
Abstract
Design
Pragmatic, two-arm, parallel-group, superiority randomised controlled trial with assessor-blinding and statistician-blinding.
Setting
Single orthopaedic centre in Shanghai, China.
Participants
One hundred and eighty adults (aged 18–50 years) with femoroacetabular impingement syndrome scheduled for hip arthroscopy were randomised to prehabilitation (n = 90) or usual care (n = 90).
Intervention
The prehabilitation group received 6 weeks of supervised exercise, education and home activity before surgery. Controls received standard preoperative advice. All patients received identical postoperative rehabilitation.
Main measures
The primary outcome was the Harris Hip Score at 24 weeks. Secondary outcomes included pain, maximal hip muscle strength, range of motion, dynamic balance, quality of life, mental health and cost.
Results
At 24 weeks, the Harris Hip Score did not differ significantly between groups (adjusted between-group difference 0.98 points [95% CI −0.11 to 2.07], p = 0.08). At 4 and 12 weeks, differences numerically favoured prehabilitation (1.52 points, uncorrected p = 0.02; 1.14 points, uncorrected p = 0.04) but did not reach significance after Bonferroni correction (threshold p < 0.0167). Secondary outcomes favoured prehabilitation, including pain, maximal hip strength, range of motion and dynamic balance, though all between-group differences were below published thresholds for clinically important change.
Conclusions
Prehabilitation before hip arthroscopy for femoroacetabular impingement syndrome was associated with small early improvements that did not reach statistical significance for the primary outcome after correction for multiple comparisons and were below clinically important thresholds. Total costs did not differ significantly between groups.
Trial registration number
ChiCTR2500113298 (Chinese Clinical Trial Registry, https://www.chictr.org.cn/, date of registration: 26 November 2025). This trial was registered retrospectively.
Keywords
Introduction
For many young adults, chronic hip and groin pain is attributable to femoroacetabular impingement syndrome. 1 This condition is characterised by abnormal contact between the femoral head–neck and acetabulum (cam or pincer morphology) that damages the labrum and cartilage and can lead to early osteoarthritis.1,2 Hip arthroscopy is the standard surgical treatment to correct the underlying cam or pincer morphology, and trials have shown it yields better short-term outcomes than conservative care.3,4 However, not all patients achieve optimal recovery after surgery. In one trial, only about half of patients had a significant improvement 1 year after arthroscopy. 3 Similarly, a large registry study of nearly 5000 cases found that roughly one-third of patients failed to reach an optimal outcome. 5 These findings suggest that factors beyond surgical correction influence postoperative outcomes.
Researchers have identified several factors that could be addressed to improve outcomes. A longer duration of preoperative symptoms is linked to worse postoperative results. 6 Patients with femoroacetabular impingement syndrome often have deficits in hip muscle strength and range of motion. 7 Psychological distress such as depression or anxiety can also negatively affect recovery. 8 Addressing these issues before surgery may help maximise functional gains.
Pre-operative rehabilitation, or prehabilitation, is a strategy to optimise a patient's condition before surgery and improve recovery. 9 It typically consists of a structured exercise and education programme in the weeks prior to surgery to enhance strength, flexibility and mental readiness. In orthopaedic patients, prehabilitation has shown benefits such as increased muscle strength, reduced pain and better health-related quality of life compared to standard care.10,11 It also encourages patients to take an active role, which may reduce anxiety and improve engagement in rehabilitation.
Despite the promise of prehabilitation in other areas, its effectiveness before surgery for femoroacetabular impingement syndrome remains unclear. Only one small pilot trial has examined prehabilitation before hip arthroscopy for femoroacetabular impingement, which suggested better early post-operative outcomes with pre-operative exercise training but had methodological limitations. 12 Thus, a rigorous evaluation is needed. We designed a randomised controlled trial to test whether a 6-week prehabilitation programme before hip arthroscopy for femoroacetabular impingement syndrome can improve post-operative outcomes compared to usual care. We hypothesised that the prehabilitation group would achieve greater improvements in Harris Hip Score and other outcomes than the control group.
Methods
Ethics and permissions
This study was approved by the Ethics Committee of the participating hospital (approval number: 2024-KY-217(K)). All procedures were conducted in accordance with the ethical standards of human research, including the principles outlined in the Declaration of Helsinki. Written informed consent was obtained from every participant before randomisation.
Study design and setting
This trial was designed as a pragmatic, two-arm, parallel-group, superiority randomised controlled study evaluating the intervention under routine clinical conditions. Randomisation allocated participants evenly into two groups, and outcome assessment was assessor-blinded and statistician-blinded, meaning the investigators measuring the endpoints and the statistician analysing the data were kept unaware of group assignments to minimise bias.
Participants were recruited from September 2024 to July 2025 at a single centre. The trial took place at one of the National Centres for Orthopaedics in China, which served as the only site for all patient enrolments and interventions.
This trial was registered retrospectively (ChiCTR2500113298, Chinese Clinical Trial Registry; date of registration: 26 November 2025). Although retrospective, the registration was completed before any data analysis, and the registered protocol matches the study as conducted. No separate published protocol was available for this trial. No formal data monitoring committee was convened. The intervention consisted of a low-risk, exercise-based programme with no pharmacological component, and the trial had a relatively short intervention period (6 weeks) using a well-established surgical procedure. An independent safety monitor reviewed all serious adverse events as they occurred. Given these factors and the absence of interim efficacy analyses, a formal data monitoring committee was not deemed necessary, consistent with guidance for low-risk behavioural interventions. The trial had no external sponsor or funding source, and all aspects of study design, implementation, and analysis were investigator-initiated and academically driven.
Participants
Participants from the surgical waiting lists for hip arthroscopy for femoroacetabular impingement syndrome were screened and enrolled from the orthopaedic clinics of a tertiary referral hospital. Eligible participants were required to meet all of the inclusion criteria, and patients were excluded from the study if any of the exclusion criteria applied. The inclusion and exclusion criteria are shown in Table 1.
Inclusion and exclusion criteria.
