
Abstract
Objectives
This scoping review maps evidence on sex and gender differences in technology-assisted stroke rehabilitation and identifies gaps to inform equitable approaches.
Data sources
Searches were conducted in two rounds (up to March 2025 and April 2025–March 2026) on MEDLINE, CINAHL, Scopus, Web of Science, Cochrane Library, and Google Scholar.
Review methods
Following PRISMA-ScR guidelines, we included primary studies reporting sex and gender outcomes in adults with stroke receiving technological interventions, guided by the PCC framework.
Results
From 7071 records, 11 studies (1626 stroke survivors, 39.9% female) met inclusion criteria. Interventions included robotic exoskeletons, soft robotic gloves, virtual reality, exergaming, functional electrical stimulation, and biofeedback. Five studies found no significant sex differences. However, others reported female advantages in robotic gait training (p = 0.007), functional electrical stimulation (OR = 3.92), soft robotic glove hand function (3.43-fold greater improvement), and Virtual Reality-based balance recovery (p = 0.03). Younger women (<62 years) outperformed men in fine motor tasks, a pattern reversing with age.
Conclusion
Gender and sex disparities in rehabilitation outcomes vary by technology type, underscoring the need for inclusive device designs and improved female representation in trials. Future research must integrate biological and sociocultural perspectives and standardize outcome measures to optimize tailored rehabilitation for all stroke survivors.
Keywords
Introduction
Stroke is a leading cause of death and disability worldwide, with over 7 million deaths and 160 million disability-adjusted life years lost annually. 1 Post-stroke disability, particularly in motor and balance domains, is expected to rise with population ageing.2,3 Technology-based rehabilitation, including robotics, exoskeletons, virtual reality, augmented reality, telerehabilitation, and wearable sensors, offers intensive and adaptive training that supports motor recovery, gait, balance, and upper limb function.4–7 Recent evidence highlights the significant potential for improvement in functional mobility and gait adaptability through these advanced systems. For example, gait adaptation training on an augmented reality treadmill 8 and digital exercise combined with augmented reality training systems 9 have demonstrated substantial benefits in improving mobility and walking performance among patients with stroke. Efficacy, however, depends on matching the right device to the right patient. 10
Sex refers to biological attributes that influence cardiovascular and neurological function, whereas gender encompasses socially constructed roles and behaviors that shape health experiences. 11 Both dimensions affect outcomes: sex determines vulnerability and recovery potential, while gender influences risk exposure, access to care, adherence, and social support. 11
While men have higher incidence rates in midlife for stroke, women, especially postmenopausal, experience poorer outcomes, influenced by biological, psychosocial, and systemic sampling bias factors.12–14 Yet, sex and gender remain under-investigated in rehabilitation research. 15 Male-centered device design may compromise fit or efficacy for women, while virtual therapy and gaming interfaces may engage genders differently, influencing adherence. 16 Similarly, acceptance of home-based wearable technologies may vary by gender. 17
This scoping review maps current evidence on sex and gender differences in technologically assisted stroke rehabilitation, focusing on functional outcomes such as motor recovery, gait, balance, endurance, and upper limb function.
Methods
This scoping review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses for Scoping Reviews. The protocol was prospectively registered on the Open Science Framework (https://doi.org/10.17605/OSF.IO/2EGXB) and structured according to the Population–Concept–Context framework.
Studies were eligible if they included adults (≥18 years) with ischemic or hemorrhagic stroke and reported sex- or gender-based outcomes. The review focused on functional recovery measures: motor recovery, gait, balance, endurance, and upper limb function after technology-based rehabilitation. Eligible interventions included robotics, exoskeletons, virtual reality, telerehabilitation, brain–computer interfaces, neuromodulation, wearable sensors, and haptic feedback. Both clinical and home-based settings were included, whereas secondary literature and studies using only conventional rehabilitation were excluded.
Six databases were searched: MEDLINE, CINAHL, Scopus, Web of Science, Cochrane Library, and Google Scholar for grey literature. No limits on publication year or language were applied. The strategy involved three stages: preliminary searches to identify keywords, refined search strings with Boolean operators applied across all databases, and manual screening of reference lists (full syntax is available in Supplemental material).
