
Abstract
Objective
To examine physical activity and its spatial context after geriatric rehabilitation and to identify determinants of out-of-home activity in older adults with cognitive impairment.
Design
Cross-sectional observational study.
Setting
Community, following discharge from geriatric rehabilitation.
Participants
113 geriatric patients (mean age 82.1 ± 6.0 years; 76.1% female) with cognitive impairment following geriatric rehabilitation.
Main Measures
Physical activity was assessed over 48 h using a body-worn accelerometer (PamSys®) and location-based tracking derived from the Global Positioning System (Qstarz BT-Q1000XT). Group differences between participants with and without out-of-home activity were analysed. Multivariable logistic regression identified predictors across physical, psycho-social, cognitive, environmental, financial, and personal domains.
Results
Only 36 (31.9%) of the 113 participants (82.1 ± 6.0 years; 76.1% female) left their homes. Those with out-of-home activity accumulated significantly more daily steps, walking episodes, active time, and less sedentary time than those staying in-home (all p < .01). Receiver operating characteristic analyses identified thresholds of 2140 steps/day (area under the curve 0.81) and 29.6 s mean walking episode duration (area under the curve 0.73) for discriminating between participants with and without out-of-home activity. Physical capacity (OR: 1.30, 95% CI: 1.02–1.65) and cognitive function (OR: 1.29, 95% CI: 1.02–1.62) were independent predictors of out-of-home activity.
Conclusion
Out-of-home activity is infrequent after rehabilitation in older adults with cognitive impairment and closely reflects overall physical activity. It may serve as a practical marker of mobility and highlights the need for targeted interventions to support community mobility during this vulnerable phase.
Introduction
Mobility in older age is a multifaceted construct, shaped by a dynamic interplay of personal, environmental, and contextual factors. 1 It encompasses not only physical activity ‒ defined as any bodily movement that results in energy expenditure ‒ but also spatial expansion, with reference to the concept of life-space. 2 In this context, out-of-home activity ‒ regularly leaving the home for various purposes ‒ is a facilitator for maintaining a physically and socially active lifestyle, 3 and is also associated with substantial physical and mental health benefits. Older adults engaging more frequently in out-of-home activities are at lower risk for nursing home admission 4 and mortality. 5 Furthermore, studies have linked out-of-home activity with higher levels of physical activity across various populations, 6 including older adults. 7 Declining neurological, physical, musculoskeletal, metabolic, and sensory status as part of the ageing process profoundly impacts mobility behaviour. 8 Out-of-home mobility frequently declines in older adults, (partly) leading to an increased focus on in-home activities. 9 This decline can be attributed to the complexity of mobility and the intricate interplay of the different influencing factors. 10 As out-of-home activity requires physical, psychological, and cognitive engagement, it is inherently more demanding than in-home activity. 11 Accordingly, cognitive impairment, which is highly prevalent in geriatric rehabilitation patients, 12 is associated with reduced out-of-home activity,11,13 reduced life-space, 14 and shorter average daily walking time, 15 contributing to the ‘shrinking world phenomenon’ in older adults with cognitive impairment. 16 However, it remains unclear whether the findings apply to older adults with cognitive impairment during the highly vulnerable transition phase following ward-based geriatric rehabilitation, a period marked by substantially increased risks of deconditioning, functional decline, and loss of independence. 17 Importantly, it is unknown whether engaging in out-of-home activity after discharge in this vulnerable population increases physical activity levels or is offset by compensatory rest or inactivity at home as suggested for discussion earlier. 18
The introduction of small, lightweight Global Navigation Satellite System devices, such as Global Positioning System trackers, has substantially improved the objective assessment of out-of-home activity by enabling continuous, non-invasive location tracking of real-world mobility. 19 Combined use of accelerometer and Global Positioning System measures reduces recall bias and enhances data quality compared to self-report and has demonstrated feasibility in community-dwelling adults with cognitive impairment. 20 Despite increasing recognition of mobility metrics as valuable health biomarkers, studies objectively examining determinants of out-of-home activity among adults with cognitive impairment in the critical post-discharge phase remain scarce, although such activity may represent a key marker of overall mobility and health status. Therefore, the present study aims to analyse overall physical activity in relation to spatial location, and to identify determinants of out-of-home activity across personal/biographical, cognitive, physical, psycho-social, environmental and financial domains in adults with cognitive impairment following inpatient rehabilitation.
