
Abstract
Objective
To examine the association between increased energy and protein intake through oral nutritional supplements and mortality and hospital admissions in older hip fracture patients at nutritional risk, using a preplanned secondary analysis of a randomised controlled trial.
Setting
Department of Orthopaedic Surgery, Copenhagen University Hospital – Herlev and Gentofte, Herlev, Denmark.
Participants
Hip fracture patients aged ≥65 at nutritional risk.
Intervention
Participants were randomised to receive two cans daily of high-energy, high-protein oral nutritional supplements enriched with vitamin D and omega-3 fatty acids for 12 weeks after discharge or standard care.
Main Measures
All-cause mortality and hospital admissions during a pre-planned 38-week follow-up after discharge, including time to first admission and length of hospital stay.
Results
All-cause mortality was low, with no difference between intervention and control groups 2 (3%) versus 3 (5%). During follow-up, 31% (n = 19) of intervention participants was admitted to hospital compared with 47% (n = 29) in the control group. The difference approached significance in the intention-to-treat analysis (Risk ratio 0.72, 95% CI 0.51–1.03, p = 0.075) and was statistically significant in the per-protocol analysis (18% vs. 44%; Risk ratio 0.69, 95% CI 0.52–0.92, p = 0.019). No significant differences were observed in admissions frequency, length of hospital stay, or time to first admission.
Conclusion
Post-discharge oral nutritional supplementation was associated with a trend towards fewer hospital admission, with the strongest effect among adherent participants. No significant effects were observed in mortality, admission frequency, length of hospital stay or time to admission.
ClinicalTrials.gov: NCT05556876. Date of registration: 2022-09-23.
Introduction
Hip fractures represent one of the most serious injuries affecting older adults and are associated with substantial morbidity and mortality. In Denmark, approximately 8% of older patients die within 30 days of a hip fracture, and nearly one in four dies within the first year following injury. 1 In addition to the high mortality burden, hospital readmissions are frequent, with a reported 30-day readmission rate of 15%. 1 This increased risk of death is supported by findings in a systematic review and meta-analysis. 2 The cost of medical and social care, including formal residential care, home adaptations and informal caregiving provided by family and friends, has been reported to be substantial in both international and Danish settings.3,4 Together, these data underscore the severe clinical consequences and healthcare burden associated with hip fractures, especially among malnourished older adults.
A large proportion of older patients sustaining a hip fracture are at nutritional risk or malnourished at the time of admission. Poor nutritional status is independently associated with adverse outcomes, including increased mortality, delayed recovery and a higher risk of hospital admission. 5 In a recent Danish 6-month follow-up study, malnourished hip-fracture patients were three times more likely to be readmitted to hospital one or more times after discharge compared to well-nourished patients (29.2% vs. 9.2%; adjusted OR 4.59, 95% CI 1.70–12.4, p = 0.003), and the total length of hospital stay, including readmissions, was significantly longer. 6 Further, survival analysis from the same study showed an adjusted hazard ratio of 2.48 (95% CI 1.33–4.59, p = 0.004) for mortality over 5 years among patients who were malnourished or at nutritional risk compared with well-nourished patients. 6
Adequate energy and protein intake during hospital admission has been shown to improve survival and reduce readmissions among patients at nutritional risk.5,7 In contrast, a systematic review of previous studies evaluating oral nutritional supplements during the rehabilitation period in older hip fracture patients have generally not found effects on mortality or readmission rates. 8 However, the included studies were performed several years ago and may not reflect the present population and operational procedures. Given the high prevalence of nutritional risk in this population and the potential for nutritional interventions and sufficient energy and protein intake to improve recovery and survival, further investigation is warranted. Therefore, we conducted a preplanned secondary analysis of a randomised clinical trial to investigate the association between increased energy and protein intake through oral nutritional supplements during rehabilitation and mortality, hospital admissions and length of hospital stay in older hip fracture patients at nutritional risk.
Methods
This study was a preplanned secondary analysis of an open-label, parallel-group randomised controlled trial conducted at the Department of Orthopaedic Surgery. All outcomes included in the present analysis were pre-specified prior to data analysis. The study was reported in accordance with the Consolidated Standards of Reporting Trials guidelines. 9 The study was approved by the Danish Regional Ethics Committee of the Capital Region (Journal no.: H-21064554) and the Danish Data Protection Agency (P-2022-293).
Participants were eligible if they were aged ≥65 years, admitted with a hip fracture, at nutritional risk according to the Nutritional Risk Screening 2002, 10 and expected to be discharged with a rehabilitation plan. Eligible fracture types included femoral neck, pertrochanteric, subtrochanteric, distal femur or sequelae of femoral fractures. Key exclusion criteria were active cancer, severe renal insufficiency (estimated glomerular filtration rate <27 mL/min/1.73 m2), cognitive impairment precluding informed consent, terminal illness, exclusive reliance on texture-modified diets, allergies to milk or fish, enteral or parenteral nutrition, current use of fish oil supplements for medical indications or inability to understand Danish. Prescription of oral nutritional supplements at discharge was permitted in both groups and recorded. Due to the nature of the intervention, blinding of participants, care providers and outcome assessors was not feasible; however, data analysts were blinded to group allocation.
Participants were identified through daily screening of admissions and approached by ward-based clinical dietitians. Written and oral study information was provided prior to written informed consent. Participants who declined trial participation were asked for permission to collect follow-up data on hospital admissions and mortality. Those who consented were included in outcome comparisons with trial participants. Baseline characteristics were not collected for non-participants.
