
Abstract
Objective
Altered motor excitability is a proposed mechanism of musculoskeletal shoulder pain. This scoping review aims to summarise studies examining motor excitability in individuals with painful musculoskeletal shoulder conditions, identify research gaps, and suggest clinical and research insights from these studies.
Data Sources
PubMed, EMBASE, CINAHL
Review methods
Databases were searched for studies from January 2004 to April 2026. Studies were included if they assessed motor excitability in participants with painful musculoskeletal shoulder conditions or healthy participants with experimentally induced shoulder pain.
Results
A total of 19 studies were included. Shoulder pain condition, target muscle selection, participant positioning, and measures of motor excitability varied between studies. Moreover, 11 of 16 studies comparing shoulder motor excitability in those with clinical or experimental shoulder pain to controls reported decreases in motor excitability in those with shoulder pain. Two of three studies reporting intervention effects describe increased excitability following interventions in at least one measure.
Conclusion
Shoulder motor excitability appears decreased in those with clinical shoulder pain. Mixed effects of experimental shoulder pain models on motor excitability suggest that more work clarifying the effect of pain on motor excitability changes is warranted. Preliminary studies report increased excitability following interventions, yet the clinical significance of these improvements is unclear. In order to minimise nervous system maladaptations in those with shoulder pain, clinicians may emphasise pain management and consider interventions that enhance motor excitability of the shoulder musculature. Because of heterogeneity in methodology and experimental pain models, further exploration of motor excitability as a mechanism and treatment target in musculoskeletal shoulder pain appears warranted.
Introduction
Musculoskeletal shoulder pain is prevalent and represents a large focus in rehabilitation practice and research.1,2 Shoulder muscle weakness, altered muscle activation, and altered pain processing are thought to contribute to musculoskeletal shoulder pain conditions,3–15 and previous work has started to explore neurophysiological mechanisms underlying these alterations.13–19
Motor excitability is gaining attention as a potential mechanism contributing to both muscle weakness and altered motor activation, and refers to the excitability of the neural structures involved in motor activation. Motor excitability is measured using either transcranial magnetic stimulation to measure corticospinal excitability,9,20 or using Hoffman reflexes to measure alpha motor neuron excitability.20–23 A schematic of transcranial magnetic stimulation and Hoffman reflexes is illustrated in
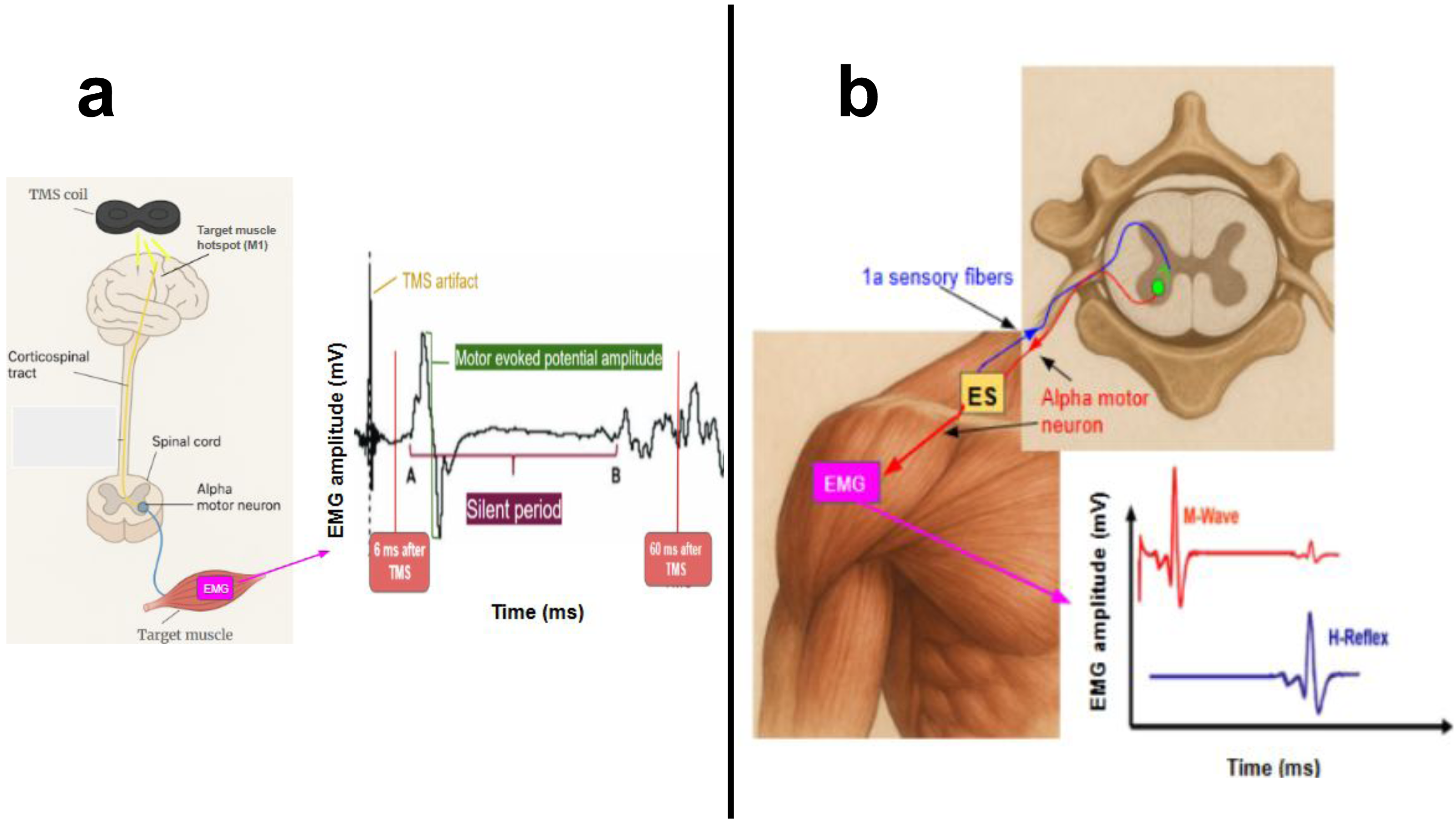
Motor excitability may influence the motor alterations seen in those with clinical shoulder pain.24–26 Furthermore, measures of motor excitability overcome significant limitations of electromyographic measurements because they are taken during rest or light muscle activation and therefore do not require maximal contraction during assessment, which can be altered in the presence of pain. Furthermore, the measures are thought to reflect excitability of neural pathways which may generalise across all tasks, whereas electromyographic activity reflects muscle activation during specific tasks, and likely varies between tasks.
