
Abstract
Objective
To investigate if post-discharge oral nutritional supplementation improves physical functional performance and other outcomes in older hip fracture patients at nutritional risk.
Setting
Department of Orthopaedic Surgery, Copenhagen University Hospital – Herlev and Gentofte, Herlev, Denmark.
Participants
Hip fracture patients aged ≥65 years and identified as being at nutritional risk. Of 768 individuals screened, 123 were randomised and 109 (89%) completed the 12-week follow-up.
Intervention
Participants were randomised to receive either two cans of high energy, high protein oral nutritional supplementation enriched with vitamin D and omega 3 fatty acids daily for 12 weeks after discharge or standard care.
Main measures
The primary outcome was physical functional performance assessed by the 30-s chair-stand test. Secondary outcomes included muscle mass, hand grip strength, activities of daily living, hydration status, inflammation, appetite, quality of life, energy and protein intake, and omega-3 fatty acid status.
Results
Physical functional performance improved in both groups, with no significant between-group difference in the number of repetitions performed in the intention-to-treat analysis. Protein intake increased in the intervention group (p = 0.003), while no between-group differences were observed for other outcomes. In the per-protocol analysis, the intervention group showed greater improvement in physical functional performance compared with the control group (p = 0.040). Energy and protein intake were also higher in the intervention group (p = 0.003, p = <.001),
Conclusions
Post-discharge oral nutritional supplementation increased protein intake but did not improve physical functional performance. Per-protocol findings suggest that high adherence may be necessary to achieve functional benefits.
Introduction
Hip fractures are among the most serious and prevalent injuries affecting older adults. In Denmark, 7400 hip fractures were registered among individuals aged 65 years or older in 2023, corresponding to an incidence of six per 1000. 1 As global life expectancy continues to rise, the incidence of hip fractures is expected to increase significantly, posing growing challenges to healthcare systems worldwide. 2 Sustaining a hip fracture leads to hospitalisation, functional limitations, and a decline in muscle mass and physical functional performance, significantly affecting both immediate and long-term health outcomes. 2 Recovery after hip fracture remains limited for many patients, and only 40–60% of older adults regain their pre-fracture activities of daily living, and many experience reduced survival, post-operative complications and reduced quality of life.3–7
Nutritional status plays a critical role in recovery following hip fracture. Malnutrition and inadequate protein and energy intake are common in this population, and are associated with impaired functional recovery, reduced quality of life, increased risk of readmissions and decreased survival. 8
Addressing malnutrition through adequate energy, protein and essential micronutrients intake may enhance recovery, including physical functional performance during rehabilitation. 4 While oral nutritional supplements are recommended to support rehabilitation, existing evidence in this target population is inconsistent and largely outdated. Many studies were conducted before the implementation of fast-track surgical pathways and enhanced recovery after surgery protocols, resulting in early discharge that characterises modern hip fracture care.9–11 Recent systematic reviews have highlighted methodological limitations in the literature, including short intervention periods, and limited focus on clinically relevant outcomes such as, physical functional performance, functional limitations and quality of life.9,10
This randomised controlled trial builds on a prior feasibility study. The primary objective was to investigate if post-discharge oral nutritional supplementation improves physical functional performance in older hip fracture patients at nutritional risk. Secondary objectives included effects on functional limitation, muscle strength, quality of life and muscle mass.
Methods
Ethics considerations and consent to participate
The study has been approved by The Danish Regional Ethics Committee of the Capital Region (Journal No.: H-21064554) and the Danish Data Protection Agency (P-2022-293). Eligible patients received both written and oral information before signing an informed consent form. During the trial, the Ethical Committee accepted a protocol amendment approving the measurement of hydration status at follow-up.
Trial design and participants
