
Abstract
Objective
To explore the barriers and facilitators to leisure-time physical activity among community-dwelling adults with spinal cord injury in China, using the Capability, Opportunity, Motivation-Behaviour model as a theoretical framework.
Design
A qualitative study employing semi-structured interviews.
Setting
Two rehabilitation centres in Guangzhou, China.
Participants
Twenty community-dwelling adults with spinal cord injury, purposively sampled for diversity in gender, age, injury level and severity.
Results
The analysis identified multifaceted factors across the Capability, Opportunity and Motivation-Behaviour domains. Within the Capability domain, barriers included limited physical function and a pessimistic mindset, whereas facilitators encompassed strong psychological resilience, high self-efficacy and positive beliefs in rehabilitation. Opportunity was constrained by limited social resources, inadequate rehabilitation facilities and financial constraints, but was enhanced by diverse social support. Within the Motivation domain, engagement in leisure-time physical activity was hindered by low self-discipline, fear of physical activity and motivational conflict, while motivation was strengthened by reflection on the benefits of physical activity, a desire for social reintegration and return to work.
Conclusions
Promoting leisure-time physical activity among this population requires a theory-informed, multi-level intervention strategy. Interventions should simultaneously strengthen individual capability, expand opportunity and foster motivation. Crucially, such interventions must be contextually adapted to address China-specific socioeconomic constraints and cultural norms.
Introduction
Spinal cord injury is a severe, life-altering condition associated with profound impairments in physical function, mental health and quality of life.1–3 For individuals living in the community, insufficient physical activity further increases the risk of debilitating secondary complications. 4 Leisure-time physical activity represents a vital health behaviour that can mitigate these risks, conferring substantial benefits for physical capacity, psychological well-being and social integration.5–9
Despite these well-documented benefits, engagement in leisure-time physical activity among individuals with spinal cord injury worldwide remains critically low.10,11 This issue is particularly pronounced in China, where community-dwelling individuals with spinal cord injury face substantial challenges to participation. 12 Although previous studies have identified a range of influencing factors – including physical impairments, 13 environmental barriers 12 and social support, 14 as well as facilitators such as positive attitudes 15 and strong social networks14,16 – the existing literature is limited in three key respects: a paucity of theory-guided investigations 13 ; an over-reliance on quantitative approaches that inadequately capture lived experiences17,18; and a predominant focus on Western contexts, which restricts applicability to the Chinese setting.10,13 Collectively, these gaps underscore the need for a theoretically grounded qualitative study situated within China's socio-cultural context.
To address these gaps, the present study adopts the Capability, Opportunity, Motivation-Behaviour model, a comprehensive framework for understanding behaviour change. 19 This model, which has been widely applied in chronic disease management 19 and health promotion, 20 is particularly well suited to elucidating the complex determinants of leisure-time physical activity. Guided by this framework, the study systematically examines the barriers and facilitators influencing leisure-time physical activity among community-dwelling individuals with spinal cord injury in China. The findings aim to generate actionable, theory-informed insights to guide the development of targeted interventions. 21
Methods
The study was approved by the Nursing Ethics Committee of Sun Yat-sen University (Approval Number: L2022SYSU-HL-071). All participants voluntarily agreed to participate and provided written informed consent prior to data collection. This qualitative study was reported in accordance with the Consolidated Criteria for Reporting Qualitative Research, 22 which guided the reporting of the study design, participant recruitment, data collection, data analysis, and presentation of findings.
Participants
A purposive sampling method was employed, based on the principle of maximum variation sampling, selecting community-dwelling individuals with spinal cord injury with variations in gender, age, level of injury and injury severity. Semi-structured interviews were conducted with individuals with spinal cord injury who had undergone rehabilitation at two rehabilitation centres in Guangzhou, Guangdong Province, from September to December 2023. Inclusion criteria were: (1) diagnosis of spinal cord injury confirmed by spinal computed tomography or magnetic resonance imaging, assessed according to the International Standards for Neurological Classification of Spinal Cord Injury revised by the American Spinal Injury Association, 23 and confirmed by physicians; (2) age ≥18 years; (3) completion of acute treatment and residence at home for at least 2 months after discharge 24 ; and (4) clear consciousness and ability to communicate verbally. Exclusion criteria were: (1) congenital or hereditary spinal cord injury; and (2) severe conditions with unstable vital signs.
