
Abstract
Objective
This feasibility study examined the following aspects of applying Cognitive Orientation to daily Occupational Performance to stroke survivors: recruitment, dose, fidelity, perceived value, benefits, harms and potential outcomes.
Design
Single-group pretest–posttest design.
Setting
Danish municipal neurorehabilitation centre.
Subjects
Home-living stroke survivors aged 45 years or older, with a score of at least 20 on the Montreal Cognitive Assessment, referred from hospital or rehabilitation units. Participants identified at least two occupational performance issues.
Interventions
The Cognitive Orientation to daily Occupational Performance approach aims to improve occupational performance through a therapist-guided process focusing on problem-solving, strategy use, generalisation and transfer. Three occupational therapists delivered the intervention.
Main measures
Data on participant characteristics and feasibility aspects were collected using surveys, registration forms, interviews and performance-based measures. Occupational performance was assessed using the Canadian Occupational Performance Measure and the Performance Quality Rating Scale.
Results
Of 65 invited stroke survivors, 20 (30.8%) were enrolled. Recruitment took longer than expected due to organisational factors. The intervention was delivered with high fidelity and was perceived as meaningful by both therapists and participants. Significant improvements (p < 0.001) were observed in occupational performance on the Canadian Occupational Performance Measure: performance (mean difference 2.98), satisfaction (mean difference 4.33) and on the Performance Quality Rating Scale (mean difference 2.69).
Conclusion
The intervention was feasible in this setting. A full-scale effectiveness study is warranted.
Keywords
Introduction
Stroke is one of the primary causes of disability worldwide, affecting millions of people annually. 1 The most recent figures suggest an incidence of 12 million new stroke cases per year worldwide. 2 The incidence of stroke is closely related to age, and the number of people who will suffer a stroke will therefore inevitably continue to rise over the next decades as the population ages. 3 Stroke survivors often experience changes in their physical, cognitive and emotional abilities impeding their day-to-day function, aka occupational performance. 4 Research shows that six months after the event, 25% of stroke survivors are still dependent on assistance to perform their daily activities despite having received rehabilitation. 4 Even a higher percentage find that complex activities and participation in the community are challenging. Further, occupational performance and quality of life may decline over several years post-event, even in the absence of further clinical strokes, which leads to increased use of healthcare services. 5
Cognitive Orientation to daily Occupational Performance (CO-OP) is a client-centred, problem-solving approach designed to address occupational performance issues. 4 CO-OP has four main objectives: acquisition of client-chosen skills, strategy use, generalisation and transfer. CO-OP comprises five essential elements: (1) client-centred occupation-focused performance goals, (2) dynamic performance analysis, (3) cognitive strategy use (Goal-Plan-Do-Check and domain-specific strategy use), (4) the therapeutic approach guided discovery and (5) enabling principles. 4 It is based on neuroplasticity, learning and motor-learning theories, and is the result of over 20 years of research within a variety of populations. 4 In several studies, CO-OP has been shown to effectively improve occupational performance among people with stroke, traumatic brain injury and older adults with cognitive complaints, to name a few.6–16 In addition, scoping reviews have indicated that CO-OP can improve generalisation and transfer of achieved performance skills and strategy use to everyday life, post-rehabilitation.17–19 Given these promising results, CO-OP has the potential to answer the need for a specific, evidence-based intervention to apply within municipal outpatient neurorehabilitation to improve occupational performance as well as transfer and maintenance of achieved results.
