital to home*” OR “discharge plan*” OR “patient discharge*” OR “hospital discharge*” OR discharge* OR “coach* program*” OR “health coach*” OR “caregiver-oriented” OR “holistic care”) AND (nurse* OR nursing OR “nurse-led” OR multidisciplinary OR integrated OR “nurse-coordinated” OR interprofessional*). References of included studies, grey literature and Google Scholar were manually screened for additional studies, and corresponding authors were contacted if additional clarification was required. Studies published in English from 2009 onward were included, as they represent the current body of evidence on transitional care.
The PICOS framework was used to identify eligible studies. 30 The inclusion criteria were as follows:
Population: Stroke survivors aged ≥60 years, 3 or with a mean age ≥60 in studies including participants of any age; diagnosed with haemorrhagic, ischaemic or recurrent stroke; and discharged from hospital to home, with or without family caregivers.
Intervention: Interventions were implemented during both pre-discharge and post-discharge periods to support older stroke survivors and/or caregivers in the transition from hospital to home, lasting up to six months after discharge; initiated by nurses or a multidisciplinary team, with nurses performing at least one of the following tasks: assessing patients’ and/or caregivers’ needs, providing discharge planning, health education, self-management support, health coaching or conducting follow-up after discharge.24–28
Comparison: Other interventions or usual care.
Outcome: Older stroke survivors: activities of daily living, depression, anxiety, quality of life, self-efficacy, stroke-related knowledge and satisfaction with care. Caregivers: self-efficacy, caregiver burden, quality of life and satisfaction with care. Healthcare service utilisation: emergency department visits and hospital readmissions. Measurement: outcomes were assessed at baseline and at all follow-up points after discharge.
Study design: Any published randomised controlled trials (RCTs) or cluster-RCTs.
Studies were excluded if the mean age of stroke survivors was under 60 years or if participants were discharged to care homes or nursing care facilities. Interventions delivered only pre- or only post-discharge, those lasting beyond six months post-discharge and those led by multidisciplinary teams without clear delineation of nurses’ roles or involvement were excluded.
All records were imported into Covidence, with duplicates removed by one reviewer (UA). Two reviewers (UA, LK) independently screened titles and abstracts, resolving discrepancies through discussion. Full texts of eligible studies were independently reviewed (UA, LK), with disagreements resolved via discussion or consultation with a third reviewer (DAS). Further clarification was sought from six studies regarding sample details, nursing roles and intervention data. The selection process was documented using a PRISMA flow diagram. 29
A bespoke data extraction form was used to capture key details from each eligible study (i.e. authors, publication year, country, design, participant characteristics, intervention/comparator details and outcomes). Intervention descriptions followed the Template for Intervention Description and Replication (TIDieR) checklist. 31 Outcome data were collected at baseline, post-intervention and follow-up (if any). The data extraction form was pilot tested (UA, LK) using two studies, then refined. A subset of studies (n = 4, 24%) underwent independent double extraction by two authors (UA and LK or DAS), with discrepancies resolved through discussion. The remaining 13 studies were extracted by one author (UA).
Risk of bias was assessed using the Cochrane Risk of Bias 2 tool for randomised trials (RoB2) 32 and its extension for cluster-RCTs (RoB 2 CRT). 33 Two authors (UA and LK or DAS) independently assessed four studies, resolving discrepancies through discussion or third-author arbitration if needed. One author (UA) conducted initial quality assessments for the remaining studies, with another (LK) verifying judgements and any disagreements resolved by the third author when necessary. Certainty of evidence for each outcome was rated using GRADE (high, moderate, low, or very low) 34 by one author (UA) and checked by a second (LK).
A narrative synthesis was used to summarise study characteristics, participant demographics, intervention components and underpinning theories. Meta-analysis was undertaken using Review Manager 5 (RevMan5) when data from two or more studies were available. 35 For duplicate reports of the same study, only one dataset was used. Treatment effects were assessed post-intervention and at follow-ups 36 (1, 3 and 6 months). Where standard deviations were missing, they were calculated from standard errors 36 using RevMan5. Mean differences (MDs) with 95% confidence intervals (CIs) were pooled for continuous outcomes, while standardised mean differences (SMDs) were used when multiple measures assessed the same outcome. 36 Risk ratios (RRs) with 95% CIs were calculated for dichotomous outcomes (e.g. hospital readmission). Due to the complexity and heterogeneity of the intervention characteristics, it was anticipated that the effects of the interventions would vary across studies, making it unlikely that a single common effect size could be assumed. A random-effects model was chosen to estimate the expected distribution of intervention effects. CIs were estimated using the Wald-type method. 35 Heterogeneity was assessed using Tau2, I2 and forest plots. 35 Restricted Maximum Likelihood was used to estimate variance. 35 Sensitivity analysis excluded studies with high or unclear risk of bias to evaluate the robustness of the findings in a meta-analysis. Post-hoc subgroup analyses explored the impact of intervention duration, theory, contact mode, provider type, contact intensity and number of components on activities of daily living and readmission rates. Selective outcome reporting was evaluated by comparing the analyses pre-specified in the study protocol or outcome measures and analyses listed in the methods section of each study with those published. 37 A funnel plot was employed to visually assess publication bias when the meta-analysis included ten or more studies. 37
Results
The search identified 11,888 records. After duplicates were removed, 7441 records were screened for titles and abstracts. Of these, 7338 records were removed because they did not meet the review criteria, and two full-text articles could not be retrieved. The remaining 101 reports, along with an additional three reports identified through reference lists of included studies, underwent full-text screening for eligibility. Eighty-four reports did not meet the inclusion criteria. In total, there were 20 articles reporting on 17 trials included in this systematic review (Figure 1).