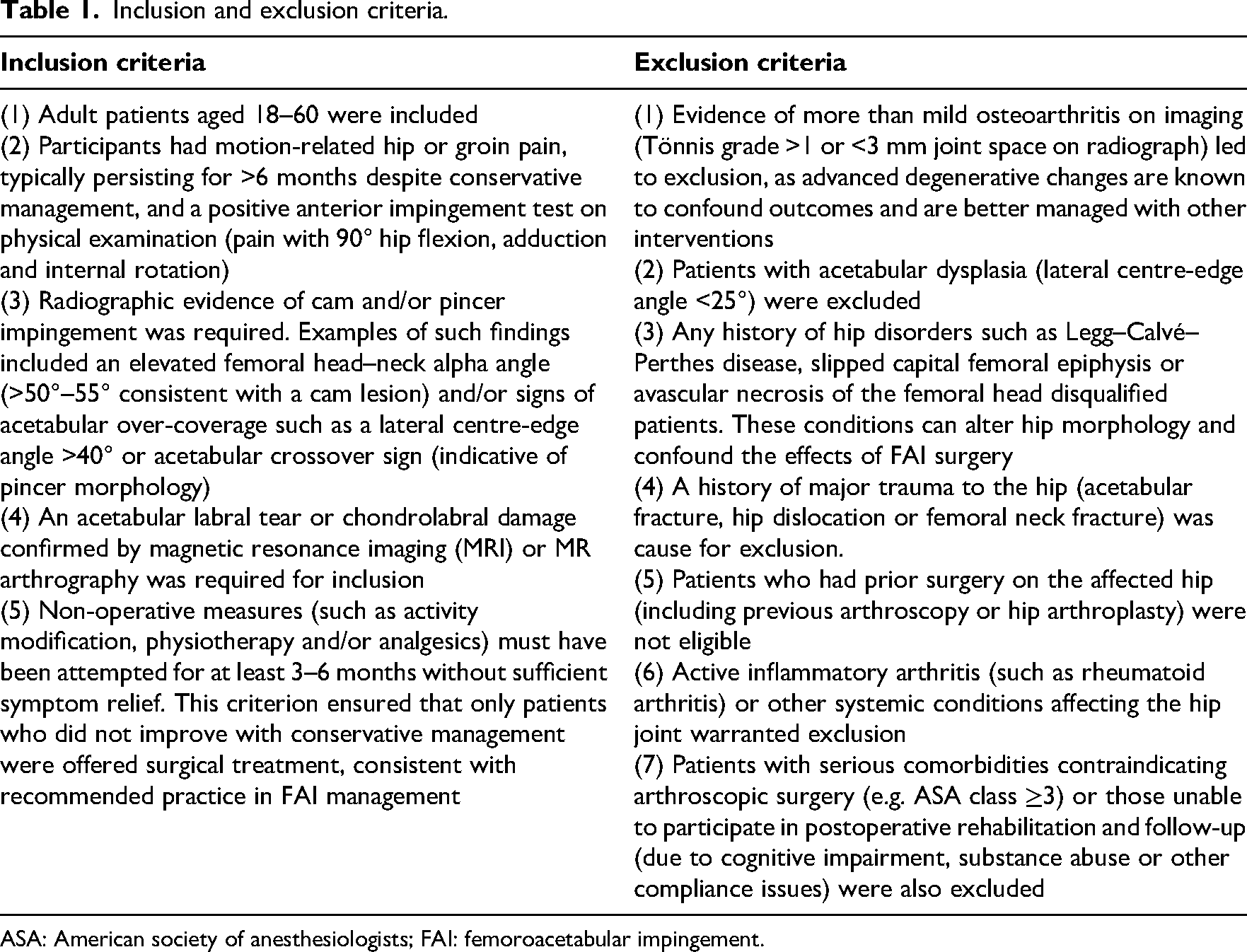
ASA: American society of anesthesiologists; FAI: femoroacetabular impingement.
Intervention
Patients assigned to the prehabilitation arm participated in a structured 6-week pre-surgical rehabilitation programme prior to hip arthroscopy. This programme was designed from prior evidence in hip arthroscopy prehabilitation10–12 to optimise patients’ readiness for surgery across multiple domains. Under the guidance of a physiotherapist, patients attended supervised exercise sessions 5 days per week at the hospital physiotherapy clinic. Each session focused on targeted exercises to improve maximal hip muscle strength and joint range of motion, as well as neuromuscular control training for better balance and movement mechanics. An education component was included to inform patients about their upcoming surgery and recovery, aiming to reduce anxiety and align expectations. The programme was individualised based on each patient's baseline assessment, with exercises progressed or modified according to the patient's ability and symptoms. Participants were encouraged to continue prescribed home exercises outside of clinic sessions to reinforce gains. Attendance and adherence to the prehabilitation sessions were tracked, and any adverse events or symptom exacerbations were recorded throughout the pre-surgical period.
Patients in the control group did not receive a structured pre-operative exercise regimen. They continued with usual care in the weeks before surgery, meaning they were given the standard hospital advice to remain as active as tolerable and routine educational materials, but no formal supervised exercise.
Both groups received identical standard post-operative rehabilitation after surgery.
The detailed prehabilitation programme as well as the standard postoperative rehabilitation are shown in the Supplemental materials.
Outcomes and data collection
The primary outcome was the Harris Hip Score at 24 weeks post-surgery, a clinician-administered measure of hip function and pain originally developed to evaluate results after hip arthroplasty. 13 The Harris Hip Score assigns a total score out of 100 (higher scores indicate better hip function) based on domains of pain, daily activities, gait, deformity and range of motion. We used the original Harris Hip Score rather than the modified version. We acknowledge that the Harris Hip Score was not specifically developed or validated for the femoroacetabular impingement population, and patient-reported outcome measures such as the international Hip Outcome Tool (iHOT-33) or the Hip Outcome Score are now recommended for this group. We selected the Harris Hip Score because it was the primary outcome used in the only prior prehabilitation trial for hip arthroscopy, 12 facilitating comparison, and because a validated Chinese-language version was available at our institution. This choice represents a limitation that may affect the sensitivity of the instrument to detect clinically meaningful change in our population.
Secondary outcomes included patient-reported pain (Visual Analogue Scale), objective performance measures of hip function (isokinetic maximal muscle strength, hip range of motion and Star Excursion Balance Test), patient-reported quality of life (36-Item Short Form Health Survey), psychological status (Hospital Anxiety and Depression Scale), and health economic outcomes.14–20 Details of outcome measures are shown in the Supplemental materials.
Sample size calculation
The required sample size was determined a priori based on the primary outcome, the Harris Hip Score. We pre-specified a clinically important between-group difference of eight points 21 and assumed a common standard deviation of 17 points based on published hip arthroscopy cohorts. 22 Using a two-sided alpha of 0.05 and 80% power, the calculation yielded 72 participants per group. To account for up to 20% loss to follow-up, the estimate was inflated by 25%, giving an enrolment target of 180 participants (90 per arm). The detailed narrative rationale is provided in the Supplemental materials.
Randomisation, allocation and blinding
We implemented a central computerised randomisation process to assign participants equally in a one-to-one ratio into the two study groups. The allocation sequence was generated using permuted blocks with randomly varying block sizes of four, six and eight participants to maintain balanced group numbers while preserving unpredictability. The detailed randomisation, allocation and blinding protocol is shown in the Supplemental materials.
Statistical analysis
Continuous variables were examined for normality using the Shapiro–Wilk test and visual Q–Q plots, and summarised as mean and standard deviation where approximately normally distributed. For each time point, outcomes in the two groups were compared and reported as the between-group difference (intervention minus control) with the corresponding 95% confidence interval. We interpreted results primarily using the magnitude and precision of these effect estimates. p-Values were reported as secondary information, with statistical significance assessed using two-sided tests at an alpha level of 0.05. p-Values are reported to two decimal places; values below 0.01 are reported as “p < 0.01” and values below 0.001 as “p < 0.001”, consistent with recognised reporting recommendations.
The primary efficacy analysis evaluated whether the prehabilitation intervention led to superior hip function (Harris Hip Score at 24 weeks postoperatively) compared to control, analysed in the intention-to-treat population. We employed a linear mixed-effects regression model for the Harris Hip Score, which included fixed effects for treatment group, time (as categorical follow-up visits), treatment-by-time interaction, patient age, sex and baseline Harris Hip Score. The model featured random intercepts for patients. To control the family-wise error rate for repeated between-group comparisons at three follow-up time points, we applied a Bonferroni adjustment, using a corrected alpha of 0.05/3 = 0.0167 for each pairwise comparison. Missing data were handled following the intention-to-treat principle; the mixed-effects model using maximum likelihood estimation uses all available longitudinal data and produces valid estimates under a missing-at-random assumption, so no imputation was applied. A per-protocol analysis was conducted as a sensitivity analysis. Cost-effectiveness was evaluated using the incremental cost-effectiveness ratio with non-parametric bootstrapping (1000 iterations). Full details of the model specification, diagnostic procedures, missing data strategy and cost-effectiveness methodology are provided in the Supplemental Statistical Methods.