The trial was a single-site, open-label, parallel-group randomised controlled trial with two arms. An overview of the trial design is presented in Figure 1. The study was designed to test superiority of the intervention compared to standard care. All outcomes were collected by study investigators, and standard operational procedures for each assessment were prepared in advance, to ensure consistency in data collection. Blinding was not feasible for participants, care providers or outcome assessors; only the data analysts conducting the statistical analyses were blinded to group allocation. The study is reported in accordance with the CONSORT guidelines for randomised trials. 13
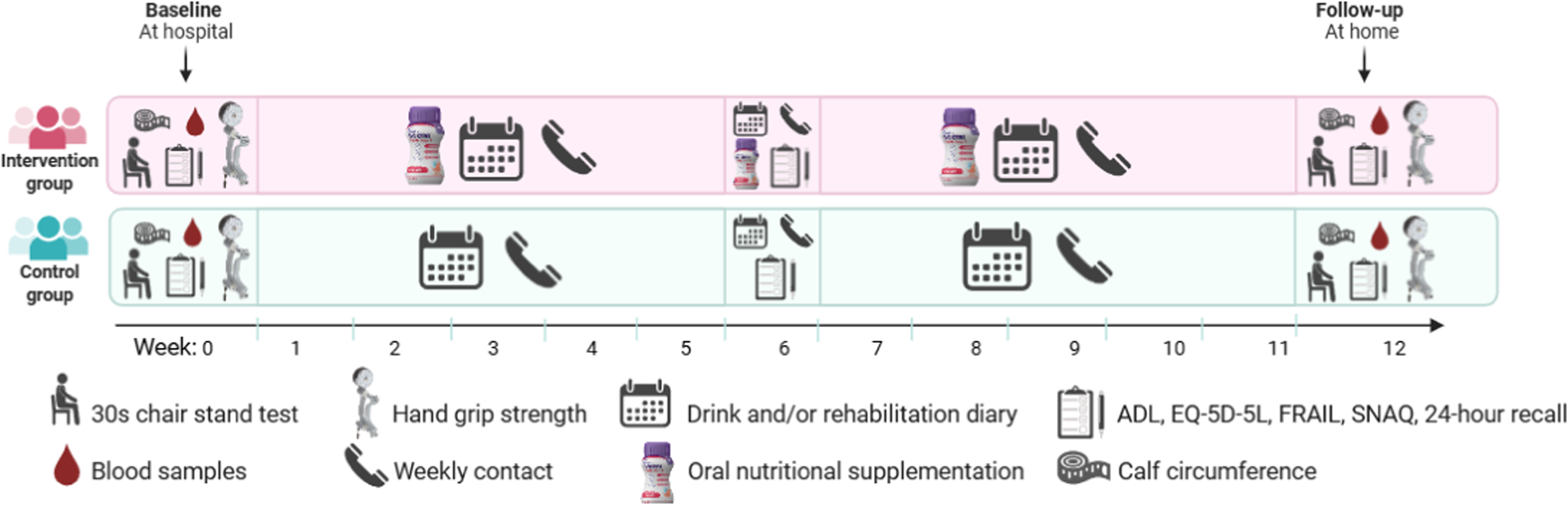
Overview of trial design. Abbreviations: ADL: activities of daily living; EQ-5D-5L: The European Quality of Llife-5 Dimensions-5 Levels; SNAQ: Simplified Nutritional Appetite Questionnaire. Reproduced from Jensen et al. 12
Eligible participants were 65 years or older at nutritional risk according to the Nutritional Risk Screening 2002, 14 admitted with a hip fracture to the Department of Orthopaedic surgery and expected to be discharged with a rehabilitation plan. Hip fracture types included femoral neck fracture, pertrochanteric fracture, subtrochanteric fracture, sequela of fracture of femur or distal femur fractures. Exclusion criteria were active cancer, renal inefficiency (eGFR < 27, mL/min/1.73 m2), cognitive impairment preventing informed consent, terminal illness, exclusive reliance on texture-modified food, allergies to milk or fish, enteral or parenteral nutrition, intention to lose weight or go on a special diet, current use of fish oil supplements for medical reasons such as hypertriglyceridemia, unwillingness to discontinue fish-oil supplements during the trial period or inability to understand or speak Danish. Cognitive status was systematically approached via existing diagnoses of Alzheimer's or dementia in the Danish Health Informatics platform. Prescription of other oral nutritional supplementation at discharge was not an exclusion criterion. Participants in the intervention group who were prescribed additional oral nutritional supplementation were instructed to prioritise the study-provided oral nutritional supplementation. In the control group, any prescription for oral nutritional supplementation was recorded.
Primary screening was done through a daily inventory of patients 65 years or older admitted with a hip fracture to the orthopaedic surgical ward using the Health Informatics platform. Secondary screening and initial contact were carried out by clinical dietitians assigned to the ward. Eligible patients received written and oral study information from a member of the research staff before signing an informed consent form.
Randomisation
Participants were randomised in block sizes of 2, 4, 6 and 8 by computer-generated randomisation sequence in a 1:1 allocation ratio. Allocation concealment was ensured by an impartial staff member with no clinical involvement in the trial, who prepared the allocation sequence and the sealed envelopes. A total of 130 envelopes containing the group allocated, A or B, were prepared. Concealment was ensured by wrapping the allocation paper in aluminium foil to render the envelopes impermeable to intense light. The envelopes were stored in a locked cupboard in a locked room, only accessible to research staff. After completion of baseline assessments, the subsequent envelope was delivered to the participant by research staff to reveal the designated allocation.
Intervention and control
The intervention group was provided with the study oral nutritional supplementation which should be ingested from the first day of discharge from the hospital and continued for 12 weeks. Details about the nutritional content can be found in Table 1. The study oral nutritional supplements were high-protein and enriched with essential micronutrients including vitamin D, both expected to have a beneficial effect on physical functional performance. 15 Further, the study oral nutritional supplementation contained essential fatty acids expected to have a beneficial effect on the degree of inflammation by lowering it and hence improve appetite. 16 Two different flavours of the study oral nutritional supplementation (Cool Berry or Cool Mango Peach) were available and provided free of charge. Before discharge, the participants received counselling by research staff to drink a total of 250 mL per day corresponding to two cans, one in the morning and one in the evening. Participants were also provided with written material on serving recommendations and the importance of protein intake. At discharge, the participants were given a one-week supply of S-ONS. During the 12-week intervention period, study oral nutritional supplements were delivered to the participants’ home twice and adjustments in flavour preferences were based on feed-back from the participants (see details below).
Nutritional content in the study oral nutritional supplementation.
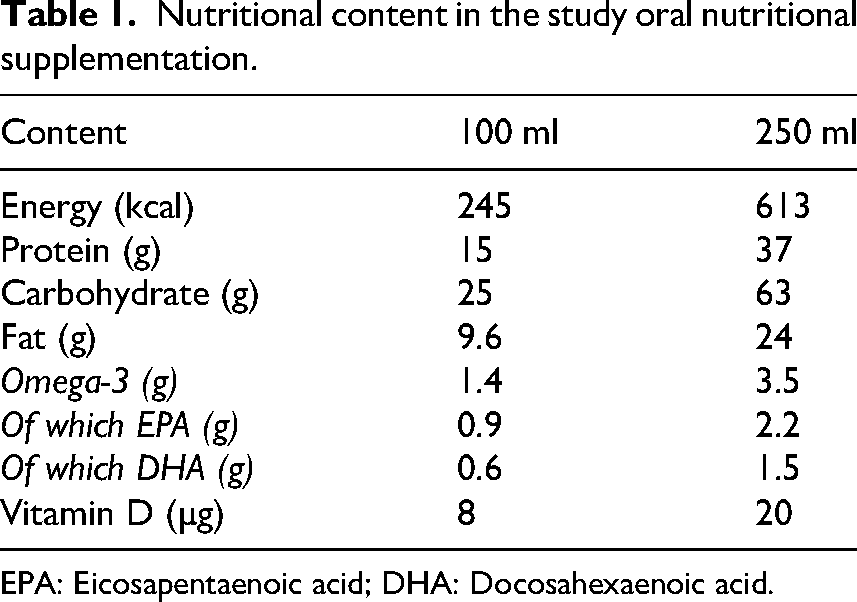
EPA: Eicosapentaenoic acid; DHA: Docosahexaenoic acid.