The target sample size was prospectively set at 15–25 participants, which is consistent with recommendations for qualitative research on data saturation.25,26 A data saturation principle was adopted: recruitment was planned to continue until no new codes or themes emerged from three consecutive interviews. Recruitment ceased when this criterion was met, and pseudonyms (P1–P20) were used to protect participant confidentiality.
Development of interview guide
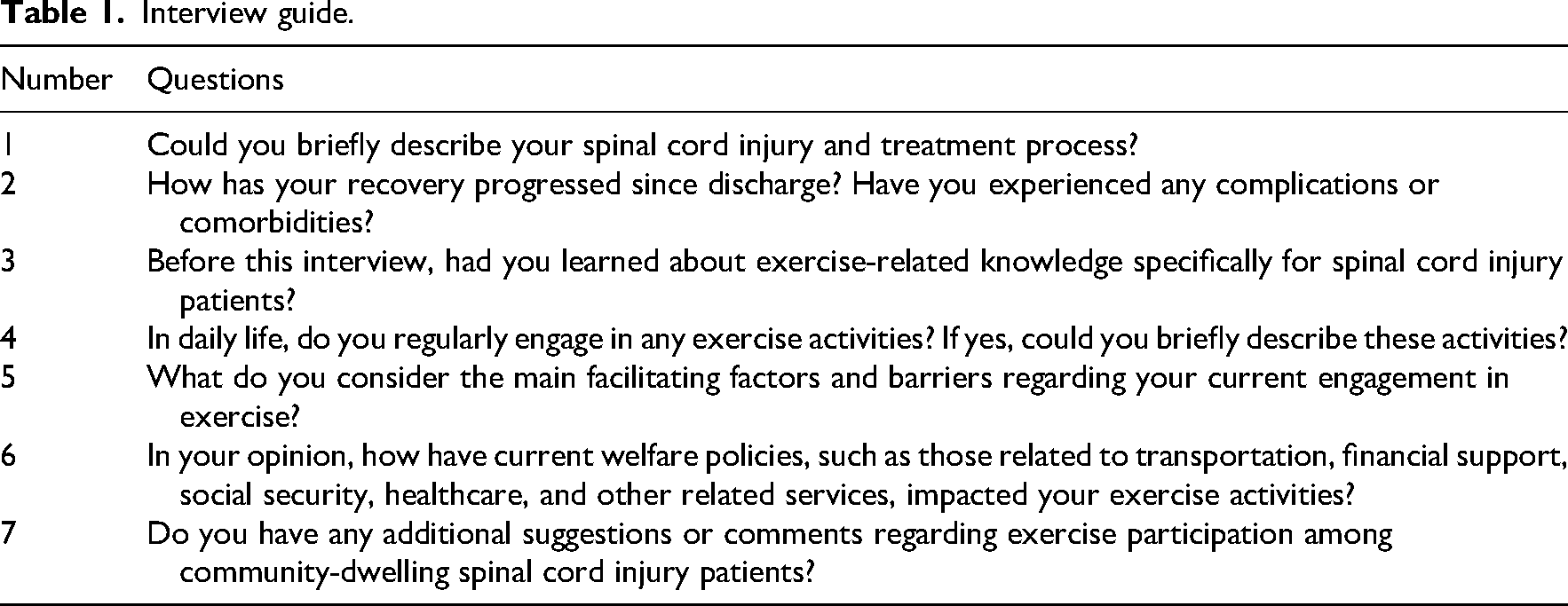
Based on a literature review, this study developed an interview guide focusing on community-dwelling individuals with spinal cord injury perceptions, engagement and influencing factors regarding participation in leisure-time physical activity. Subsequently, five nursing experts with clinical expertise in spinal cord injury – including faculty from nursing colleges holding titles of associate professor or higher and head nurses from comprehensive tertiary hospitals and rehabilitation hospitals – were invited to evaluate the interview guide and provide feedback. The researchers adopted the following recommendations: given the limited familiarity and general misunderstanding of the term ‘leisure-time physical activity’ among the general public in China, the term was replaced with ‘exercise’ throughout the interview guide to facilitate understanding and smooth communication during interviews. The final version of the interview guide is presented in Table 1.