Results
Participants
There were 201 participants screened for eligibility and 180 were finally enrolled for randomisation. The flow diagram of the study is shown in Figure 1. Baseline characteristics were balanced between the prehabilitation group (n = 90) and the usual care group (n = 90) in the intention-to-treat population. Demographic data are shown in Table 2. The femoroacetabular impingement subtype distribution was balanced. Other baseline clinical factors – symptom duration, previous treatments, comorbidities and baseline outcome measures (Harris Hip Score, Visual Analogue Scale for pain, maximal muscle strength, range of motion, Star Excursion Balance Test, 36-Item Short Form Health Survey, and Hospital Anxiety and Depression Scale) – did not differ significantly between groups. The per-protocol population had comparable baseline characteristics between the prehabilitation and usual care groups (Supplemental Table 1).
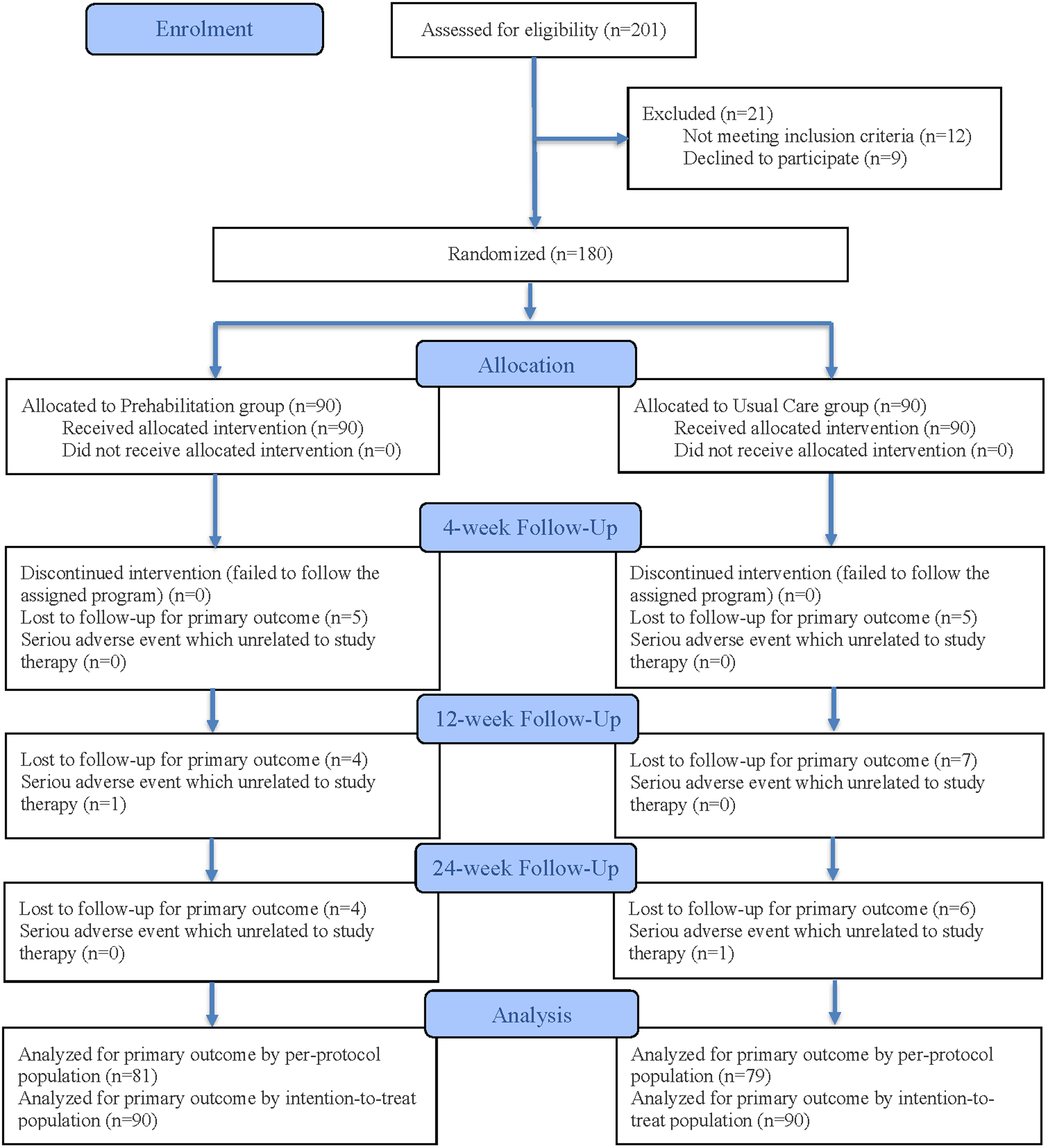
Flow diagram of the study.
Baseline characteristics of the prehabilitation group and usual care group (intention-to-treat population).
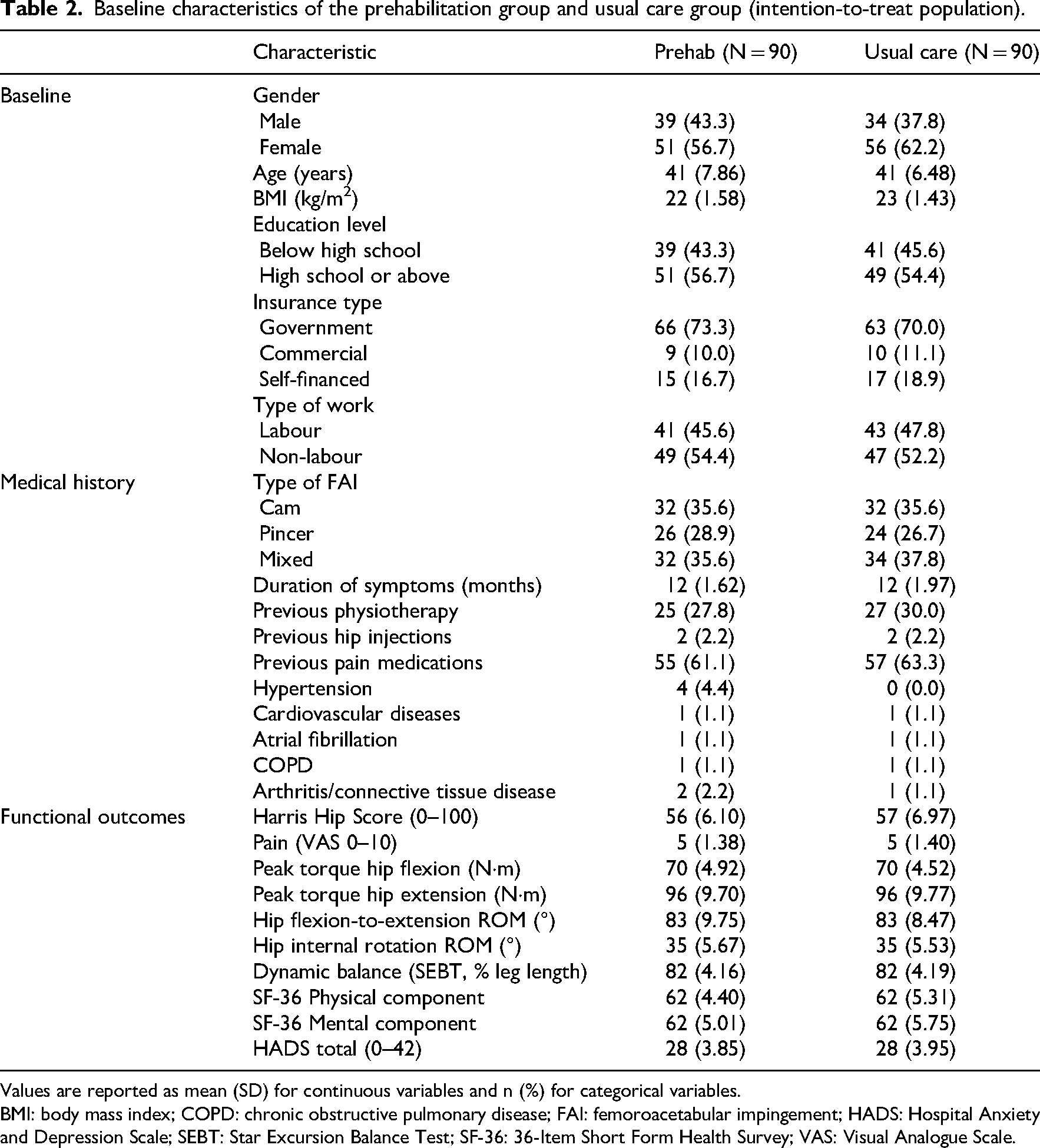
Values are reported as mean (SD) for continuous variables and n (%) for categorical variables.
