
Abstract
Objective
Falls are a serious complication of Parkinson's disease, leading to functional decline, psychological distress, and substantial economic burden. Although multiple interventions have been proposed, structured quantitative guidance on prioritising fall-prevention strategies for clinical implementation in Parkinson's disease remains limited.
Design
A multi-method study integrating a structured narrative review, expert consensus via a two-round Delphi process with 15 multidisciplinary Parkinson's disease experts, and multi-criteria decision-making using the Best–Worst Method to identify and quantitatively prioritise fall-prevention strategies for people with Parkinson's disease.
Setting
Expert-based consensus and decision-analysis study.
Participants
Fifteen multidisciplinary experts with clinical and research expertise in Parkinson's disease and neurorehabilitation.
Intervention
Fall-prevention interventions identified through a structured narrative review and refined through a two-round Delphi process, followed by prioritisation using the Best–Worst Method.
Main measures
Relative priority weights of intervention categories and sub-criteria derived using the Best–Worst Method based on expert judgements.
Results
The Delphi process yielded three main criteria (exercise, dance-based interventions, and neuroscience-based interventions) and 14 sub-criteria. Best–Worst Method weighting showed that exercise had the highest priority (weight=0.49), followed by dance-based interventions (weight=0.32) and neuroscience-based interventions (weight=0.19). Within exercise, balance training and resistance strength training received the greatest weights, whereas Tai Chi and transcranial direct current stimulation received the highest expert-derived priority weights within the dance-based and neuroscience-based categories, respectively.
Conclusion
This integrative framework provides an evidence-informed hierarchy of expert-derived priorities for fall-prevention interventions and may support clinical decision-making and programme design, while highlighting the need for further effectiveness and implementation research.
Introduction
Parkinson's disease is the second most common neurodegenerative disorder, a progressive condition that affects the central nervous system.1,2 It affects approximately 1–2% of the elderly population, with prevalence expected to rise substantially in the coming decades due to global population ageing. 3 By 2050, an estimated 25.2 million people are projected to be living with Parkinson's disease worldwide, representing a 112% increase compared with 2021. 4 Impaired balance is a major cause of falls in Parkinson's disease, arising from motor, sensory, and cognitive dysfunctions that progressively impair postural control.5–7 Individuals with Parkinson's disease commonly exhibit reduced proprioceptive accuracy, decreased lower-limb strength, delayed motor responses, and deficits in sensory integration.8–10 Consequently, falls are highly prevalent, affecting 38–68% of individuals with Parkinson's disease annually, 11 with up to 87% experiencing at least one fall over the disease course. 12 These falls lead to fractures, hospitalisations, reduced activity, and accelerated functional decline,13–15 while also triggering psychological distress, particularly fear of falling,8,16 and imposing a considerable personal, social, and economic burden. 17
While a wide range of fall-prevention strategies have been established, there remains no consensus regarding which interventions should be prioritised for individuals with Parkinson's disease. Previous findings report mixed results, with some studies demonstrating significant reductions in fall rates following exercise, dance-based, and neuroscience-based interventions,18–20 while others report limited or inconsistent effects on fall-prevention outcomes.21–23 Existing systematic reviews and meta-analyses typically focus on intervention efficacy in isolation,24–27 rather than providing comparative, clinically actionable rankings that integrate expert judgement and multiple decision-making criteria. To address this gap, this study employs a comprehensive, multi-method approach to evaluate and rank fall-prevention interventions in Parkinson's disease, aiming to enhance rehabilitation outcomes and reduce both financial and caregiving burdens. Specifically, the objectives were to: (1) identify fall-prevention interventions for Parkinson's disease through a structured narrative review; (2) develop and refine a set of prioritisation criteria using a Delphi process with multidisciplinary Parkinson's disease experts; and (3) apply the Best–Worst Method to derive quantitative weights for each intervention category and sub-category.