While motor excitability is known to influence motor performance, emerging evidence suggests that motor excitability may also be related to the neurophysiological processing of pain, with preliminary evidence from studies examining repetitive motor cortex stimulation, which have shown improved pain and quality of life in individuals with fibromyalgia following stimulation.27–30
Since motor excitability of the shoulder muscle is a factor thought to underlie altered shoulder muscle performance and potentially pain processing, it may be an important factor to consider to prevent the development or progression of shoulder pain. A framework describing motor excitability as a potential mechanism of shoulder pain and progression is presented in
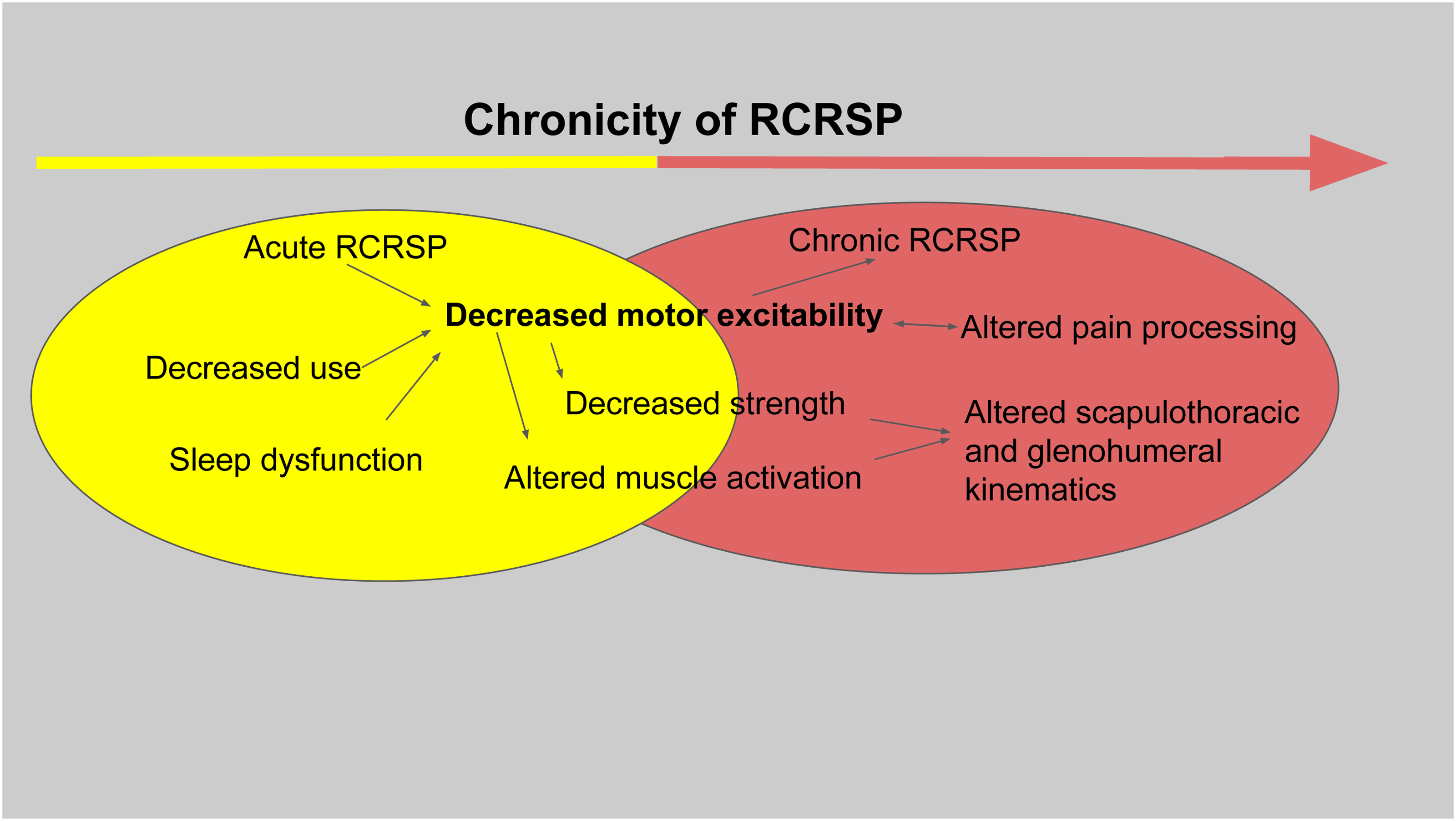
Framework describing decreased motor excitability as a mechanism of shoulder pain and progression.
