
Abstract
Objective
To analyse physical fitness trajectories in paediatric burn survivors from discharge to 2 years post-injury, compare them with an age- and gender-matched control group, and identify baseline demographic and clinical determinants.
Design
Prospective and longitudinal cohort study.
Participants
The study included participants with burn injuries (burn group, n = 45), aged 10–17 years, with burns involving ≥25% of total body surface area, and an age- and gender-matched group of healthy children (control group, n = 45).
Main measures
Participants underwent standardised fitness assessments at discharge and 24 months later. Health-related physical fitness was quantitatively assessed using the validated EUROFIT physical fitness test battery.
Results
Longitudinal analysis revealed significant improvements in seven of nine fitness domains for participants with burn injuries over two years (pFDR < 0.001). Despite these gains, these participants exhibited persistent fitness deficits compared to healthy controls across all domains at follow-up (all p < 0.001). Among those with burn injuries, greater total body surface area (β = –0.007, p = 0.03) and third-degree burn percentage (β = –0.57, p < 0.001) predicted lower overall fitness, while longer rehabilitation predicted higher fitness (β = 0.50, p < 0.001). No baseline clinical factors significantly predicted the rate of fitness change over time (all interaction p > 0.05).
Conclusion
Paediatric burn survivors demonstrated significant improvements in physical fitness over 2 years but failed to close the performance gap with their healthy peers. Injury severity and rehabilitation duration were strong determinants of fitness level, but they did not predict the rate of improvement.
Keywords
Introduction
Following discharge from medical care, burn survivors face a prolonged recovery, with significant risks to physical function. A major obstacle is the ‘negative cycle of deconditioning’, whereby post-injury inactivity fosters a downward spiral of worsening physical condition, functional decline and potential disability.1,2 This challenge is magnified in paediatric patients, for whom sustained physical activity is integral to healthy development. As childhood is the period during which foundational motor skills and health habits are formed, maintaining functional capacity is imperative for preventing long-term impairments and chronic disease.1–4
The evolution of modern burn care has been marked by a significant reduction in mortality. This achievement has altered the focus, shifting the primary objective from survival to the optimisation of long-term functional outcomes and quality of life.5–7 In line with this paradigm shift, specialised burn centres have implemented multidisciplinary rehabilitation programmes that commence at admission and extend into the post-discharge period.6–9 Despite these advancements, a substantial cohort of burn survivors continues to report enduring deficits in physical and psychological health, which compromise their overall well-being.10,11
Restoring physical function is critical for paediatric burn survivors because childhood and adolescence are foundational periods for neuromuscular development and lifelong health trajectories.3,4,12 Burn injury creates major obstacles to physical fitness due to a hypermetabolic, hypercatabolic state combined with immobilisation, leading to rapid physical deconditioning.13–15 This systemic response persists for two to three years post-injury, leading to significant muscle wasting, diminished lean body mass and profound fatigability.9,10,15
Although existing rehabilitative strategies have demonstrated efficacy in improving functional outcomes following hospital discharge,6,7,16,17 the long-term effectiveness of these interventions remains inadequately characterised. A critical gap exists in our understanding of whether paediatric burn survivors eventually catch up to their healthy peers or whether a persistent deficit in physical fitness remains. This study, therefore, was designed to address this critical knowledge gap.
The specific aims were: (1) to longitudinally analyse the trajectories of key health-related physical fitness components (balance, flexibility, muscular strength, power, speed, agility and cardiorespiratory endurance) in paediatric burn survivors from discharge to two years post-injury, and to compare these trajectories against an age- and gender-matched control group; and (2) to identify the baseline demographic and clinical determinants of physical fitness trajectories within the burn-injured cohort.
Materials and methods
Study protocol and participants
This prospective, longitudinal cohort study was approved by the Research Ethics Committee of the Faculty of Physical Therapy at Cairo University (P.T.REC/012/004940). Prior to enrolment, written informed consent was obtained from the parents or legal guardians of all participants. Child assent was secured. The study was conducted in accordance with the Declaration of Helsinki.