While CO-OP has shown effectiveness in several rehabilitation settings, its potential cannot be assumed when transferring from one context to another, as each context brings its own particularities. Accordingly, while promising, it cannot be assumed that CO-OP would be feasible in a Danish municipal context. The tax-funded Danish healthcare system provides free and equitable access to rehabilitation, typically delivered through municipalities in a coordinated, multidisciplinary framework. The context is characterised by offering a highly individualised rehabilitation course with a high degree of flexibility concerning intervention site (rehabilitation centre or the client's home), length of intervention course, involved professions and choice of therapeutic approaches. Municipal occupational therapists have no prior experience with CO-OP, which may influence the delivery and fidelity. These contextual characteristics introduce uncertainties which necessitate adaptation of the delivery of CO-OP and a feasibility study prior to a further evaluation of effectiveness. A thorough description of the adaptation and a protocol for a feasibility study have been published.20,21
The objective of the feasibility study reported here was to examine the following feasibility aspects: reach/recruitment, dose, fidelity, perceived value, benefits/harms and potential outcomes of CO-OP applied at a Danish municipal neurorehabilitation centre. 21
Methods
This feasibility study applied a single-group pretest–posttest design and was approved by the local Data Protection Committee (J.nr. 394562). The Regional Ethics Committee classified the study as a quality assurance project with no need for further approval (J. nr. 1-–10-72-1-21). The study protocol, following the Standard Protocol Items: Recommendations for Interventions Trials (SPIRIT) Statement, has been published.21,22 The present report follows the Consolidated Standards of Reporting Trials (CONSORT) statement for pilot and feasibility trials. 23
The study was conducted at a Danish municipal neurorehabilitation Centre between March 2022 and April 2023. Three occupational therapists were trained in the CO-OP approach through a 3-day online workshop offered by ICAN 24 and practised CO-OP delivery before the study started.
The intervention was delivered individually in participants’ homes and at sites in the community such as a local supermarket.
As this was a feasibility study, no formal sample size calculation was conducted; instead, a sample of 20 participants was planned. 21 Stroke survivors were included if aged ≥45 years, living at home, with a Montreal Cognitive Assessment score ≥20, 25 and able to identify two to five occupational performance goals for improvement. Exclusion criteria were severe psychiatric conditions, 26 substance abuse or language barriers.
Participants were recruited consecutively upon referral to the rehabilitation centre by a local coordinator, and written informed consent was obtained prior to participation.
CO-OP consisted of assessment, education and intervention sessions. To ensure consistency, a manual describing the intervention procedures was developed. 21 In line with Danish municipal rehabilitation practice, the frequency and duration of the CO-OP intervention were individually tailored and based on the participant's needs and goals.
Initial assessment (Session 1) was conducted using the Canadian Occupational Performance Measure (COPM).27,28 The participant then identified two to five occupational performance issues that they wanted to improve on. The occupational therapist rated the participant’s a priori performance of the selected occupational performance goals, using the observation-based Performance Quality Rating Scale (PQRS). 29 When performance was not directly observable, ratings were based on participants’ detailed descriptions. 4 Participants then prioritised which goals to work on; typically, one to three goals were selected for intervention, while the remaining goals were left untrained. In the education session (Session 2), each participant was individually taught the metacognitive Goal-Plan-Do-Check strategy, 4 which was used as the main problem-solving framework to facilitate skill acquisition. The educational materials on CO-OP included a visual presentation, a personal binder and goal tracking sheets. 21 In up to seven intervention sessions, each participant worked on one or more of the chosen goals with the occupational therapist who used dynamic performance analysis and guided discovery to support the participant's understanding of performance breakdowns, their plan development and the identification of domain-specific strategies. When the participant was satisfied with the performance of parts of the task being worked on, further parts of the task were addressed, and a new learning cycle began. This was repeated, ideally until goal achievement. Homework was encouraged after each CO-OP session and followed up at the subsequent session. CO-OP could be supplemented with other approaches (e.g. body function training) based on clinical reasoning when considered necessary to support occupational performance.
Data regarding participant characteristics and feasibility aspects were collected using surveys, registration forms, interviews and performance outcome measures. Baseline data included age, gender, stroke location, general health (SF1 from Short Form 36), 30 and self-reported problem-solving ability.
Reach/recruitment: Who accepted and who declined participation was documented by the recruitment coordinator at the neurorehabilitation centre.
Dose: Number and duration of sessions, time spent on CO-OP and supplementary approaches and factors influencing delivery were recorded by the occupational therapists after each session.
Fidelity: After each session, the occupational therapist recorded use of the following essential CO-OP elements: occupation-focused goals, dynamic performance analysis, cognitive strategy use and guided discovery, using dichotomous ratings based on the CO-OP fidelity checklist 4 (see Supplemental material).
Perceived value: Occupational therapists rated meaningfulness of the CO-OP intervention on a 5-point scale after each session and overall relevance at the last session of each participant's intervention on numeric rating scales (0–10). Participants rated their satisfaction (0–10). Perceived value was further explored through individual semi-structured interviews with participants and a group interview with occupational therapists. The individual interviews were conducted primarily by LMN, TLN and a research assistant, while the group interview was moderated by HWHS.