Methods
Ethical approval for the study was obtained from the Ethics Committee of the Medical Faculty at Heidelberg University (S-252/2015), and the trial was conducted in accordance with the Declaration of Helsinki. We performed a cross-sectional analysis of baseline data from a double-blinded, randomised, placebo-controlled trial designed to improve physical capacity and activity in community-dwelling older adults with cognitive impairment following geriatric rehabilitation (ISRCTN82378327). 21
Participants were recruited consecutively from geriatric rehabilitation wards of a German geriatric hospital between September 2015 and April 2017. Patients with mild to moderate impairment were included in the study. Further inclusion criteria were: age ≥ 65 years; ability to walk at least 4 m without a walking aid; residence within 30 km of the study centre; community-dwelling status (i.e., discharge to the patients’ own home); no terminal disease; no delirium; no language restrictions; and written informed consent.
The data were collected in the participants’ home after discharge from rehabilitation (except for age, sex, and number of comorbidities that were documented from patient charts during inpatient rehabilitation). All interviews and testing procedures were consistently administered by assessors trained in interviewing and testing geriatric patients with cognitive impairment.
Descriptive and potentially associated variables with out-of-home activity were selected according to a comprehensive mobility framework, 1 covering physical, psycho-social, cognitive, environmental, financial, and personal/biographical domains, complemented by health characteristics relevant in clinical populations, as in the present study, life-space mobility and physical activity assessment.
The measures listed below represent the domains examined in this study. Detailed information and references for all instruments and assessment procedures are available in the published study protocol 21 and the Supplementary Material (Table A).
The physical domain was represented by physical capacity as measured with the Short Physical Performance Battery, and data for habitual walking speed (metres/seconds) were extracted from the test battery.
The psycho-social domain was covered by the assessment of the social situation (Assessment of the Social Situation, depressive symptoms (Geriatric Depression Scale), apathetic symptoms (Apathy Evaluation Scale-Clinical Version), fall-related concerns (Short Falls Efficacy Scale-International), and related avoidance behaviour (Fear of Falling Avoidance Behavior Questionnaire).
The cognitive domain was analysed via the Montreal Cognitive Assessment scores.
As environmental factors weather data (temperature and precipitation) during the 48 h measurement period, recorded from the weather station closest to each participant's home, were included (Deutscher Wetterdienst, Climate Data Centre).
To represent the financial domain, a self-reported rating of ‘insufficient’ vs. ‘sufficient’ money available was considered (as part of the Assessment of the Social Situation).
Personal/biographical and health characteristics included age, sex, and number of comorbidities. Other sociocultural and health-related factors encompassed living situation (‘alone’ vs. ‘with others’), marital status (‘married’ vs. ‘not married’), educational level (‘< 8 years’ vs. ‘≥ 8 years’), as well as the self-rated health status (European Quality of Life 5 Dimensions ‒ Visual Analog Scale), falls in the previous year, documented following an established classification, and care related aspects (documented as ‘number of physician appointments’ and ‘duration of outpatient care’ in the past 3 months; based on a questionnaire for the use of medical and non-medical services in old age (‘Questionnaire for Health-Related Resource Use in an Elderly Population’).
The ‘Life-Space Assessment for persons with cognitive impairment’ was included as a questionnaire-based measure of comprehensive mobility. The tool provides a composite score and three subdomains, each accounting for different levels of support (by equipment or human).
Physical activity and Global Positioning System measures were performed over 48 h during weekdays only. To ensure consistency, the time-based results are presented as averages over a 24-h period. Participants were provided with basic information about the application and use of the equipment to enhance compliance and facilitate problem detection.
Physical activity was measured by a small, wearable motion sensor (PAMSys™, BioSensics, Cambridge, MA, USA) fixed at the participant's chest by use of adhesive tape. The sensors were calibrated by the manufacturer before being used in the study. The sensor was worn continuously, day and night. As no adhesive was provided to participants, removal or replacement would have been noticed by the assessors. The PAMSys
Global Positioning System is a satellite-based global navigation system for tracking geolocation data. The Global Positioning System tracking device recorded location (i.e., longitude and latitude coordinates), speed, and heading direction with corresponding time and date stamps. The QStarz (QStarz BT1000X, Qstarz International Co., Ltd, Taipei, Taiwan) is a portable, stand-alone wireless device and able to measure the spatial location of a person. 23 Participants were asked to place the Global Positioning System sensor on their belts or pockets or to wear them as a pendant. Global Positioning System data were uploaded to the ‘Personal Activity Location Measurement System’ (available from: http://ucsd-palms-project.wikispaces.com/.), and saved in formats appropriate for Google Earth (Google, Inc., Mountain View, CA). Data of the Global Positioning System and physical activity sensor were analysed using the ‘Personal Activity Location Measurement System’, which has been validated for processing Global Positioning System and physical activity data. 24 The outcome variable used in the present study was staying (without out-of-home activity) versus leaving-home (with out-of-home activity) as dichotomous measure, verified by visual inspection of Global Positioning System screenshots.