After discharge, intake of study oral nutritional supplementation was recorded using a daily drink diary. Participants registered the proportion of each prescribed can consumed per day (0%, 25%, 50%, 75% or 100%). The staff at the rehabilitation centres helped to record the intake, if the participants were not able to document it themselves. Research staff conducted weekly phone calls to remind participants to consume the supplement and complete the diary. Participants were provided with a brochure to record any potential side-effect related to the supplement. Side-effects mentioned during weekly phone calls were also documented by the research staff. The control group was provided with standard care, which in most cases do not include a provision or prescription of oral nutritional supplementation at discharge.
All participants were discharged with a rehabilitation plan, consistent with standard care and the trial's inclusion criteria. Rehabilitation was initiated in the municipalities as part of the established care pathway for hip fracture patients. During weekly phone calls, study investigators monitored rehabilitation progress and reminded participants to record their activities in a rehabilitation diary.
Baseline characteristics
Data regarding age, gender, height, weight, BMI, diagnosis, albumin, American Society of Anaesthesiologists physical status classification (ASA score) and length of hospital stay were collected at baseline.
Outcomes and measurements
All outcomes and measurements were assessed through validated measures often used in former nutritional intervention studies among older adults and identified as critical in a recent Delphi consensus and are suggested as core outcomes for nutritional intervention studies in older adults who are malnourished or at risk of malnutrition. 17 Outcomes and measurements were collected by research staff at baseline and 12-week follow-up. Dietary intake assessed by 24-h recall was collected at follow-up only, whereas activities of daily living and quality of life were additionally assessed at 6 weeks. When feasible, the same researcher conducted both the baseline and follow-up assessments.
Physical functional performance (the primary outcome) was assessed using the 30-s chair stand test. Participants performed as many full stands as possible within 30 s, sitting between each stand. The standard version required arms folded across the chest. Participants were instructed to perform both the standard version and a modified version, allowing use of armrests. Results were recorded for both versions. Participants unable to perform the test scored zero. Results were reported as number of repetitions, and categorised as normal, decreased, or highly decreased.18,19 The proportion completing the standard version and the proportion improving their test score were recording. It was considered an improvement if the test score for either the standard or modified version were higher, or if they performed modified at baseline but were able to perform the standard version at follow-up. The cut-off for having decreased physical functional performance was based on the Danish reference values according to sex and age. 20
Muscle strength was measured through hand grip strength, measured in kg, and was used as a proxy for upper-body muscle strength. Hand grip strength of the dominant hand was assessed using a Saehan DHD-1 Digital Hand Dynamometer following a standardised protocol. 20 The test was performed three times with 15-s breaks, and the highest value was recorded. Results were reported in kilograms and categorised and reported as proportion with normal, decreased, and highly decreased hand grip strength. The cut-off for having decreased hand grip strength was based on Danish reference values according to sex and age. 20 Functional limitations were measured using the Functional Recovery Score, a self-reported questionnaire assessing their pre-fracture function (at baseline) and current function (at 12-week follow-up). Outcomes included Activities of Daily Living (total score 0–100), divided as Basal Activities of Daily Living (score 0–44), Instrumental Activities of Daily Living (score 0–23) and Mobility (0–33) scores. The highest score reflects complete independence. The proportion of participants who regained pre-fracture function was also reported, defined as regaining 100% or more of their pre-fracture Functional Recovery Score. Health-related quality of life was measured using The European Quality of Life-5 Dimensions-5 Levels (EQ-5D-5L), 21 including five dimensions (mobility, self-care, usual activities, pain/discomfort and anxiety/depression). Responses were scored on five levels from no problems to extreme problems and converted into an index score (utility) based on Danish population norms (−0.757 to 1.000).22,23 A visual analogue scale (EQ-VAS) records self-rated health from 0 (worst) to 100 (best). Participants who died during the study were given a score of 0 according to the instructions. 21 Permission to use the tool was given by the EuroQol organisation. Results were reported as index and visual analogue scale scores. Energy, protein and fluid intake were assessed at the 12-week follow-up via 24-h dietary recall. Participants reported a typical day's intake, with focus on the intake of oral nutritional supplements, in the intervention group. Portion sizes were estimated using a picture chart, 24 and intake was calculated using the Danish Food Database © 2025 VITAKOST. Results included total energy (kcal), protein (g) and fluid (L) intake. Results for kcal pr. kilogram and protein pr. kilograms were also recorded. Frailty was with the FRAIL scale 25 covering fatigue, resistance, ambulation, illness and weight loss. Scores range 0–5, with 3–5 indicating frailty, 1–2 pre-frailty and 0 robustness. Results were reported as the number of participants classified as frail, pre-frail and not-frail. Appetite was assessed using the Simplified Nutritional Appetite Questionnaire (SNAQ), 26 which includes four items on appetite, taste, satiety and meal frequency, each scored 1–5 (total 4–20). A score ≤ 14 indicates risk of 5–10% weight loss. 26 Results were reported as total scores and proportions scoring ≤ 14. Biomarkers were collected from blood samples (non-fasting venous) to measure vitamin D (25-OH), albumin, sodium, potassium, glucose, urea and C-reactive protein. Simple hyperosmolar dehydration was calculated as 1.86 × (Na+ + K+) + 1.15 × glucose + urea + 14, with ≥295 mOsm/L indicating dehydration. 