A cohort of paediatric patients was recruited following discharge. Inclusion criteria were: (1) age between 10 and 17 years; (2) total body surface area burn injury of ≥25% and (3) participation in a post-discharge rehabilitative exercise programme. During hospitalisation, all patients received standard burn treatment, including medical management, wound care and a physiotherapy-led mobilisation programme. Exclusion criteria included non-thermal injuries, unhealed or open wounds and respiratory, cardiac, neurological or neuromuscular deficits.
The control group included age- and gender-matched healthy children (n = 45) recruited through public flyers, word-of-mouth and siblings of the patients. Each participant in the burn cohort was individually matched to a healthy control by age (±6 months) and gender. This matching was maintained across both assessment time points. To ensure a valid comparison between cohorts, children with respiratory, cardiac, neurological or neuromuscular conditions were excluded.
For this analysis, data were utilised from two assessment points. The initial evaluation of health-related physical fitness in the burn cohort was conducted at the time of hospital discharge. A follow-up evaluation was performed 24 months later to establish the long-term fitness trajectory. The control cohort underwent identical assessments at corresponding time intervals to provide a comparative reference.
Assessment procedures
Physical fitness was assessed using the validated EUROFIT test battery.18,19 The EUROFIT battery is a standardised, multidimensional field-based assessment designed for school-aged children and adolescents and evaluates several fitness domains, including balance, flexibility, muscular strength, muscular endurance, power, speed, agility, coordination and cardiorespiratory endurance. Nine EUROFIT-based tests were administered: the Flamingo balance test, Plate Tapping test, Sit-and-Reach test, Standing Broad Jump, Handgrip Strength test, 30-s Sit-Up test, Bent Arm Hang test, 10 × 5-m Shuttle Run test and 20-m Multistage Shuttle Run test. These tests were completed during a single assessment session, following one familiarisation session. All participants completed the same testing protocol at baseline and at the 24-month follow-up.
Prior to testing, participants attended one introductory session to familiarise themselves with the protocol and receive instruction on proper technique. Participants were instructed to abstain from strenuous physical activity for 48 h preceding the test day. All measurements were preceded by a standardised 10-min warm-up consisting of light jogging and dynamic stretching. Before each test, participants were reminded of the importance of providing a maximal effort.
Anthropometric data were collected prior to fitness testing. Height was measured to the nearest 0.1 cm using a wall-mounted stadiometer (SECA, model 220, Hamburg, Germany). Body mass was measured to the nearest 0.1 kg using a digital scale (HBF-352-W, Omron Healthcare Co., Kyoto, Japan). Body Mass Index (BMI) was subsequently calculated using the standard Quetelet's formula: BMI = mass (kg) / height (m)2.
Health-related physical fitness assessments
Flamingo Balance Test was used to measure static balance. Participants stood barefoot on a narrow beam with their preferred leg, with the opposite leg flexed and held at the ankle. The trial was initiated on a verbal command. The timer was paused each time the participant lost balance, released the held foot, or touched the floor, and was restarted once the correct position was regained. If a participant lost balance more than 15 times within the first 30 s, the test was terminated, and a score of zero was recorded. The final score was the total number of balance losses over the 60-s period.
The Plate Tapping Test was used to measure upper-limb movement speed and hand-eye coordination. The participant stood in front of a table with two target discs (20 cm diameter) placed 60 cm apart. A rectangular plate was positioned centred between them. The non-preferred hand was placed on the central plate while the preferred hand moved back and forth between the two outer discs as rapidly as possible for 25 cycles (50 taps). The time taken to complete the 50 taps was recorded to the nearest 0.1 s. The best of two trials was used for analysis.
The Sit-and-Reach Test was used to measure flexibility of the lower back and hamstring muscles using a standard sit-and-reach box. Participants sat on the floor with legs fully extended, feet placed flat against the box. They were instructed to reach forward smoothly along the measuring scale with both hands and palms down and hold the maximal reach position for at least two seconds. The score was the furthest point reached, measured in centimetres. The best of two trials was recorded for analysis.
The Standing Broad Jump Test was used to assess lower-body muscular power by measuring the maximum horizontal distance jumped from a static start. Participants stood with feet parallel behind a starting line and performed a two-footed maximal forward jump, propelling themselves with both arm and leg action. The distance was measured in centimetres from the starting line to the point where the back of the heels landed. A stable, upright landing was required. The best of two trials was recorded for analysis.