BMI: body mass index; COPD: chronic obstructive pulmonary disease; FAI: femoroacetabular impingement; HADS: Hospital Anxiety and Depression Scale; SEBT: Star Excursion Balance Test; SF-36: 36-Item Short Form Health Survey; VAS: Visual Analogue Scale.
Outcomes
In the intention-to-treat population, the primary outcome (Harris Hip Score) improved from baseline in both groups by 24 weeks (Table 3). The adjusted between-group difference in change from baseline at 24 weeks was not statistically significant (mean group difference [95% CI] at 24 weeks: 0.98 [–0.11; 2.07], p = 0.08; Table 4). At 4 and 12 weeks, adjusted Harris Hip Score differences numerically favoured prehabilitation, with a mean group difference of 1.52 points (uncorrected p = 0.02) at 4 weeks and 1.14 points (uncorrected p = 0.04) at 12 weeks. However, after applying the pre-specified Bonferroni correction for three time-point comparisons (adjusted significance threshold p < 0.0167), neither the 4-week nor the 12-week comparison reached statistical significance (Bonferroni-adjusted p = 0.05 and p = 0.11, respectively).
Unadjusted changes in outcomes at weeks 4, 12 and 24 (intention-to-treat population).
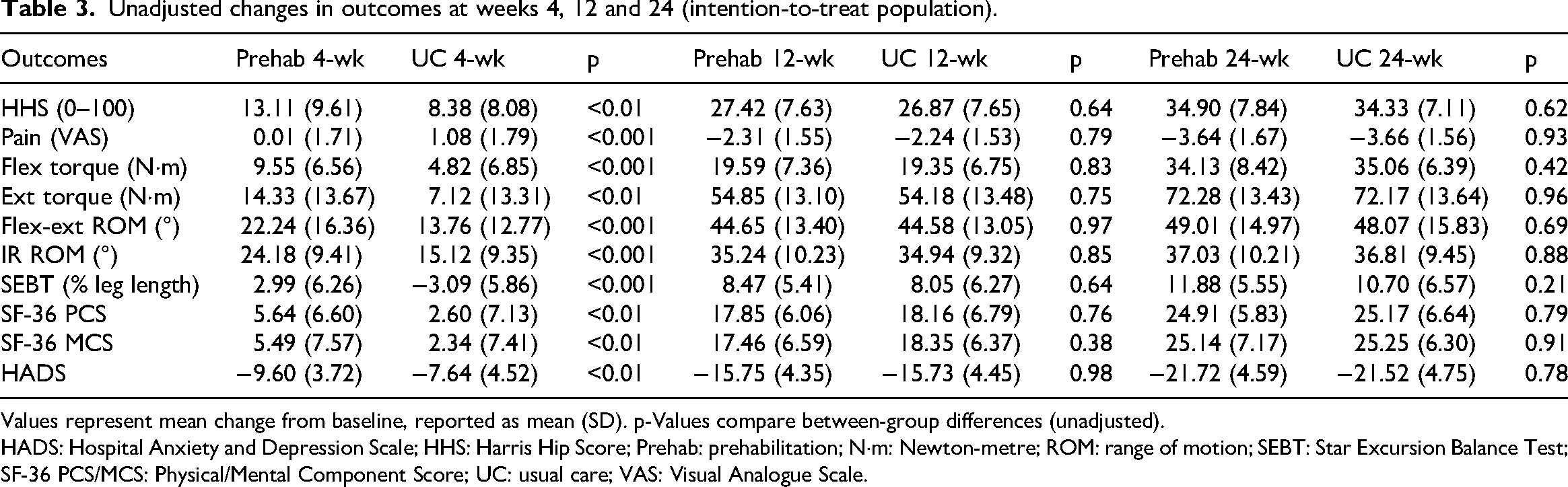
Values represent mean change from baseline, reported as mean (SD). p-Values compare between-group differences (unadjusted).
HADS: Hospital Anxiety and Depression Scale; HHS: Harris Hip Score; Prehab: prehabilitation; N·m: Newton-metre; ROM: range of motion; SEBT: Star Excursion Balance Test; SF-36 PCS/MCS: Physical/Mental Component Score; UC: usual care; VAS: Visual Analogue Scale.
Adjusted effectiveness at weeks 4, 12 and 24 (intention-to-treat population).
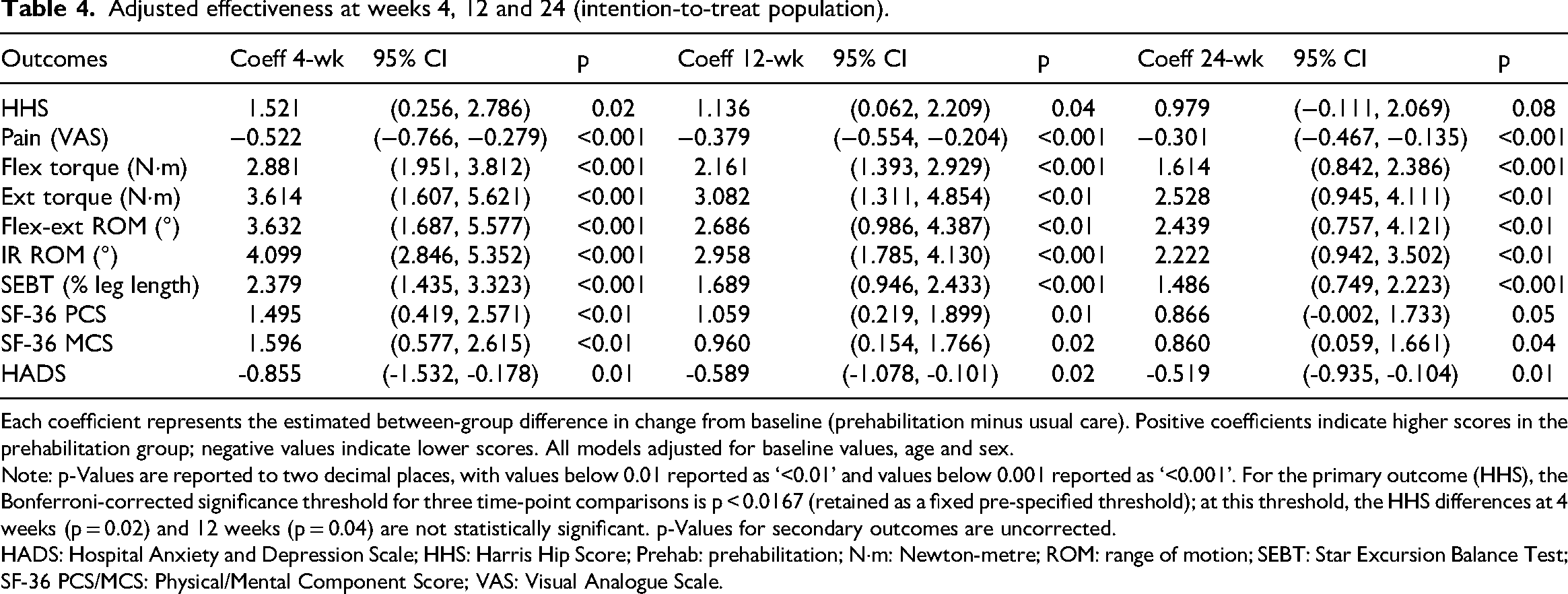
Each coefficient represents the estimated between-group difference in change from baseline (prehabilitation minus usual care). Positive coefficients indicate higher scores in the prehabilitation group; negative values indicate lower scores. All models adjusted for baseline values, age and sex.