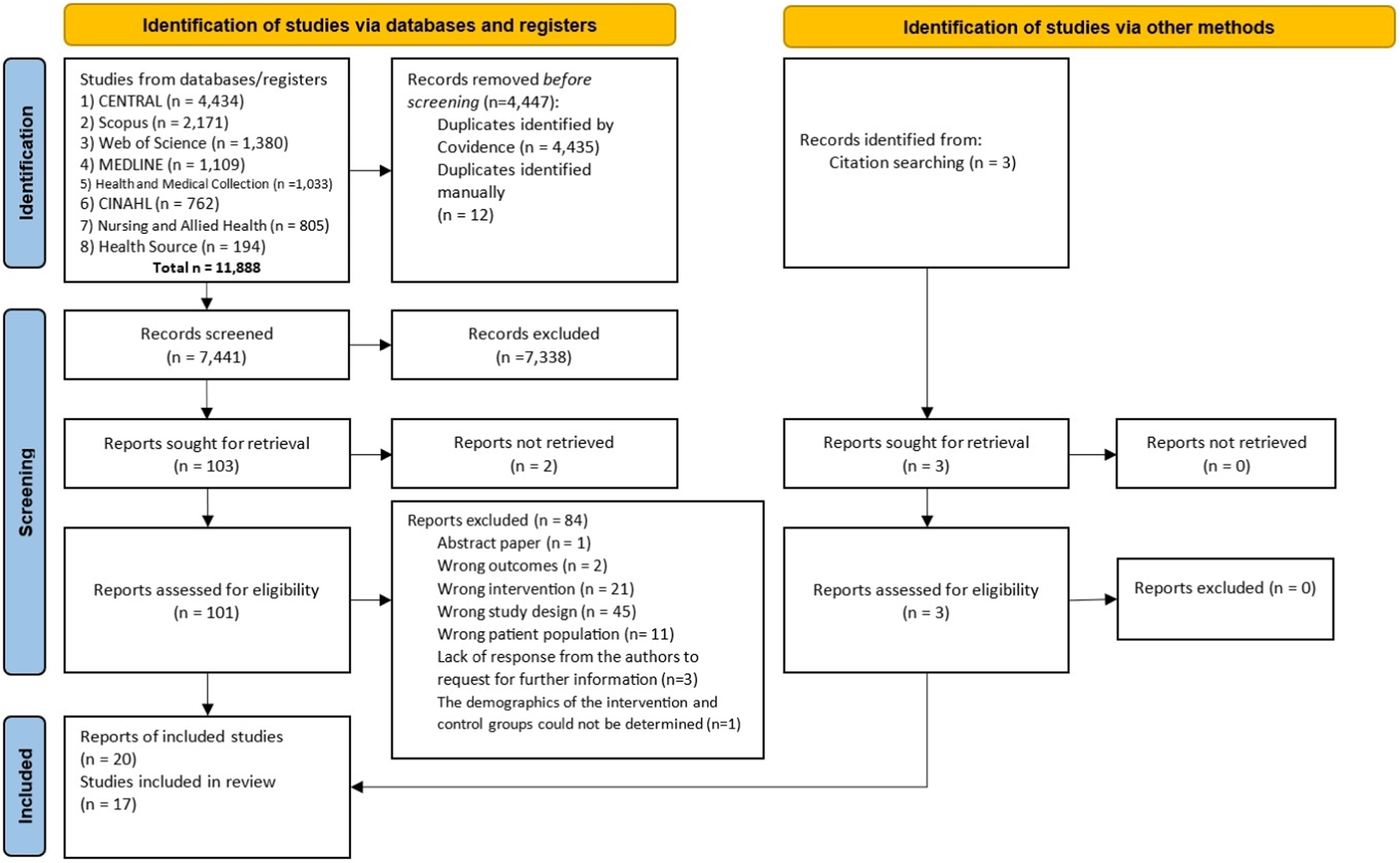
PRISMA flow diagram of search process.
The risk of bias assessments for the included studies are summarised in Figure 2 and Supplemental Tables 4 and 5. Six studies were assessed as having a low risk of bias,25,28,38–41 while some concerns were noted in six studies,26,42–46 and five studies were assessed as having a high risk of bias.27,47–50 The main methodological issues identified were as follows: several trials reported unclear details regarding randomisation methods, inconsistencies in measurement time points, and insufficient information about missing outcome data. Four included studies reported outcomes according to a prespecified plan for outcome measures and analyses, as outlined in pre-trial protocols,27,39–41 and outcomes reported in 13 studies followed the plan listed in the methods section. None of the selected studies employed a double-blind design, owing to the nature of the interventions, which focused on health-related behaviour change and relied on patient-reported outcome measures. Funnel plots could not be used to evaluate publication bias due to the small number of included studies in the meta-analysis. 37
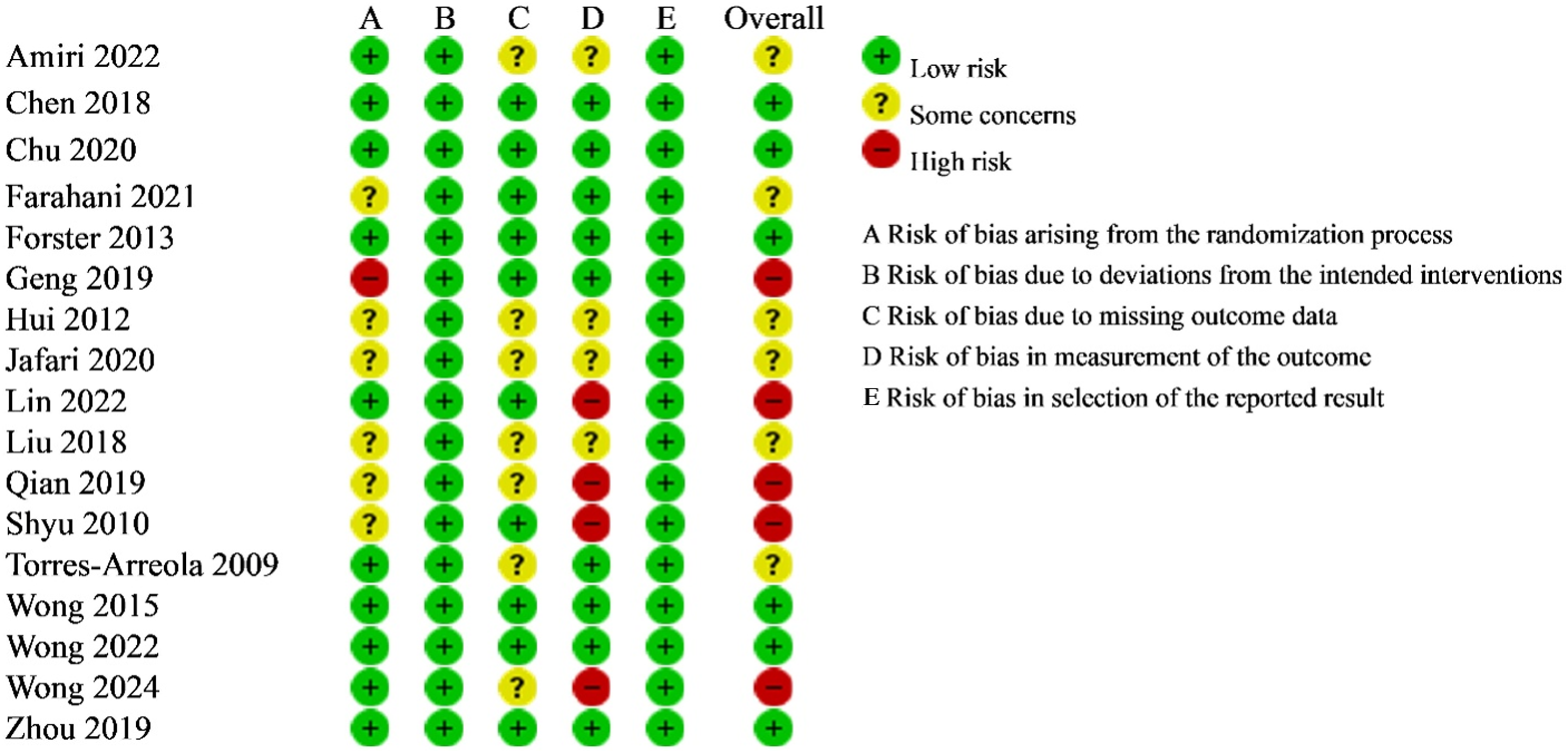
Risk of bias of included studies.