Interview guide.
Data collection and quality control
Data were collected through semi-structured face-to-face interviews conducted by a master's-level nursing student who had received systematic training and acquired qualitative interviewing skills. After obtaining approval from the School of Nursing at Sun Yat-sen University and the nursing departments of two rehabilitation centres, the interviewer briefed the head nurses on the research purpose, gaining their consent and access to patient medical records. Community-dwelling individuals with spinal cord injury were purposively selected from rehabilitation centres based on gender, age, injury level and severity of injury. Appropriate times were identified to contact participants through outpatient visits, inpatient units or via WeChat, clearly explaining the research objectives and obtaining informed consent. Individual interviews were conducted either face-to-face or online via audio calls.
Interviews were carried out in quiet settings to minimize environmental interference. Each interview lasted at least 20 min but did not exceed 60 min and was audio-recorded. Throughout the interview, the interviewer maintained a neutral stance, adjusting the sequence of interview questions according to the situation, offering appropriate encouragement, and engaging in follow-up questions or responses as necessary. After each interview, recordings were promptly transcribed into text, and follow-up interviews were conducted with participants if additional clarification was needed.
Data analysis
The audio recordings from the interviews were transcribed verbatim and imported into NVivo 15 for analysis. To ensure participants’ confidentiality, transcripts were anonymized by removing names and assigning numerical identifiers. An inductive thematic analysis approach (a bottom-up method in which themes were generated from the data rather than from pre-existing theory) was used, as it can help identify both manifest and latent aspects and form in-depth understandings of a phenomenon.27–29 We followed a six-step framework to draw the themes 27 : (1) Being fully familiar with the data: two researchers who were graduate nursing students with rich experience in qualitative research independently read and reread the transcripts and took notes for formulating latent codes using a semantic coding approach. (2) Creating initial codes: a list of codes was generated and modified during the open coding process to identify interesting and noteworthy features in the transcripts and label paragraphs that contained relevant information. (3) Searching for themes: various themes were formed by identifying consistent patterns among codes. (4) Reviewing themes: the two researchers jointly reviewed the themes