Note: p-Values are reported to two decimal places, with values below 0.01 reported as ‘<0.01’ and values below 0.001 reported as ‘<0.001’. For the primary outcome (HHS), the Bonferroni-corrected significance threshold for three time-point comparisons is p < 0.0167 (retained as a fixed pre-specified threshold); at this threshold, the HHS differences at 4 weeks (p = 0.02) and 12 weeks (p = 0.04) are not statistically significant. p-Values for secondary outcomes are uncorrected.
HADS: Hospital Anxiety and Depression Scale; HHS: Harris Hip Score; Prehab: prehabilitation; N·m: Newton-metre; ROM: range of motion; SEBT: Star Excursion Balance Test; SF-36 PCS/MCS: Physical/Mental Component Score; VAS: Visual Analogue Scale.
Pain improved in both groups. At 24 weeks, the adjusted between-group difference on the zero-to-ten Visual Analogue Scale was 0.3 points lower in the prehabilitation group (p < 0.001). Maximal hip strength favoured prehabilitation at 24 weeks, with adjusted between-group differences of peak hip flexion torque higher by 1.6 N·m (p < 0.001) and peak hip extension torque higher by 2.5 N·m (p < 0.01). Hip range of motion at 24 weeks also favoured prehabilitation, with a 2.4° greater flexion-to-extension arc (p < 0.01) and 2.2° greater internal rotation (p < 0.01). Dynamic balance at 24 weeks, measured by Star Excursion Balance Test reach distance, was higher by 1.5% of leg length (p < 0.001). Quality of life improved in both groups. At 24 weeks, the 36-Item Short Form Health Survey physical component difference was 0.9 points (p = 0.05) and the mental component difference was 0.9 points (p = 0.04). Hospital Anxiety and Depression Scale scores improved in both groups, and at 24 weeks the prehabilitation group was 0.5 points lower (p = 0.01). Sensitivity analyses in the per-protocol population showed a consistent pattern of results (Supplemental Tables 2 and 3).
Although several secondary outcomes showed statistically significant between-group differences at the uncorrected alpha level, the absolute magnitudes were small. The between-group pain difference of 0.3 on a zero-to-ten scale was below the published minimal clinically important difference of 1.5 points after hip arthroscopy. 23 The 36-Item Short Form Health Survey component differences of approximately one point were below the commonly cited minimal important difference of three points. 24 The Hospital Anxiety and Depression Scale between-group difference of under one point was below a reported minimal clinically important difference of 1.7 points. 25 For the Harris Hip Score, published minimal clinically important difference values in hip arthroscopy for femoroacetabular impingement typically range from 7 to 17 points.26,27
In the intention-to-treat analysis at 24 weeks, total cost per patient was 101,251 Chinese Yuan (CNY) in the prehabilitation group and 94,101 CNY in the usual care group (Table 5). The prehabilitation group incurred a direct prehabilitation programme cost of 6980 CNY for the 6-week programme, which was the primary driver of the cost difference; the overall difference was not statistically significant (p = 0.06). The incremental cost-effectiveness ratio for the Harris Hip Score was 7303 CNY per point improvement (Table 6). For pain and the Hospital Anxiety and Depression Scale, the incremental cost-effectiveness ratio was negative; because these are outcomes where lower scores indicate better status, the prehabilitation group achieved more favourable scores at higher total cost, producing a negative ratio that is conventionally interpreted as cost-effective on that outcome dimension. The per-protocol sensitivity analysis (Supplemental Table 4) produced consistent results. Figure 2 shows the cost-effectiveness acceptability curves and Figure 3 shows the probabilistic sensitivity analysis.
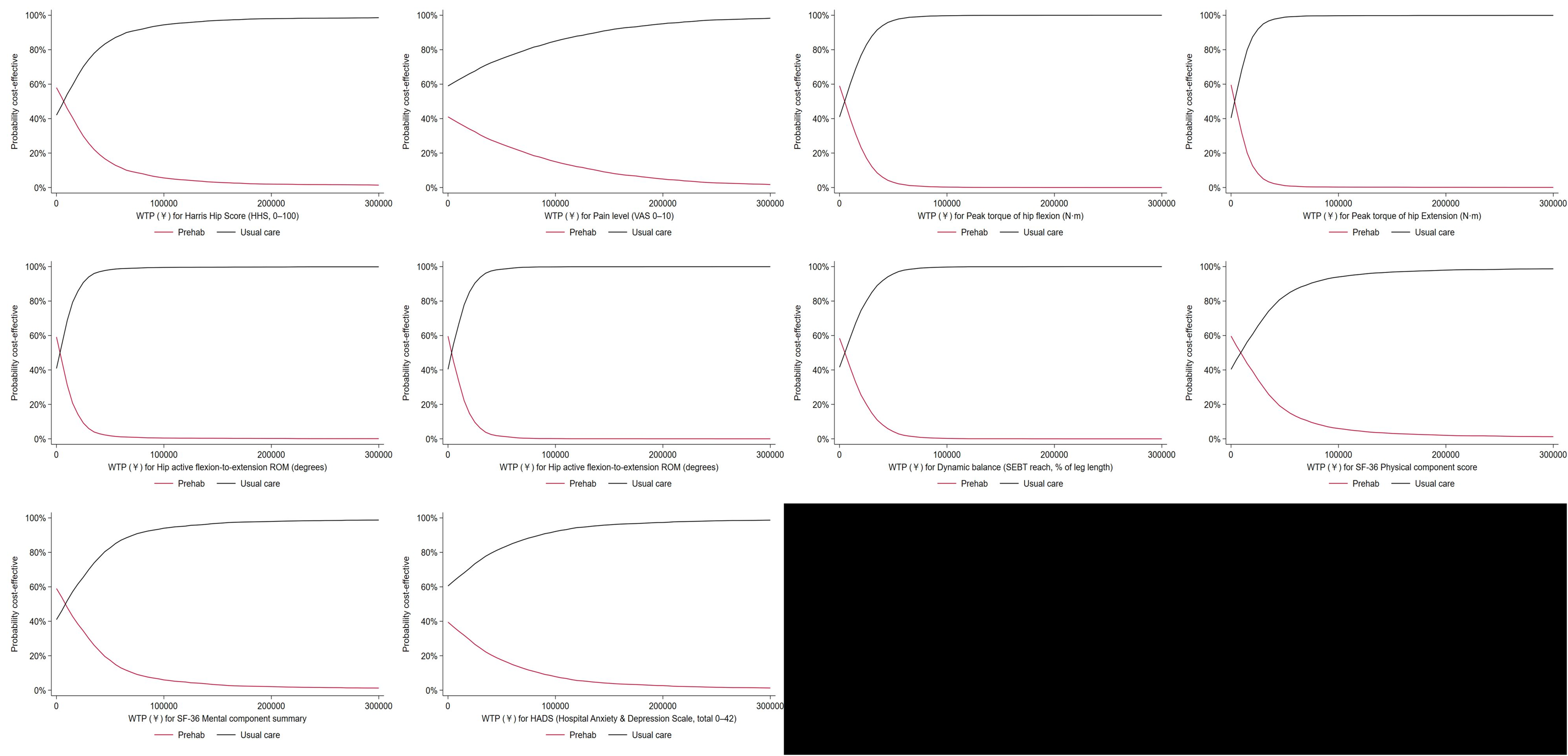
Cost-effectiveness acceptability curves for various indicators in the intention-to-treat analysis, comparing the prehabilitation group and the usual care group. The vertical axis illustrates the probability of each strategy being deemed cost-effective at different willingness-to-pay thresholds (horizontal axis). The horizontal axis ranges from one to three times China's per capita GDP in 2024.