Participants were randomised 1:1 using a computer-generated block randomisation sequence with variable block sizes from two to eight. Allocation concealment was ensured using sequentially numbered, opaque, sealed envelopes prepared by an independent staff member. Group allocation was revealed after completion of baseline assessments.
The intervention consisted of two cans daily of high-energy, high-protein oral nutritional supplements enriched with vitamin D and omega-3 fatty acids initiated at discharge and continued for 12 weeks, as previously described. 11 Supplement intake was monitored using daily intake diaries and weekly follow-up. The control group received standard care, which did not include routine provision of oral nutritional supplements at discharge. All participants followed a municipal rehabilitation programme consistent with standard care pathways for hip fracture patients.
The full trial methodology, including detailed descriptions of the intervention, adherence monitoring and primary outcomes, has been reported previously. 12 Baseline nutritional status was additionally described using the Global Leadership Initiative on Malnutrition criteria. 13 the Global Leadership Initiative on Malnutrition criteria uses a two-step approach for the malnutrition diagnosis: first, screening to identify ‘at risk’ status using a validated screening tool, and second, diagnostic assessment and grading the severity of malnutrition. 13 the Global Leadership Initiative on Malnutrition criteria classification was retrospectively derived at baseline using available phenotypic (non-volitional weight loss, low body mass index and reduced muscle mass) and etiologic (reduced food intake or assimilation and inflammation or disease burden) data collected in the parent trial and was not incorporated in the primary publication. Specifically, all patients were considered at nutritional risk in the first step and the Global Leadership Initiative on Malnutrition criteria was operationalised using calf circumference or body mass index as phenotypic criteria and C-reactive protein as an etiologic criterion. 13 Severity grading of malnutrition was not used in the present analysis.
Outcomes
The main outcomes of this secondary analysis were mortality and hospital admissions following discharge. Data were retrieved from the electronic health record system. All-cause mortality at 38 weeks following hospital discharge was assessed as a binary outcome (yes/no) and reported as number of events (percentage). Hospital admissions were assessed in two different ways. First, admissions were recorded as a binary outcome (any admission vs. no admission), and proportions were compared between groups. Second, the number of admissions was analysed as a categorical count variable, and between-group differences in the distribution of admission were assessed. Post-discharge hospital admission was defined as any hospital stay lasting more than 24 h occurring after discharge from the index hip fracture hospitalisation, regardless of cause or planning status. Length of stay was assessed and reported as total number of days during post-discharge admissions. Time until first post-discharge admission was reported as median number of days from hospital discharge. All outcomes were analysed for between group differences according to randomised allocation.
Statistics
Continuous variables are presented as medians (interquartile range) and categorical variables as number (percentage). Between-group comparisons were performed using appropriate parametric or non-parametric tests, and categorical variables were compared using the χ2 or Fisher's exact test, as appropriate, based on data distribution. Given the low prevalence of mortality events in the study population, time-to-event analysis using Kaplan–Meier methods was considered statistically underpowered and potentially unreliable. Analyses were conducted according to the intention-to-treat principle, with per-protocol analyses excluding participants with compliance < 75% to the planned two servings of the high-protein, micronutrient-enriched oral nutritional supplement in the intervention group performed as sensitivity analyses. For categorical outcomes, including post-discharge mortality and hospital admissions, between-group differences were quantified using risk ratios with 95% confidence intervals, calculated as the ratio of event risk in the intervention group to that in the control group. Statistical analyses were performed using Statistical Analysis System, Version 8.
Results
All 123 randomised participants were included in the intention-to-treat analyses. Participant flow is identical to that reported in the primary trial publication and is therefore not reproduced here.
Mean compliance with the study oral nutritional supplements was 66% (n = 54), based on counting cans, and 85% based on daily drink diaries. The weighted mean compliance was 72% (n = 54), corresponding to a mean intake of 1.44 cans per day. In total, 28 of 54 participants (52%) in the intervention group met the predefined compliance criterion (≥75%) and were included in the per-protocol analyses.
The protein intake was significantly higher in the intervention group compared with the control group (p = 0.003). Energy intake showed a trend towards a between-group difference, with a higher intake in the intervention group (p = 0.064). In the per-protocol analysis, both the energy and protein intake was significantly increased in the intervention group compared to the control group (p = 0.003, p = <.001) 12 (Table 1).
Baseline characteristics of the study population.