Statistical analysis
Descriptive data included frequencies and percentages, medians and interquartile ranges, or means and standard deviations. Independent-samples t-tests, Mann‒Whitney U-tests, Wilcoxon-tests, and chi-square tests were used to analyse the group differences in descriptive characteristics between those with out-of-home activity and those with in-home activity only. To determine the optimal threshold of daily steps and mean walking duration distinguishing out-of-home from only in-home activity, receiver operating characteristic analyses were performed. The state variable was defined as being outdoors (1 = yes, 0 = no), and daily steps and mean walking duration per episode were entered as the test variables. The area under the curve with 95% confidence intervals was computed to evaluate the discriminative ability of steps to predict out-of-home activity. Optimal cut-off values were determined using Youden's index (J = sensitivity + specificity − 1), with higher values indicating better overall diagnostic performance. Logistic regression modelling was conducted to examine the independent predictors of out-of-home activity. Independent variables for model inclusion to represent all domains of the mobility framework 1 were selected based on statistically significant bivariate correlations (p < .05) using Spearman or point-biserial tests. Variables with non-normally distributed residuals were naturally log-transformed before regression analyses. To avoid multicollinearity, variables with intercorrelations > 0.70 were not included simultaneously. Where multiple variables reflected overlapping constructs or domains, the following prioritisation criteria were applied: (a) conceptual comprehensiveness or clinical relevance of the variable, and (b) the strength of the bivariate association with out-of-home activity. Odds ratios with corresponding 95% confidence intervals were reported to indicate the strength and direction of associations. Model fit was evaluated using Nagelkerke's R2 to represent the proportion of explained variance. Statistical significance was set at p < .05. All analyses were conducted using IBM SPSS Statistics for Windows, Version 29.0.
Results