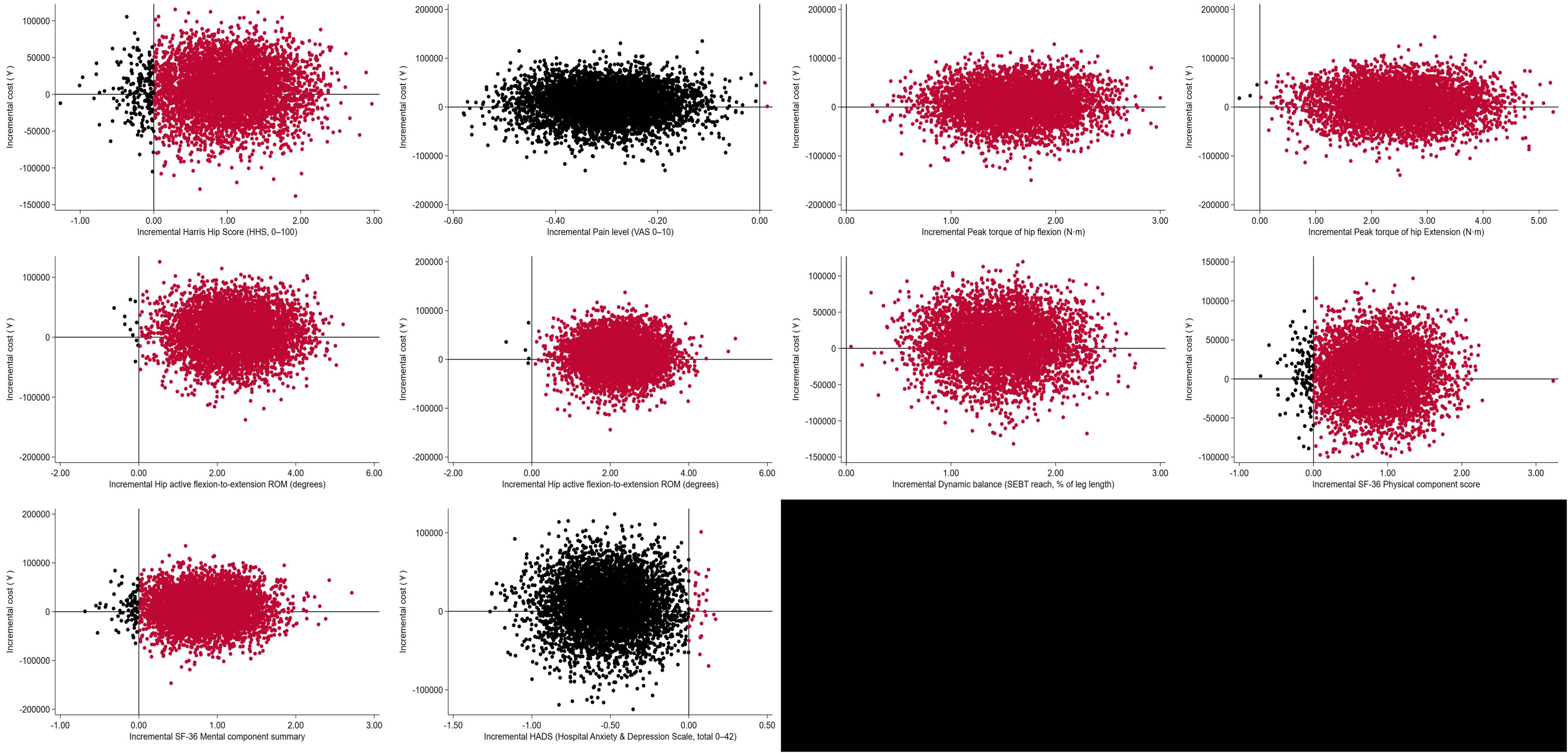
Probabilistic sensitivity analysis of the intention-to-treat set across different metrics, illustrating the distribution of incremental cost-effectiveness ratios for the prehabilitation group and the usual care group. Sampling was performed 5000 times using normal distributions for incremental benefits and gamma distributions for costs.
Costs of the prehabilitation group and usual care group at week 24 (intention-to-treat population).