4 C-reactive protein was used to evaluate the level of inflammation, with a cut-off set at >30 to indicate increased inflammation. The proportion of participants with inflammation was documented. The lowest value possible to measure through the laboratory analysis was 4 mg/L. Vitamin D deficiency was defined as < 30 nmol/L. 27 Omega-3 status was assessed via finger-prick, providing the omega-3 index, omega-6/omega-3 ratio and Eicosapentaenoic acid and Docosahexaenoic acid content. Muscle mass was estimated by measuring calf circumference on the non-operated leg. Calf circumference values <33 cm for men and <32 cm for women were classified as low skeletal muscle mass.28,29 Measurements were obtained at the point of maximal calf circumference with the participant seated (or in bed if necessary), avoiding compression of the skin. 30 The largest value from repeated measurements was recorded. Results were reported as median calf circumference, in cm and the number of participants with normal or low muscle mass. Mortality and readmissions were documented as the number of events at 30 days and 38 weeks after hospital discharge. Admission to the emergency department which lasted < 1 day were not included. Information on initiation and completion of the rehabilitation programme was collected using a rehabilitation diary. Participants were instructed to record each rehabilitation training session attended during the 12-week intervention period. Additional data were obtained on the duration of rehabilitation stay and time from enrolment to rehabilitation start. Adherence towards the intervention was assessed by calculating compliance. Compliance with study oral nutritional supplementation intake was evaluated using both the daily drink diary and count of remaining cans at the 12-week follow-up. The number of remaining cans was compared with the number of prescribed cans to calculate compliance. Compliance (%) was defined as (number of supplements consumed / number prescribed) × 100. When both diary-based and can-count compliance were available, the mean of the two was used. If only one source was available, that value was used. High compliance was defined as consumption of ≥ 75% of the prescribed study oral nutritional supplementation. 31 Adverse events were assessed for the intervention group and documented through the drinking diary and through weekly follow-up.
Power calculation and statistics
The sample size was calculated to detect a clinically relevant difference of 2.0 repetitions in the 30-sesond chair stand test, based on previous studies in older adults with hip and knee osteoarthritis, which reported a clinically meaningful change of 2.0–2.6 repetitions. 32 Using a pooled standard deviation of 3.31 derived from published data in community-dwelling older adults. 33 Adopting a power of 80%, a two-sided alpha-error of 0.05, and an anticipated dropout rate of 30%, the required sample size is 62 participants in each group, resulting in a total number of 124 participants.
Continuous variables are presented as medians (interquartile range) and categorical variables as number of subjects (percentage). Statistical significance was set at α = 0.05. Analysis was performed using Statistical Analysis System, Version 8. Normality was assessed by the Shapiro–Wilk test, boxplots, and histograms. Between-group comparisons of continuous variables were analysed using the Student t-test for normally distributed data and the Mann–Whitney U-test otherwise. Categorical variables were compared using the χ2 test or Fisher's exact test, as appropriate. Group differences in change over time were analysed using a linear mixed-effects model including fixed effects for group, time, and their interaction, with repeated measurements within participants.
Primary analyses were conducted according to the intention-to-treat principle; per-protocol analyses are presented as sensitivity analyses. The intention-to-treat population included all participants as randomised, the per-protocol analysis included only participants with ≥ 75% compliance. Missing data were handled using predefined deterministic imputation rules. For continuous variables, missing values were imputed using the sample median and, when relevant, adding the observed delta. When baseline values were missing, the overall baseline median was used. For categorical variables, including use of fish oil, calcium or vitamin D supplements, missing follow-up values were imputed using baseline responses (last observation carried forward). Participants with missing baseline data were classified as non-users. This approach was also applied to other categorical variables, such as the presence of oedema when measuring calf circumference. Exploratory analyses of missing-data patterns showed no evidence of systematic differences by treatment group or patient characteristics, supporting the assumption that data were missing completely at random. Data not shown.
Changes from baseline to 6 weeks and 12 weeks were analysed for functional limitations and quality of life. Outcomes related to 38-week readmissions and mortality will be reported separately when follow-up is complete.
Results
Participant flow, recruitment and characteristics
Participant inclusion began on 4 December 2023 and ended on 27 May 2025. The final 12-week follow-up was completed on 3 September 2025. The median time to follow-up was 85 (83–88) and 86 (84–90) days after discharge for the intervention and control group, respectively. An overview of participant recruitment, allocation, follow-up and analysis is illustrated in the CONSORT flow diagram (Figure 2). A total of 768 individuals were screened for eligibility. Of these, 309 (40%) met the inclusion criteria and a total of 123 (40%) were randomised. Reasons for exclusion and loss to follow-up are detailed in the figure. A total of 14 participants discontinued (11%).