The primary aim of this scoping review is to summarise work that has examined motor excitability in individuals with painful musculoskeletal shoulder conditions to answer three questions: First, is motor excitability of shoulder musculature altered in those with clinical shoulder conditions compared to controls? Second, does experimental shoulder pain result in altered motor excitability of local shoulder musculature? Third, what effects of interventions on shoulder muscle motor excitability have been observed?
Methods
Cochrane Database Systematic Reviews and the Joanna Briggs Institute database were searched to confirm that there were not any reviews in progress or to be published that would be redundant in scope. After confirmation, the databases PubMed, EMBASE, and CINAHL were searched for relevant studies from 1 January 2004 to 30th April 2026. Full descriptions of database search queries are located in Supplementary file 1.
During database searches, titles and abstracts of studies were screened, and initial eligibility was determined. Initial eligibility was determined for studies by the primary author if upon abstract screening they included participants with painful musculoskeletal shoulder conditions (rotator cuff tendinopathy, adhesive capsulitis, total shoulder arthroplasty, reverse total shoulder arthroplasty, Bankart repair, superior labrum anterior–posterior repair, glenohumeral osteoarthritis, glenohumeral instability, acromioclavicular joint osteoarthritis) or healthy participants with experimentally induced shoulder pain and examined either the effect of painful musculoskeletal shoulder conditions or experimental pain on motor excitability measured using corticospinal excitability or Hoffman reflex. In addition, studies were included if they examined the effect of intervention on motor excitability in participants with musculoskeletal shoulder conditions. Studies involving participants with