Methods
Literature review
A structured narrative review was undertaken to map and appraise fall-prevention interventions for Parkinson's disease, identifying candidates for expert prioritisation amid heterogeneous evidence. The search encompassed English-language papers published from 2010 to 2025 and was developed using the population, intervention, comparison, and outcome method using ‘‘OR,’’ ‘‘AND,’’ ‘‘NOT’’ between the selected keywords (Parkinson's disease, Falling, Falls, Neurorehabilitation, Exercise Therapies, Aquatic Therapy, Dance Therapies, Telemedicine, transcranial direct current stimulation, Neurofeedback, Biofeedback) in PubMed, Scopus, and Web of Science. Although this review is narrative rather than systematic, a flow diagram was used to enhance transparency by describing the detailed search strategy, exclusion criteria, and article selection process (Figure 1). Data extracted included study design, sample size, intervention type, fall-related outcomes, and key findings.
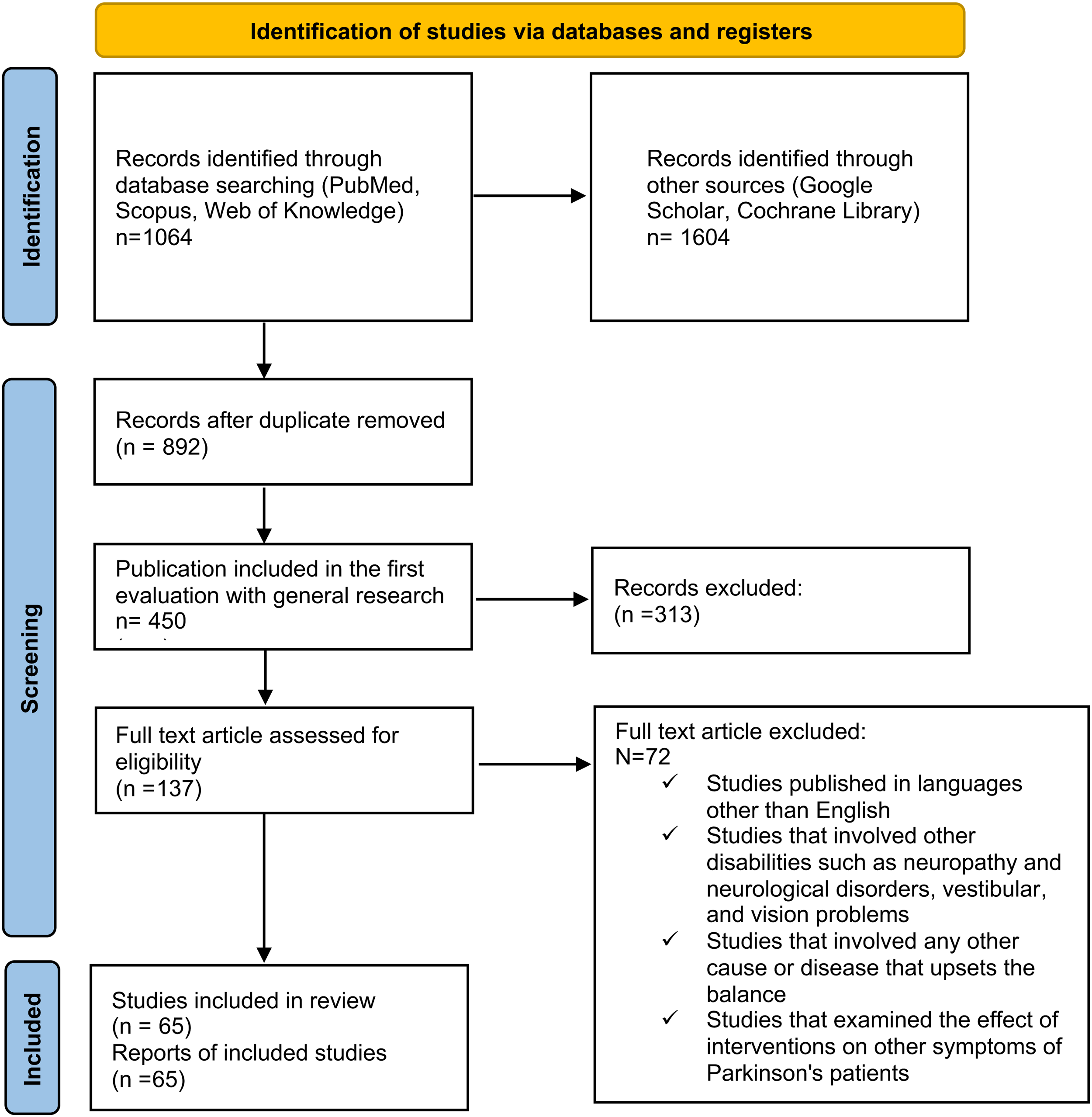
The flow diagram of the study selection process.