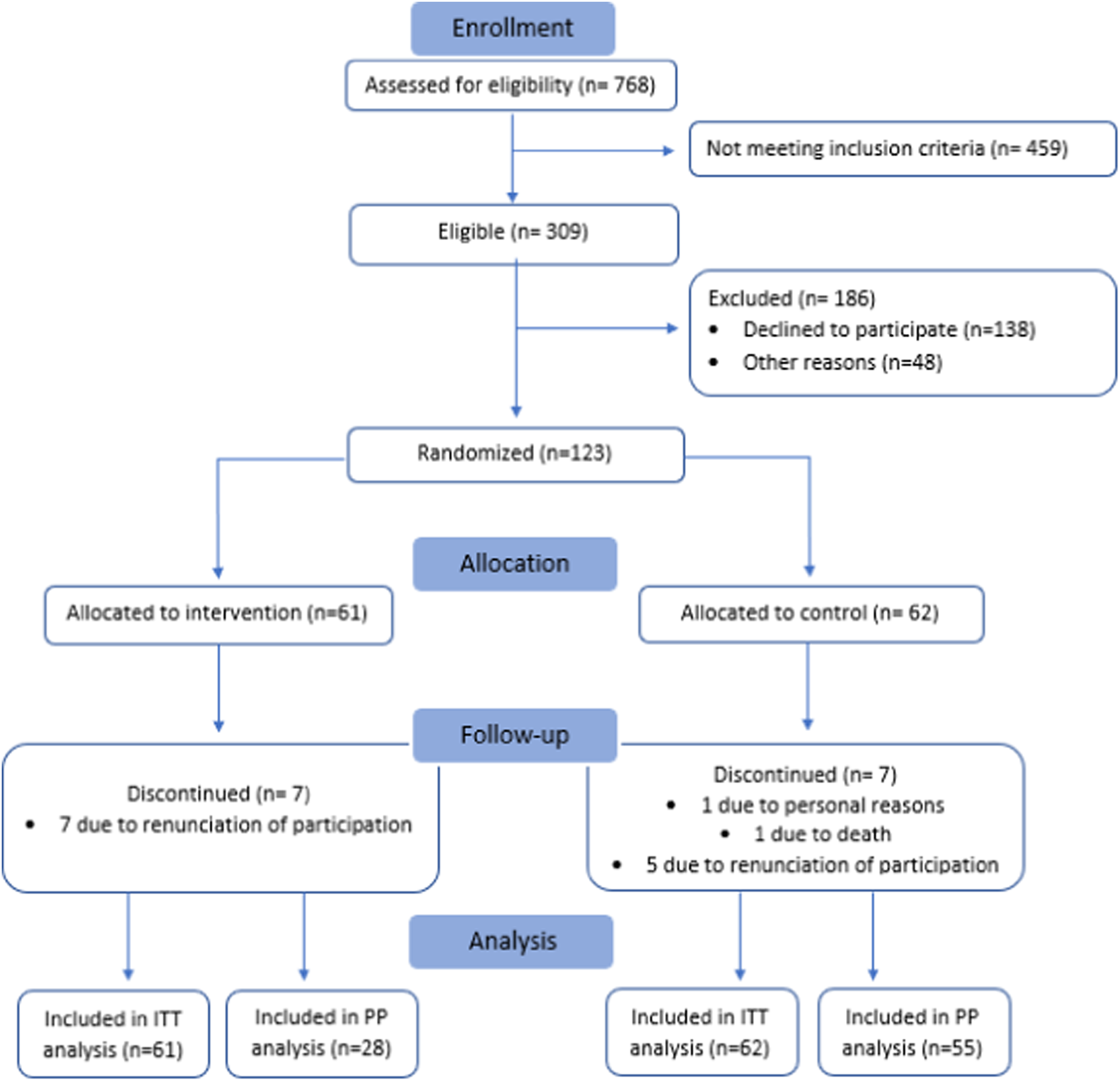
CONSORT flow diagram. Flow-chart showing inclusion, randomisation and participation throughout the study. Abbreviations: IIT: Intention To Treat; PP: Per-Protocol.
Baseline characteristics for 123 randomised participants are presented in Table 2.
Baseline characteristics.
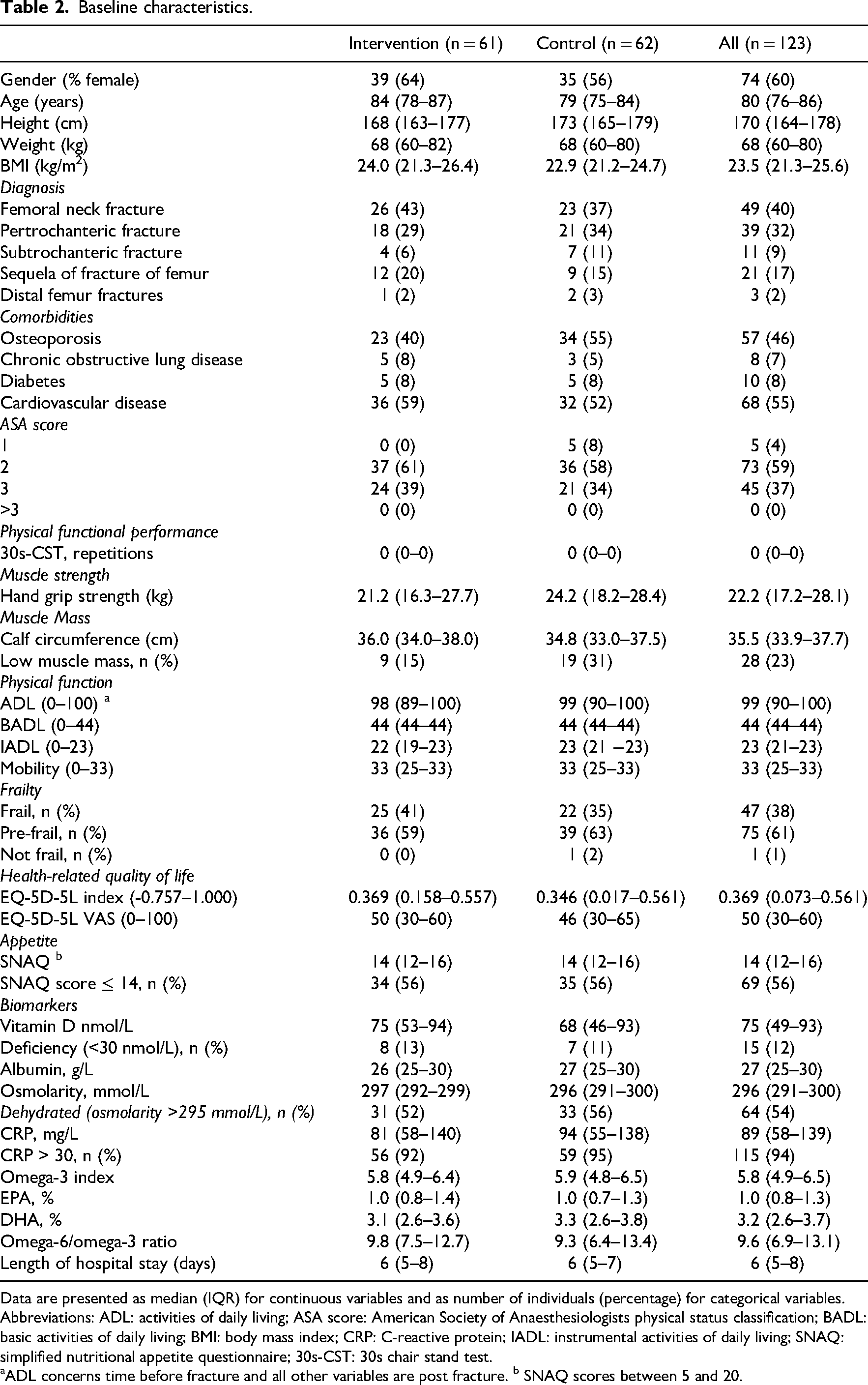
Data are presented as median (IQR) for continuous variables and as number of individuals (percentage) for categorical variables. Abbreviations: ADL: activities of daily living; ASA score: American Society of Anaesthesiologists physical status classification; BADL: basic activities of daily living; BMI: body mass index; CRP: C-reactive protein; IADL: instrumental activities of daily living; SNAQ: simplified nutritional appetite questionnaire; 30s-CST: 30s chair stand test.
ADL concerns time before fracture and all other variables are post fracture. b SNAQ scores between 5 and 20.
Adherence towards the intervention