All records were imported into Rayyan for deduplication and screening. 18 Two reviewers independently screened titles, abstracts, and full texts; disagreements were resolved with a third reviewer. The study selection process is presented in the PRISMA flow diagram.
Results
The systematic search was conducted in two consecutive rounds: the first up to March 2025 and the second from April 2025 to March 2026. Overall, 7071 records were identified. After duplicate removal, 5735 records were screened by title and abstract, of which 5715 were excluded. Twenty full-text reports were assessed for eligibility. Following exclusion of reports without sex- or gender-stratified analyses and one review article, 11 studies met the inclusion criteria: 10 from the first search and 1 from the second (Figure 1).
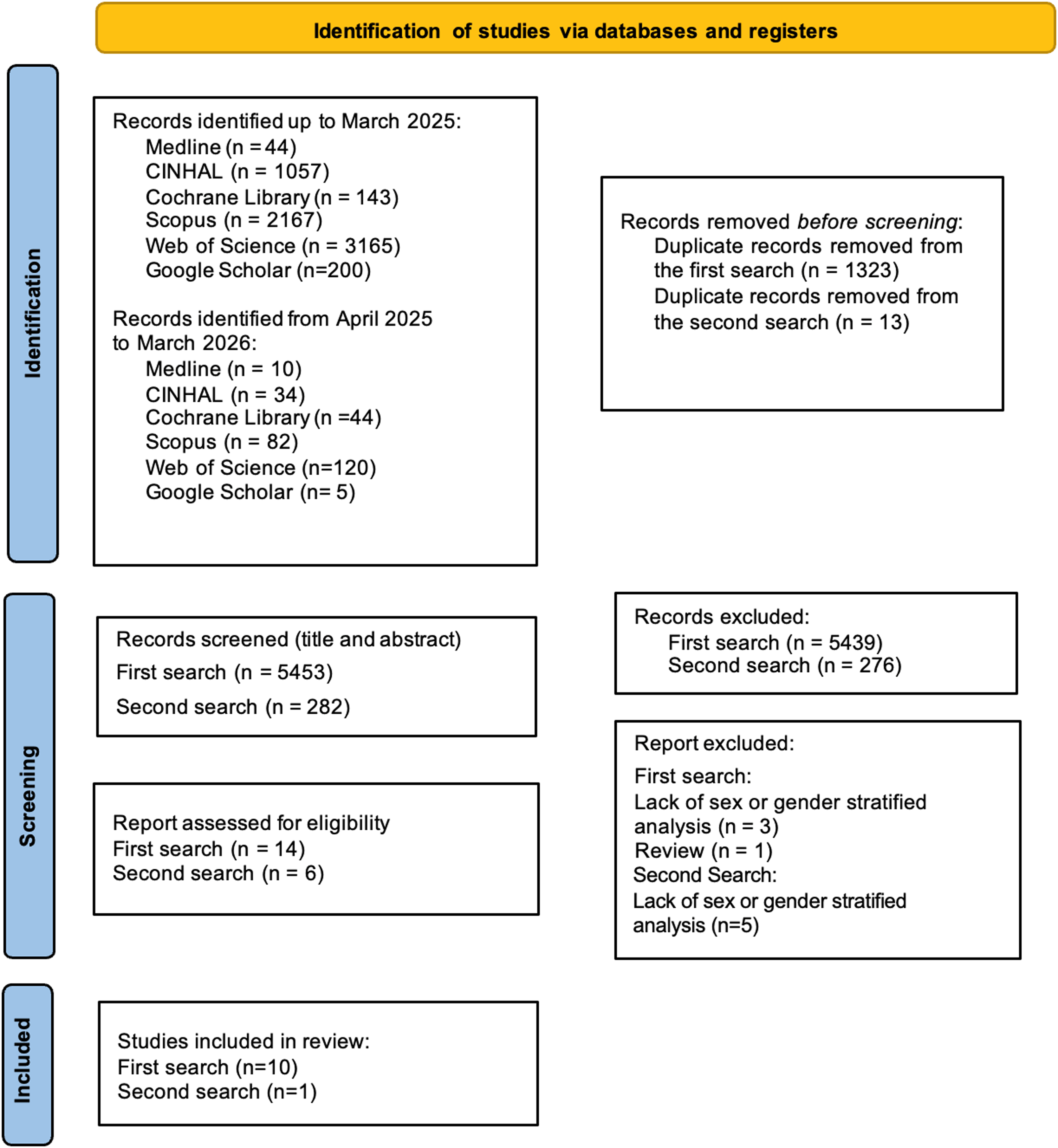
PRISMA-ScR flow diagram.