Out of 1981 patients screened for eligibility, 113 community-dwelling older adults (mean age = 82.1 ± 6.0 years) following geriatric rehabilitation with mild to moderate cognitive impairment (mean score 16.7 ± 2.8), physical impairment (mean score = 5.3 ± 2.3), and multimorbidity (mean number of diagnoses: 11.4 ± 4.4) were included. Daily step counts were low (median 2468; Inter Quartile Range 1115–4056), reflecting the limited mobility. About two-thirds reported a history of fall in the past year (67%). Most participants were women (76.1% female); 50% lived alone, 30% with a spouse, and 20% were supported by a carer permanently residing in their home. Further characteristics are presented in Table 1.
Participant characteristics.
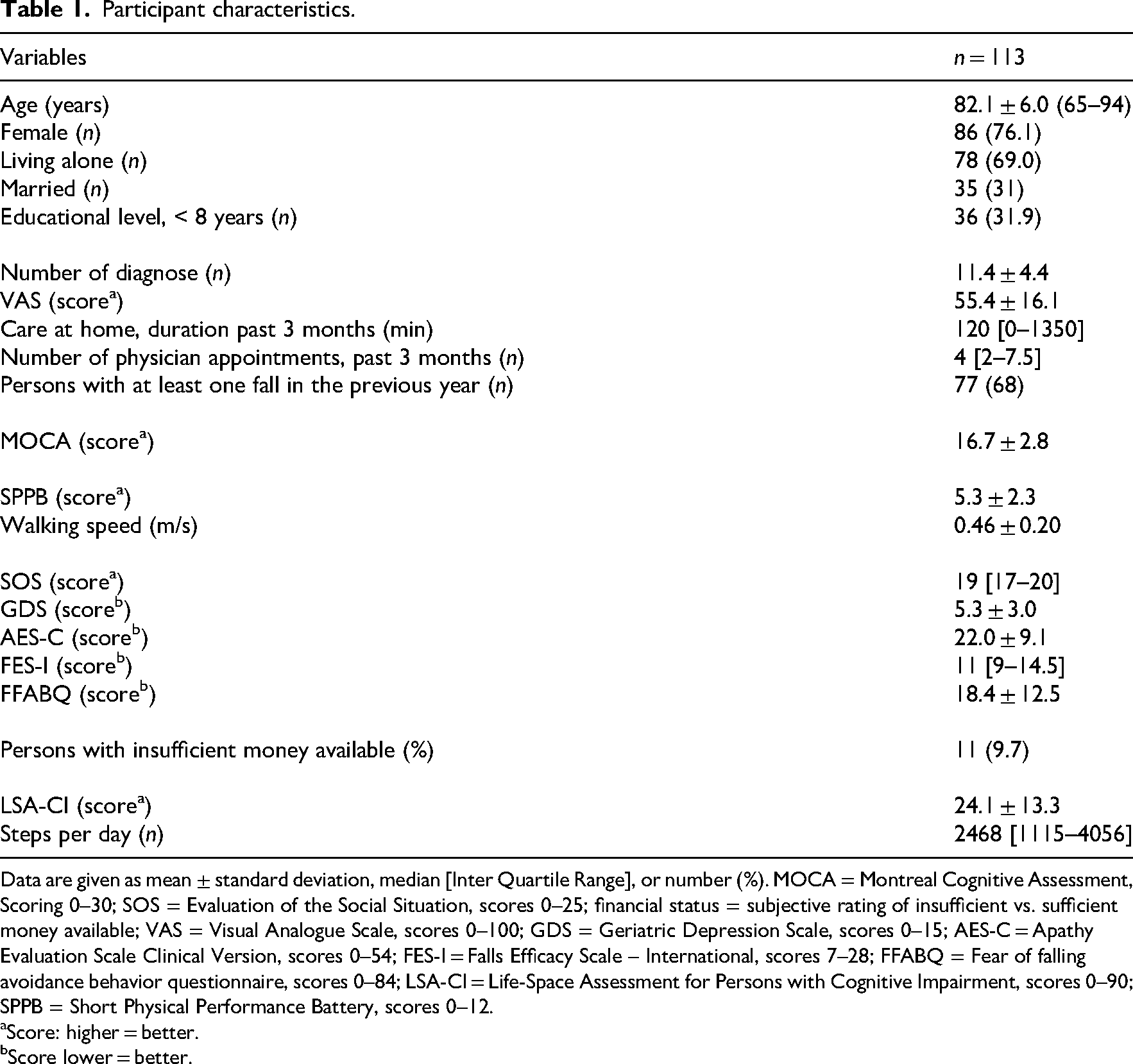
Data are given as mean ± standard deviation, median [Inter Quartile Range], or number (%). MOCA = Montreal Cognitive Assessment, Scoring 0–30; SOS = Evaluation of the Social Situation, scores 0–25; financial status = subjective rating of insufficient vs. sufficient money available; VAS = Visual Analogue Scale, scores 0–100; GDS = Geriatric Depression Scale, scores 0–15; AES-C = Apathy Evaluation Scale Clinical Version, scores 0–54; FES-I = Falls Efficacy Scale – International, scores 7–28; FFABQ = Fear of falling avoidance behavior questionnaire, scores 0–84; LSA-CI = Life-Space Assessment for Persons with Cognitive Impairment, scores 0–90; SPPB = Short Physical Performance Battery, scores 0–12.
Score: higher = better.
Score lower = better.
Differences between participants with and without out-of-home activity
The majority of participants stayed in-home during the measurement period (n = 77; 68.1%) and only one third (n = 36; 31.9%) left their home at all and engaged in out-of-home activity.
Adults with out-of-home activity differed significantly from those who remained in-home across a range of variables (Table 2). These included not only several physical activity measures, but also almost all domains including the physical, psycho-social, cognitive, and personal/biographical domains, as well as health characteristics and life-space mobility.
Differences between persons with and without out-of-home activity.
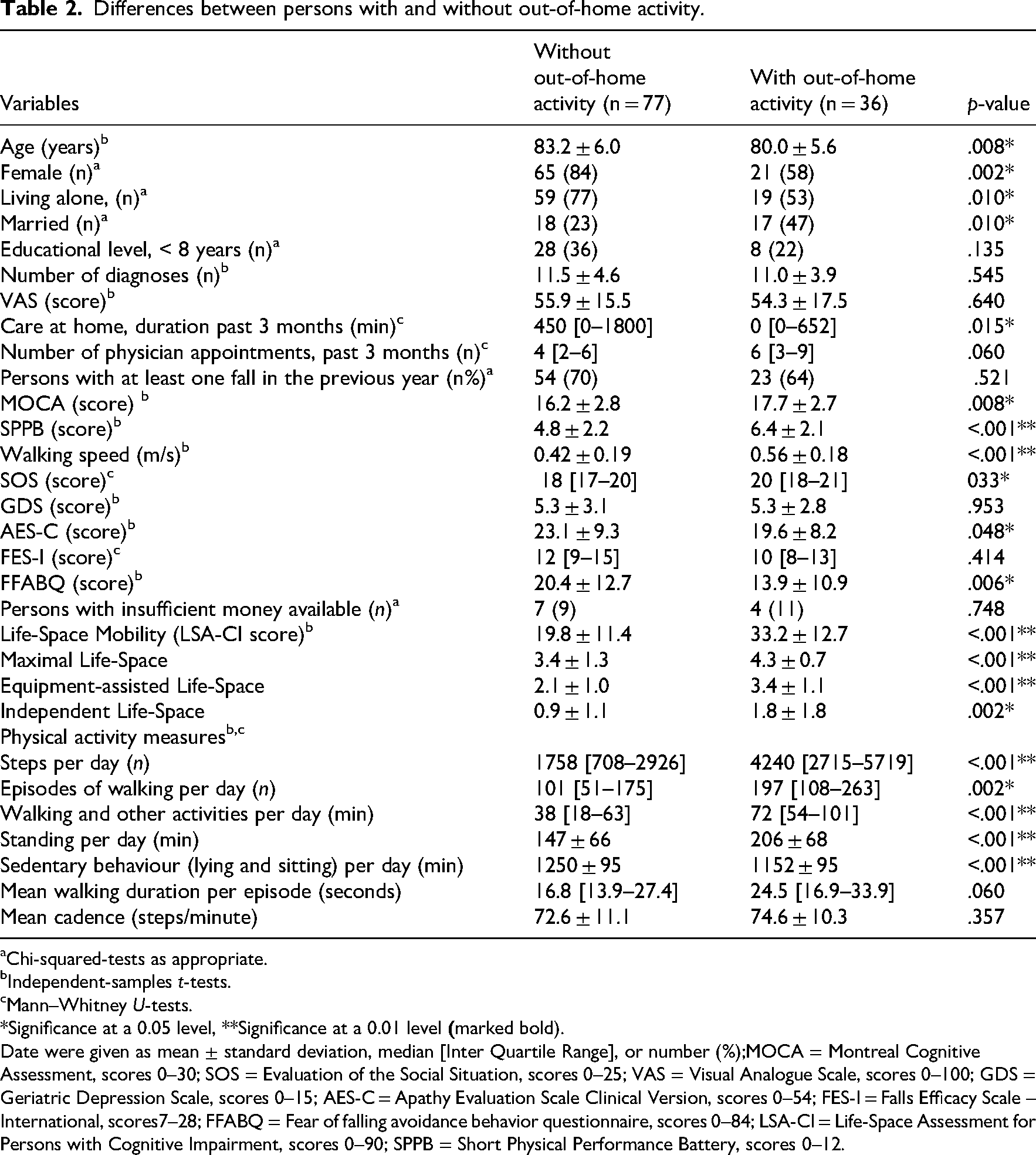
Chi-squared-tests as appropriate.
Independent-samples t-tests.
Mann–Whitney U-tests.
*Significance at a 0.05 level, **Significance at a 0.01 level
Date were given as mean ± standard deviation, median [Inter Quartile Range], or number (%);MOCA = Montreal Cognitive Assessment, scores 0–30; SOS = Evaluation of the Social Situation, scores 0–25; VAS = Visual Analogue Scale, scores 0–100; GDS = Geriatric Depression Scale, scores 0–15; AES-C = Apathy Evaluation Scale Clinical Version, scores 0–54; FES-I = Falls Efficacy Scale – International, scores7–28; FFABQ = Fear of falling avoidance behavior questionnaire, scores 0–84; LSA-CI = Life-Space Assessment for Persons with Cognitive Impairment, scores 0–90; SPPB = Short Physical Performance Battery, scores 0–12.