Compliance with the intervention was evaluated to determine adherence to the study protocol. Mean compliance with the study oral nutritional supplementation was 66%, based on counting cans, and 85% based on daily drink diaries. Compliance calculated using the weighed mean was 72%, corresponding to a mean intake of 1.44 study oral nutritional supplement cans per day. Overall, 28 of 54 participants (52%) achieved a compliance level of at least 75%.
Outcomes
At follow-up, physical functional performance (the primary outcome) improved in both groups with no significant between-group difference in the number of repetitions performed (Table 3).
Results for physical functional performance: Intention to treat analysis.
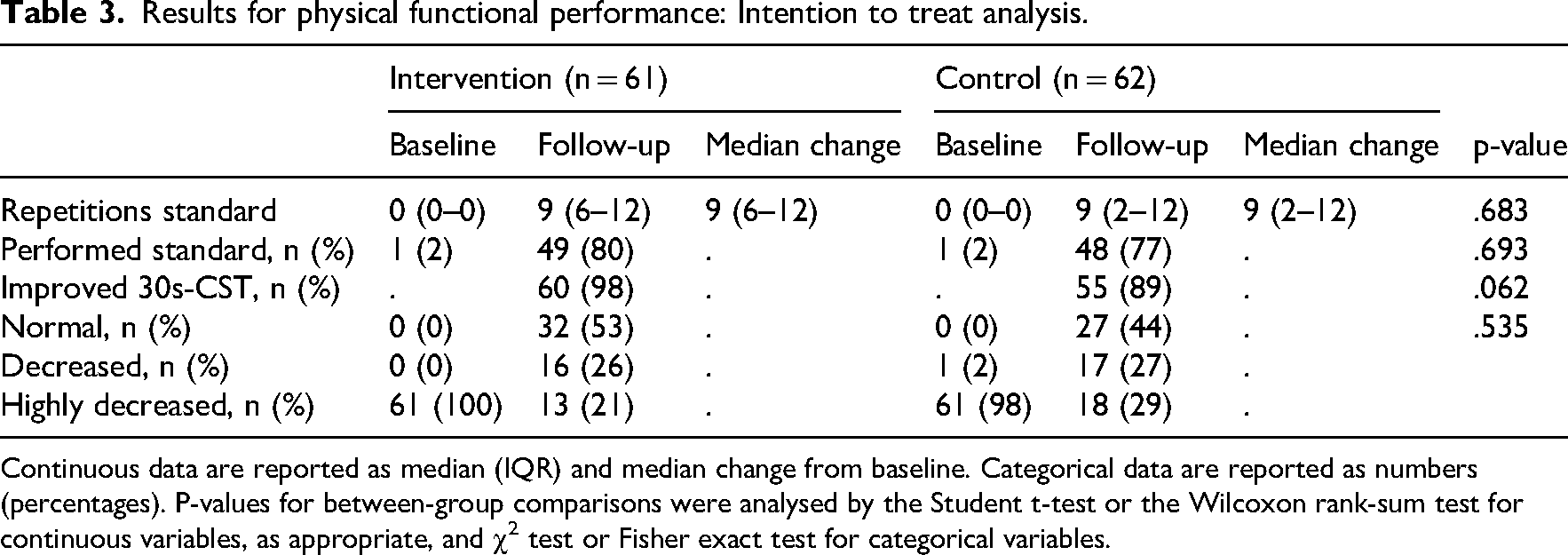
Continuous data are reported as median (IQR) and median change from baseline. Categorical data are reported as numbers (percentages). P-values for between-group comparisons were analysed by the Student t-test or the Wilcoxon rank-sum test for continuous variables, as appropriate, and χ2 test or Fisher exact test for categorical variables.