The details of the study characteristics are shown in Table 1 and Supplemental Table 3. Sixteen studies were RCTs, and one study was a cluster-RCT. 40 Eleven studies were conducted in China,25,27,28,38,39,41,43,45,47,48,50 three in Iran,26,42,44 one in Taiwan, 49 one in UK 40 and one in Mexico. 46 Twelve studies recruited solely stroke survivors, while five studies recruited both stroke survivors and caregivers.26,27,40,41,49 Participants were recruited from stroke units or neurological wards (n = 13) and acute stroke care settings (n = 4). The sample sizes of stroke survivors ranged from 20 to 478 in each group, with a total of 1276 intervention stroke participants and 1264 stroke participants in the control groups. The mean age of stroke survivors ranged from 60.20 (4.35) to 76.32 (4.56) years. Nine studies had participants with both ischaemic and haemorrhagic stroke, and two studies had only ischaemic patients, while six studies did not report the type of stroke.26,28,45,46,48,50 In 11 studies, interventions were delivered solely by nurses, whereas in six studies,28,40,42,45,47,50 they were provided by nurses in collaboration with other multidisciplinary team members (i.e. medical staff, psychologists, physiotherapists and social workers). Interventions were initiated 48–72 h after admission (n = 3),44,46,49 after patients’ conditions had stabilised (n = 9),26–28,38–41,48,50 prior to discharge (n = 5),25,42,43,45,47 and continued into the post-discharge period (n = 17), lasting 2 weeks to 6 months with follow-up periods of 2 weeks to 12 months. The most frequently reported outcomes were activities of daily living (n = 11) and quality of life (n = 11). Intervention materials of the included studies were brochures for exercise programs, educational booklets, videos, training manuals, a stroke self-management home care toolkit, and a stroke health coaching diary. Control groups received standard or usual care, which was articulated differently across studies, including discharge planning, health education, rehabilitation training, follow-up and home visits.
Characteristics of included studies.
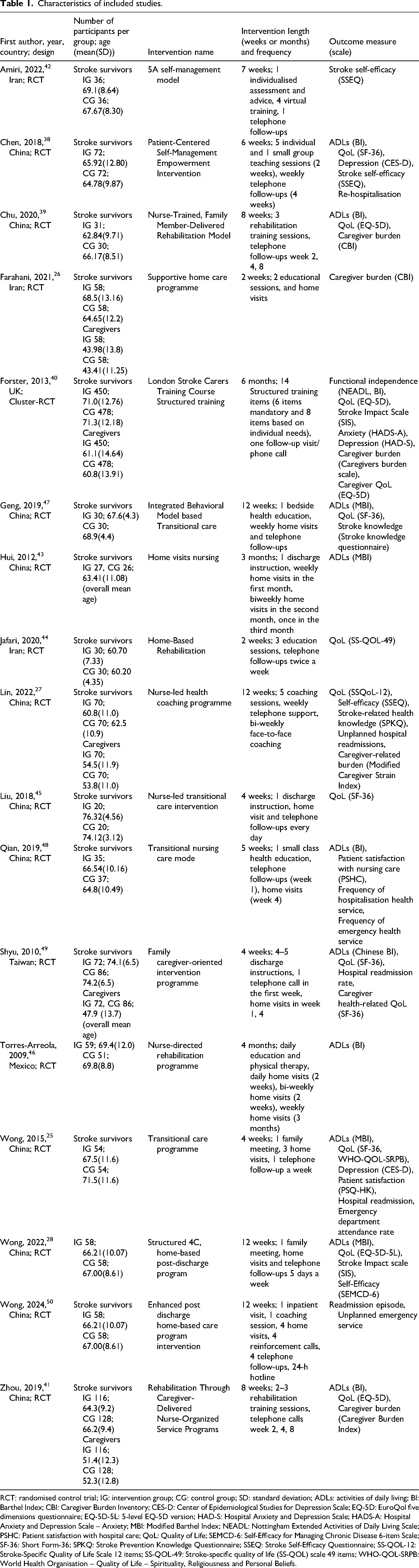
RCT: randomised control trial; IG: intervention group; CG: control group; SD: standard deviation; ADLs: activities of daily living; BI: Barthel Index; CBI: Caregiver Burden Inventory; CES-D: Center of Epidemiological Studies for Depression Scale; EQ-5D: EuroQol five dimensions questionnaire; EQ-5D-5L: 5-level EQ-5D version; HAD-S: Hospital Anxiety and Depression Scale; HADS-A: Hospital Anxiety and Depression Scale – Anxiety; MBI: Modified Barthel Index; NEADL: Nottingham Extended Activities of Daily Living Scale; PSHC: Patient satisfaction with hospital care; QoL: Quality of Life; SEMCD-6: Self-Efficacy for Managing Chronic Disease 6-item Scale; SF-36: Short Form-36; SPKQ: Stroke Prevention Knowledge Questionnaire; SSEQ: Stroke Self-Efficacy Questionnaire; SS-QOL-12: Stroke-Specific Quality of Life Scale 12 items; SS-QOL-49: Stroke-specific quality of life (SS-QOL) scale 49 items; WHO-QOL-SRPB: World Health Organisation – Quality of Life – Spirituality, Religiousness and Personal Beliefs.