Two independent reviewers screened titles and abstracts, followed by full-text review against predefined eligibility criteria. When disagreements occurred, the reviewers re-examined the relevant article against the eligibility criteria and discussed the decision until consensus was reached. If consensus could not be reached, a third reviewer made the final decision. Studies were included if they (i) were written in English, (ii) targeted individuals with a clinical diagnosis of Parkinson's disease, (iii) evaluated a fall-prevention intervention, and (iv) reported at least one fall-related or balance outcome. A detailed summary of the included studies is provided in Supplemental Table 1.
This screening process identified interventions for further evaluation and informed their subsequent prioritisation. Interventions were first refined through a Delphi study, allowing a multidisciplinary expert panel to achieve consensus on the most relevant and feasible strategies. Following this, the Best–Worst Method, a quantitative multi-criteria decision-making tool, was applied to mathematically weight each intervention based on expert-defined criteria. This integrated approach ensures that the selected interventions are both evidence-informed and contextually prioritised, combining structured mapping of the narrative review with expert judgement and robust quantitative ranking.
Decision-making involves evaluating options to select the most appropriate course of action. In healthcare, this integrates medical, technical, social, ethical, and economic factors to achieve precise, cost-effective, and transparent outcomes. Given the complexity of fall-prevention strategies, collaboration among patients, clinicians, and stakeholders is essential. Accordingly, a Delphi study was employed to establish expert consensus on prioritising interventions for Parkinson's disease.
Delphi method
The Delphi approach was chosen for its iterative nature, which allows refinement of expert opinions, facilitates meaningful agreement, minimises groupthink, 28 and provides a structured consensus for prioritising fall-prevention interventions for individuals with Parkinson's disease. The Delphi method was conducted in two iterative Rounds using an anonymous online questionnaire and was reported in line with the Accurate Consensus Reporting Document guidelines (Figure 2). Candidate interventions were derived from the structured review and refined by the steering group prior to Round 1. In Round 1, experts assessed the importance and feasibility of each fall-prevention strategy using a 7-point Likert scale (1 = strongly disagree to 7 = strongly agree). Strategies achieving high agreement (≥80% consensus) were retained, while those with lower agreement were revised or discarded. In Round 2, experts reassessed strategies that did not reach consensus in Round 1 and provided justifications for their evaluations. Consensus was defined a priori as ≥80% of ratings within two adjacent scale points; items failing to meet this threshold after Round 2 were excluded from subsequent Best–Worst Method weighting.