nonmusculoskeletal shoulder pain (poststroke shoulder pain, for example) were excluded. Following initial screening, duplicate studies were removed, and the primary author then read full-text articles of potentially eligible studies to determine eligibility for final inclusion. References of included studies were then screened for the presence of additional relevant studies. Variables that were extracted if present in each study included participant demographic information, the shoulder condition of participants, methods for obtaining measurements of motor excitability, and details of the interventions used and effects of interventions on motor excitability. Independent data extraction was completed using standardised, preorganised digital templates by two assessors who subsequently remediated any disagreements until consensus was achieved. Supplementary file 2 includes a blank template of the data extraction spreadsheet used during data extraction. Once consensus was achieved for all disagreements, data were transcribed by the primary author into a final tabulated form. During this data synthesis process, studies were grouped by the aims that they addressed. Specifically, studies were organised into three groups, with the first group consisting of studies comparing motor excitability in those with clinical shoulder pain to controls, the second group consisting of studies comparing motor excitability in participants before and during experimental pain, and the third group consisting of studies reporting intervention effects on motor excitability in those with clinical shoulder pain.
Results
The search yielded 1558 references, which were screened and resulted in 21 unique full-text articles assessed. 19 studies were ultimately included following full-text screening.24–26,31–46
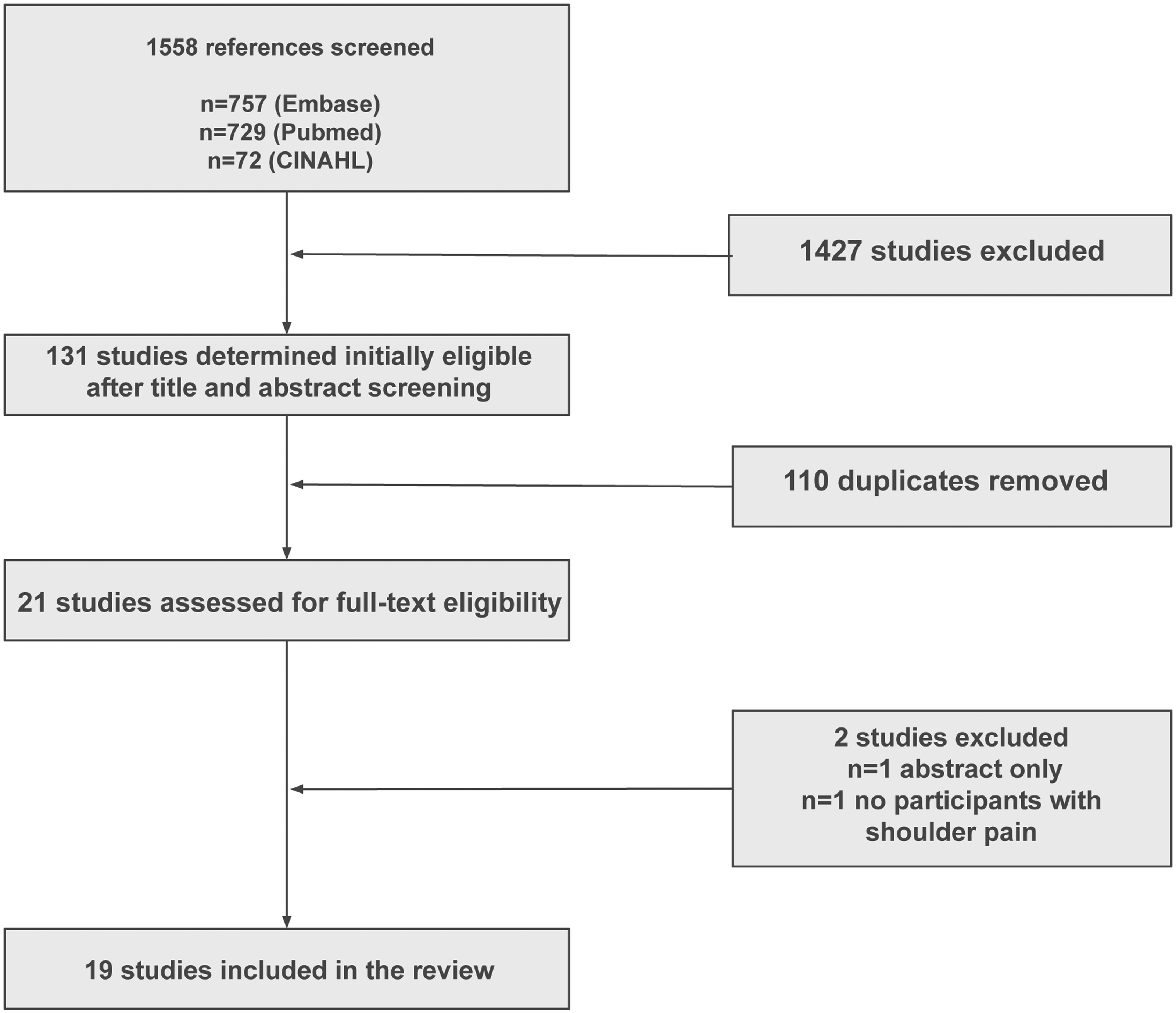
PRISMA flowchart.
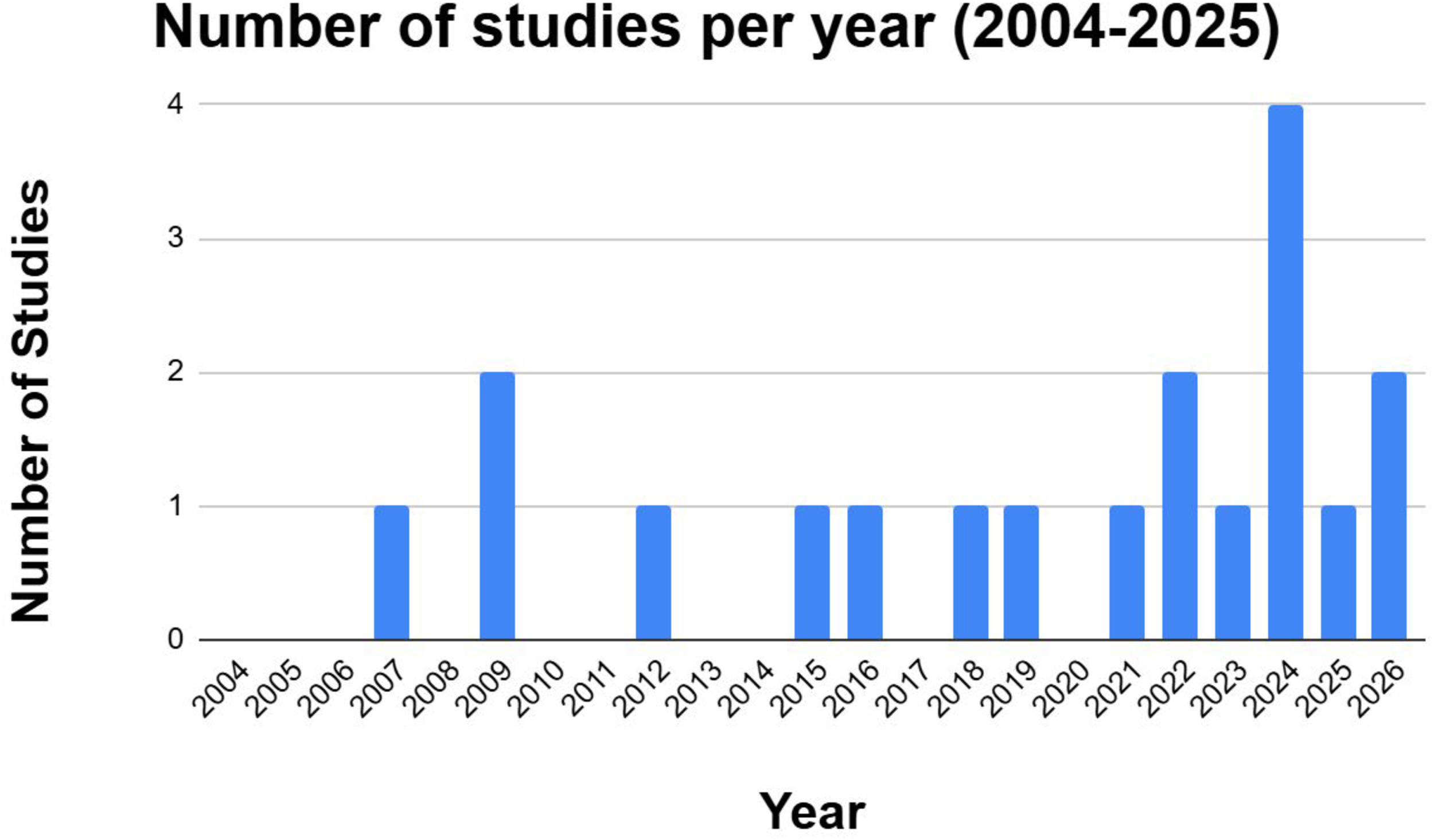
Publication timeline of included studies.