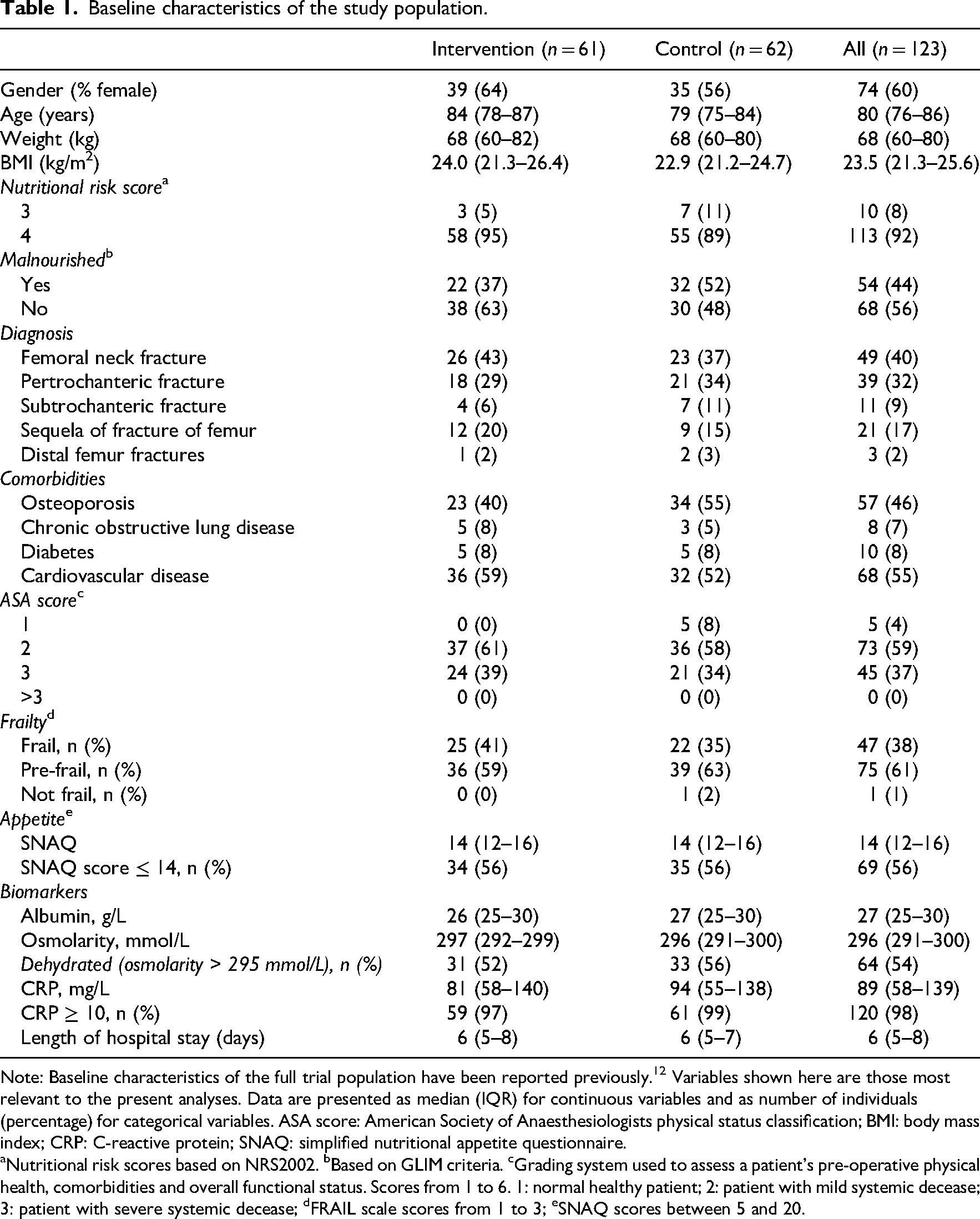
Note: Baseline characteristics of the full trial population have been reported previously. 12 Variables shown here are those most relevant to the present analyses. Data are presented as median (IQR) for continuous variables and as number of individuals (percentage) for categorical variables. ASA score: American Society of Anaesthesiologists physical status classification; BMI: body mass index; CRP: C-reactive protein; SNAQ: simplified nutritional appetite questionnaire.
Nutritional risk scores based on NRS2002. bBased on GLIM criteria. cGrading system used to assess a patient's pre-operative physical health, comorbidities and overall functional status. Scores from 1 to 6. 1: normal healthy patient; 2: patient with mild systemic decease; 3: patient with severe systemic decease; dFRAIL scale scores from 1 to 3; eSNAQ scores between 5 and 20.
Post-discharge all-cause mortality
At 38-week follow-up, mortality was 3% (n = 2) in the intervention group and 5% (n = 3) in the control group, with no significant difference between groups (Table 2). In the per-protocol analysis, no deaths occurred in the intervention group, compared with 4% (n = 2) in the control group, also without a significant difference (Table 3).
Results on 38-week mortality, hospital admissions and length of stay.