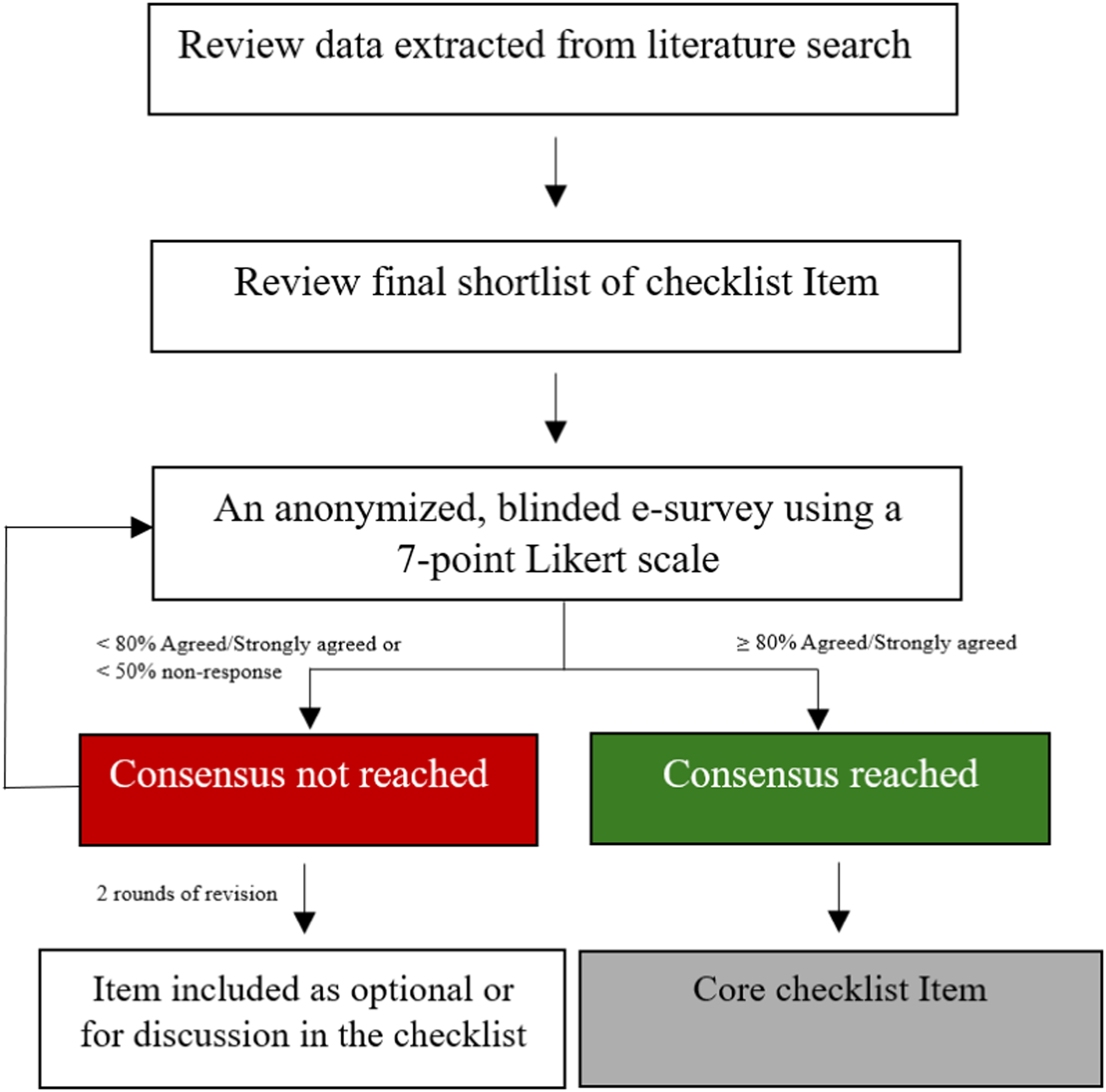
Methodology used for Delphi panel based on accurate consensus reporting document guideline.
Panel composition and response rates
The panel comprised three physiotherapists, three neurologists, three occupational therapists, three neuropsychologists, and three geriatric medicine specialists, each with ≥10 years of clinical experience in Parkinson's disease care and involvement in fall-prevention research or service delivery. Recruitment was conducted through direct invitations and targeted outreach via professional networks. A total of 29 invitations were sent, yielding a response rate of 52% (number=15). All experts completed both Delphi Rounds via anonymous online questionnaires, resulting in a 100% retention rate between Rounds and supporting the reliability of the consensus estimates.
Data analysis and reporting
Quantitative analysis involved calculating mean scores, standard deviation, and interquartile range for each strategy to assess consensus levels. In Round 1, these measures evaluated central tendency, response dispersion, and variability while minimising the influence of outliers. In Round 2, the same statistical metrics were applied, resulting in the removal of two interventions that did not meet the 80% consensus threshold, as experts judged them less feasible in clinical practice. Qualitative data from expert justifications in Round 2 were thematically analysed to provide context for strategy revisions or exclusions. To ensure transparency and reproducibility, all steps of the Delphi process, including statistical analyses, were meticulously documented.
Multi-criteria decision-making
Best–Worst Method
The Best–Worst Method is a validated multi-criteria decision-making technique that derives criterion weights from expert pairwise comparisons between the most and least important criteria. Compared with other methods, Best–Worst Method requires fewer pairwise comparisons, produces more consistent and precise results, and employs integer values for comparisons, making it a robust and efficient tool for prioritisation. 29 It has been widely applied in healthcare decision-making, as described in detail by Rezaee et al. 29 and other previous studies14,29–35 In the present study, Best–Worst Method was used to prioritise fall-prevention strategies based on expert-assigned criteria. The Best–Worst Method procedure involves listing the decision criteria, identifying the best and worst criteria, conducting pairwise comparisons using a 1–9 scale, calculating criterion weights, and assessing consistency. The detailed stepwise procedure, mathematical models, and consistency calculations are provided in Supplemental Material A.