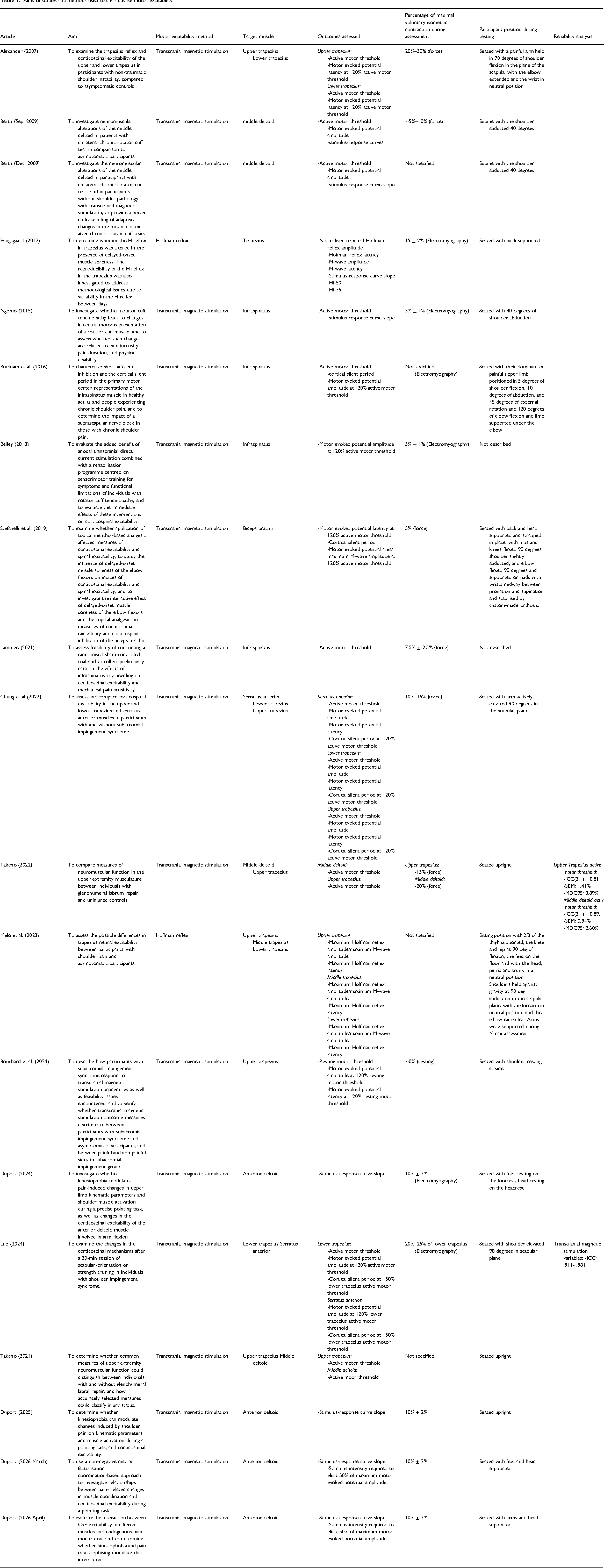
Aims of studies and methods used to characterise motor excitability.
Comparisons of shoulder muscle motor excitability between participants with clinical shoulder pain and controls.