Transitional care interventions comprised multiple components, predominantly health education (n = 15, 88%), goal setting and personalised care planning (n = 10, 59%), functional rehabilitation (n = 9, 53%), patient- and caregiver-centred assessment (n = 9, 53%) and self-management (n = 5, 29%) (Supplemental Table 3 and Table 6). Health education was implemented either as a comprehensive package or curriculum,26,27,40,44,48 or integrated into transitional care.28,38,41–43,45–47,49–50 Goal setting and planning were conducted to promote behavioural change, enhance self-care skills25,27,28,38,42,43,45 and support physical function recovery.39,41,50 Rehabilitation plans and practical rehabilitation training sessions were developed with support from physiotherapists or medical specialists.27,28,38,39,41,43,45,46,48 Patient- and caregiver-centred assessment mainly focused on patients’ health status, functional abilities, stroke-related knowledge and health behaviours.25,28,38,40,42,45,47,49,50 Self-management was primarily structured around comprehensive case management.25,28,38,42,50 Eleven studies reported using underpinning theories or frameworks (Supplemental Table 6), which included the Omaha System,25,28,48,50 Transitional Care Framework, 28 Brunnstrom's Stages of Recovery,46,48 Naylor's Transitional Care Model,25,45 the Behavioural Model, 47 the 5A Self-Management Model, 42 the Health Empowerment Model, 38 Self-Efficacy Theory 27 and the Motor Relearning Theory. 41
The effects of transitional care interventions were assessed based on outcomes for older stroke survivors, caregivers and the utilisation of health care services. The meta-analyses are presented first, followed by a narrative review of findings from studies not included in the meta-analyses.
Activities of daily living: Eleven studies assessed activities of daily living. Pooled results showed an effect in favour of the intervention group compared with the control group at 1 month25,38,43,49 (RE, SMD 0.54, 95% CI 0.12 to 0.97, I2 = 79%, 4 trials, 463 participants) and at 3 months28,38,39,41,43,48,49 (RE, SMD 0.43, 95% CI 0.12 to 0.74, I2 = 78%, 7 trials, 848 participants) (Figure 3). The certainty of the evidence was rated as very low due to risk of bias, inconsistency and imprecision (Supplemental Table 7). The effect remained significant in the sensitivity analysis after excluding studies with some concerns regarding the risk of bias (Supplemental Figures S2 and S4). There was no effect in favour of the intervention on activities of daily living at 6 months28,39,41,47,49 (RE, SMD 0.25, 95% CI −0.05 to 0.55; I2 = 70%) (Supplemental Figure 1). The findings indicated that the intervention produced a medium effect on activities of daily living at 1 month and 3 months, but not at 6 months, as determined by the SMD effect size interpreted according to Cohen's rules of thumb (0.2 = small, 0.5 = medium, 0.8 = large). 51 Two studies not included in the meta-analysis showed no significant improvements in activities of daily living at 6 months40,46 and 12 months (MD 0.2, 95% CI −0.5 to 0.8). 40
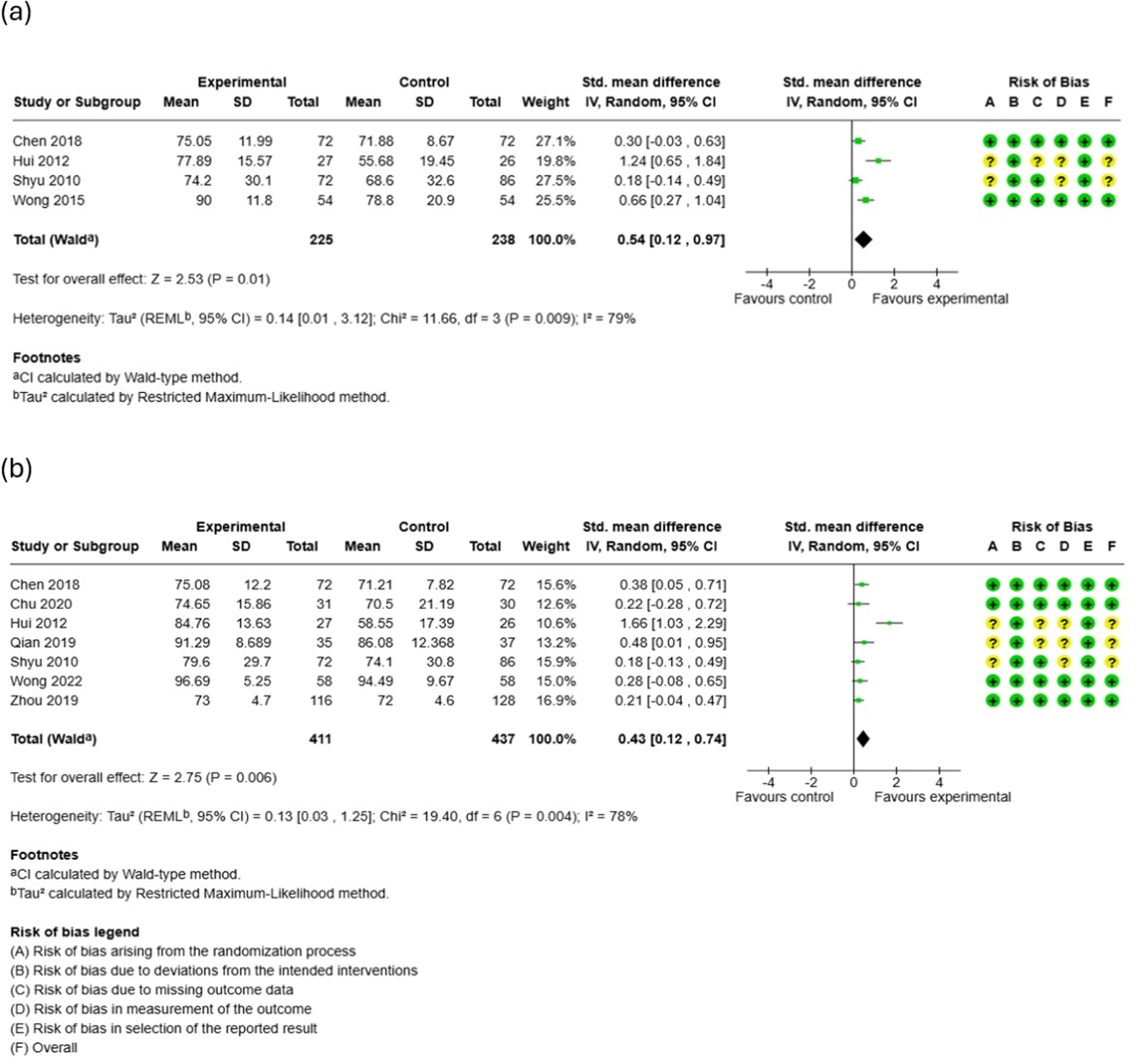
Forest plots for activities of daily living (ADLs) at (a) 1 month and (b) 3 months.