Results
Delphi method
The two-round Delphi process demonstrated clear convergence in expert ratings. In Round 1, the mean criterion score was 4.26 (standard deviation = 2.17, interquartile range = 3.03), and in Round 2, 4.24 (standard deviation = 2.16, interquartile range = 3.05), indicating stable central tendencies but persistent variability in dispersion indices. The normalised inter-round consensus level was 0.94, indicating strong overall stability of expert judgements between Rounds. Ultimately, three main criteria and 14 sub-criteria for Parkinson's disease fall-prevention interventions were identified based on the Delphi method (Table 1).
Criteria for evaluation of the preventive falling interventions in Parkinson's disease.
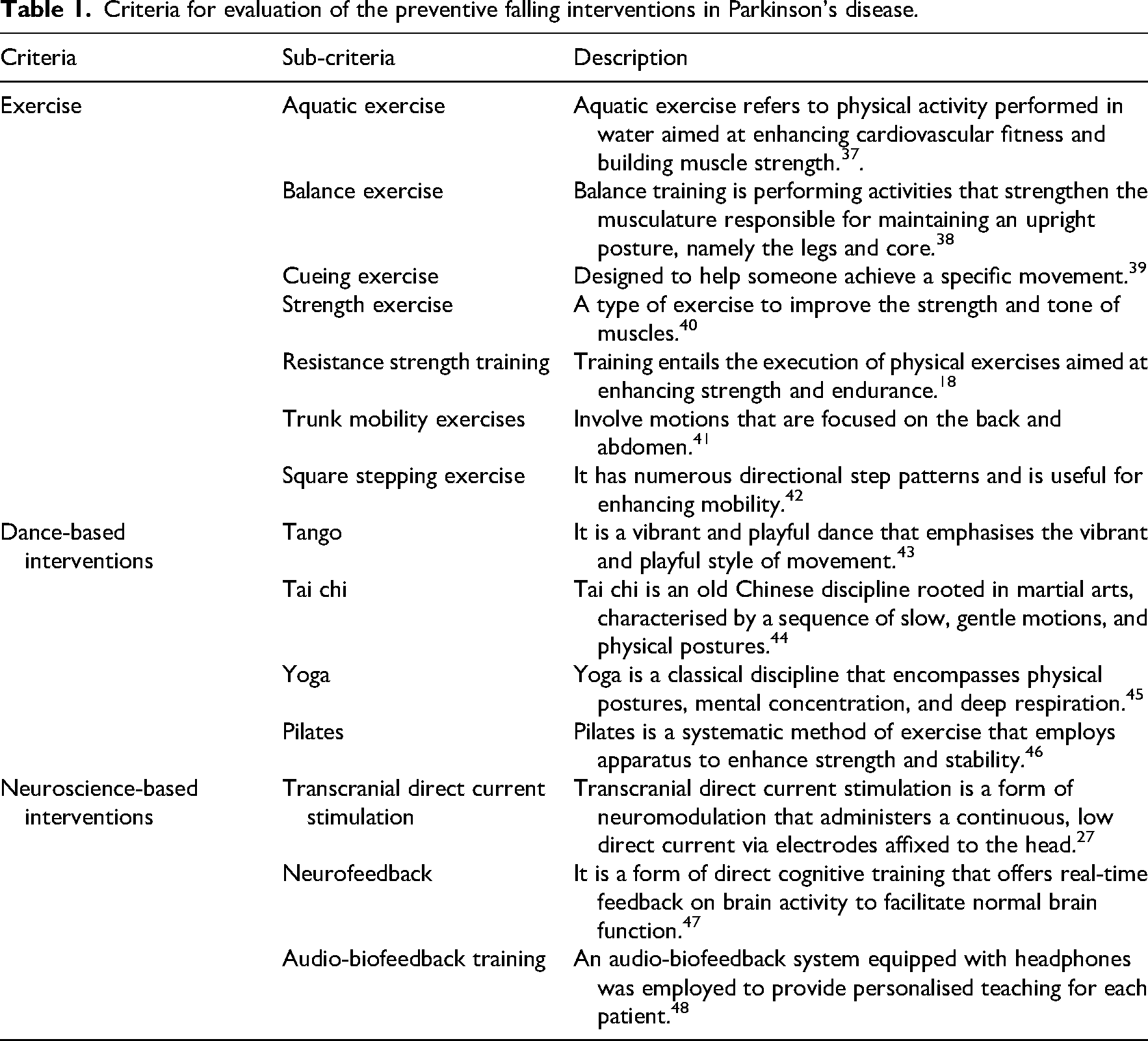
Exercise-based interventions refer to structured physical training mainly targeting strength, balance, mobility, endurance, and functional capacity. In contrast, dance-based interventions were defined as movement-based interventions in which rhythm, choreographed or patterned movement, body awareness, postural alignment, engagement, or dance-specific motor sequencing constituted key therapeutic components, rather than primarily targeting isolated strength, endurance, or conventional functional training. Although Tai Chi, Yoga, and Pilates may also be considered exercise-based in rehabilitation contexts, consistent with previous literature, 36 they were grouped separately in this study because they share movement-based and mind–body features, including coordinated movement, rhythm, and movement sequencing. Neuroscience-based interventions were defined as approaches targeting neural modulation, feedback, or motor-control mechanisms.
The Best–Worst Method for criteria weight calculation
Experts applied Best–Worst Method to rate the relative importance of the three primary intervention categories: Exercise, Dance-based interventions, and Neuroscience-based interventions. Most experts selected exercise as the best main criterion, whereas neuroscience-based interventions were most frequently designated as the least important (Table 2). These selections reflect expert judgements about relative priority for fall-prevention programme design, rather than direct evidence of comparative clinical effectiveness.