they had extracted independently to reach a shared agreement by combining, splitting, creating or discarding themes. (5) Defining and naming themes: regular meetings with the full research team were held to iteratively refine and finalize thematic definitions and labels. (6) Writing the report: during the process, coding and theme generation were conducted in the local language and were only translated into English with semantic equivalence when writing the report. The researchers also wrote memos to record their thoughts and questions for discussion.
Rigor and trustworthiness
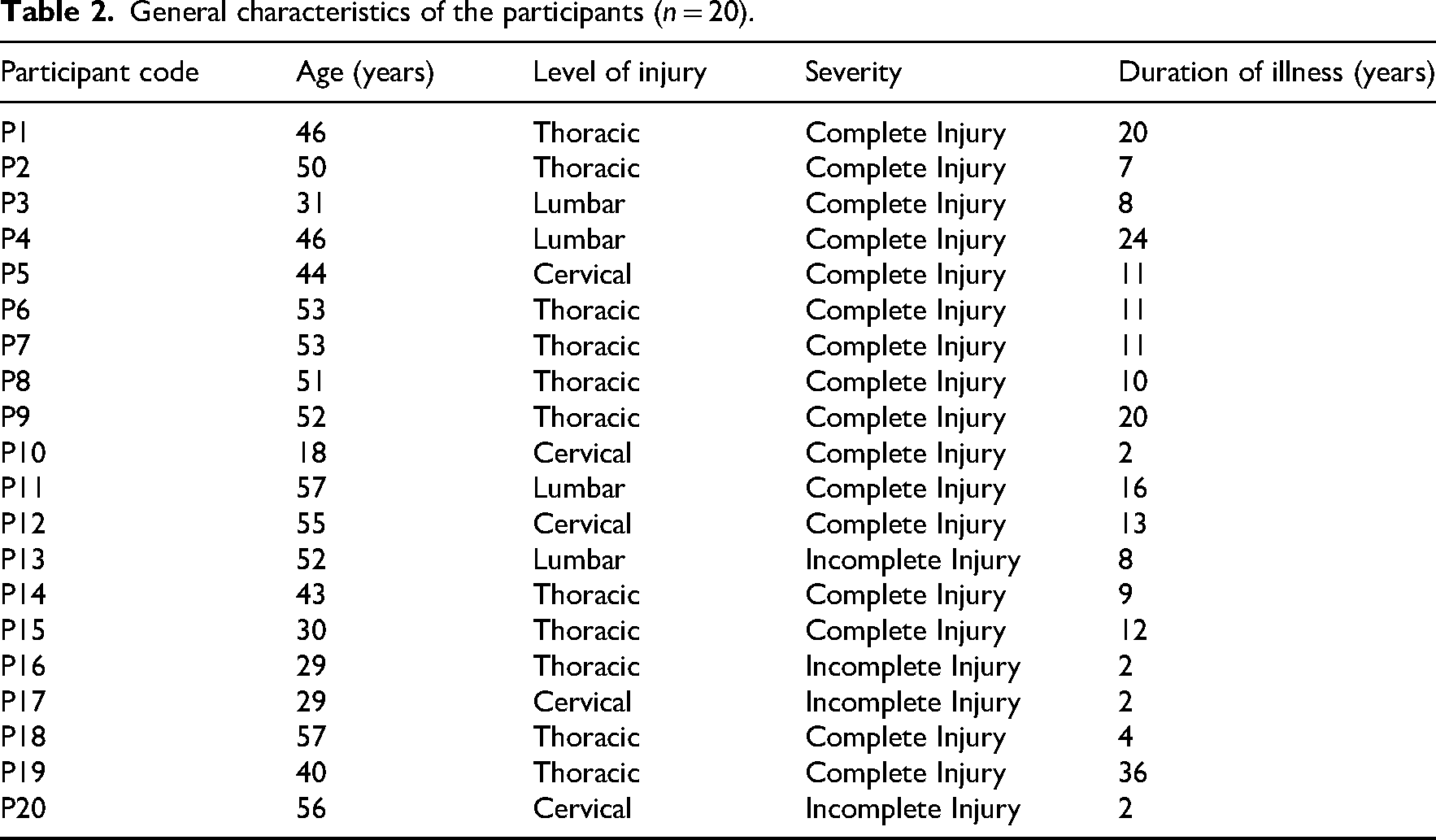
Several strategies were employed to ensure the rigor and trustworthiness of the findings, drawing on Lincoln and Guba's criteria for qualitative research. 30 Credibility was established through prolonged engagement with the topic, peer debriefing (regular meetings within the research team to discuss coding and interpretations), and member checking (summaries of key findings were shared with three participants, who confirmed that the findings resonated with their experiences). Dependability and confirmability were ensured by maintaining a clear audit trail, which included raw interview transcripts, analytical memos and records of all coding decisions. The research team engaged in reflexive discussions to acknowledge and mitigate potential biases, particularly the interviewer's background as a nursing student, which could influence participant responses. Transferability is supported by the detailed description of participant characteristics (Table 2), the study context (rehabilitation centres in Guangzhou, China), and the inclusion of rich, verbatim quotes in the results, allowing readers to assess the applicability of our findings to other settings.
General characteristics of the participants (n = 20).
Results
A total of 20 participants were recruited. Data saturation was achieved, as no new themes emerged from the final three interviews. The final sample comprised 20 participants, including 13 males and 7 females, aged 18–57 years. Regarding the injury level, 5 participants had cervical injuries, 11 had thoracic injuries, and 4 had lumbar injuries. In terms of injury severity, 16 participants had complete injuries, while 4 had incomplete injuries. Detailed general characteristics of participants are shown in Table 2.
Using inductive thematic analysis guided by the Capability, Opportunity, Motivation-Behaviour model, barriers and facilitators influencing leisure-time physical activity among community-dwelling individuals with spinal cord injury were categorized into three core domains: capability, opportunity and motivation. Within each domain, specific themes and corresponding subthemes were identified.