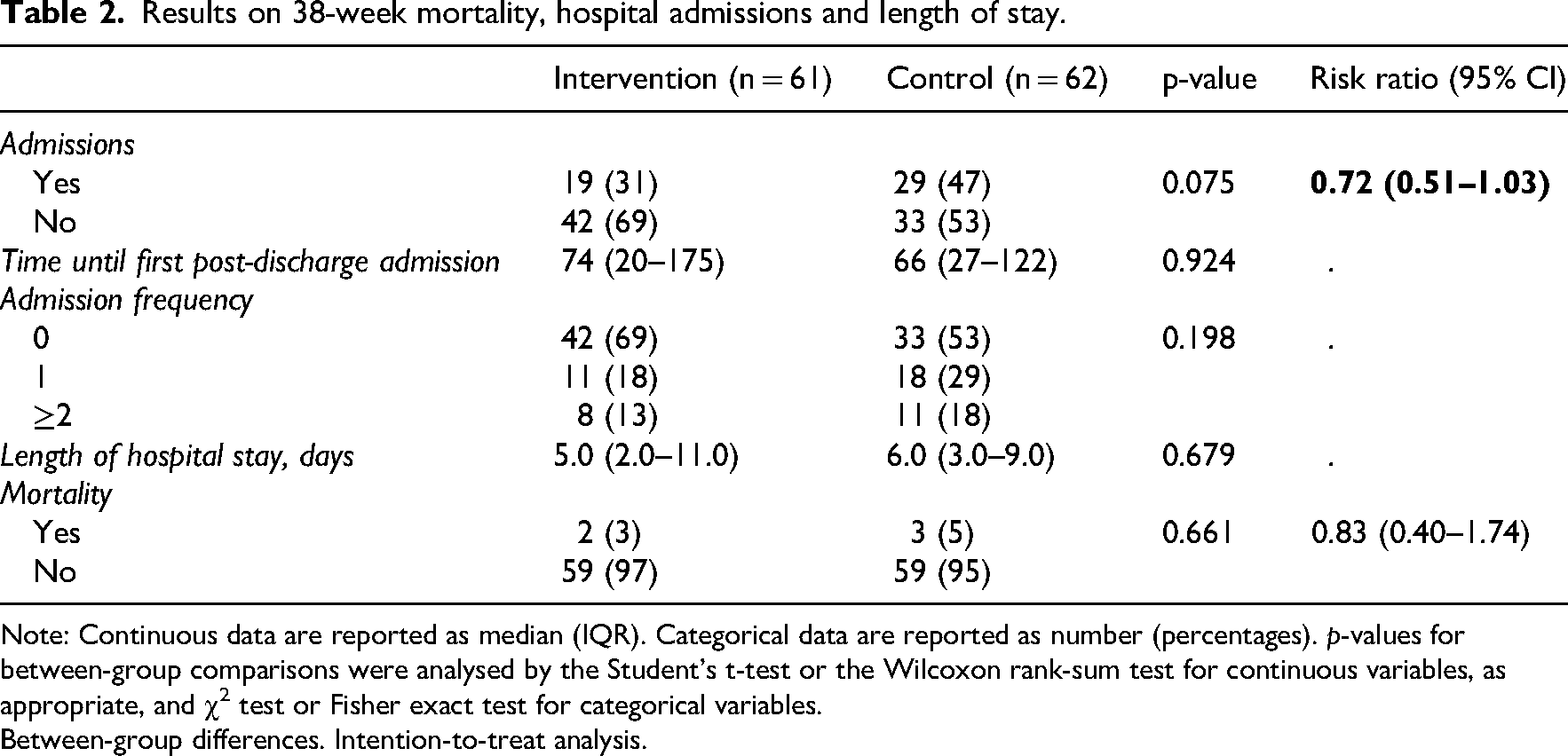
Note: Continuous data are reported as median (IQR). Categorical data are reported as number (percentages). p-values for between-group comparisons were analysed by the Student’s t-test or the Wilcoxon rank-sum test for continuous variables, as appropriate, and χ2 test or Fisher exact test for categorical variables.
Between-group differences. Intention-to-treat analysis.
Results on 38-week mortality, hospital admissions and length of stay.
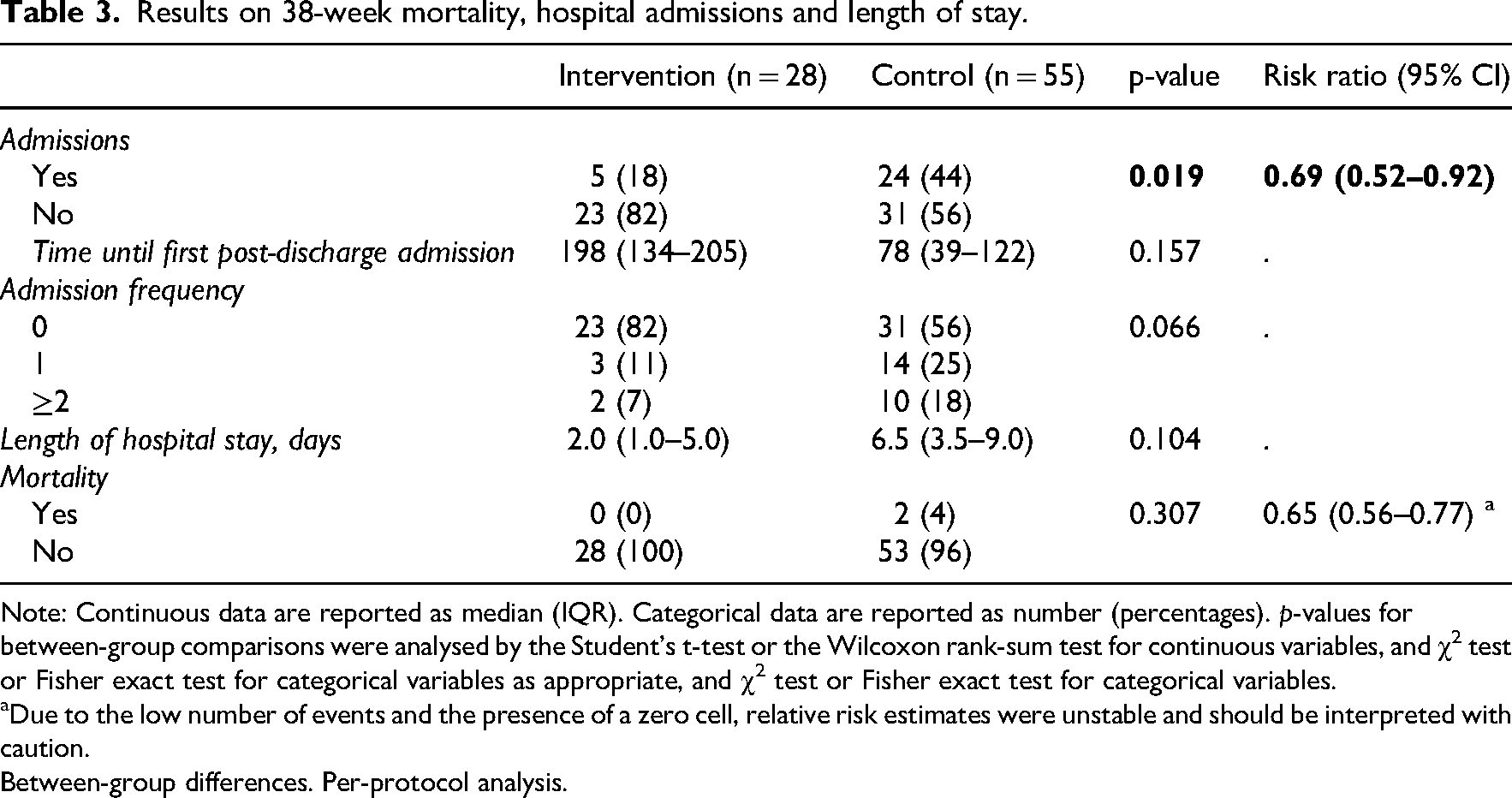
Note: Continuous data are reported as median (IQR). Categorical data are reported as number (percentages). p-values for between-group comparisons were analysed by the Student’s t-test or the Wilcoxon rank-sum test for continuous variables, and χ2 test or Fisher exact test for categorical variables as appropriate, and χ2 test or Fisher exact test for categorical variables.
Due to the low number of events and the presence of a zero cell, relative risk estimates were unstable and should be interpreted with caution.
Between-group differences. Per-protocol analysis.
Post-discharge hospital admissions