Handgrip strength was assessed by measuring the maximal voluntary isometric grip force of the preferred hand using a calibrated handheld dynamometer (Jamar). Participants gripped the dynamometer with their preferred hand with the arm hanging down by the side of the body. On command, they squeezed the dynamometer with maximal effort for 3–5 s. The peak force achieved, recorded in kilograms, was noted. The best of two trials, separated by a 30-s rest interval, were used for analysis.
The Sit-Up Test was used to assess trunk muscle endurance by recording the maximum number of completed sit-ups in 30 s. Participants lay in a supine position with knees flexed to 90 degrees and feet flat on the floor. The assessor stabilised the ankles. On command, the participant performed repeated trunk flexions until their elbows touched their ipsilateral knees, then returned to the starting position where their scapulae contacted the mat. The total number of correctly performed repetitions in 30 s was recorded from a single trial.
The Bent Arm Hang Test was used to assess upper-body relative strength and endurance by measuring the duration for which a static flexed-arm position could be maintained. The participants used an overhead pronated grip, shoulder-width apart to hang from a horizontal bar. They were assisted into a position where their elbows were flexed, and their chin was held above the bar without touching it. The timer started when they were released and stopped when their eyes descended below the level of the bar. The total time, recorded in seconds from a single trial, was used as the score.
The 10 × 5-m Shuttle Run Test was used to assess agility and speed of movement. Two parallel lines were marked 5-m apart on a non-slip surface. On a verbal command, participants ran from a standing start at one line to the other, touched the line with one foot, and returned to the starting line. This circuit was completed five times without rest, covering a total distance of 50-m. The total time taken to complete the 50-m course was recorded to the nearest 0.1 s. A single trial was administered.
The 20-m Multistage Shuttle Run Test was used to measure cardiorespiratory endurance. The test required participants to run back and forth between two lines set 20-m apart on a non-slip surface. The running pace was dictated by pre-recorded audio signals (beeps). The speed required to complete each shuttle progressively increased at 1-min intervals (stages). The test was terminated when the participant failed to reach the designated line in time with the audio signal on two consecutive occasions (volitional exhaustion). The final score was recorded as the last successfully completed stage and shuttle number, which was then used to estimate maximal aerobic capacity. A single trial was performed.
Statistical analysis
Analyses were performed using IBM SPSS Statistics (v28, IBM Corp., Armonk, NY, USA). A two-sided significance level of 0.05 was used, and adjustments for multiple comparisons were applied. To assess fitness differences between groups across the two time points, each of the nine tests was analysed separately. A series of linear mixed-effects models was fitted for each test. Each model included group (patients vs. control), time (baseline vs. 2-year) and their interaction term as fixed effects. A random intercept for subject ID was incorporated to account for within-subject correlation. The Group × Time interaction term was the primary effect of interest, testing whether longitudinal change differed between groups. To control the family-wise error rate, the False Discovery Rate (FDR) correction was applied to the p-values. For any test that exhibited statistically significant interaction after FDR correction, post-hoc analyses of simple effects were conducted using estimated marginal means with Bonferroni's adjustment.
To explore how baseline clinical factors predicted fitness, a composite score was utilised. This score was created by standardising each of the nine raw test scores into Z-scores. All Z-scores were oriented so that higher values indicate better fitness, and the composite score was calculated as the mean of their nine Z-scores. A linear mixed-effects model was constructed using data from the patient cohort only, with the composite score as the dependent variable. The model included time and time-invariant clinical factors as fixed effects, along with interaction terms between time and each clinical factor to determine if characteristics predicted the rate of change. A random intercept for subjects was included. Model selection was performed using Least Absolute Shrinkage and Selection Operator regression to identify a parsimonious set of predictors and mitigate overfitting. In the final model, a significant main effect for a clinical factor indicated it predicted an overall higher or lower fitness score, while a significant time x clinical factor interaction indicated the baseline factor predicted a trajectory of fitness change.