Best and worst main criteria identified by the decision team.

All participants compared their selected best and worst primary criteria against the remaining criteria using a 1 to 9 scale, where 1 indicated equal importance, and 9 indicated a substantially stronger preference. These comparisons were used to generate the Best-to-Others and Others-to-Worst vectors. The resulting comparison matrices for each expert are presented in Supplementary Tables 2 and 3.
After computing the individual weights for each criterion using model, 2 described in Supplementary Material A and the corresponding linear programming procedure, the final weight of each criterion was obtained by calculating the arithmetic mean across all members of the decision team. The final weights for the main criteria, exercise, dance-based interventions, and neuroscience-based interventions, are presented in Table 3. The main criteria weights, obtained via expert assessments using the Best–Worst Method, represent the relative expert-derived priority of each criterion. After computing individual weights and averaging across experts, exercise received the highest main criterion weight (0.49 ± 0.26), followed by dance-based interventions (0.32 ± 0.25) and neuroscience-based interventions (0.19 ± 0.16). These weights reflect expert judgement informed by available evidence, feasibility, and perceived clinical relevance, rather than comparative effect sizes or direct measures of clinical effectiveness.
Weights and rankings of main intervention criteria.
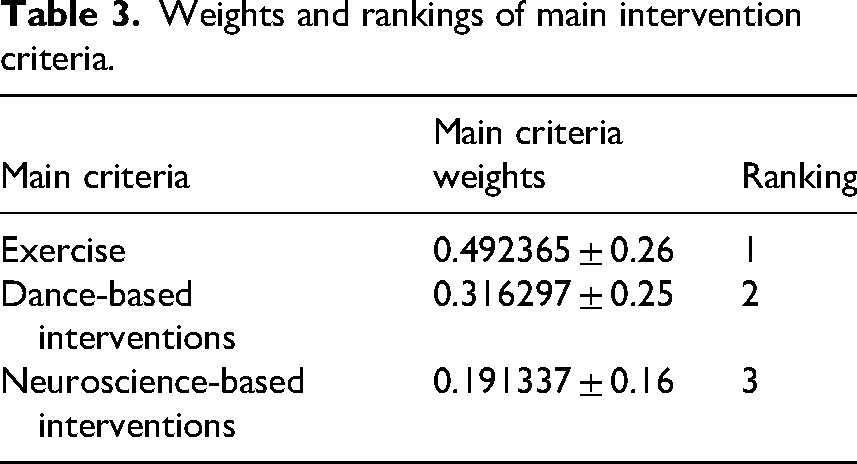
Within exercise, the sub-criteria were prioritised as Balance exercise > Resistance strength training > Strength exercise > Square Stepping exercise > Trunk mobility exercises > Cueing exercise > Aquatic exercise, ranging from balance exercise (weight 0.25) to aquatic exercise (0.05) (Supplemental Table 4). For dance-based interventions, Tai Chi (0.50) and Tango (0.29) received the highest weights, followed by Pilates and Yoga (Supplemental Table 5). Within neuroscience-based interventions, transcranial direct current stimulation was assigned the highest weight (0.66), followed by neurofeedback (0.26) and audio-biofeedback (0.07) (Supplemental Table 6).