At 38-week follow-up, 31% (n = 19) of the participants in the intervention group were admitted to the hospital post-discharge, compared with 47% (n = 29) in the control group (Figure 1). The risk of post-discharge admission was lower in the intervention group, and was borderline statistically significant (Risk Ratio 0.72, 95% Confidence interval 0.51–1.03, p = 0.075) (Table 2). When comparing the groups in the per-protocol analysis, the difference reached significance (Risk ratio 0.69, 95% Confidence interval 0.52–0.92, p = 0.019) (Table 3). A total of 18% (n = 5) of the participants in the intervention group were admitted post-discharge compared with 44% (n = 24) in the control group (Figure 2). Post-discharge admission frequency did not differ in the intention-to-treat analysis but tended to be lower in the per-protocol analysis (Tables 2 and 3).
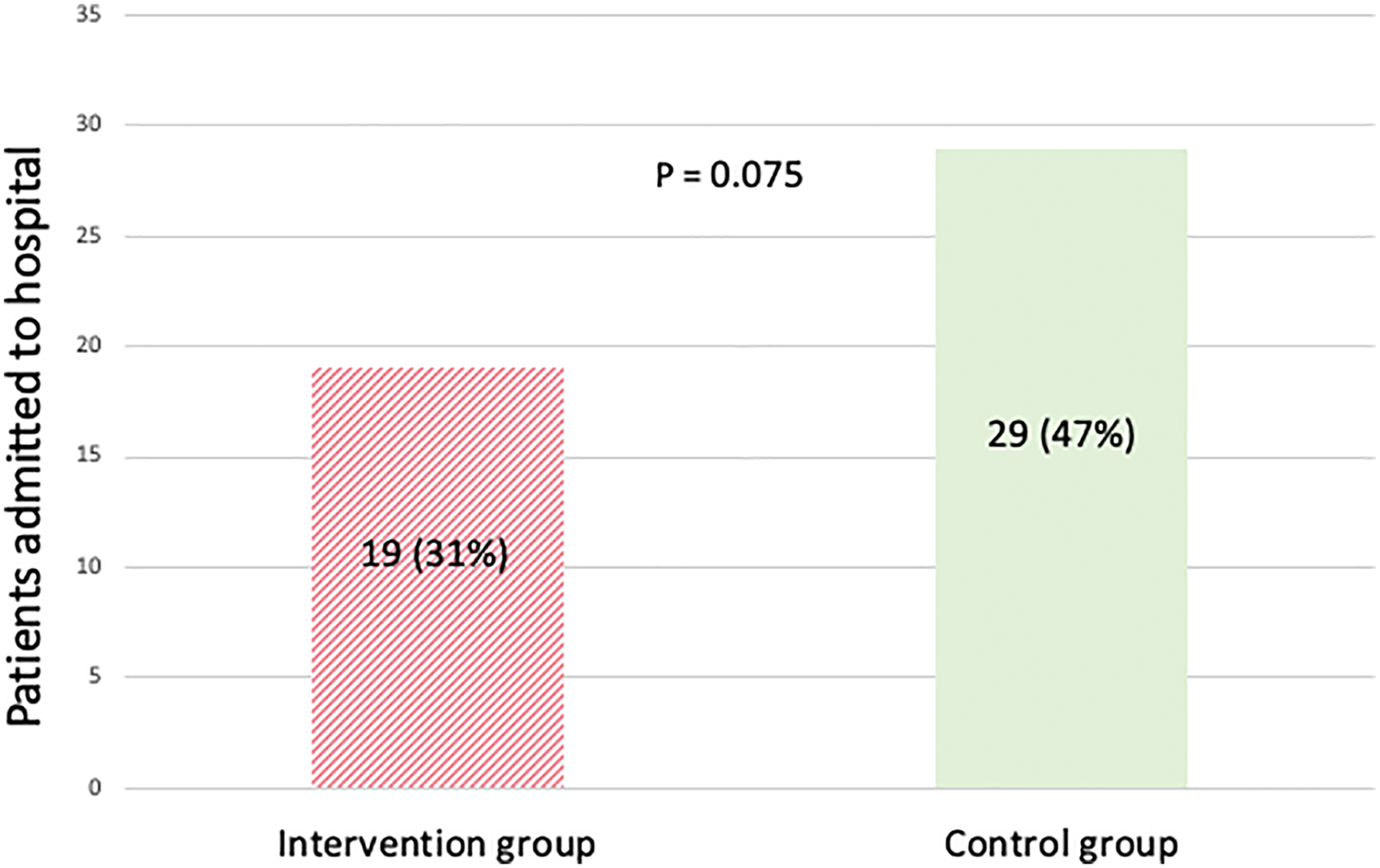
Number of patients admitted to hospital after discharge at 38-week follow-up. Intention-to-treat analysis. Data are expressed as number (percentages). p-values for between-group comparisons were analysed by the χ2 test.