Results
Baseline characteristics of the study cohorts
The study enrolled 90 participants, comprising two cohorts (burn-injured group and healthy control) of equal size (n = 45). The baseline demographic and clinical characteristics of both cohorts are detailed in Table 1. The groups were statistically comparable at the baseline, with no significant differences observed in age (p = 0.44), sex distribution (p = 0.83), weight (p = 0.52), height (p = 0.69) or body mass index (p = 0.34). The burn group had a mean hospital stay of 55.60 days, a mean total body surface area burned of 40.44%, a mean third-degree burn involvement of 18.47% and underwent rehabilitation for a mean duration of 4.42 months.
Baseline demographic and clinical characteristics of the burn and control cohorts.
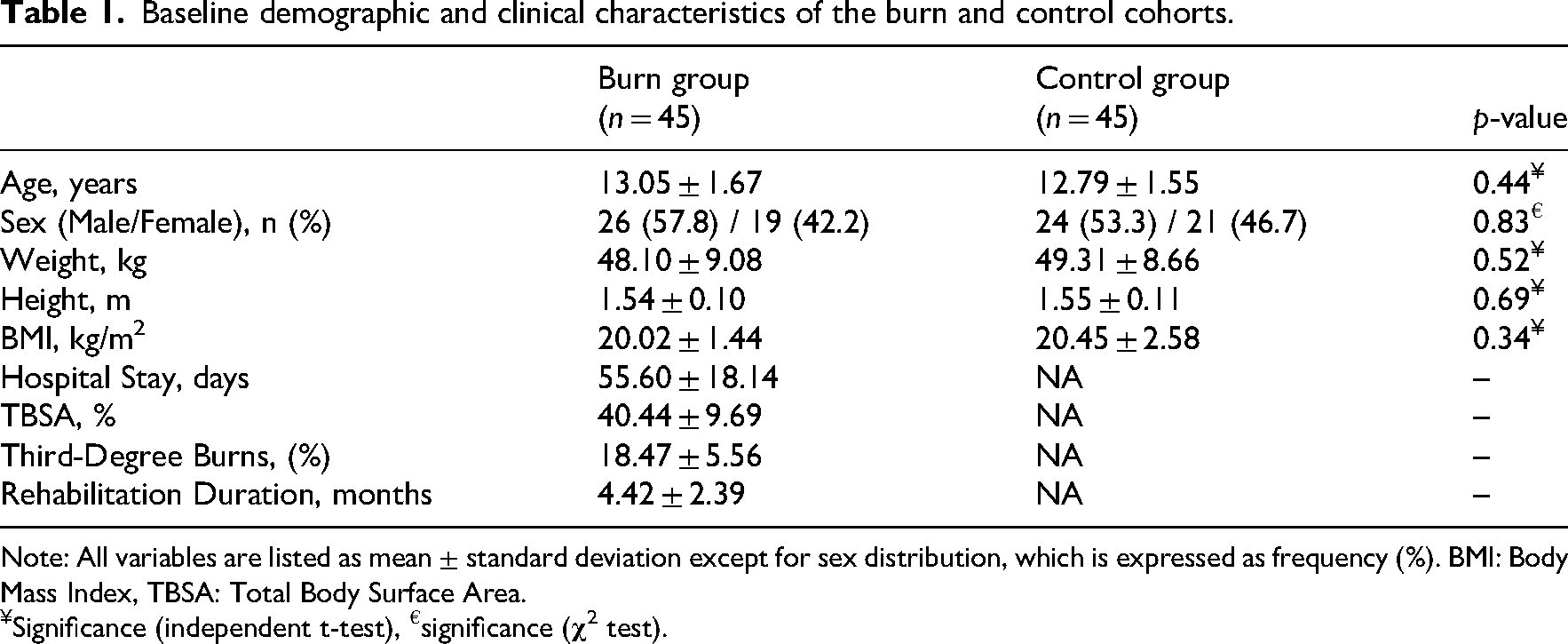
Note: All variables are listed as mean ± standard deviation except for sex distribution, which is expressed as frequency (%). BMI: Body Mass Index, TBSA: Total Body Surface Area.