Quality of life: Quality of life was measured in 11 studies. Using the SF-36, the pooled effect sizes for quality of life subdomains showed significant between-group differences in the Mental Component Score at 1 month25,38 (RE, MD 0.73, 95% CI 0.34 to 1.12, I2 = 0%, 2 trials, 252 participants) (Figure 4). The certainty of the evidence was rated as low due to imprecision (Supplemental Table 7). There were no significant differences for the Mental Component Score at 3 months25,38 (RE, MD 0.88, 95% CI −0.50 to 2.25, I2 = 41%, 2 trials, 252 participants) (Supplemental Figures 2). No differences were observed in the Physical Component Score at either 1 or 3 months25,38 (Supplemental Figures 3 and 4). At 6 months, pooled results showed a favourable effect for the intervention group compared with the control group in the Role Limitations due to Physical Problems component score45,47,49 (RE, MD 7.70, 95% CI 0.17 to 15.23, I2 = 20%, 3 trials, 258 participants) and the General Health component score45,47,49 (RE, MD 5.32, 95% CI 0.87 to 9.77, I2 = 0%, 3 trials, 258 participants) (Figure 5). The certainty of the evidence was rated as very low due to risk of bias and imprecision (Supplemental Table 7). No significant between-group differences were found for the remaining six subdomains of the SF-3645,47,49 (Supplemental Figures 5–10). Six studies not included in the meta-analysis considered this outcome. As the overall quality of life score, one showed significant improvements in 1 month and 3 months (p < 0.001). 44 Two showed significant improvements in quality of life at 3 months and 6 months.27,28 Three studies found no effect on quality of life at 6 months.39–41
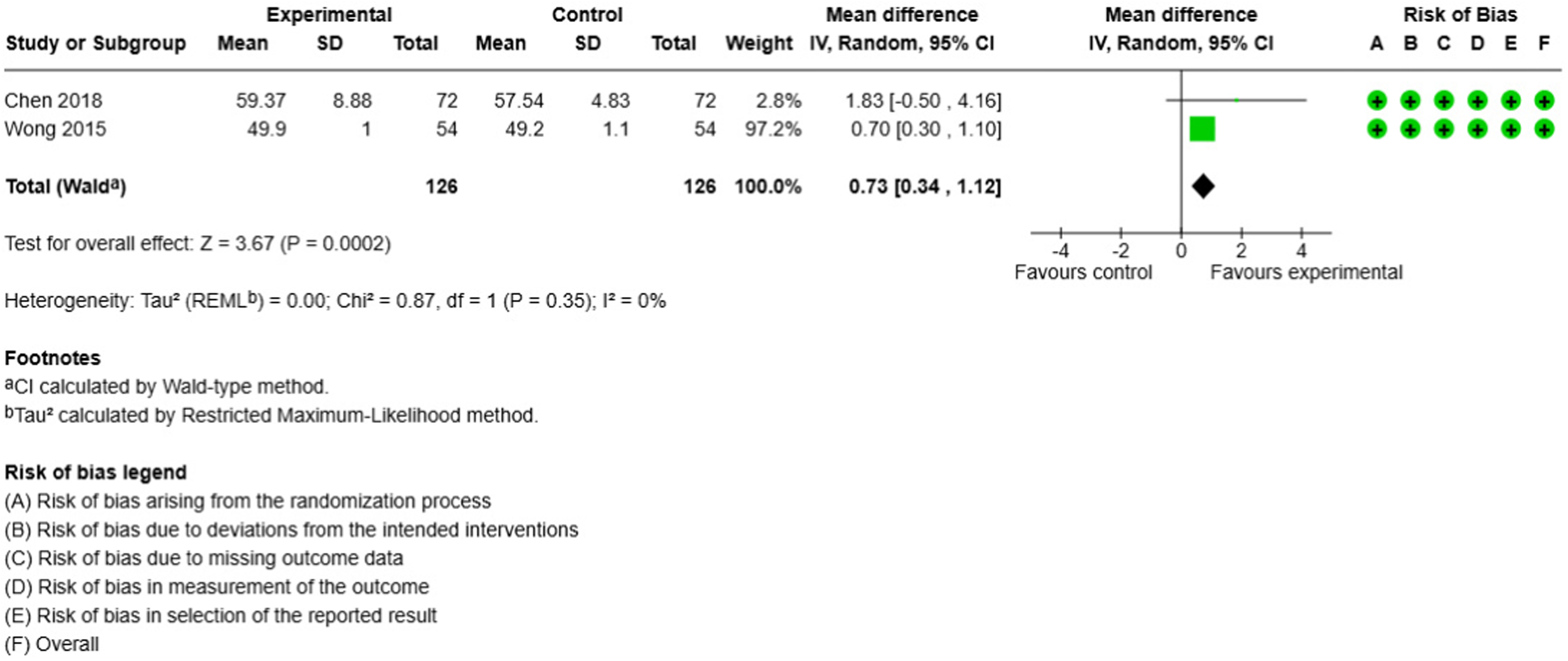
Forest plots for the mental component score (MCS) at 1 month.