At follow-up 12 (24%) from the intervention group had reported minor adverse events. These included nausea (6%), loss of appetite (6%), weight gain (2%), obstipation (6%), diarrhoea (2%) and vomiting (2%). No major adverse events were reported.
At follow-up, the intervention group had a significantly higher protein intake than the control group (p = 0.003). There was no significant difference in the energy or the fluid intake
At the 12-week follow-up, omega-3 fatty acid status had increased significantly in the intervention group compared with the control group (p = <.001). Inflammation, assessed by C-reactive protein, decreased in both groups, with no significant between-group difference. Likewise, no significant differences were observed between the groups in vitamin D levels or serum osmolarity.
There was no significant difference in muscle strength, muscle mass, appetite, frailty, weight, BMI, quality of life, functional limitation or proportion of participants who regained pre-fracture status. The full set of results can be found in the supplementary material.
Within 30 days, one participant (2%) in the control group died, whereas no deaths occurred in the intervention group. Seven participants (11%) in the control group and three participants (5%) in the intervention group were readmitted (p = 0.379). The difference was non-significant.
There was a significant difference between the groups in length of rehabilitation stay (p = 0.045). The intervention group had a median stay of 27 days (21–39), compared with 24 days (14–30) in the control group. There was no difference in the number of training sessions, the number of days before initiation of training or the proportion of participants with restrictions.
Additional results for the secondary outcomes are available in the supplementary material.
Results from the per-protocol analysis
Baseline characteristics were comparable for the intervention and control group in the per-protocol. In the per-protocol analysis, the intervention group showed significantly greater improvement in physical functional performance compared with the control group (p = 0.040). Energy and protein intake were also significantly higher in the intervention group (p = 0.003, p = <.001), and omega-3 status improved significantly following the intervention (p = <.001). On average, the intervention group achieved an additional intake of 376 kcal and 23 g of protein compared to the control group. However, the per-protocol analysis was based on a reduced sample size and was not powered for formal between-group comparisons; therefore, these findings should be interpreted with caution. Results from the per-protocol analysis are presented in Table 4. No significant between-group differences were observed for the remaining outcomes. Additional results are available in supplementary material.
Between-group comparison at 12-week follow-up: Per-protocol analysis.
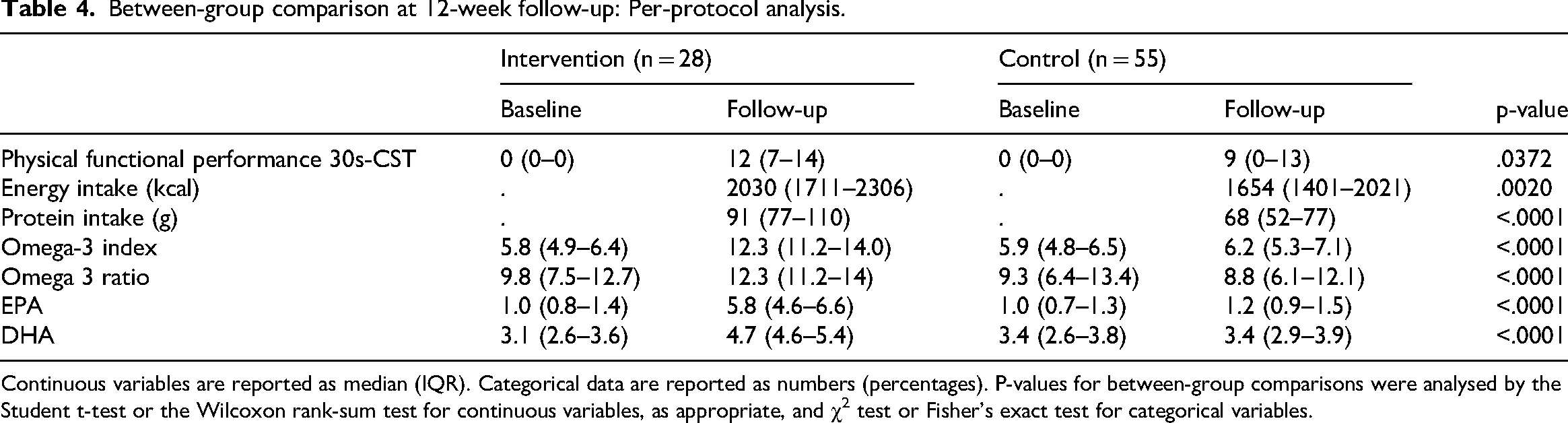
Continuous variables are reported as median (IQR). Categorical data are reported as numbers (percentages). P-values for between-group comparisons were analysed by the Student t-test or the Wilcoxon rank-sum test for continuous variables, as appropriate, and χ2 test or Fisher's exact test for categorical variables.
Discussion
In this randomised controlled trial of older patients with hip fractures at nutritional risk, post discharge oral nutritional supplementation increased energy and protein intake but did not result in a significant between-group difference in physical functional performance in the intention-to-treat analysis. However, in the per-protocol analysis, greater improvements were observed in physical functional performance among participants with high adherence, suggesting that the clinical effect of supplementation may depend on sufficient intake. These findings should however be interpreted with caution as the per-protocol analysis is underpowered and thus limits the validity.
Physical functional performance improved in both groups, reflecting the expected rehabilitation trajectory following hip fracture. Further, participants with high adherence to oral nutritional supplementation achieved significantly greater gains in physical functional performance, suggesting that adequate nutritional intake may enhance physical recovery after hip fracture when the intervention is followed as intended.
Despite these findings, no between-group difference was detected in functional limitations as measured by activities of daily living. Several factors may explain this discrepancy. Functional independence typically recovers more slowly than physical capacity and previous studies have demonstrated delayed effect on activities of daily living indicating that improvements may emerge beyond three months. One example is the study from Tidermark et al. (2004) which reported improvements in functional independence only after six months of follow-up. Although a longer follow-up might have revealed group differences, the 12-week follow-up was chosen to align with the average length of municipal rehabilitation.