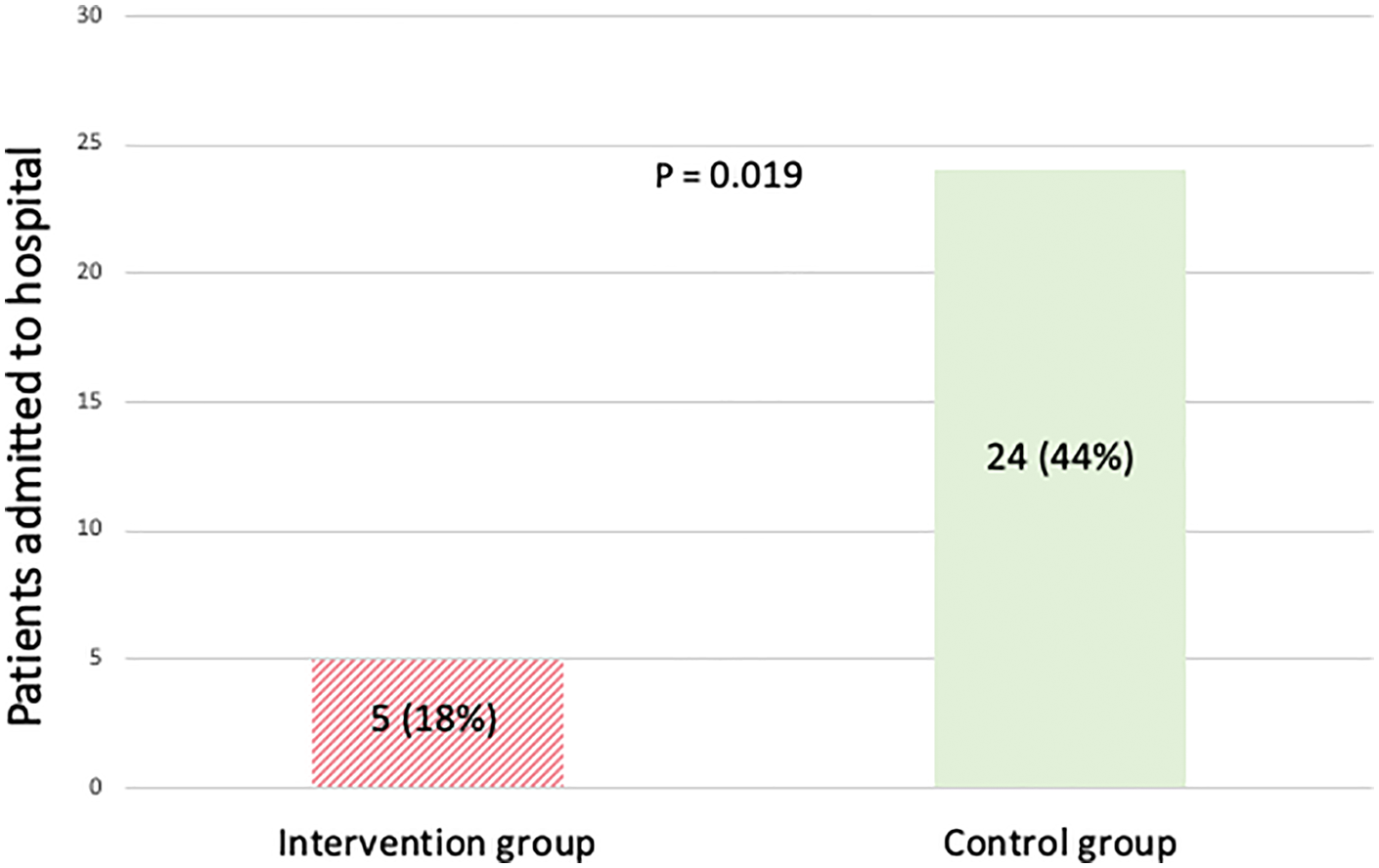
Number of patients admitted to hospital after discharge at 38-week follow-up. Per-protocol analysis. Data are expressed as number (percentages). p-values for between-group comparisons were analysed by the χ2 test.