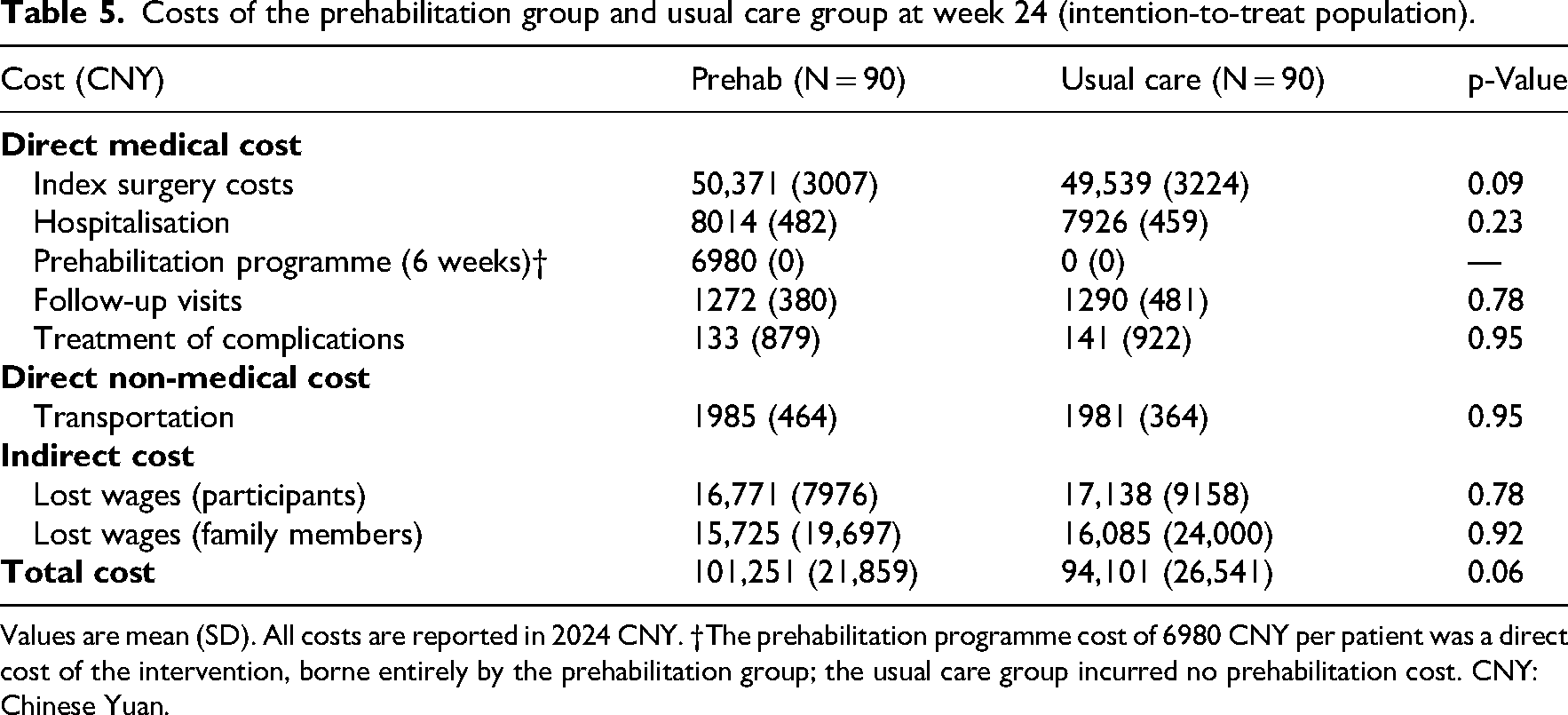
Values are mean (SD). All costs are reported in 2024 CNY. †The prehabilitation programme cost of 6980 CNY per patient was a direct cost of the intervention, borne entirely by the prehabilitation group; the usual care group incurred no prehabilitation cost. CNY: Chinese Yuan.
Incremental cost-effectiveness ratio (ICER).
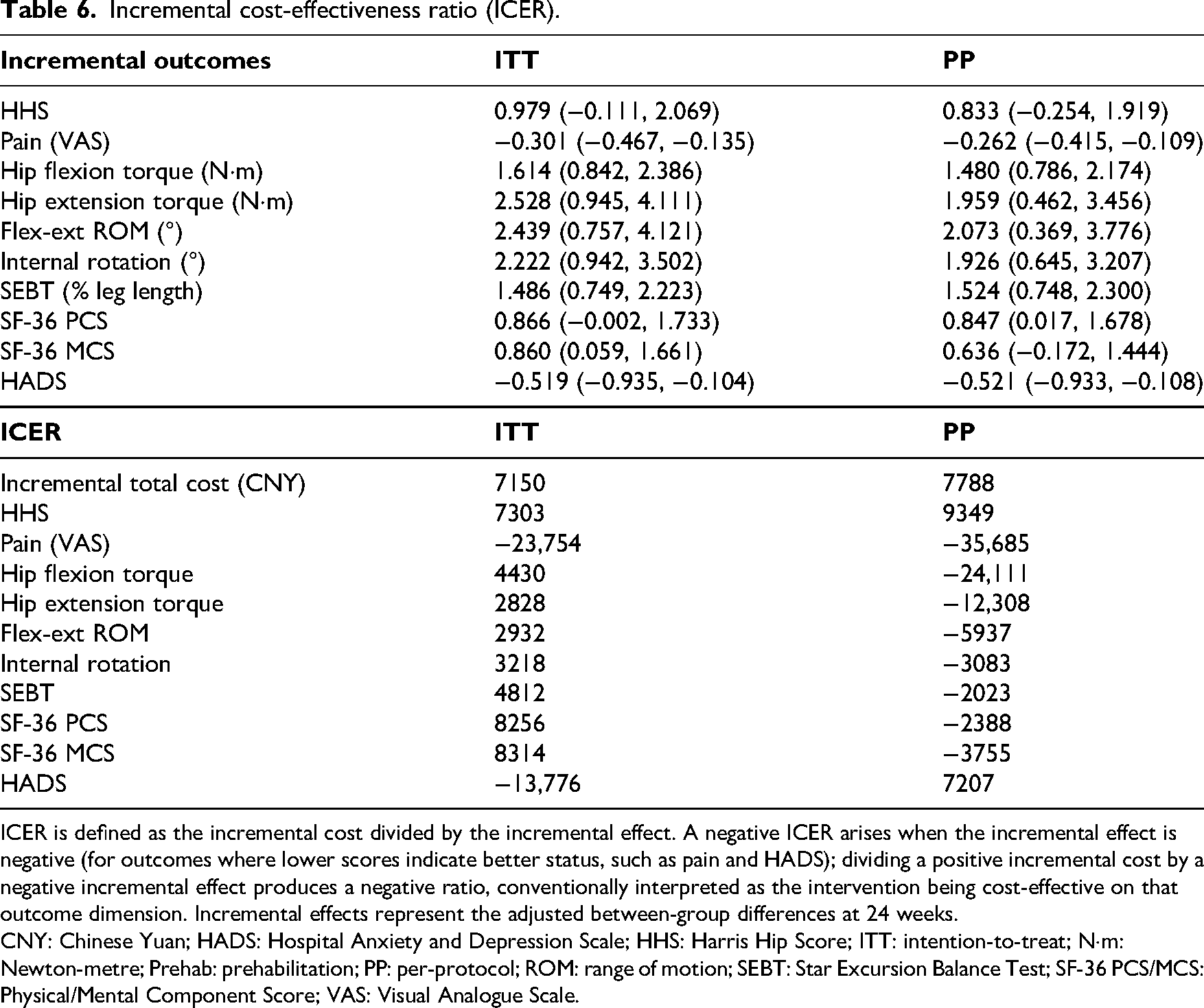
ICER is defined as the incremental cost divided by the incremental effect. A negative ICER arises when the incremental effect is negative (for outcomes where lower scores indicate better status, such as pain and HADS); dividing a positive incremental cost by a negative incremental effect produces a negative ratio, conventionally interpreted as the intervention being cost-effective on that outcome dimension. Incremental effects represent the adjusted between-group differences at 24 weeks.
CNY: Chinese Yuan; HADS: Hospital Anxiety and Depression Scale; HHS: Harris Hip Score; ITT: intention-to-treat; N·m: Newton-metre; Prehab: prehabilitation; PP: per-protocol; ROM: range of motion; SEBT: Star Excursion Balance Test; SF-36 PCS/MCS: Physical/Mental Component Score; VAS: Visual Analogue Scale.
Participants in the prehabilitation group completed 28.5 of 30 exercise sessions, 5.6 of 6 weekly self-examinations, and received 5.4 of 6 follow-up calls. They reported mean satisfaction ratings of 4.7 for the exercise component (Likert scale 1 to 5). Postoperative rehabilitation adherence did not differ significantly between groups, including sessions per week and average daily exercise time. The prehabilitation group completed more weekly assessments (Supplemental Table 5).
The proportion of participants with adverse events was 11.1% in the prehabilitation group and 8.9% in the usual care group, with 10 and 8 participants, respectively. One serious adverse event (1.1%) occurred in each group. In the usual care group, one patient developed a postoperative deep vein thrombosis requiring anticoagulation therapy; this was judged to be related to the surgical procedure. In the prehabilitation group, one patient required an unplanned surgical procedure unrelated to the prehabilitation programme. Neither serious adverse event was attributed to the prehabilitation intervention. All other adverse events were minor and are detailed in Supplemental Table 6.