Discussion
This study systematically identified and prioritised fall-prevention interventions for individuals with Parkinson's disease through a rigorous two-phase process combining the Delphi method and Best–Worst Method. By integrating expert consensus with a formal multi-criteria decision-making framework, the study extends beyond traditional narrative or efficacy-focused reviews and provides a transparent, quantitative prioritisation of intervention categories and sub-criteria. The Delphi process ensured that criterion selection and refinement were grounded in multidisciplinary expertise, yielding strong inter-round stability and high consensus, which supported the reliability of the expert-derived criteria. This multidisciplinary approach reinforced the clinical and neurorehabilitative relevance of the identified criteria. In turn, the application of Best–Worst Method provided a mathematically robust means of quantifying relative priority with high internal consistency. Together, these methods support the use of the integrated Delphi–BWM framework for prioritising healthcare interventions and ranking fall-prevention strategies in Parkinson's disease.
The results highlight exercise-based strategies as the most highly prioritised by experts, followed by dance-based and neuroscience-based interventions. The prioritisation of exercise aligns with previous meta-analyses demonstrating its efficacy in reducing fall risk and improving gait, balance, and motor control in Parkinson's disease. 49 Within the exercise domain, balance training received the highest weight, reflecting expert judgement regarding the centrality of postural control in Parkinson's disease-related falls, alongside evidence that targeted balance exercises can improve stability and reduce falls.50,51 Resistance and strength training were also highly prioritised, reflecting growing evidence that muscle weakness and impaired force generation are modifiable contributors to fall-prevention.24,52 Strength training may enhance neural drive and motor unit recruitment, contributing to improved postural stability.53,54 However, the inconsistent findings in individual trials, including those reporting no significant effect on fall rates, underscore that the expert-derived weights should not be interpreted as definitive effect sizes or direct measures of comparative clinical effectiveness. These weights should be integrated with patient characteristics, disease stage, and service capacity. For instance, Canning et al. observed no significant impact of balance and strength exercises on fall-prevention, potentially reflecting limitations related to disease severity or insufficient exercise intensity. 55 Similarly, Goodwin et al. (2011) reported no effect, possibly due to small sample sizes. 21
Dance-based interventions received the second-highest expert-derived priority among the major criteria, with Tai Chi receiving the highest weight within the dance sub-criteria. This is consistent with previous reports 19 and systematic reviews and meta-analyses, 44 showing that these interventions, including Tai Chi, can improve functional mobility and balance and contribute to fall-prevention in individuals with Parkinson's disease. Dance-based interventions involve weight shifting, trunk rotation, and precise, controlled movements, which may enhance proprioceptive and vestibular function and support postural stability. 36 However, trial findings remain heterogeneous, with effects varying according to intervention duration, training intensity, and participant disease severity. 23
Neuroscience-based interventions, although assigned the lowest relative weight at the main-criteria level, represent a rapidly evolving complementary domain. Within this category, transcranial direct current stimulation received the highest sub-criterion weight, consistent with evidence supporting its benefits for balance, mobility, and fall-prevention in Parkinson's disease.56–58 Consistent with the interpretation of all Best–Worst Method weights in this study, these weights reflect prioritisation rather than comparative effectiveness. Transcranial direct current stimulation modulates cortical excitability and may induce long-term changes in central nervous system activity, particularly when applied over regions involved in postural control and motor function. However, its effectiveness depends on stimulation parameters and montage. The lower weighting of this category may reflect the still-emerging evidence base, heterogeneity of protocols, training requirements, and practical implementation challenges. Consequently, experts may perceive neuroscience-based interventions as adjunctive rather than primary strategies.