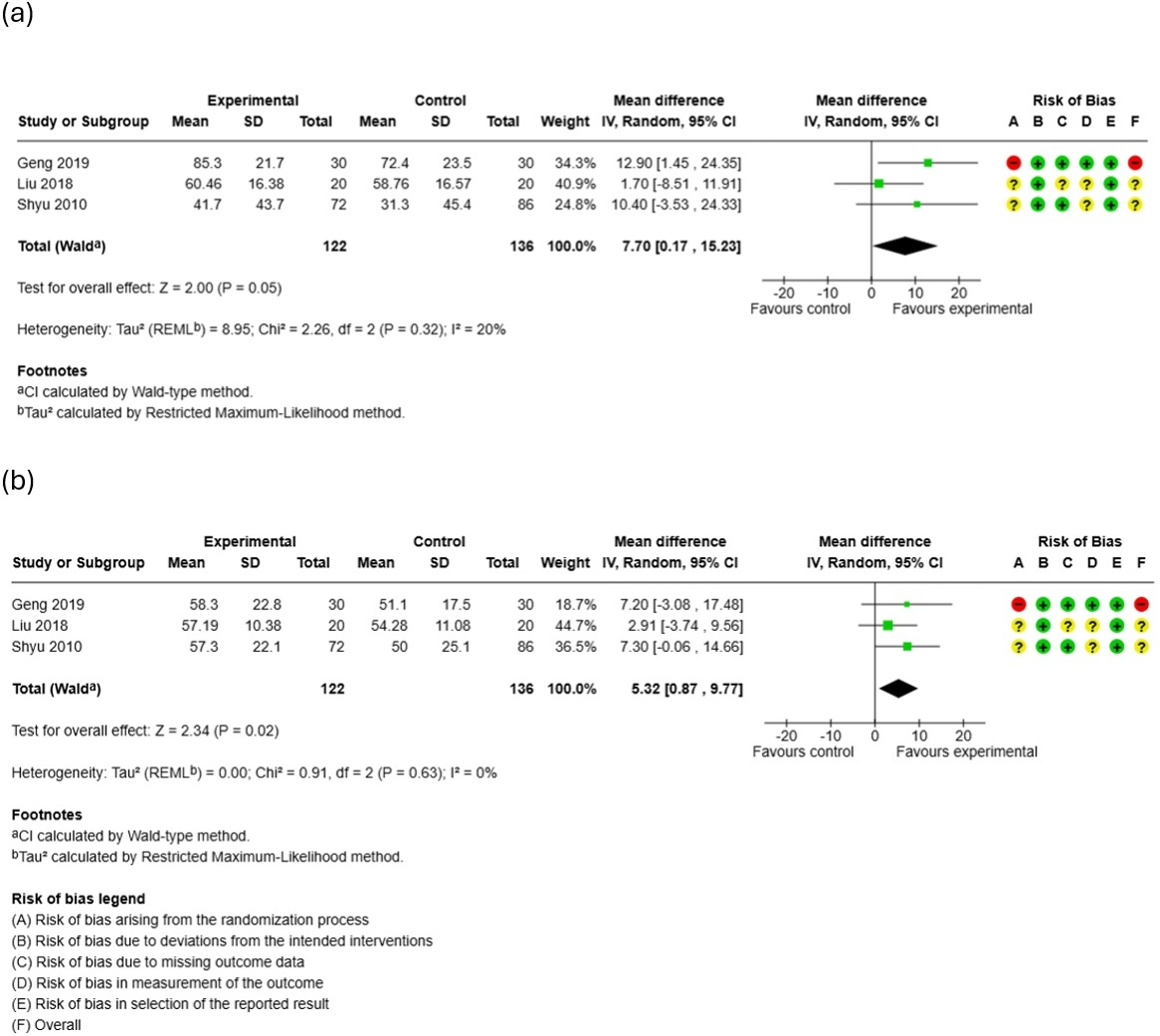
Forest plots for (a) the role limitations due to physical problems (RP) at 6 months and (b) the general health component (GH) at 6 months.
Depression and anxiety: Depression was measured in three studies. Meta-analysis of two studies showed no effect in favour of transitional care interventions on depression at 1 month25,38 (RE, SMD −1.08, 95% CI −2.19 to 0.03, I2 = 94%) (Supplemental Figure 11). A cluster-RCT 40 found no important between-group differences in depression at 6 months (MD 0.1, 95% CI −0.5 to 0.7) and 12 months (MD −0.4, 95% CI −1.1 to 0.3), or in anxiety at 6 months (MD 0.1, 95% CI −0.5 to 0.7) and 12 months (MD −0.2, 95% CI −0.9 to 0.3).
Self-efficacy: Self-efficacy was measured in four studies. Pooled results indicated no effect in favour of transitional care interventions on self-efficacy at 3 months27,28,38 (RE, SMD 6.95, 95% CI −5.86 to 19.76, I2 = 100%) and 6 months27,28 (RE, SMD 9.84, 95% CI −8.73 to 28.42, I2 = 100%) (Supplemental Figures 12 and 13). One study 42 not included in the meta-analysis considered this outcome and showed a statistically significant improvement in self-efficacy scores at 6 weeks (p < 0.001) and 18 weeks (p < 0.001).
Stroke-related knowledge: Stroke-related knowledge was measured in two studies. Meta-analysis showed no effect in favour of transitional care interventions on stroke knowledge at 3 months (RE, SMD 15.73, 95% CI −13.20 to 44.66, I2 = 100%)27,47 and 6 months (RE, SMD 14.41, 95% CI −11.67 to 40.50, I2 = 100%)27,47 (Supplemental Figures 14 and 15).
Patient satisfaction: Two studies reported the effect of the intervention on patient satisfaction with care.25,48 Meta-analysis indicated an effect in favour of transitional care interventions up to 3 months (RE, SMD 3.62; 95% CI 1.08 to 6.17, I2 = 96%, 2 trials, 180 participants; very low certainty of evidence (downgraded for inconsistency and imprecision)), effect was sustained in sensitivity analysis excluding studies with some concern (Supplemental Figure 16, Figure S7, Table 7).