Benefits/harms: Possible unexpected side effects were recorded (yes/no and details) by the occupational therapist at the end of each intervention session.
Potential outcomes: The COPM (performance and satisfaction) and the PQRS27–29 were used to assess occupational performance at baseline and post intervention. The feasibility aspects covered whether both measures could detect possible changes, and whether, specifically, the COPM performance scale could detect possible differences in occupational performance of trained and untrained activities. In addition, the occupational therapists were asked whether each measure was relevant for assessment, using an ordinal 1–5 scale. This was further elaborated on in the abovementioned group interview.
Data analysis of participants’ characteristics was primarily descriptive. Categorical data were presented as frequencies and proportions, and continuous data as means (SD) or medians (IQR).
Reach/recruitment: The proportion of invited stroke survivors who agreed to participate was calculated and presented as a percentage.
Dose: Number of sessions and duration were described using medians and ranges, while time spent on CO-OP was described using means and ranges.
Fidelity: For each of the four essential elements, the proportion of participants receiving the element in at least two-thirds of sessions was calculated. In addition, a joint adherence score was calculated as the proportion of participants to whom all four essential elements were generally delivered, as suggested by Dawson et al. in the CO-OP Fidelity Checklist. 4
Perceived value: Quantitative data were summarised using medians (ranges) or means (SD). Qualitative interviews were transcribed and analysed using deductive content analysis, 31 applying predefined categories of perceived value. For the analysis of perceived values from the perspectives of the participants, one main code ‘perceived value’ with the subcodes ‘positive’, ‘negative’ and ‘neutral’ was applied following Schreier's approach. 31 The coding frame was tested through trial coding by LMN and TLN, after which LMN coded all material. Group interviews with occupational therapists were analysed using the same framework by TLN and HWHS, and findings were summarised across participants.
Benefits/harms: Unexpected events were planned to be described qualitatively.
Potential outcomes: COPM (performance and satisfaction) and PQRS scores were calculated at baseline and post-intervention.27–29 Pre–post differences were analysed using paired t-tests (p < 0.05), including comparisons between trained and untrained goals. Relevance of the measures was summarised descriptively and further explored in the qualitative analyses.
Results
Twenty participants, mean age 67 years, were included; 60% were men. The majority (80%) were living with others. The educational level was evenly distributed on the three levels described in Table 1. Most participants had a stroke in the left hemisphere, and about half of the participants found problem solving somewhat or very difficult. General health status (SF1) was reported as ‘good’ on a scale from ‘excellent’ to ‘poor’.
Baseline participant characteristics (n = 20).
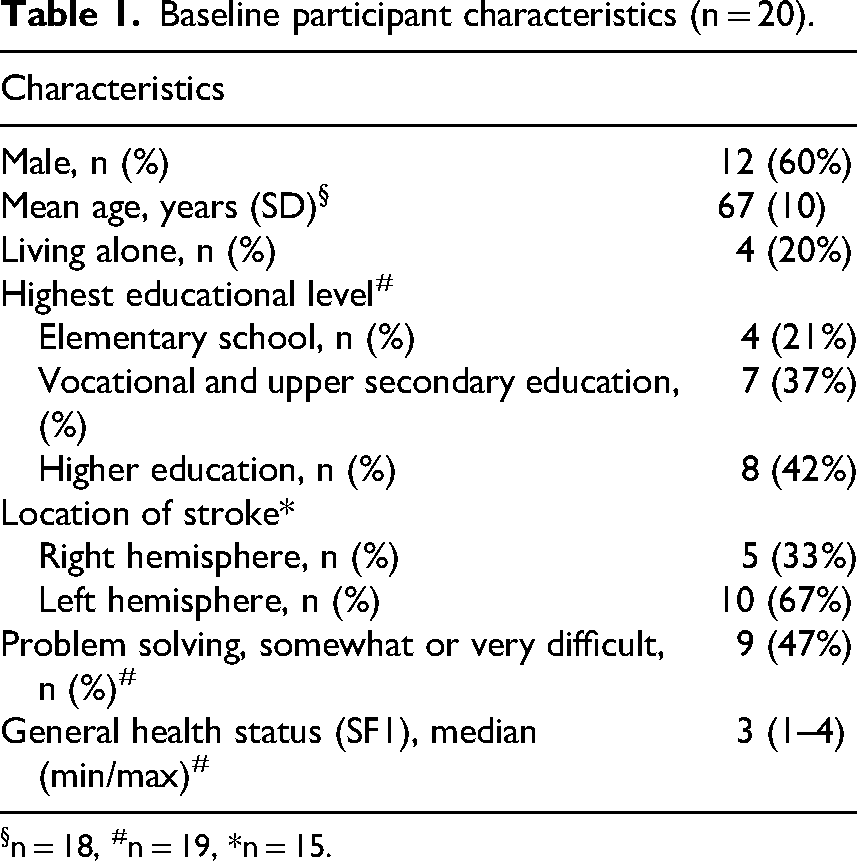
n = 18, #n = 19, *n = 15.