As expected, adults with out-home activity showed higher levels of physical activity, covering more steps and walking episodes, longer durations of walking, other active behaviour, and standing, and less sedentary behaviour (lying or sitting) (p = .001–.002). In contrast, measures not directly related to activity volume, including mean walking duration per episode and mean cadence, did not differ between participants with and without out-of-home activity. Participants with out-of-home activity also reported a higher subjective mobility, as indicated by higher life-space mobility (mean score 33.2 ± 12.7 vs. 19.8 ± 11.8; p < .001; and subdomains: Maximal life-space (4.3 ± 0.7 vs. 3.4 ± 1.3; p < .001), equipment-assisted life-space (3.4 ± 1.1 vs. 2.1 ± 1.0; p < .001) and independent life-space (1.8 ± 1.8 vs. 0.9 ± 1.1; p = .002)).
Physical capacity in Short Physical Performance Battery score and walking speed (both p < .001), was greater in participants with out-of-home activity, with clinically meaningful between-group differences (Short Physical Performance Battery >1 point; walking speed >0.1 m/s).
Significant group differences emerged for most variables of the psycho-social domain. Participants with out-of-home activity reported a more favorable social situation, less fear of falling-related avoidance behaviour, and fewer apathetic symptoms (p = .002‒.029). No differences were observed for depressive symptoms or concerns about falling.
Cognitive function was significantly higher among those with out-of-home activity (p = .005).
Environmental variables (e.g., mean temperature and precipitation) and financial domain did not differ between the groups (not shown in the table; p = .132‒.497).
In the personal/biographical domain, participants with out-of-home activity were significantly younger, less often female, and more frequently married, while living alone was less common (p = .004‒.011). Indicators of health-related care suggested a better status in this group, including fewer physician appointments (p = .026) and less outpatient care (p = .005) in the past three months. No significant differences were found for educational level, multimorbidity, self-rated health status, or fall history.