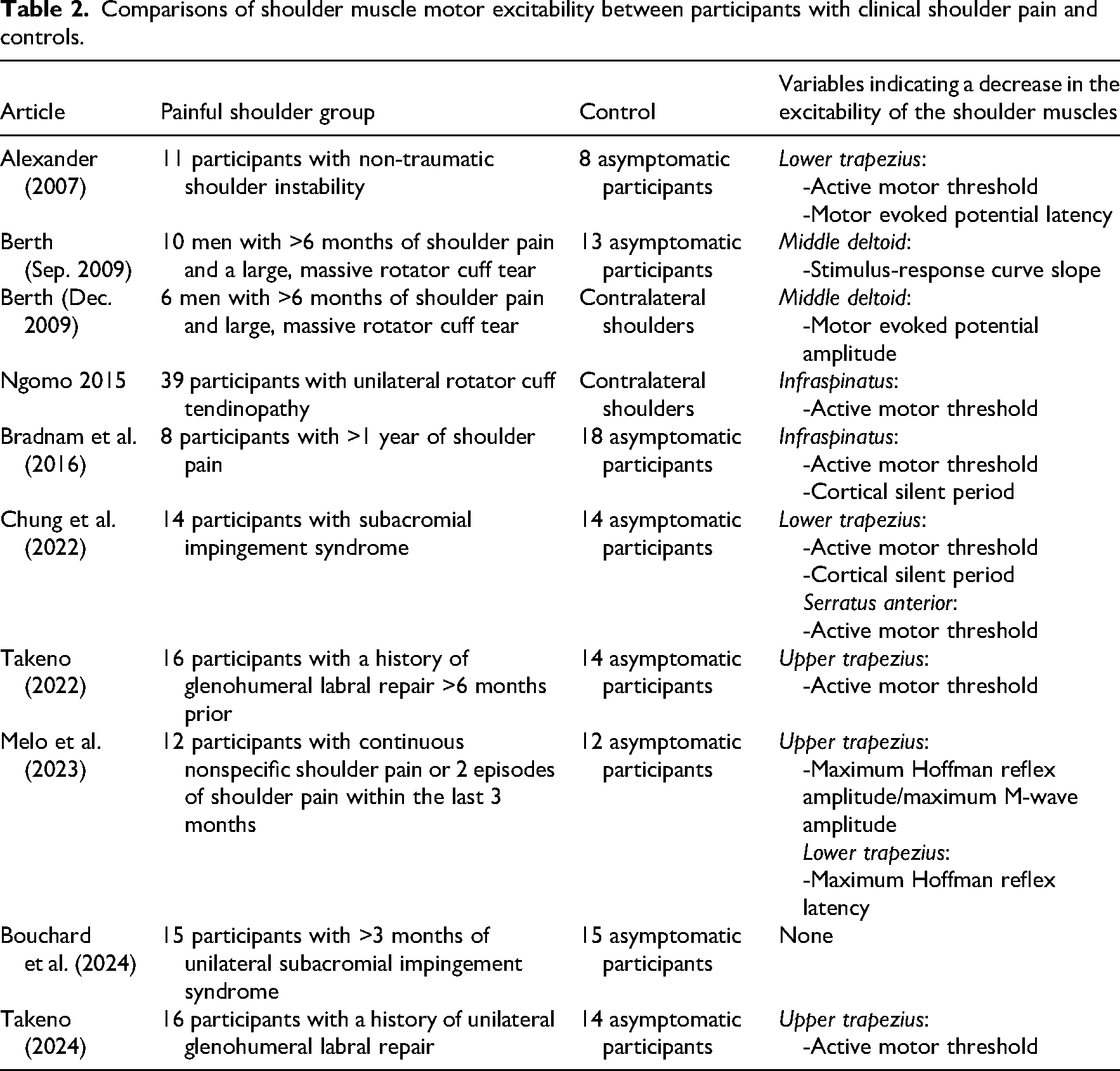
Table 3 summarises the included studies which compare participants before and after experimental shoulder pain is induced. Participants with experimental shoulder pain induced by a topical irritant were assessed in four studies,37,44–46 and participants with experimental pain induced by delayed onset muscle soreness were included in two studies.39,41 In both studies using delayed-onset muscle soreness as an experimental pain model, decreases in motor excitability in at least one measure of motor excitability were observed.39,41 In three of four studies using topical irritant (1% topical capsaicin cream) as the experimental pain model, no alterations in motor excitability were observed for any measure of motor