Domain 1: Capability
The ‘capability’ domain encompassed themes related to physical and psychological capacities influencing participation in leisure-time physical activity.
Theme 1: Physical capability
Barriers under this theme involved limited physical function, including reduced mobility, strength and endurance, which considerably hindered participants’ ability to regularly engage in leisure-time physical activity.
Theme 2: Psychological capability
Under this theme, barriers involved negative psychological states, particularly a pessimistic mindset characterized by decreased confidence, frustration with slow recovery progress and feelings of helplessness.
Conversely, facilitators of psychological capability included strong psychological resources, high self-efficacy and positive rehabilitation beliefs. These psychological resources enhanced individuals’ acceptance of and adaptation to their conditions, promoting continued engagement in physical activities.
Domain 2: Opportunity
The ‘opportunity’ domain captured physical and social opportunities affecting leisure-time physical activity participation.
Theme 1: Physical opportunity
Barriers included inadequate rehabilitation conditions, such as a lack of mobility aids, insufficient exercise facilities and venues and a lack of barrier-free infrastructure for individuals with disabilities. Financial constraints were also frequently reported as significant barriers restricting access to these essential exercise resources.
Theme 2: Social opportunity
Social opportunity barriers included insufficient societal resources, such as inadequate support from disability-related organizations and a general lack of societal assistance aimed at facilitating rehabilitation and social participation.
Conversely, facilitators within social opportunity predominantly included diverse social support networks provided by family, friends and community groups. Such social support offered crucial practical assistance, emotional encouragement and companionship, significantly facilitating regular engagement in leisure-time physical activity.
Domain 3: Motivation
The ‘motivation’ domain involved both automatic and reflective aspects influencing leisure-time physical activity adherence.