A Receiver Operating Curve analysis identified the optimal cut-off for steps predicting out-of-home activity. The area under the curve was 0.81 (95% CI: 0.74–0.88), indicating good discrimination. The optimal threshold of 2140 steps/day yielded a sensitivity of 0.92 and a specificity of 0.38 (Supplemental Figure A). When evaluating walking pattern rather than volume, a second Receiver Operating Curve analysis identified an optimal mean walking duration cut-off of 29.6 s (sensitivity: 0.94, specificity: 0.58). The area under the curve was 0.73 (95% CI: 0.63–0.83), reflecting acceptable discrimination (Supplemental Figure B).
Determinants of out-of-home activity
Correlational Spearman and point-biserial analyses revealed many associated variables out of the domains outlined by Webber et al. 1 with out-of-home activity (Supplemental Table B), serving as a basis for selecting independent variables for the regression analysis. The subsequent logistic regression model revealed only higher cognitive function (OR: 95% 1.24; CI: 1.02–1.50) and physical capacity (Short Physical Performance Battery OR: 95% 1.30; CI: 1.02–1.66; Table 3) to be independently predictive of out-of-home activity. The model demonstrated a significant fit to the data (χ28 = 38.738, p < .001), with a Nagelkerke R2 of 0.407, indicating that the model explained 40.7% of the variance in the outcome variable.
Logistic regression analysis for out-of-home activity.
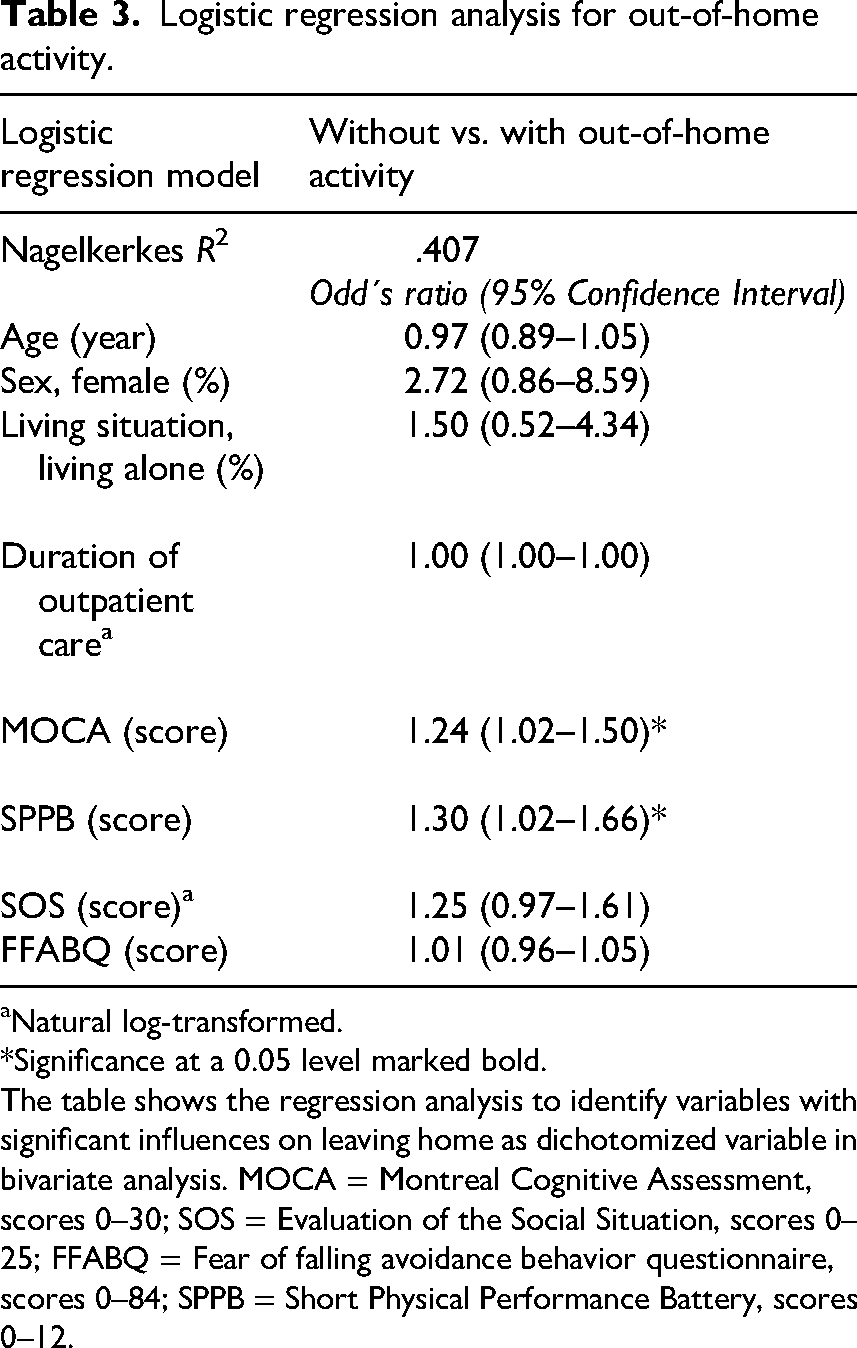
Natural log-transformed.