The novelty and added value of this framework lie in translating existing evidence and expert judgement into a structured prioritisation of fall-prevention interventions, rather than simply reaffirming established evidence supporting exercise-based strategies, to support clinical decision-making when several options are feasible. A more detailed comparison with existing systematic reviews and clinical guidelines is provided in Supplementary Material C. This study has important implications for clinical practice, service delivery, and policy in Parkinson's disease fall-prevention. The prioritisation framework translates the results into practical guidance for programme design, resource allocation, and stepped-care planning. Rehabilitation services could use the hierarchy to guide the selection and sequencing of intervention options within standard fall-prevention programmes. This approach may also support stepped-care models, in which core exercise-based programmes are offered first, followed by dance-based interventions as adjunctive or complementary options for individuals who require additional support or do not respond sufficiently to first-line strategies. Neuroscience-based interventions may then be considered adjunctive or emerging options until supported by stronger evidence. At a policy level, identifying these priorities may help guide decisions about staff training, service pathways, implementation resources, and investment toward higher-priority interventions within the expert-informed framework.
Several limitations should be acknowledged. Although the expert panel was diverse and experienced, the sample size remains characteristic of Delphi research but may not capture the full variability present across global clinical settings. The study relied exclusively on expert judgements, omitting the perspectives of patients and caregivers, who could provide critical insights regarding the feasibility, acceptability, and practical relevance of the interventions. Additional limitations include the lack of long-term effectiveness or real-world implementation data, the possibility that intervention categories may differ across rehabilitation frameworks, and the absence of stratification according to disease stage, cognitive status, freezing of gait, comorbidity burden, or functional capacity. Accordingly, the findings should be interpreted as broad expert-derived priorities for fall-prevention programme design, most directly applicable to general clinical planning for people with mild-to-moderate Parkinson's disease. For individuals with more advanced disease or more complex clinical profiles, intervention selection should be individualised according to safety, functional capacity, and rehabilitation goals. Further detail on the implementation-related limitation, intervention classification, and subgroup-specific considerations is provided in Supplementary Material D. Future studies should develop and validate subgroup-specific prioritisation frameworks and assess the long-term effectiveness, feasibility, safety, adherence, perceived benefit, and real-world uptake of high-priority fall-prevention interventions while incorporating patient and caregiver perspectives. Additional research should evaluate emerging approaches, such as neurofeedback and audio-biofeedback, and examine whether expert-derived priority weights correspond to real-world effectiveness, including through trials combining exercise, dance-based interventions, and neuroscience-based interventions.
In conclusion, this study provides an evidence-based framework for prioritising fall-prevention interventions in Parkinson's disease. The findings can support more structured, multidisciplinary rehabilitation programmes that consider patient needs and available resources. By presenting a data-driven prioritisation model, the study supports evidence-informed decision-making and future guideline and implementation research.
Clinical messages
Exercise, particularly balance and resistance strength training, may be prioritised as core components of Parkinson's disease fall-prevention programmes based on the highest expert-derived priority weights.
Tai Chi and tango may be considered dance-based adjuncts.
Transcranial direct current stimulation may be used cautiously as an adjunctive option pending stronger evidence.
Supplemental Material
sj-docx-1-cre-10.1177_02692155261464597 - Supplemental material for Prioritising fall prevention strategies in Parkinson's disease: A multi-method evaluation
Supplemental material, sj-docx-1-cre-10.1177_02692155261464597 for Prioritising fall prevention strategies in Parkinson's disease: A multi-method evaluation by Fatemeh Bahramian, Ali Bahramian, Seyed Abolfazl Mousavi, Bahareh Ahmadinejad and Alireza Jalali in Clinical Rehabilitation
Footnotes
Acknowledgements
There are no acknowledgements.
Ethics approval
The study was documented in the Open Science Framework, ensuring transparency and adherence to best research practices. Additionally, ethical approval was obtained from the Milad Hospital Review Board, confirming compliance with ethical standards for research involving human participants.
Consent to participate
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.