The included studies, published between 2014 and 2026, were conducted across Italy, Poland, Canada, Russia, Japan, Hungary, and Iraq. Overall, 1626 stroke survivors were enrolled across the 11 studies. Female representation ranged from 32.4% to 47%, with an overall mean of approximately 39.9%. Study designs included randomized controlled trials,19–22 one pseudorandomized trial, 23 retrospective cohorts,24–25 and prospective cohorts.26–29
Participants were predominantly in the subacute phase (eight studies), while chronic stroke populations were investigated in three studies.27–29 Mean age ranged from 51.9 (12.5) years 26 to 66.5 (5.9) years. 23
A broad range of rehabilitation technologies was employed. Robotic systems included InMotion 2.0, 24 KINARM exoskeleton, 29 Lokomat, 21 Gait Trainer GT,19–20 and the ARAMIS exoskeleton. 25 Treadmill-based biofeedback was delivered through Gait Trainer 2, 28 while immersive virtual reality was implemented using the GRAIL system. 26 Functional electrical stimulation with WalkAide was used to improve gait speed. 27 Additional interventions included Xbox 360-based exergaming 23 and a soft robotic glove for upper-limb recovery. 22 All included studies were conducted in clinical rehabilitation settings.
Intervention intensity and duration varied substantially across studies. The number of sessions ranged from 4 29 to 50, 23 with most protocols delivered five times per week. Examples included 20 sessions over 4 weeks (45 min/session) in robotic upper-limb rehabilitation, 24 10 sessions over 2 weeks (90 min/session) for treadmill biofeedback, 28 twice-daily exergaming sessions over 5 weeks, 23 and 8 weeks of soft robotic glove training performed 3–4 times weekly. 22
Primary outcomes mainly focused on motor recovery, including Fugl-Meyer Assessment scores22,24–25,27 and Functional Ambulation Category.19–21 Additional measures assessed activities of daily living, such as the Modified Barthel Index23–24 and Functional Independence Measure,21,26,28–29 as well as gait and balance outcomes, including the 10-meter walk test,27,29 Berg Balance Scale,23,26 and 6-minute walk test.23,26 Psychosocial outcomes, particularly anxiety and depression, were also evaluated in selected studies.23,26
Sex and gender related analyses were reported in all 11 studies, although no study included data on non-binary individuals. Across the evidence base, findings were mixed but suggest a recurring trend toward greater responsiveness among women in selected technology-assisted rehabilitation outcomes. Five studies reported no significant sex differences in their primary outcomes.19,23,25,28–29 However, the remaining studies identified clinically relevant female advantages in specific domains.
Women showed superior gains in robotic gait rehabilitation, 19 greater session-normalized improvements in functional independence after Lokomat training, 21 and a markedly higher likelihood of responding to functional electrical stimulation for gait recovery, with almost fourfold greater odds compared with men. 27 Similarly, immersive virtual reality rehabilitation was associated with better balance recovery in women. 26 In upper-limb rehabilitation, women receiving soft robotic glove therapy demonstrated substantially greater improvements in hand opening rate than men, while no sex-related differences emerged in the control condition. 22
Some findings suggest that the relationship between sex and recovery may be further modified by age. One study reported a significant age by sex interaction in manual dexterity, whereby women younger than 62 years outperformed men, whereas the opposite pattern was observed in older participants. 29 A summary of the included studies is presented in Table 1.
Summary of included studies.