Discussion
In this randomised controlled trial, adding a 6-week prehabilitation programme before hip arthroscopy for femoroacetabular impingement syndrome was associated with numerically faster early improvement in patient recovery compared to usual care. However, after applying the pre-specified Bonferroni correction, the Harris Hip Score did not reach statistical significance at any time point, and by 6 months after surgery both groups had achieved substantial gains. The primary outcome showed only a small between-group difference (mean group difference [95% CI] at 24 weeks: 0.98 [–0.11; 2.07]). Patients who underwent prehabilitation reported less pain and showed greater improvements in maximal hip muscle strength, joint range of motion and dynamic balance relative to those receiving usual care. Quality of life and psychological well-being also improved in both groups, with small additional gains in the prehabilitation group. These benefits were observed without a statistically significant increase in overall healthcare costs (p = 0.06). Adherence to the pre-surgery programme was high.
Our findings suggest that the prehabilitation programme mainly shifted the recovery trajectory earlier rather than producing a sustained advantage in hip function at 6 months. The adjusted between-group effect on the Harris Hip Score attenuated over time, from 1.5 points at week f4 to 1.1 points at week 12 and 1.0 points at week 24. Importantly, none of these comparisons reached statistical significance after Bonferroni correction for three time-point comparisons. This pattern is consistent with broader prehabilitation evidence in orthopaedic surgery, where postoperative benefits are often more apparent early while later differences are less consistent.11,28
The effect sizes for hip function were modest. Published minimal clinically important difference values for hip function scores such as the modified Harris Hip Score after hip arthroscopy for femoroacetabular impingement typically range from 7 to 17 points, with a 6-month estimate around 9 points.26,27 For this reason, we interpret the 6-month primary outcome as showing no clinically important advantage. The between-group pain difference of 0.3 on a zero-to-ten scale was below a published minimal clinically important difference of 1.5 points. 23 The 36-Item Short Form Health Survey component differences were approximately one point, below the commonly cited minimal important difference of three points. 24 The Hospital Anxiety and Depression Scale between-group difference was under one point, below a reported minimal clinically important difference of 1.7 points. 25 The early benefits may still matter to patients because they occur during the initial recovery window. Importantly, we found no evidence of harm; adverse event rates were low and comparable in both groups.
To our knowledge, the only prior trial focusing on prehabilitation before hip arthroscopy for femoroacetabular impingement was a small pilot study by Grant et al. 12 that suggested an 8-week exercise programme might improve post-operative muscle strength and patient-reported health status. Our larger trial reinforces those early observations. Notably, the prehabilitation group showed a slight but statistically significant reduction in anxiety and depression scores, though the absolute between-group difference on the Hospital Anxiety and Depression Scale was under one point, below the published minimal clinically important difference of 1.7 points. 25 Previous systematic reviews did not clearly show a mental health benefit from orthopaedic prehabilitation, 11 so this finding adds new nuance. The most defensible clinical message from our data is about timing: prehabilitation may improve early recovery across several domains but does not show a clear benefit for the 6-month primary endpoint.
This trial has several strengths, including concealed allocation and blinded outcome assessment, a relatively large sample size compared to prior studies, and comprehensive outcome measures encompassing clinical, functional, patient-reported and cost-effectiveness data. However, we acknowledge several limitations. First, the Harris Hip Score, our primary outcome, was not specifically developed or validated for the femoroacetabular impingement population; patient-reported outcome measures such as the iHOT-33 or the Hip Outcome Score are now considered more appropriate, and the use of the Harris Hip Score may have limited the sensitivity of our primary outcome to detect clinically meaningful change. Second, the study was conducted at a single high-volume orthopaedic centre, which may limit generalisability. Third, participants and therapists could not be blinded, introducing potential performance and response biases. Fourth, the control group received only usual care without a sham or active alternative, so the benefits observed might partly reflect the additional attention and exercise rather than the specific prehabilitation protocol alone. Fifth, our follow-up was limited to 24 weeks post-surgery; longer-term outcomes remain unknown. Sixth, the trial was registered retrospectively, though registration was completed before data analysis. Finally, some loss to follow-up occurred, and although we used intention-to-treat analyses, missing data could still introduce bias. These limitations do not change the key conclusion that prehabilitation produced small early differences that did not reach statistical significance for the primary outcome after Bonferroni correction, and that the between-group differences in patient-reported measures did not meet published thresholds for clinically important change.23–27,29,30
In conclusion, this trial shows that a 6-week prehabilitation programme before hip arthroscopy for femoroacetabular impingement syndrome is feasible and safe, with high adherence. The prehabilitation group showed small numerically favourable effects at early follow-up, but these effects did not survive Bonferroni correction for the primary outcome and were well below published thresholds for minimal clinically important difference. By 24 weeks the primary outcome difference was small, with a confidence interval that included zero. Future multicentre studies with longer follow-up and validated patient-reported outcome measures for the femoroacetabular impingement population can clarify whether early improvements translate into clinically important longer-term benefits.
Six weeks of supervised prehabilitation before hip arthroscopy for femoroacetabular impingement syndrome accelerated early functional recovery, with numerically higher Harris Hip Score at 4 and 12 weeks but no statistically significant advantage by 24 weeks. Between-group differences in patient-reported outcomes were below published thresholds for clinically important change, and the Harris Hip Score used as the primary outcome has not been validated specifically for the femoroacetabular impingement syndrome population. Prehabilitation produced consistent small gains in pain, maximal hip strength, range of motion, dynamic balance and mental health across follow-up, without increasing adverse events. Prehabilitation should be positioned as a safe approach to accelerate early recovery rather than a strategy to improve 6-month hip function.Clinical message
Supplemental Material
sj-docx-1-cre-10.1177_02692155261450149 - Supplemental material for Prehabilitation before hip arthroscopy for femoroacetabular impingement syndrome: A randomised controlled trial
Supplemental material, sj-docx-1-cre-10.1177_02692155261450149 for Prehabilitation before hip arthroscopy for femoroacetabular impingement syndrome: A randomised controlled trial by Min Li, Chenyi Jiang, Ruixin Wang, Lihua Huang, Yanhong Ma, Yun Shen, Jimin Yin and Shengdi Lu in Clinical Rehabilitation
Footnotes
Ethical consideration
The study received ethical approval from the Ethics Committee of Shanghai Sixth People's Hospital (IRB approval no.: 2024-KY-217(K)). Other participating institutions and hospitals acknowledged the IRB approval.
Consent for publication
Patient consent for publication was not required for this study (no identifiable patient information is presented).
Patient and public involvement
Patients or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Author contributions
Min Li and Shengdi Lu: Conceptualisation.
Yun Shen and Shengdi Lu: Methodology.
Chenyi Jiang and Ruixin Wang: Data curation.
Yun Shen and Jimin Yin: Formal analysis.
Min Li, Chenyi Jiang, Yanhong Ma and Lihua Huang: Investigation.
Jimin Yin and Shengdi Lu: Writing – review & editing.
All authors: Writing – original draft preparation.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Trial registration
The study protocol was preregistered in the Chinese Clinical Trial Registry (registration number ChiCTR2500113298).
Data availability statement
De-identified participant data that underlie the results reported in this article are available from the corresponding author upon reasonable request. No public data repository was used as no explicit data sharing plan was specified.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.