excitability37,44–45 with one study reporting conflicting evidence with one variable indicating a decrease in motor excitability. 46
Comparisons of motor excitability in participants before and after experimentally induced shoulder pain.
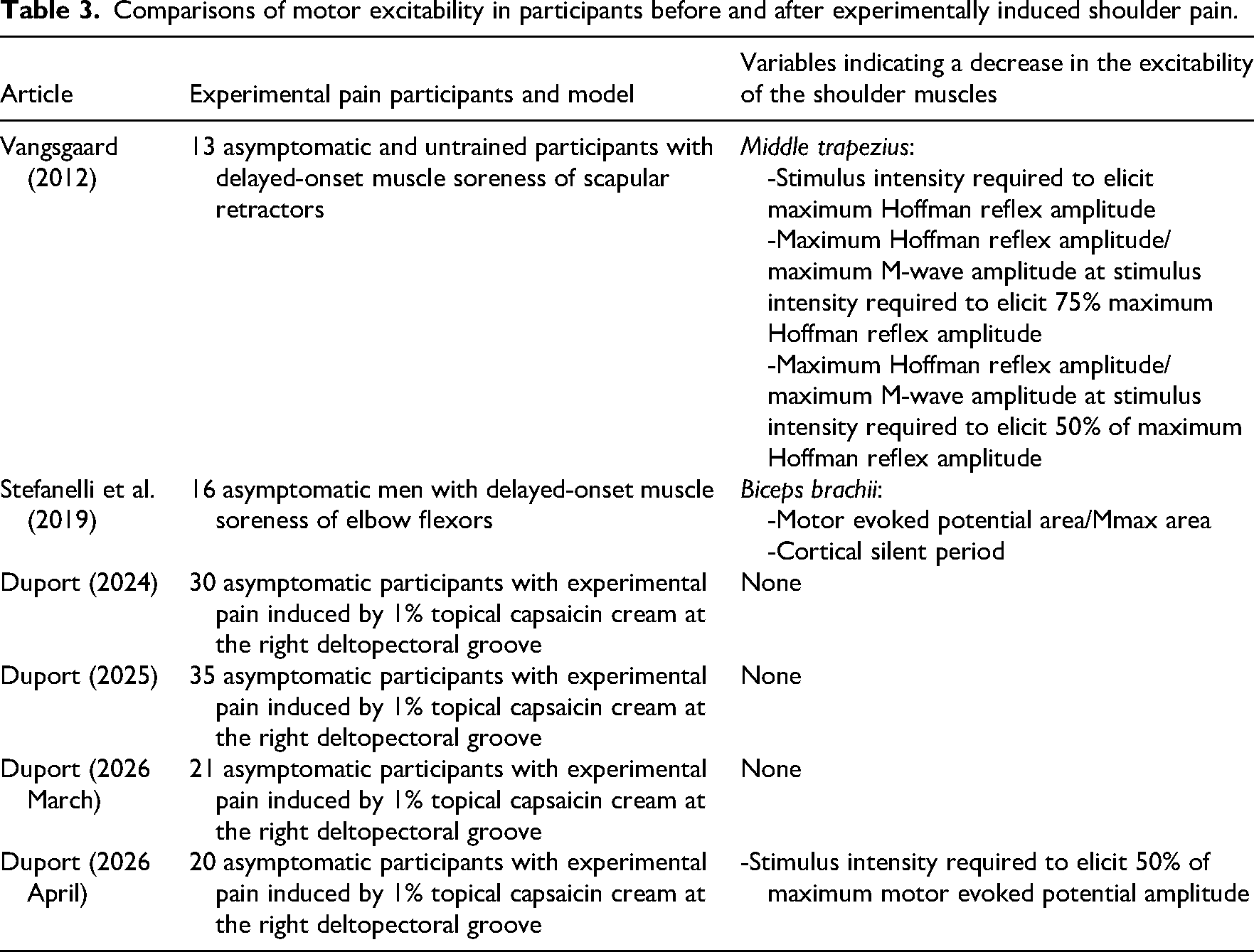
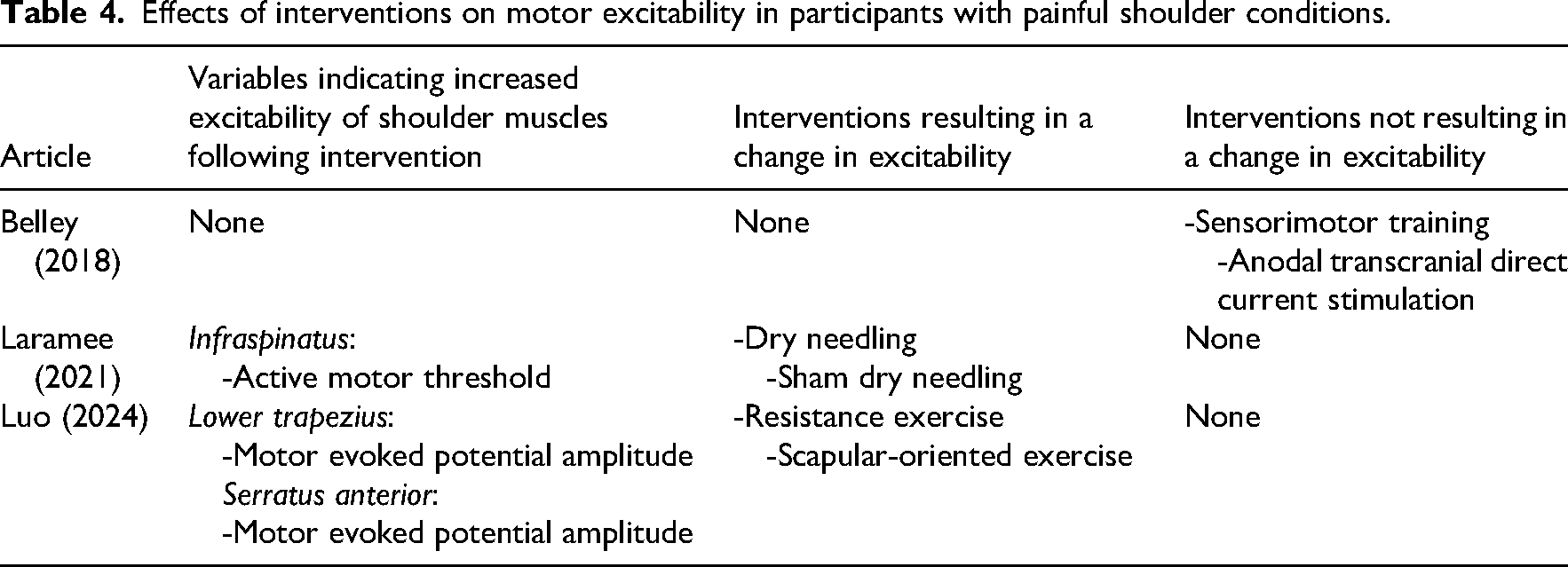
Table 4 summarises the included studies which examine intervention effects on shoulder muscle motor excitability. Among the three studies examining intervention effects on motor excitability, increased excitability was observed in two studies in at least one measure of motor excitability.31,32,42 Increases in motor excitability were observed following dry needling, sham dry needling, and resistance-based exercise with and without feedback.