Significance (independent t-test), €significance (
Differential changes in fitness domains over time:
The longitudinal analysis of the nine fitness variables revealed distinct trajectories between the burn and control groups over the 2 years. The linear mixed models identified statistically significant Group × Time interactions for seven measures after correction for multiple comparisons using the False Discovery Rate: Flamingo test (F1,88 = 92.697; pFDR = 2.09 × 10−15), Plate tapping (F1,88 = 104.710; pFDR = 1.19 × 10−16), Standing Broad Jump (F1,88 = 158.709; pFDR = 2.1 × 10−21), hand grip strength (F1,88 = 24.963; pFDR = 3 × 10−6), Sit-Up (F1,88 = 53.443; pFDR = 1.16 × 10−10), 10 × 5 m Shuttle Run (F1,88 = 234.701; pFDR = 1.47 × 10−26) and 20 m Shuttle Run (F1,88 = 78.037; pFDR = 9.02 × 10−14). The interactions for the other two tests were not statistically significant after False Discovery Rate adjustment (all pFDR > 0.05), indicating parallel trajectories for patients and controls in these domains (Table 2).
Longitudinal comparison of fitness measures between burn and control groups.
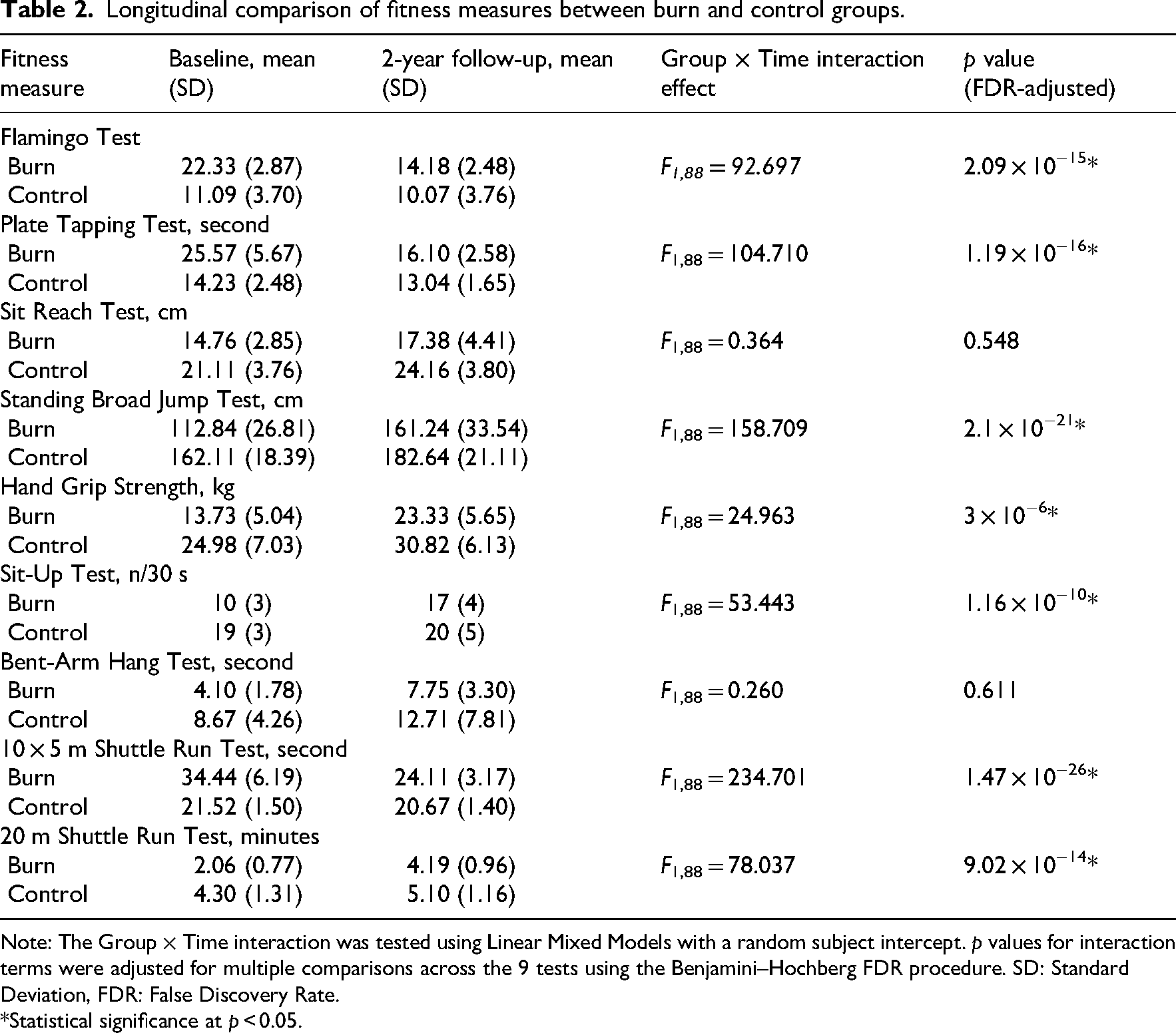
Note: The Group × Time interaction was tested using Linear Mixed Models with a random subject intercept. p values for interaction terms were adjusted for multiple comparisons across the 9 tests using the Benjamini–Hochberg FDR procedure. SD: Standard Deviation, FDR: False Discovery Rate.