Theme 1: Automatic motivation
Barriers to automatic motivation included low self-discipline and fear of physical harm from exercise. Participants frequently described struggling to maintain regular exercise routines because they had difficulty forming consistent habits or experienced negative emotional responses associated with physical activity.
Facilitators included self-rehabilitation, self-care and self-esteem fulfilment. Participants highlighted that intrinsic needs for improving physical functioning, proactively managing their own health and achieving greater self-worth served as powerful automatic motivational drivers, significantly encouraging regular participation in leisure-time physical activity.
Theme 2: Reflective motivation
Barriers to reflective motivation included motivational conflicts. Participants reported difficulty balancing rehabilitation goals with other demands, which reduced their engagement in leisure-time physical activity.
Conversely, facilitators within reflective motivation included active reflection on the benefits of physical activity and clear aspirations for social reintegration and returning to work. These reflective considerations significantly reinforced their continued engagement in leisure-time physical activity.
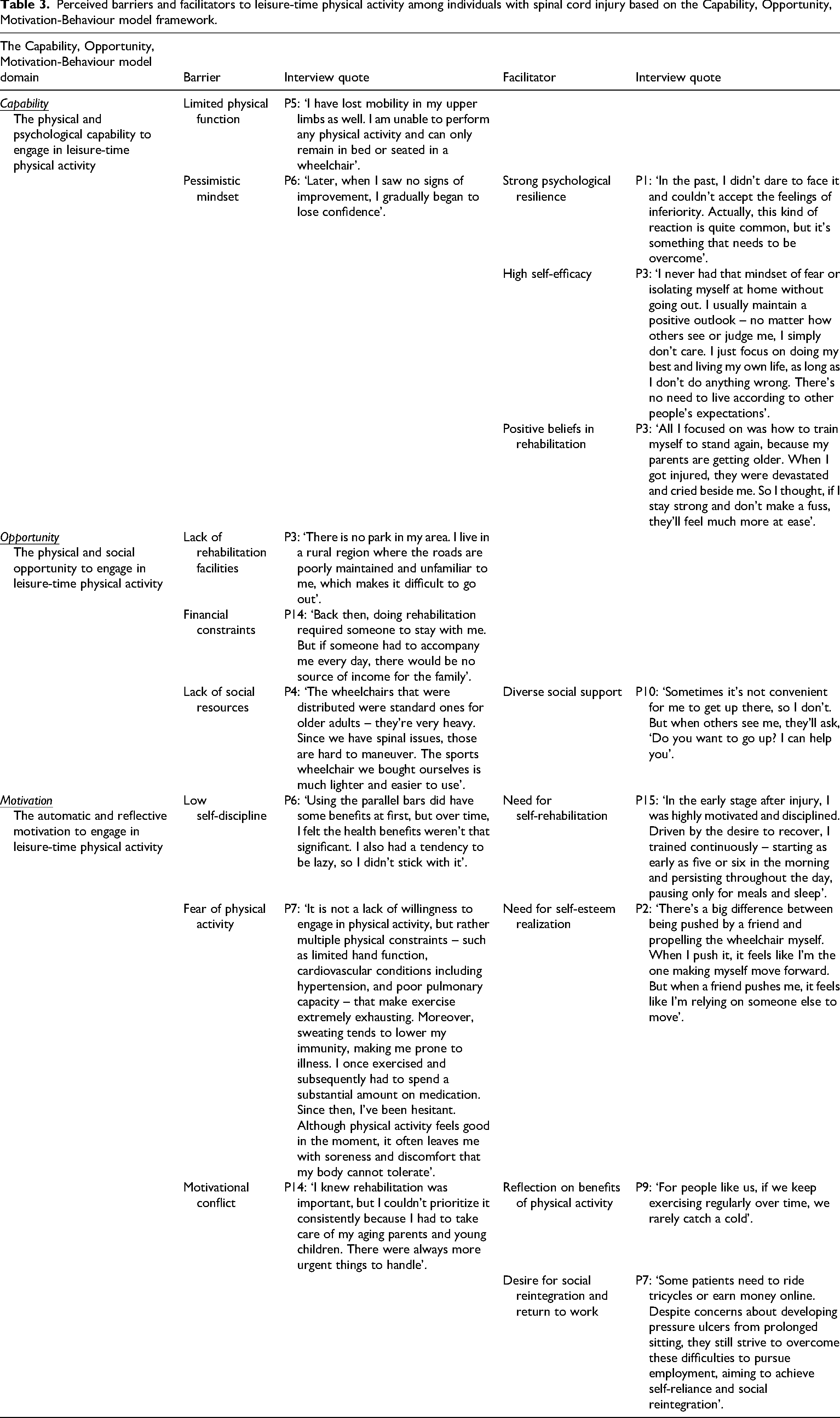
A visual representation of these themes is provided in Figure 1, and detailed descriptions of perceived barriers and facilitators are summarized in Table 3.
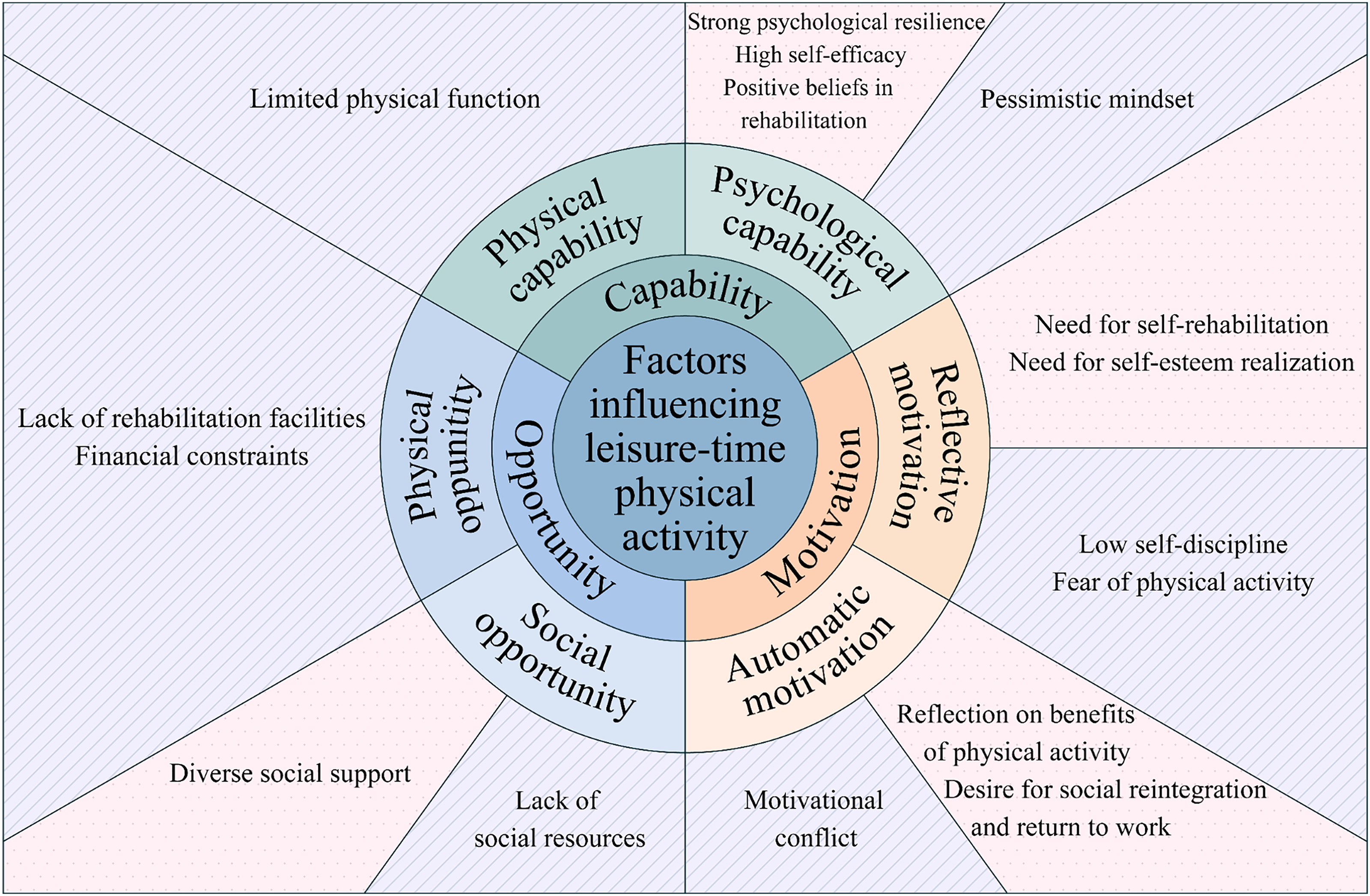
Factors influencing leisure-time physical activity in community-dwelling individuals with spinal cord injury.
Perceived barriers and facilitators to leisure-time physical activity among individuals with spinal cord injury based on the Capability, Opportunity, Motivation-Behaviour model framework.
Discussion
Grounded in the Capability, Opportunity, Motivation-Behaviour model, this study provides the first theory-driven, systematic exploration of the multifaceted barriers and facilitators influencing leisure-time physical activity among community-dwelling individuals with spinal cord injury in China.