Through COPM, the participants scored a total of 58 occupational performance issues at baseline and again post-intervention. Of these issues, 18 were tasks and activities within self-care (e.g. eating with knife and fork), 11 within productivity (e.g. cooking) and 13 within leisure (e.g. gardening). Sixteen issues were related to general problems described as decreased energy levels, physical symptoms and cognitive problems. The same performance issues were scored on the PQRS by the therapist.
Reach/recruitment: In the enrolment period, 221 stroke survivors met the inclusion criteria. As seen in Figure 1, exclusion mainly took place because some needed only physiotherapy. Of the 152 eligible stroke survivors, 87 were not invited because no CO-OP occupational therapist was available at the time of referral to neurorehabilitation. Of the remaining 65 invited stroke survivors, 20 participants were finally enrolled (30.8%).
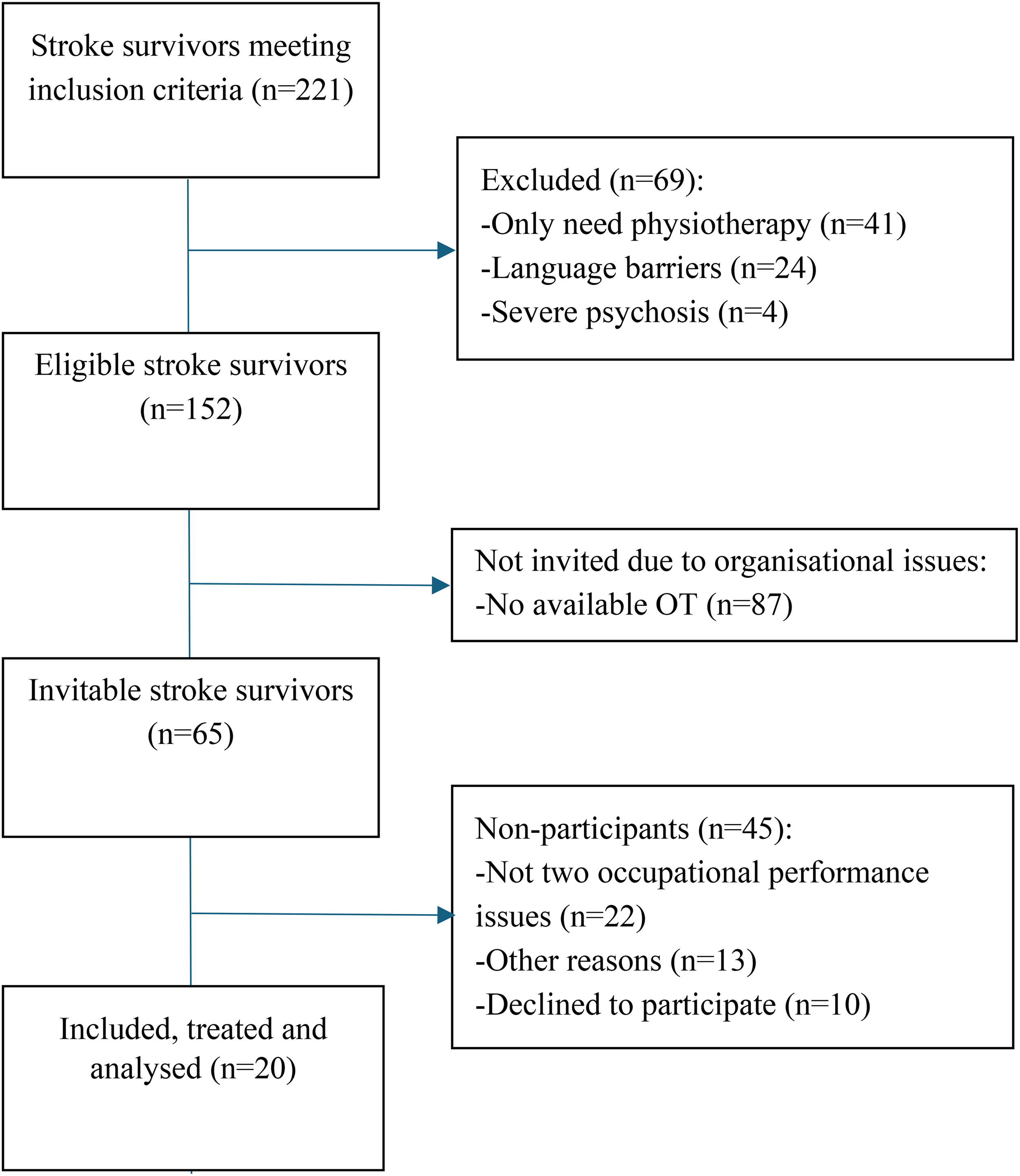
Flow-chart, recruitment.