*Statistical significance at p < 0.05.
Post-hoc analysis consistently showed that the patient group demonstrated significant improvements in all these measures over time (all p < 0.001), whereas the control group performance remained stable in the Flamingo and 10 × 5 m shuttle run tests (p = 0.054 and p = 0.054, respectively), improved significantly in hand grip strength (p < 0.001), standing broad jump (p < 0.001), sit-up (p = 0.004), 20 m shuttle run (p < 0.001) tests and showed only modest, though significant, improvements in the plate tapping test (p = 0.042). Despite these marked improvements, the patient group's performance remained poorer than that of the healthy controls across all domains at the 2-year follow-up (all p < 0.001), suggesting a persistent fitness deficit.
Predictors of fitness in burn cohort
The linear mixed model analysis revealed several significant baseline predictors of overall fitness levels (composite fitness score) in the burn group, but no predictors of fitness change over time. The main effect of time was non-significant (F1,76 = 2.63, p = 0.109) indicating no systematic change in the composite fitness score across the entire patient cohort from baseline to the 2-year follow-up. Among the clinical factors, both the TBSA affected by burns (β = –0.007, p = 0.03) and percentage of third-degree burns (β = –0.57, p < 0.001) were significant negative predictors, with greater burn severity associated with lower overall fitness scores. Conversely, rehabilitation duration was a significant positive predictor (β = 0.50, p < 0.001), with longer rehabilitation associated with higher fitness levels. Age, sex and hospital stay duration showed no significant associations with fitness level (p = 0.912, p = 0.341 and p = 0.977, respectively). Crucially, none of the Time x Predictor interaction terms reached statistical significance (all p > 0.05), indicating that none of the baseline clinical factors predicted the rate of fitness change over the 2-year study period (Table 3).
Linear mixed model analysis of baseline predictors for composite fitness score in burn cohort.