In terms of Capability, our findings highlight both physical and psychological factors as critical components. Physical impairments, such as restricted mobility and loss of strength, and psychological barriers, such as diminished confidence and a pessimistic mindset, were predominant challenges to engaging in leisure-time physical activity. These results align with the ‘Capability’ component of the Capability, Opportunity, Motivation-Behaviour model, which encompasses both the physical and psychological capacity to perform a behavior. 19 They are also consistent with international studies identifying physical function and self-efficacy as key determinants of activity participation in spinal cord injury populations.31,32 Conversely, and crucially for intervention design, our study identified psychological resilience, high self-efficacy and positive rehabilitation beliefs as key facilitators within the capability domain. This reinforces the Capability, Opportunity, Motivation-Behaviour model's tenet that interventions must address both physical and psychological dimensions of capability to effectively promote behaviour change.10,19
The Opportunity domain revealed several contextual and structural factors that shape behaviour. In the Chinese context, major barriers included a lack of rehabilitation facilities, financial constraints and insufficient social support. These findings resonate strongly with the ‘Opportunity’ construct, which includes the physical and social environment that either enables or hinders behaviour. They align with prior research on environmental barriers in low- and middle-income settings13,33 and contrast with barriers more frequently reported in high-income countries, where the challenges often involve a lack of specialized programs rather than basic accessibility. 34 Importantly, robust social support from family and community emerged as a powerful facilitator within the social opportunity component. This finding reinforces existing evidence on the vital role of social networks in enabling health behaviors7,16 and suggests that, in the Chinese context, strong social ties can partially promote physical activity and other health-related behaviours.