*Significance at a 0.05 level marked bold.
The table shows the regression analysis to identify variables with significant influences on leaving home as dichotomized variable in bivariate analysis. MOCA = Montreal Cognitive Assessment, scores 0–30; SOS = Evaluation of the Social Situation, scores 0–25; FFABQ = Fear of falling avoidance behavior questionnaire, scores 0–84; SPPB = Short Physical Performance Battery, scores 0–12.
Discussion
The present study provides a comprehensive comparison of multimorbid older adults with and without out-of-home activity following geriatric rehabilitation and identifies key determinants of out-of-home activity among persons with cognitive impairment. The findings reveal a markedly restricted mobility profile, with more than two-thirds of participants remaining exclusively at home, exceeding prevalence rates reported in previous studies of older populations. 13 This highlights a pronounced risk of a ‘shrinking world’ in this particularly vulnerable group, 16 likely driven by the accumulation of physical, cognitive, and psycho-social limitations.
Participants engaging in out-of-home activity demonstrated consistently higher activity levels across multiple dimensions, including step counts, walking episodes and duration, other active behaviour, standing time, and life-space mobility. Importantly, greater out-of-home activity was not compensated by reduction in in-home activity, suggesting that individuals remaining at home are not reallocating activity indoors but are instead constrained by limited physical capacity, exhaustion, or reduced energy. 25 These findings are consistent with previous studies in community-dwelling older adults, 6 including those with cognitive impairment but not undergoing post-rehabilitation transition, 7 and underline out-of-home activity as a marker of overall mobility rather than simple displacement of activity location.
Out-of-home activity was strongly associated with physical capacity, reflected by a clinically meaningful 1.6-point difference in Short Physical Performance Battery scores. 26 Physical and cognitive limitations are known to interact and may form a ‘vicious cycle’ accelerating functional decline and loss of independence. 27 In line with this, cognitive performance was lower among participants who remained homebound, consistent with previous findings in less vulnerable older adults with cognitive impairment. 28 Progressing cognitive deficits, particularly impairments in executive function, memory, and spatial navigation, likely limit planning abilities and reduce engagement in complex behaviours such as out-of-home activity. 29 In the present study, among psycho-social factors, apathetic symptoms were more prevalent in those staying at home, supporting apathy, alongside cognitive impairment, as a relevant barrier to out-of-home activity. 14 In contrast, depressive symptoms did not differ significantly between groups, possibly reflecting the presence of meaningful in-home activities or social interactions that buffer mood despite reduced participation. Fear-of-falling-related avoidance behaviour, but not fall-related self-efficacy, was higher among homebound participants, suggesting that avoidance tendencies may more directly capture restrictions in out-of-home activity than self-efficacy measures. This emphasises the need to address motivational and behavioural avoidance in addition to physical capacity and self-efficacy.11,29
Sociodemographic and environmental findings were largely consistent with previous literature. Older age and female sex were associated with staying home more frequently.9,30 Living with others and a better social situation were linked to higher out-of-home activity, highlighting the importance of the immediate social environment and support, in line with previous research that identifies social isolation as a major barrier to mobility.10,30 No differences were observed for financial sufficiency or weather conditions, likely reflecting the region's relatively homogeneous socioeconomic context and moderate climate. Increased healthcare use and support among homebound participants aligns with prior findings on growing dependency with increasing physical and cognitive impairment.31,32 Notably, multimorbidity and self-rated health did not differ between groups, reinforcing the importance of functional limitations over disease counts, as emphasised by the World Health Organisation's International Classification of Functioning, Disability and Health framework. 33
Receiver operating characteristic analysis identified a threshold of 2140 steps/day with good discriminative performance, high sensitivity, and low specificity, indicating suitability for screening rather than diagnostic purposes. These findings correspond with prior work linking daily step counts to life-space mobility in cognitively intact older adults 34 and support step count as a quantitative mobility indicator. Beyond activity volume, walking pattern characteristics also showed discriminative potential. A mean walking episode duration threshold of 29.6 s showed acceptable discrimination, suggesting that the pattern of walking behaviour may contribute meaningful contextual information beyond overall activity quantity. This aligns with prior work emphasising the relevance of everyday walking pattern characteristics in older adults. 35 Longer uninterrupted walking episodes may reflect mobility patterns more commonly associated with activity across broader environments and greater spatial navigation demands, whereas shorter and more fragmented walking episodes may characterise more restricted mobility behaviour. Thus, walking episode duration may provide an ecologically relevant indicator of functional mobility pattern in everyday life. Importantly, distinguishing between out-of-home and in-home activity may provide a more contextually meaningful characterisation of mobility behaviour, as out-of-home activity has been associated with higher physical capacity,1,6,7 better cognitive function, 4 and greater social engagement.1,3 The present study extends these findings to a highly vulnerable population, supporting out-of-home activity as a simple, multidimensional marker of mobility and vulnerability.