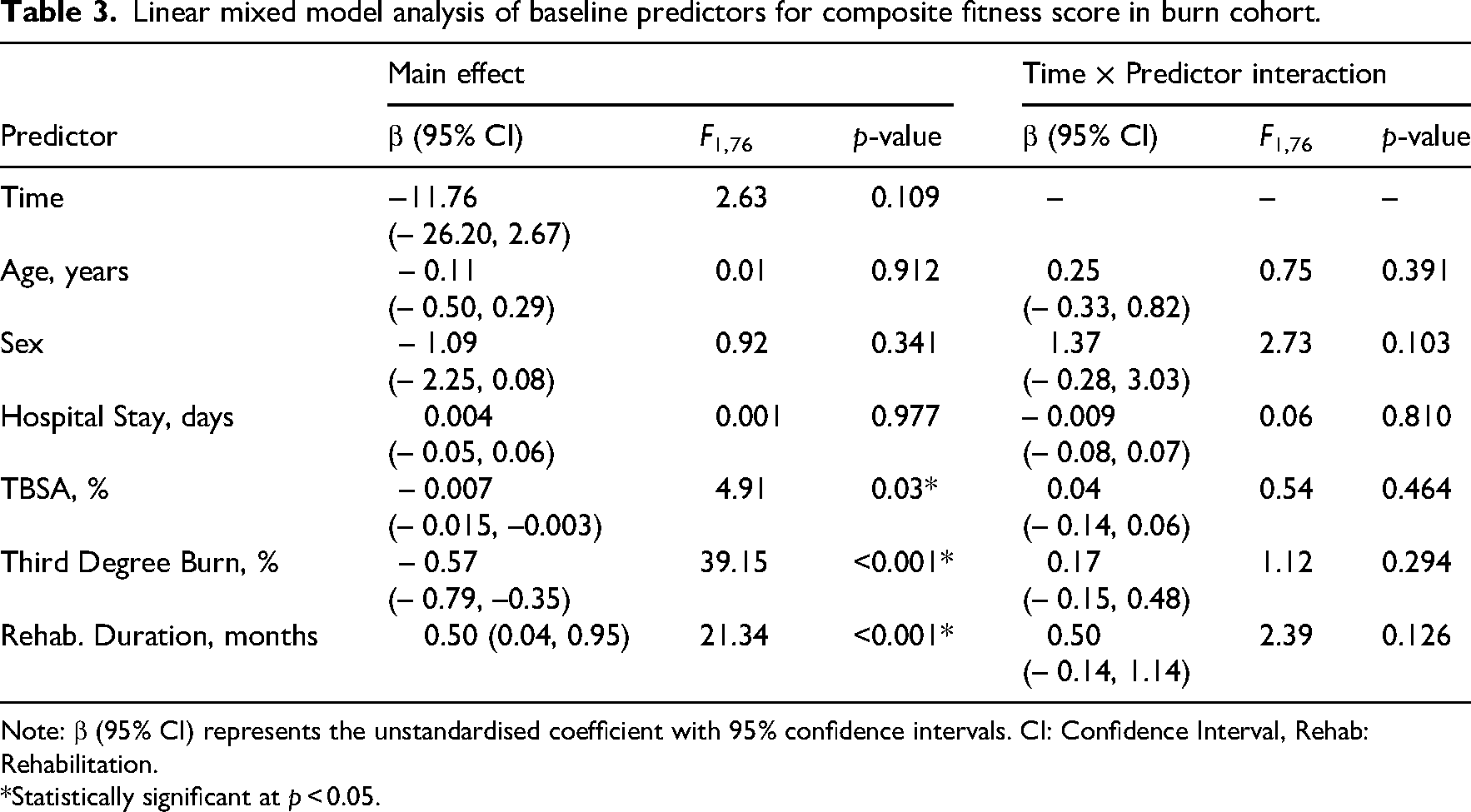
Note: β (95% CI) represents the unstandardised coefficient with 95% confidence intervals. CI: Confidence Interval, Rehab: Rehabilitation.
*Statistically significant at p < 0.05.
Discussion
This study aimed to longitudinally chart the post-discharge recovery of physical fitness in paediatric burn survivors, comparing it to non-injured peers and identifying predictive baseline factors within the burn group. The longitudinal results revealed two distinct trajectories of physical fitness. The burn group exhibited marked improvements across the assessed domains, including balance, agility, muscular strength, power and cardiorespiratory endurance, highlighting the positive effects of time and rehabilitation. Concurrently, the healthy control group demonstrated the anticipated gains associated with normal growth and maturation, showing significant improvement in strength, power and aerobic fitness, with only minor changes in coordination and relatively stable performance in balance and agility. The most salient finding, however, is the comparison at the 2-year endpoint. Despite their considerable gains, the children who had sustained burn injuries did not reach the fitness levels of the healthy control group in any of the assessed components. This indicates that even 2 years post-discharge, a significant, generalised deficit in physical fitness persists in paediatric burn survivors.