Effects of interventions on motor excitability in participants with painful shoulder conditions.
Discussion
This review has identified preliminary research exploring altered motor excitability as a mechanism and treatment target in musculoskeletal shoulder conditions. Frequently, decreases in motor excitability were observed in the studies that compared participants with clinical shoulder conditions to controls. Furthermore, decreased motor excitability was observed in three of six studies examining participants with experimental shoulder pain. These findings collectively suggest that shoulder pain may directly contribute to decreased motor excitability observed in those with clinical shoulder pain. However, the pain models in these studies used topical irritants and delayed-onset muscle soreness as experimental pain models, which may not accurately model pain experienced during many shoulder conditions.47,48 Furthermore, discordant effects that are observed between each of these models suggest that enhanced pain models that more accurately model pain experienced during clinical shoulder conditions may provide clarification. If pain directly contributes to decreased motor excitability, then adequate and early pain management may be necessary during rehabilitation of those with clinical shoulder conditions so as to minimise maladaptive decreases in motor excitability. While the acute effect of shoulder pain on motor excitability remains contentious, the acute effect of pain may not completely explain motor excitability changes in those with chronic shoulder pain. Other secondary factors apart from pain, such as decreased use 49 or sleep dysfunction 50 may also be relevant factors contributing to observed decreases in motor excitability in those with chronic clinical shoulder pain. Preliminary studies exploring the effects of exercise and non-exercise interventions on motor excitability suggest that motor excitability is increased following resistance exercise and both dry needling and sham dry needling.31,32 These early findings are consistent with previous studies examining the effects of resistance exercise on motor excitability in other body regions.44,51 Resistance exercise has shown clinical effectiveness in the management of shoulder pain and is recommended for clinical management, 52 and this review highlights one potential mechanism of effect of resistance exercise. Of note, the effect of resistance exercise on motor excitability of shoulder musculature appears mixed, as one study examining the effect of multimodal intervention, including resistance exercise, did not observe altered motor excitability following intervention. 42 These mixed results suggest that the effect of resistance exercise on motor excitability may depend on exercise parameters, which may be clarified with future research. In one study, 31 dry needling and sham dry needling resulted in increased shoulder muscle motor excitability and provided evidence that interventions that provide somatosensory input may play a role in modulating motor excitability in those with chronic shoulder pain. The clinical relevance of these neurophysiological changes following such interventions should be examined, particularly when combined with exercise-based interventions.
One limitation of this scoping review is that no quantitative analysis is provided. Heterogeneity among the included studies limits the feasibility of quantitative analyses and is evident in participant demographics, shoulder pain conditions, and methods used to characterise motor excitability. Future work appears necessary to standardise methods of both transcranial magnetic stimulation and Hoffman reflex assessment when measuring motor excitability in individuals with shoulder pain. Considering the relatively small sample sizes across the included studies, which ranged from 6 to 41 participants, more homogeneous work examining these neurophysiological measures in individuals with shoulder pain would permit pooled analyses, which would enhance the validity of conclusions derived from such work. In addition, only two of the included studies in this review reported on the reliability of the obtained measures.32,40 Given that there is otherwise limited evidence for high reliability of transcranial magnetic stimulation measurements of many shoulder muscles, 53 and that these measurements may be operator dependent, the degree of measurement error relative to the distinct effects of pain or interventions which were reported in the included studies remains unclear. Reliability analyses should be included in future work that uses these measurements. In summary, this review highlights growing acknowledgement of motor excitability as a potential mechanism and treatment target in musculoskeletal shoulder pain, but future work appears necessary to clarify factors influencing motor excitability as well as determine whether targeting of motor excitability leads to clinically significant improvement in individuals with musculoskeletal shoulder disorders.
Clinical messages
Shoulder motor excitability appears decreased in the presence of clinical musculoskeletal shoulder pain.
Experimental pain models suggest pain may contribute to decreased shoulder muscle motor excitability, but further research is warranted.
In order to minimise nervous system maladaptations in those with shoulder pain, clinicians may emphasise pain management and the use of interventions that enhance motor excitability of the shoulder musculature.
Preliminary studies report increases in excitability following interventions, yet the clinical significance of these improvements should be clarified.
Supplemental Material
sj-docx-2-cre-10.1177_02692155261458737 - Supplemental material for Motor excitability in painful musculoskeletal shoulder conditions: A scoping review
Supplemental material, sj-docx-2-cre-10.1177_02692155261458737 for Motor excitability in painful musculoskeletal shoulder conditions: A scoping review by Jeffrey S Paskewitz, Daniel W Safford, Kshamata M Shah and Philip W McClure in Clinical Rehabilitation
Supplemental Material
sj-pdf-3-cre-10.1177_02692155261458737 - Supplemental material for Motor excitability in painful musculoskeletal shoulder conditions: A scoping review
Supplemental material, sj-pdf-3-cre-10.1177_02692155261458737 for Motor excitability in painful musculoskeletal shoulder conditions: A scoping review by Jeffrey S Paskewitz, Daniel W Safford, Kshamata M Shah and Philip W McClure in Clinical Rehabilitation
Footnotes
Ethical considerations
No IRB approval was required to conduct this scoping review.
Consent to participate
Not applicable
Consent for publications
Not applicable
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data from this review are available in supplementary materials.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.