Among a broad range of potential determinants, as indicated by univariate associations to physical activity, only two major predictors were identified: physical capacity emerged as the most consistent determinant of out-of-home activity, in line with previous research, 10 highlighting its role as a prerequisite for real-life mobility. Cognitive status also remained as an independent determinant, consistent with findings in cognitively unimpaired adults, 36 and reinforcing the complexity of out-of-home activity compared to in-home activity. 11 Evidence from prior studies supports the feasibility of improving physical capacity even in comparable vulnerable populations,37–39 underscoring its relevance as a modifiable intervention target.
A key limitation of this study is the 48-h sensor monitoring period. Out-of-home activity may have been misclassified, as rare excursions could be missed, while a single event could lead to overestimation. Although short-term monitoring captures certain activity metrics reliably, 40 longer wear periods (e.g., five days) may improve reliability. Additionally, as the location tracking sensor was not body-worn, non-compliance cannot be fully excluded. Although several steps were implemented to minimise this risk, including clear placement instructions, repeated reminders, and a follow-up visit after 24 h, non-compliance of body-worn sensors cannot be fully excluded.
Overall, the findings highlight out-of-home activity as a multidimensional indicator of mobility, health, and autonomy in older adults with physical and cognitive impairment following geriatric rehabilitation. Whether assessed by sensor-based methods or a simple single-item question, out-of-home activity may offer a pragmatic and scalable approach for risk stratification and targeted intervention. The high prevalence of homebound individuals underscores the need for tailored strategies to support out-of-home mobility.
41
Determinant analyses suggest intervention targets at multiple levels, including physical training,21,39 cognitive training,
42
and support for driving or alternative transportation.
43
Multimodal approaches may be particularly effective in mitigating mobility restrictions, reducing dependency, and preventing institutionalisation, especially among cognitively impaired adults who remain underserved by post-acute and intersectoral rehabilitation pathways despite retaining substantial rehabilitation potential.38,44
Out-of-home activity is infrequent in older adults with cognitive impairment after rehabilitation, highlighting a critical period of mobility vulnerability. Sensor-derived activity metrics clearly distinguish adults who leave the home from those who remain indoors. Physical capacity and cognitive function independently predict out-of-home activity this vulnerable, multimorbid population.Clinical messages
Supplemental Material
sj-docx-1-cre-10.1177_02692155261462457 - Supplemental material for Determinants of out-of-home activity in older adults with cognitive impairment following inpatient rehabilitation: A secondary cross-sectional analysis of a randomised controlled trial using location-based and accelerometer-derived measures
Supplemental material, sj-docx-1-cre-10.1177_02692155261462457 for Determinants of out-of-home activity in older adults with cognitive impairment following inpatient rehabilitation: A secondary cross-sectional analysis of a randomised controlled trial using location-based and accelerometer-derived measures by Phoebe Ullrich, Theresa Buchner, Martin Bongartz, Tobias Eckert, Carl-Philipp Jansen, Jürgen M. Bauer, Christian Werner and Klaus Hauer in Clinical Rehabilitation
Footnotes
Acknowledgements
We thank all individuals who contributed to this study, including the participants.
Ethical approval
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors gratefully acknowledge funding from the social and private long-term care insurance (soziale und private Pflegeversicherung) and the Municipal Association for Youth and Social Affairs in Baden-Württemberg (Kommunalverband für Jugend und Soziales Baden-Württemberg) (grant number 80221-208-009-01-01).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Informed consent statement
Written informed consent by the participants was obtained.
Authors’ contributions
Phoebe Ullrich: conceptualization, data curation, formal analysis, investigation, methodology, validation, writing–original draft, and writing–review and editing.
Theresa Buchner: writing–review and editing
Martin Bongartz: data curation, writing–review and editing
Tobias Eckert: data curation, writing–review and editing
Carl-Philipp Jansen: writing–review and editing
Jürgen M. Bauer: resources, supervision, writing–review and editing
Christian Werner: writing–review and editing
Klaus Hauer: conceptualization, funding acquisition, investigation, methodology, supervision, validation, writing–review and editing.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.