Length of hospital stay and time until first post-discharge admission
Length of hospital stay did not differ between the intervention and control groups in either of the analyses (Tables 2 and 3). In the intention-to-treat analysis, the median time until first post-discharge admission was 74 days (20–175) in the intervention group and 66 days (27–122) in the control group, with no significant difference between groups (p = 0.924). In the per-protocol analysis, the median time was 198 days (134–205) in the intervention group compared with 78 days (39–159) in the control group. This difference did not reach statistically significance (p = 0.157).
Comparison between non-participants and included participants
A total of 46 patients who declined trial participation consented to follow-up assessment of admissions and mortality. No significant differences were observed between non-participants and trial participants for admission risk, time to first admission, admission frequency, length of hospital stay or mortality (Table 4).
Results on 38-week mortality, hospital admissions, and length of stay.
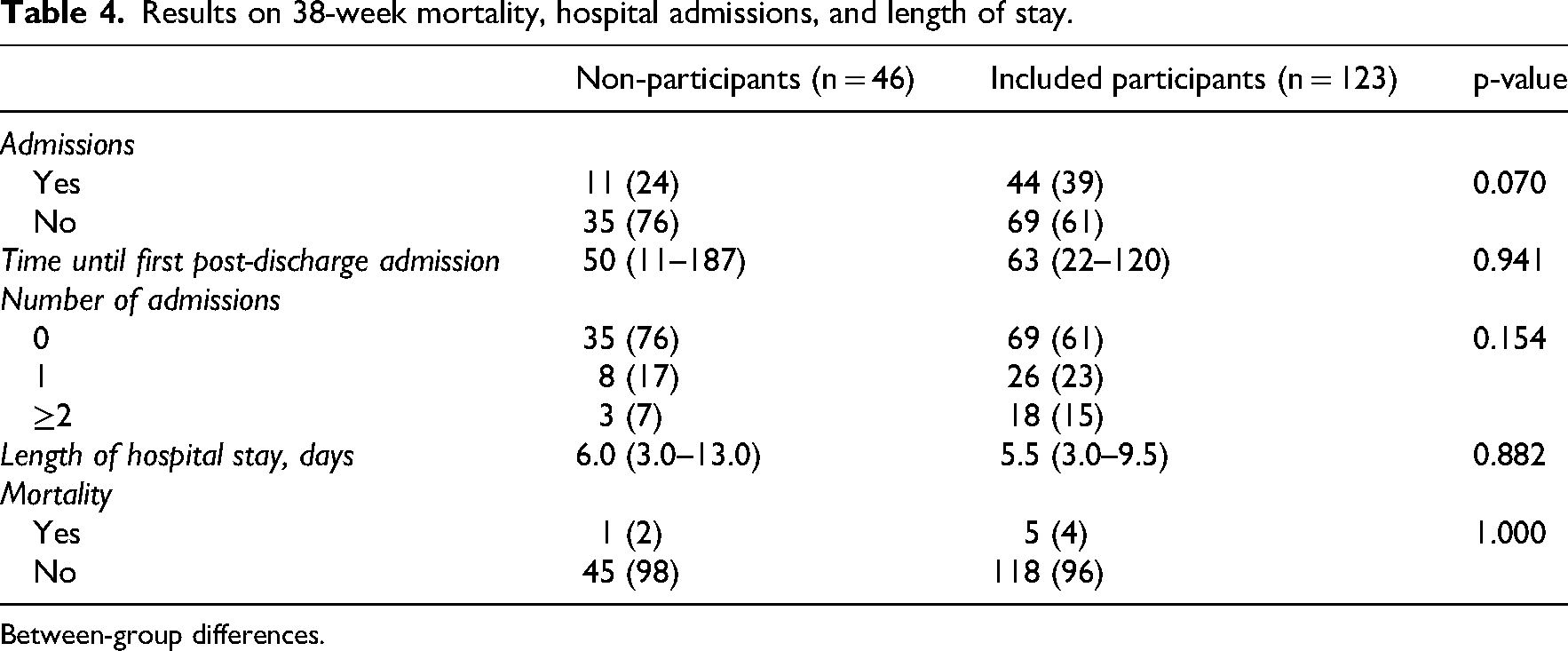
Between-group differences.
Discussion
In this study, an increased intake of energy and protein through oral nutritional supplements during rehabilitation showed no statistically significant between-group differences in mortality, admission frequency, length of hospital stay or time to first post-discharge admission in the intention-to-treat analysis. The intervention was associated with fewer patients being admitted to hospital compared with usual care. The difference approached statistical significance in the intention-to-treat analysis and reached statistical significance in the per-protocol analysis, suggesting a potential benefit among participants who adhered to the intervention. Additionally, admission frequency was lower in the intervention group and trended towards significance in the per-protocol analysis. However, these per-protocol findings must be interpreted cautiously, as adherence-based analyses are inherently non-randomised and may be influenced by residual confounding.