The Motivation domain was characterized by a dynamic tension between internal drivers and external conflicts, reflecting the Capability, Opportunity, Motivation-Behaviour distinction between reflective and automatic motivational processes. 19 Reflective motivation was constrained by low self-discipline and fear of exercise-induced harm, yet strongly driven by deep-seated needs for self-rehabilitation and esteem fulfilment. Automatic motivation was frequently undermined by competing familial obligations – a culturally salient barrier in China, as supported by studies on caregiving dynamics 35 – but was sustained by aspirations for social reintegration and return to work. This nuanced view underscores that motivational interventions for this population must simultaneously address personal goals (both reflective and automatic) and navigate contextual demands that create motivational conflicts.19,21
Beyond mapping factors onto the Capability, Opportunity, Motivation–Behaviour model, our study identifies three context-specific insights that have direct implications for practice among individuals with spinal cord injury in China: pronounced economic strain, limited availability of rehabilitation resources, and culturally embedded caregiving obligations that generate distinct motivational conflicts. These findings highlight that effective, theory-informed interventions must be adapted to localized socio-economic and cultural realities. For example, economic barriers warrant targeted financial support mechanisms, such as subsidies for assistive equipment, while environmental deficits necessitate community-level improvements in accessibility. In addition, family-centred support programmes may help alleviate motivational conflicts related to caregiving responsibilities. 35
Guided by this Capability, Opportunity, Motivation–Behaviour analysis, we propose a multi-level intervention strategy. To enhance capability, tailored rehabilitation guidance combined with structured psychological support, including cognitive-behavioural approaches designed to enhance self-efficacy, is essential. To expand opportunity, policy advocacy for inclusive community design and sustainable financial assistance is critical. To strengthen motivation, interventions should explicitly link leisure-time physical activity to meaningful life goals, such as vocational reintegration or social participation. This integrated, theory-driven approach is consistent with the Behaviour Change Wheel methodology, which advocates designing interventions based on a thorough behavioural analysis informed by models like Capability, Opportunity, Motivation-Behaviour. 19
This study has several limitations. The regional focus on Guangdong Province may not fully capture the experiences of individuals in other parts of China, particularly in under-resourced rural areas. Furthermore, individuals not engaged with rehabilitation services were not included, potentially omitting those facing the greatest barriers. Future research should employ multi-regional sampling and incorporate policymaker perspectives to deepen the understanding of systemic constraints.
In conclusion, improving leisure-time physical activity participation among individuals with spinal cord injury requires coordinated strategies that strengthen individual capability, create supportive opportunities, and cultivate motivation. Interventions should be theoretically grounded in frameworks such as the Capability, Opportunity, Motivation-Behaviour model and adapted to local sociocultural, economic and healthcare contexts – including family and caregiving responsibilities. These interventions must be implemented across individual, community and policy levels. Future research should develop and evaluate integrated interventions to support long-term physical activity participation in this population.
Footnotes
Acknowledgements
We are sincerely thankful to all the participants in the study. This work was supported by the National Natural Science Foundation of China (Grant No. 71603293).
Clinical messages
Barriers and facilitators of leisure-time physical activity among community-dwelling individuals with spinal cord injury map onto the Capability, Opportunity, Motivation-Behaviour model. Interventions should simultaneously enhance capability, expand opportunity and strengthen motivation, and be adapted to country-specific socioeconomic and cultural contexts to improve leisure-time physical activity uptake and sustainability.
Ethical approval
The study was reviewed and approved by the Institutional Review Board of Sun Yat-sen University (Approval No.: L2022SYSU-HL-071). Written informed consent was obtained from each participant.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (Grant No. 71603293).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.