The study was not powered to detect differences in activities of daily living, as the sample size was calculated based on physical functional performance. Consequently, smaller but clinically relevant effects on daily functioning may not have reached statistical significance. Although a marginal difference in rehabilitation length of stay was observed between groups, the difference was minimal and unlikely to have substantially influenced outcomes. This difference may reflect increased attention towards participants in the intervention group during rehabilitation stay, suggesting a possible performance or attention effect, despite thorough information that the study oral nutritional supplementation constituted the only intervention. However, as rehabilitation duration was determined by routine clinical practice rather than the study protocol, the longer rehabilitation stay in the intervention group may also represent a potential confounding factor. A longer rehabilitation period may have provided additional opportunity for recovery and functional improvement. Consequently, the observed between-group differences should be interpreted with this potential limitation in mind.
Compliance with the study oral nutritional supplementation was moderate, with a weighted compliance of 72%, consistent with previous studies in older hip fracture populations, reporting compliance from 67% to 78–80%.34,35 This level of adherence was only sufficient to increase protein intake at the group level. Still the intake in gram of protein per kilo was in the lower end for some participants reflected in the standard deviation. In contrast the gram protein per kg was high for all participants with adherence ≥75%. The discrepancy between intention-to-treat and per-protocol analysis suggests that the effectiveness of supplementation may depend on sufficient intake. Lower adherence in the full sample likely diluted the treatment effect. Participants with high compliance achieved substantially greater increase in energy and protein intake, which may partly explain their greater improvement in physical functional performance.
However, per-protocol analyses are susceptible to residual confounding and selection bias. Adherence itself may reflect underlying differences in health status, motivation or recovery trajectory. Participants able to comply with the intervention may have been less frail, experienced fewer postoperative complications or had better functional capacity at baseline, factors independently associated with better outcomes. These factors warrant cautious interpretation but do not preclude a clinically meaningful effect of supplementation when adequately consumed.
Adherence in this frail population is influenced by multiple factors, including reduced appetite, taste preferences and medication-related side effects. Despite targeted strategies to support adherence, including counselling, written materials and weekly follow-up, maintaining adequate intake remained challenging in this frail population. This underscores the need for more individualised and flexible approaches, such as tailored flavour selection or dosing regimens, to optimise adherence in future interventions.
Strength of this trial include a broadly representative sample of the population reflecting current clinical practice, characterised by fast-track surgical pathways, shorter hospital stays and early initiation of rehabilitation. Furthermore, the trial includes a comprehensive outcome assessment aligned with core outcome recommendations and has a high follow-up completeness of 88.6%.
Further, the study population appeared healthier than the general hip fracture population, as reflected by lower mortality rate compared with national registry data. 1 This may limit generalisability and could underestimate the potential benefits of nutritional supplementation in frailer patients. However, such selection bias is common in studies requiring informed consent and active participation, where the most vulnerable individuals are less likely to be enrolled.
Finally, even though the baseline characteristics were comparable for the intervention and control group in the per-protocol analysis such analyses are underpowered which limits their validity.
In conclusion post-discharge oral nutritional supplementation increased protein intake but did not improve physical functional performance in the intention-to-treat analysis. Per-protocol findings suggest that high adherence may be necessary to enhance physical functional performance, underscoring the importance of strategies that support a sustained intake after discharge. It is, however, important to acknowledge that the per-protocol analysis is underpowered and thus limits the validity of the findings.
Clinical messages
Providing oral nutritional supplementation at discharge improves energy and protein intake in older hip fracture patients at nutritional risk.
Oral nutritional supplementation may improve physical functional performance when integrated into rehabilitation and consumed with high adherence.
Supplemental Material
sj-docx-1-cre-10.1177_02692155261462462 - Supplemental material for Effect of oral nutritional supplements on physical functional performance in older patients at nutritional risk discharged with a rehabilitation plan: A randomised controlled trial
Supplemental material, sj-docx-1-cre-10.1177_02692155261462462 for Effect of oral nutritional supplements on physical functional performance in older patients at nutritional risk discharged with a rehabilitation plan: A randomised controlled trial by Alberte Jensen, Elna D. Ninh, Barbare B. Darlem, Line M. Haack, Cecilie M. Møller, Anne W. Knudsen, Frederikke E. Pudselykke, Pelle B. Petersen and Anne Marie Beck in Clinical Rehabilitation
Footnotes
Acknowledgements
We thank the staff of the Orthopaedic Surgical Department for their support of the project and their assistance with participant inclusion. We also thank the clinical dietitians for conducting secondary screening and initiating participant contact. Finally, we extend our sincere appreciation to all patients who participated in the study. Their willingness to contribute made this work possible.
Ethics considerations and consent to participate
The study has been approved by the Danish Regional Ethics Committee of the Capital Region (Journal No.: H-21064554) and the Danish Data Protection Agency (P-2022-293). Eligible patients received both written and oral information before signing an informed consent form. During the trial, the Ethical Committee accepted a protocol amendment approving the measurement of hydration status at follow-up.
Author contributions
AJ, EDN, AMB, FEP, PBP, BBD, LMH, AWK and CMM contributed to writing the manuscript. The trial was conducted by AJ and EDN, who also collected the data. AJ was responsible for data cleaning and management. AJ and AWK performed the statistical analyses. AMB, who initiated and designed the study and obtained funding, also supervised the trial and monitored its progress. The analytic strategy was decided by AMB, AWK and AJ. All authors read and approved the final manuscript
Funding
The study was funded by Nutricia DANONE. They were not involved in trial conduct or reporting.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.