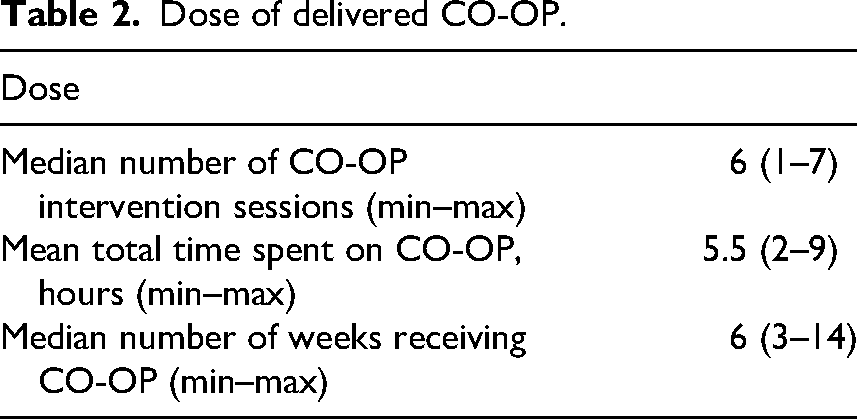
Dose: All participants received sessions 1 and 2 as planned. They had a median number of six CO-OP intervention sessions (min/max one to seven sessions); thus, a large majority received close to the described maximum number of sessions. The mean total time (session 1–9) spent on CO-OP was 5.5 h (min/max 2–9 h). For eight participants, other approaches were included to supplement CO-OP in a total of 13 intervention sessions, lasting between 5 and 35 min. These approaches comprised treatment of oedema, training of muscle strength and sensory specific training. The total delivery period varied from 3 to 14 weeks with a median number of six weeks. In 92% of the sessions, delivery of CO-OP was home-based as planned.
No specific factors facilitating or hindering the delivery of CO-OP were identified (see Table 2).
Dose of delivered CO-OP.
Fidelity: As seen in Table 3, the four essential elements of CO-OP were generally applied to almost all participants. The adherence score was 98.8%.
Fidelity in delivery of essential elements of CO-OP.

Perceived value: The occupational therapists reported CO-OP to be meaningful and generally relevant, and the participants were in general satisfied with the CO-OP intervention (see Table 4).
Participants and occupational therapists’ perspectives on perceived value.

Measured on ten-point scales from no relevance/satisfaction to high relevance/satisfaction.
The participants’ satisfaction with CO-OP was further examined through 18 individual qualitative interviews post-intervention. Most of the participants perceived the CO-OP approach to be of great value. Especially, the use of the Goal-Plan-Do-Check strategy was experienced as meaningful as it provided a simple, structured and motivating approach to address performance issues. As one participant stated: It was very simple, I fully understood what I needed to work on and how I should do it. There was one exception; one participant, who had improved significantly on COPM performance and satisfaction, said that she had difficulty seeing the purpose of CO-OP and indicated that she had profited more from physiotherapy aimed at body functions. The three occupational therapists who participated in the group interview pointed out aspects of the positive value of CO-OP. They found CO-OP supported an occupation-focused therapeutic approach. The participants gained ownership of their plans, and the plans motivated them to do their homework. Many participants expressed satisfaction with the plans they had made and with the fact that they had figured out themselves what to do. Some participants continued working with their plans post-intervention, and some even wanted to make plans to solve new problems. However, the occupational therapists also shared that some participants had negative experiences with the CO-OP process. These participants had expressed that it was too difficult to participate in making the plans; some had become irritated and expressed expectations that the occupational therapist should tell them what to do.