Caregiver burden: Caregiver burden was measured in five studies. Pooled results of three studies27,39,41 reported no effect in favour of transitional care interventions on caregiver burden at 6 months (RE, SMD −6.77, 95% CI −20.02 to 6.47, I2 = 100%) (Supplemental Figure 17). Two studies26,40 not included in the meta-analysis considered this outcome. One showed significant differences between groups at two weeks post-discharge (p < 0.001), 26 and the other showed no significant between-group differences at 6 months (MD 0.5, 95% CI −1.7 to 2.7). 40
Caregiver quality of life, self-efficacy, satisfaction: Caregiver self-efficacy and satisfaction with care were not considered in the included studies, and only two studies40,49 evaluated caregivers’ quality of life. One study found no significant difference between the two groups at 1, 3, 6 and 12 months. 49 A cluster-RCT 40 found no significant improvement in caregivers’ quality of life at 6 months (MD −0.014, 95% CI −0.044 to 0.016) and 12 months (MD 0.019, 95% CI −0.013 to 0.050).
Healthcare utilisation: Six studies evaluated the effect of the intervention on hospital readmission, while three studies examined the effect on emergency department visits. The meta-analysis results indicated an effect in favour of transitional care interventions on hospital readmission up to 3 months25,38,48 (RE, RR 0.54; 95% CI 0.30 to 0.97; I2 = 0%, 3 trials, 324 participants) (Figure 6). The effect was sustained in sensitivity analysis excluding studies with high risk of bias (Supplemental Figure S9). The certainty of the evidence was rated as very low due to risk of bias and imprecision (Supplemental Table 7). There were no between-group differences in hospital readmission at 6 months27,49 (RE, RR 0.50, 95% CI 0.21 to 1.18, I2 = 52%) or in emergency department visits up to 3 months25,48 (RE, RR 0.42, 95% CI 0.09 to 2.00, I2 = 50%) (Supplemental Figures 18 and 19). One study 50 not included in the meta-analysis considered this outcome and showed statistically significant differences in emergency department visits at 6 months.
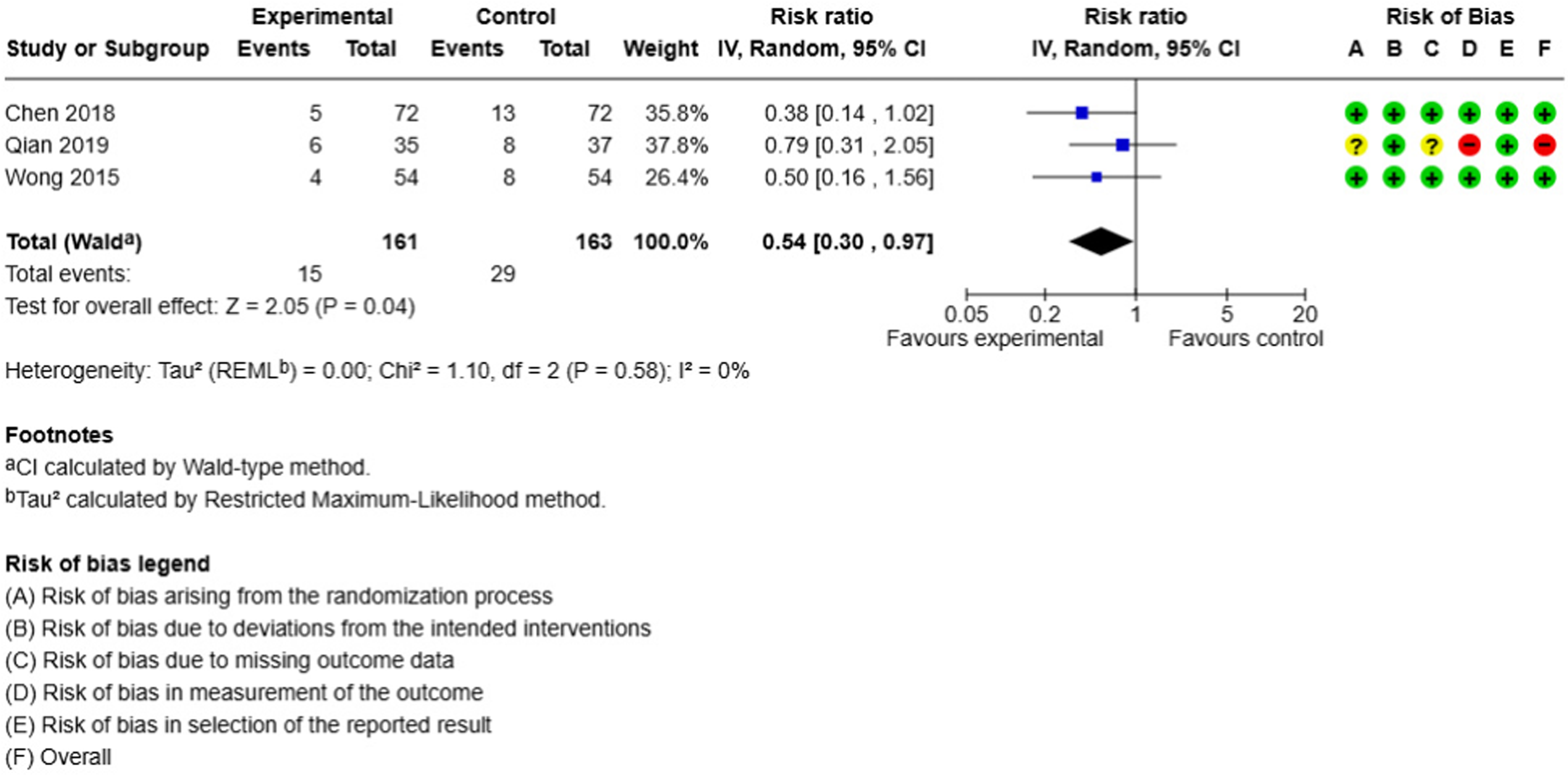
Forest plot for hospital readmissions up to 3 months.