In exploring the determinants of physical fitness within the burn survivor group, our findings distinguish between factors that predict a child's overall fitness status versus those that predict their trajectory of change. The severity of the initial burn injury—both in terms of total surface area and depth—emerged as a strong negative predictor, meaning more severe burns were linked to poorer fitness levels throughout the study period. In contrast, the duration of post-discharge rehabilitation was a strong positive predictor, underscoring that more extensive rehabilitation was associated with better overall fitness. Crucially, however, our analysis did not identify any baseline clinical factors that could predict the rate of change in fitness. This implies that the trajectory of improvement over 2 years was not dependent on the initial burn severity, the length of rehabilitation or other demographic factors like age and sex. Furthermore, when fitness was viewed as a composite measure, the patient group as a whole did not show a significant overall improvement from discharge to the 2-year mark, suggesting that the initial fitness deficit established by the injury largely persisted.
Differences in physical fitness between children with burn injuries and healthy peers matched for body mass index, age and sex may persist beyond 2 years after injury. The present findings are consistent with previous research, 10 indicating that this sustained disparity may be partly associated with reduced levels of physical activity in the years following burn injury, potentially related to posttraumatic depression and other psychosocial consequences.20–22 Evidence supporting this persistent functional limitation includes statistically lower muscle strength and cardiorespiratory capacity observed by more than two years post-injury,10,15,23 as well as balance impairments documented at discharge and may persist for up to 5 years. 24 Additional long-term impairments in physical function have also been reported at 2 years post-injury. 25
However, these persistent deficits may not be explained solely by reduced physical activity. They may also be influenced by the post-burn inflammatory response, prolonged hypermetabolism and ongoing catabolic processes, which are particularly concerning in paediatric patients because childhood and adolescence represent critical periods for growth, neuromuscular development and physical maturation.10–12 Consequently, the observed changes in physical fitness may be attributable to the burn injury itself rather than solely reflecting reduced physical activity.
Consistent with our findings, previous studies reported that children with severe burn injuries continued to demonstrate attenuated cardiorespiratory capacity and muscle strength more than 3 years after injury, despite recovery and rehabilitation. 10 Although structured exercise-based interventions can produce substantial improvements in physical activity, functional performance and fitness-related outcomes,26,27 these improvements may be insufficient to restore physical fitness to levels observed in age-matched healthy peers, suggesting that rehabilitation enhances physical fitness but may not fully normalise it.
Exercise-based rehabilitation has been shown to improve muscle strength and cardiopulmonary fitness in children with severe burn injuries; however, these benefits may diminish over time after supervised training ends. Evidence suggests that gains may remain evident up to 1-year post-burn but are substantially reduced by 24 months. 28 This pattern is consistent with youth resistance-training literature showing that strength and power gains decline after detraining, whereas twice-weekly maintenance training may help preserve adaptations. 29 Beyond physical fitness, regular exercise during childhood contributes to bone health, psychosocial well-being, healthy weight regulation and reduced cardiometabolic risk, supporting its value as a long-term component of paediatric post-burn rehabilitation. 30
Our results support a re-evaluation of the current paradigm for paediatric burn rehabilitation. Persistent, multidomain fitness deficits 2 years after injury indicate that traditional short-term rehabilitation programmes, while beneficial, may be insufficient to restore age-appropriate functional norms. Therefore, clinical practice should evolve towards a long-term, developmentally informed model of care that extends beyond hospital discharge. To address complex physical deconditioning, therapeutic interventions should include a comprehensive multidomain training approach integrating strength, power, balance, agility and cardiovascular conditioning. Periodic fitness assessments should also be embedded into long-term follow-up protocols to identify developmental lags early, titrate interventions according to individual needs and optimise outcomes, especially during the adolescent growth spurt. Future research should elucidate the biological, behavioural and psychosocial factors that contribute to persistent fitness deficits after paediatric burn injury, with the aim of designing targeted rehabilitation strategies that minimise long-term morbidity.
Clinical message
Children with burn injuries require sustained engagement in structured rehabilitative exercise beyond hospital discharge to support growth, neuromuscular development and long-term functional outcomes.
Long-term multidomain training integrating strength, power, balance, agility and cardiovascular conditioning may be necessary to optimise physical fitness after paediatric burn injury.
Footnotes
ORCID iDs
Authors’ contribution
All authors contributed equally to the manuscript and read and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data availability statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.