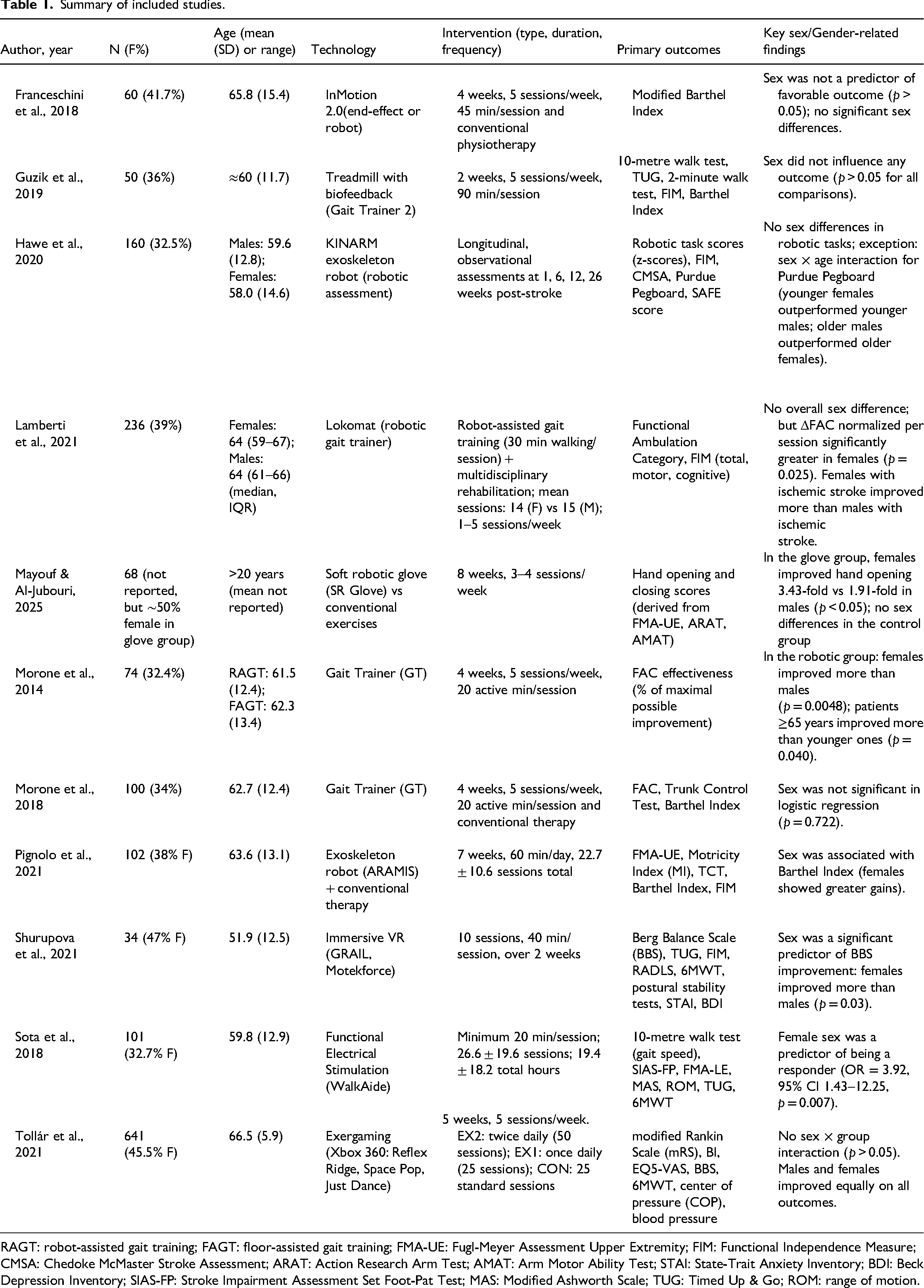
RAGT: robot-assisted gait training; FAGT: floor-assisted gait training; FMA-UE: Fugl-Meyer Assessment Upper Extremity; FIM: Functional Independence Measure; CMSA: Chedoke McMaster Stroke Assessment; ARAT: Action Research Arm Test; AMAT: Arm Motor Ability Test; STAI: State-Trait Anxiety Inventory; BDI: Beck Depression Inventory; SIAS-FP: Stroke Impairment Assessment Set Foot-Pat Test; MAS: Modified Ashworth Scale; TUG: Timed Up & Go; ROM: range of motion.