The significant lower number of patients admitted to hospital observed in the per-protocol analysis may reflect the improvements in nutritional intake and physical functional performance seen among participants with high compliance. 12 This suggests that adherence to oral nutritional supplementation may be a key determinant of potential clinical effectiveness. Insufficient compliance could partly explain the lack of significant effects on mortality and hospital admissions reported in previous studies. 8 As previously reported in the primary analysis of this study, increased energy and protein intake was associated with improved physical functional performance measured by the 30-s chair stand test. 12 Improved nutritional status may enhance muscle strength and functional reserve, potentially reducing the risk of complications, falls and functional decline, which could contribute to a reduced number of hospital admission. Nevertheless, adherence itself may reflect underlying differences in health status, motivation or recovery trajectory, which limits causal interpretation of the per-protocol findings.
Beyond the clinical consequences, hip fractures are associated with substantial societal costs, including expenses related to formal residential care, home adaptations and informal caregiving from family members. Therefore, even modest reductions in hospital admissions or functional decline may have important economic implications. Although our study was not designed to evaluate cost-effectiveness, the observed association between higher compliance and fewer hospital admissions suggests that strategies aimed at improving adherence to oral nutritional supplementation could potentially contribute to reducing healthcare utilisation and related costs.
The study population exhibited lower mortality rates than those reported in national registry data. 1 Overall mortality in the study population was 5% at 38-week follow-up, compared with approximately 25% 1-year mortality reported nationally. This discrepancy suggests that the study population may represent a healthier subset of older patients with hip fracture, which could limit generalisability and potentially underestimate the benefits of nutritional supplementation in frailer patients. Such selection bias is common in studies requiring informed consent and active participation, as inclusion depends on clinical stability and cognitive capacity. Consequently, critically ill patients and those with significant cognitive impairment were not eligible, although these groups account for a substantial proportion of mortality and hospital admissions in the broader hip fracture population. While no differences were observed between included participants and those who declined participation, the requirement for eligibility likely resulted in a healthier cohort compared with the overall registry population.
The relatively healthier study population may also have influenced adherence to oral nutritional supplements. Participation required clinical stability and cognitive capacity, which likely resulted in the inclusion of more motivated and functionally capable patients. Overall compliance with oral nutritional supplements was 66%. Although 54 participants completed the intervention period, only 28 achieved a compliance level of ≥75%, a threshold associated with improved hospital admissions and physical functional performance. 12 It is plausible that adherence would be lower in a more frail and clinically complex hip fracture population, where poor appetite, fatigue, cognitive impairment and postoperative complications may further challenge consistent intake. Consequently, the feasibility and effectiveness of oral nutritional supplements observed in this study may not fully translate to the broader, more vulnerable hip fracture population. Given that higher compliance appears essential to achieve clinically meaningful effects, future research should focus on strategies to improve adherence, particularly among frailer patients.
A strength of this study is that it is based on data from a randomised controlled trial, ensuring high internal validity and reducing confounding between the intervention and control groups. Data were collected prospectively using standardised procedures and predefined outcomes, and registry-based data on mortality and hospital admissions minimised the risk of recall bias and incomplete follow-up.
However, as a secondary analysis, the study was not originally powered to detect differences in hospital admissions or mortality. The analyses may therefore be underpowered to identify smaller, yet clinically relevant, effects. The limited number of mortality events further reduces statistical precision and increases uncertainty around effect estimates. Accordingly, the findings should be interpreted as exploratory and hypothesis – generating rather than confirmatory.
In conclusion, among older hip fracture patients at nutritional risk, oral nutritional supplements during rehabilitation did not significantly reduce mortality or hospital admissions in the intention-to-treat analysis. Per-protocol analyses suggest potential benefits among participants with high adherence, highlighting the importance of compliance for achieving clinically meaningful effects. These findings underscore the potential role of nutritional interventions in supporting recovery and reducing healthcare utilisation, and emphasise the need for strategies to improve adherence, particularly in frailer patients. Future adequately powered trials are warranted to determine whether optimised nutritional support through oral supplements can reduce mortality and decrease hospital admissions in this vulnerable population.
High compliance (≥75%) was associated with fewer hospital admissions, suggesting that sufficient intake is essential for potential clinical benefit. Clinicians should prioritise strategies that support compliance to oral nutritional supplements, particularly in frail patients where consistent intake may be most challenging.Clinical messages
Footnotes
Acknowledgements
We gratefully acknowledge the staff of the Department of Orthopaedic Surgery for their support of the original trial and their assistance with participant inclusion. We also thank the clinical dietitians for conducting the secondary screening procedures and initiating contact with eligible participants. Finally, we sincerely thank all patients who participated in the trial, as this secondary analysis would not have been possible without their valuable contribution.
Ethics considerations and consent to participate
The study was approved by the Danish Regional Ethics Committee of the Capital Region (Journal no.: H-21064554) and the Danish Data Protection Agency (P-2022–293). All eligible participants received written and oral information and provided written informed consent prior to enrolment. During the trial, the Ethics Committee approved a protocol amendment permitting the assessment of hydration status at follow-up.
Author contributions
AJ, EDN, AMB, TM and AWK contributed to drafting and revising the manuscript. The trial was conducted by AJ and EDN, who were also responsible for data collection. AJ managed and cleaned the dataset. Statistical analyses were performed by AJ and AWK. The analytical strategy was developed by AMB, AWK and AJ. All authors critically reviewed and approved the final version of the manuscript.
Funding
The study was funded by Nutricia DANONE. They were not involved in trial conduct or reporting.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data availability statement
Data are not available.