Subgroup analysis: The post-hoc subgroup analyses are presented in Supplemental Figures G1.1 to G2.3. We found differences in the effects on activities of daily living in the subgroup analyses by contact mode and number of intervention components. The pooled SMDs of activities of daily living in the trials using home visits or phone calls alone and those using a combination of home visits and phone calls were 0.53 (95% CI −0.20 to 1.26) and 0.30 (95% CI 0.08 to 0.51), respectively. The pooled SMDs in the trials applied 2–3 components, and 4–5 components were 0.47 (95% CI −0.09 to 1.04) and 0.35 (95% CI 0.10 to 0.59), respectively. We found no difference in the effect of the findings across subgroup analyses on hospital readmissions.
Discussion
Our meta-analysis shows that nurse-initiated transitional care with pre- and post-discharge components improved activities of daily living at 1 and 3 months. It also improved the Mental Component Score of quality of life at 1 month and the Role Limitations due to Physical Problems and General Health domains at 6 months post-discharge. These interventions enhanced patient satisfaction and reduced 3-month hospital readmissions. Sensitivity analysis excluding studies with some concerns or a high risk of bias showed stable effects on daily activities, satisfaction and readmissions. The certainty of evidence was low to very low. There were no significant effects on depression, anxiety, self-efficacy, stroke knowledge, emergency visits or caregiver burden. A meta-analysis of caregivers’ quality of life, self-efficacy and satisfaction was not possible due to limited data.
Although nurse-initiated transitional care interventions improved short-term activities of daily living in older stroke survivors, these benefits diminished once the intervention ended, consistent with prior studies showing gains at 3 months that are not sustained at 6–12 months.16,17 The reduced long-term effects observed in this review may be due to limited self-management or poor adherence following the intervention. Our subgroup analysis found multi-component transitional care produced greater three-month improvements, with home visits plus phone calls outperforming single approaches. This moderate effect indicates meaningful benefits for physical recovery in older stroke survivors.
The effects of transitional care on the subdomains of quality of life in older stroke survivors after discharge contrast with those of O’Callaghan et al., who found improvements in the Physical Component Score at 3 months, but no effects on the Mental Component Score or either subdomain of the SF-36 at 6–12 months in adult stroke survivors. 17 Lin et al. reported positive effects of transitional care on the overall quality-of-life score at 3 months post-discharge. 16 According to Bandura's self-efficacy theory, persistence in activities can be produced through mastery experiences, and perceived self-efficacy predicts performance. 52 Despite self-management strategies maintaining self-efficacy and improving quality of life for both stroke survivors and caregivers, 38 our review reveals that transitional care interventions primarily focus on health education rather than self-management support, which may lead to a lack of sustained improvement over time. In addition, most interventions were designed without input from stroke survivors or family members.25,38–40,42–50 Engaging key stakeholders in designing an intervention is therefore crucial for understanding the problem, prioritising needs and developing solutions for long-term self-efficacy in real-world settings. 53
The findings on the effects of depression and anxiety in our review contrast with previous reviews, which reported reductions in depression at 3 months post-discharge 16 and in both anxiety and depression between 6 and 12 months. 17 Depression in older stroke survivors relates to low self-esteem, limited social support and reduced functional ability. 54 Nurses and health professionals should recognise the risk and severity of depression and anxiety in this group, routinely screen, and provide emotional support and coping skills. 55 Caregivers play a vital role in supporting older stroke survivors’ physical and psychological health as they return home.6–8 It is necessary to involve caregivers in transitional care and provide support to help them cope with their caregiving burden. 26
This review's strength lies in its robust methodology, aligned with PRISMA guidelines. 29 Several limitations should be noted. It is possible that some literature was missed due to the language and date limitations. The scope of this study was intended to encompass complex nursing transitional care interventions, leading to a broad search strategy that yielded a very large number of records, despite the language and date filters. We need to be cautious about analysis reporting bias, as most included studies did not publish a study protocol, limiting comparisons of changes in pre-specified outcomes. Variability across intervention characteristics and heterogeneity in outcome measurement made estimating the true effect size for each outcome challenging. Random-effects models were used to estimate pooled intervention effects and to address limitations in effect-size homogeneity, and heterogeneity was explored through post hoc subgroup analyses. 35 The pooled effects are limited to associations observed across studies and cannot identify potential causal mechanisms, as inferences are made about the effectiveness of transitional care interventions as a whole, rather than for specific programmes or components. The overall certainty of the evidence was low to very low, due to high risk of bias or concerns, small sample sizes and high heterogeneity. The included studies were predominantly conducted in East Asia (China) and the Middle East (Iran), with only two originating in Europe and North America. The transferability of the findings of this study, or the adaptation of interventions for a new setting, needs to be considered in terms of intervention-context fit with healthcare systems, cultural contexts and target population. 56
In conclusion, nurses play a central role in transitional (hospital-to-home) care, as intervention providers, case managers and team collaborators, supporting post-discharge recovery in older stroke survivors.27,28,38,39,41,43–45,47–49 Effective nurse-led transitional care should incorporate patient- and caregiver-centred assessment, goal setting, personalised care planning, stroke-specific education, self-management support, rehabilitation and a combination of home visits and phone calls to optimise outcomes. However, evidence is largely limited to short-term effects. Future research should confirm these findings, examine intervention intensity and duration, and incorporate the perspectives of survivors, caregivers and multidisciplinary teams to strengthen long-term effectiveness.
Nurse-led hospital-to-home programs may boost short-term effects on activities of daily living, quality of life and satisfaction, and reduce readmissions – though current evidence remains low-certainty. Multicomponent models (including home visits, follow-up calls and self-management support) show the most promise for enhancing activities of daily living recovery over time. Co-design of transitional care interventions with diverse stakeholders, including people with lived experience, is essential to support translation into practice.Clinical messages
Supplemental Material
sj-docx-1-cre-10.1177_02692155261430092 - Supplemental material for Nurse-initiated transitional care interventions to support the transition from hospital to home amongst older stroke survivors and caregivers: A systematic review and meta-analysis
Supplemental material, sj-docx-1-cre-10.1177_02692155261430092 for Nurse-initiated transitional care interventions to support the transition from hospital to home amongst older stroke survivors and caregivers: A systematic review and meta-analysis by Usanee Ankanawin, Lisa Kidd and Dawn A Skelton in Clinical Rehabilitation
Footnotes
Author contributions
UA and LK conceptualised the review, conducted the systematic literature search and screened studies. UA, LK and DAS contributed to extracting data, assessed the quality and risk of bias in the included studies, performed the statistical analysis, interpreted the results, discussed implications and approved the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.