Discussion
Our findings indicate that female stroke survivors achieved superior gains in several specific interventions, including robotic gait training,19,21 functional electrical stimulation, 27 soft robotic glove hand therapy, 22 and virtual reality-based balance training. 26 In contrast, no sex differences emerged in upper-limb robotics, 24 exergaming, 23 treadmill biofeedback, 28 or exoskeleton path analysis. 25
Several hypotheses from the included studies may help explain why women appeared to benefit more from certain technologies. One such hypothesis relates to hormonal neuroprotection. Hawe et al. 29 observed that women under 62 years outperformed men in fine motor tasks, a pattern that reversed in older age. This finding suggests that estrogen-related neuroplasticity and post-injury protection are more pronounced in premenopausal women. Another hypothesis concerns ischemic stroke pathophysiology. Lamberti 21 and Shurupova 26 reported that female survivors of ischemic stroke responded better to intensive, repetitive training, possibly because of differences in cerebral collateral circulation or inflammatory responses. A further contributing factor may be orientation toward ADLs. Pignolo et al. 25 noted that women showed greater gains in the Barthel Index, which could reflect a higher motivation toward practical autonomy and self-care, thereby translating motor recovery into functional improvement more rapidly.
Moreover, operator bias is reduced when technology is used. Franceschini 24 and Tollár 23 suggested that robotics eliminate unconscious therapist bias, ensuring that women receive the same training intensity as men. Finally, a crucial distinction emerges between impairment and function. Hawe 29 found no sex differences in robotic measures of pure motor impairment, whereas Lamberti 21 and Sota 27 found female advantages in functional outcomes. This divergence suggests that biological recovery alone may not fully explain the observed effects; rather, social roles, behavioral adaptation, caregiving expectations, and the relevance of outcome measures may shape how similar motor gains are translated into everyday function. Prior rehabilitation evidence indicates that women may achieve similar global disability scores yet outperform men in selected self-care and home-relevant domains. 30
Taken together, these hypotheses underscore that sex differences are not merely biological but are shaped by technological design, psychosocial factors, and rehabilitation intensity. Importantly, rigid exoskeletons often incorporate male-biased anthropometrics, which may disadvantage female users. By contrast, adaptive technologies such as exergaming 23 and immersive VR 26 appear more gender neutral. The underrepresentation of women (mean enrolment 39.9%) and the complete exclusion of non-binary individuals limit the generalizability of these findings.
In conclusion, this scoping review demonstrates that sex related differences in technology-based stroke rehabilitation are domain-specific and influenced by biological factors, technological design biases, and sociocultural variables. These findings do not support a sex only stratification model but rather highlight the need for multifactorial, inclusive, and equity-oriented approaches in future research and clinical practice. Standardized reporting of sex and gender disaggregated data, and inclusion of non-binary individuals are strongly recommended.
Clinical messages
• Responses to technology-based stroke rehabilitation may differ by sex and gender, particularly when device characteristics, functional goals, and social context are taken into account.
• Women may achieve greater gains with robotic gait training, functional electrical stimulation, soft robotic gloves, and virtual reality balance interventions.
• More inclusive device design and routine sex and gender disaggregated reporting are essential for clinically applicable evidence.
Supplemental Material
sj-docx-1-cre-10.1177_02692155261462424 - Supplemental material for Sex and gender differences in technology-based rehabilitation for people with stroke: A scoping review
Supplemental material, sj-docx-1-cre-10.1177_02692155261462424 for Sex and gender differences in technology-based rehabilitation for people with stroke: A scoping review by Romina Rahmaniharedasht, Martina Andò, Alex Lando, Nicola Ferri, Valentin Konika, Maria Rosaria Leo, Roberto Piperno, Andrea Turolla, Paolo Pillastrini and Marco Tramontano in Clinical Rehabilitation
Footnotes
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.