Benefits/harms: No such unexpected side effects were recorded by the occupational therapists.
Potential outcomes: Both the COPM and the PQRS detected changes in occupational performance from baseline to post-intervention; the changes were all statistically significant at p < 0.001 (see Table 5). Change scores on COPM performance concerning trained activities were compared to change scores on untrained activities; no statistical difference was found (p = 0.660), that is, there were significant improvements in both. Concerning the COPM, the median rating of relevance was ‘very highly relevant’, ranging from ‘highly relevant’ to ‘very highly relevant’, whereas the median rating of the PQRS was ‘moderately relevant’, ranging from relevant to ‘very low degree’ to ‘very highly relevant’. In the group interview, the occupational therapists reported that it could be difficult to use the PQRS as it was a novel instrument to them and because some participants had non-observable performance issues. In the latter case, the occupational therapists scored the PQRS after an interview with the participants. They were aware that in this way, the scoring of PQRS was not exclusively done by the professionals but under the influence of the participants’ explanations.
Change in occupational performance measured with COPM and PQRS (n = 20).
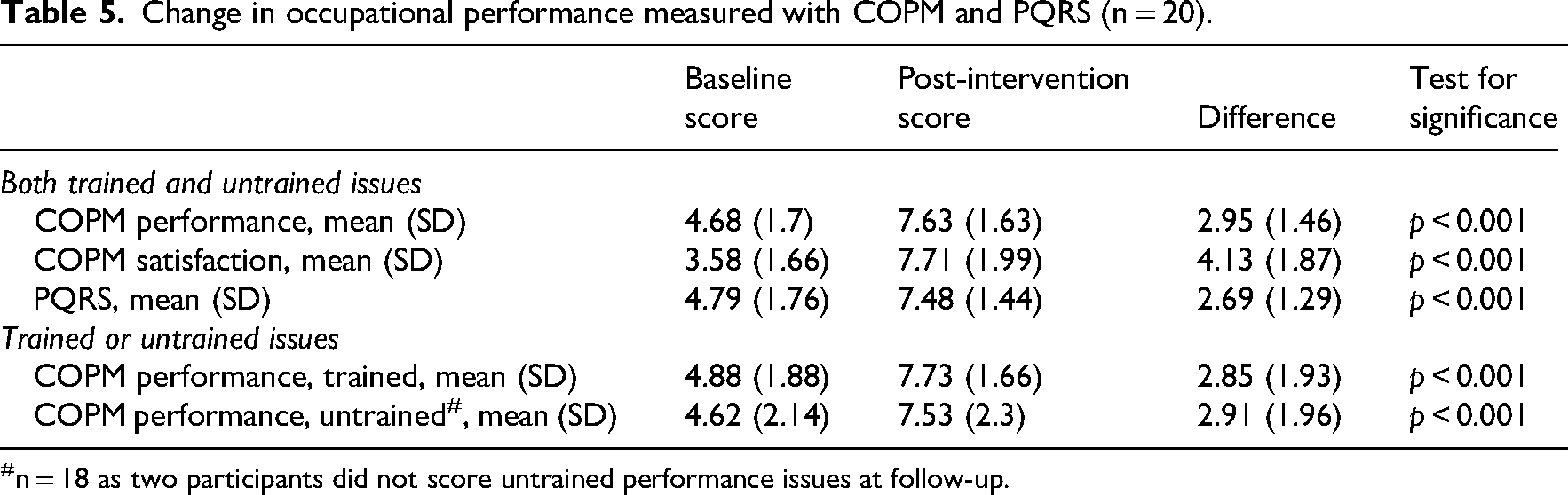
n = 18 as two participants did not score untrained performance issues at follow-up.
Discussion
The objective of this feasibility study was to examine the feasibility aspects: reach/recruitment, dose, fidelity, perceived value, benefits, harms and potential outcomes of CO-OP applied at a Danish municipal neurorehabilitation centre. 21
Reach/recruitment: The intended number of 20 participants was included from 65 stroke survivors who were found to be eligible (recruitment rate 30.7%). In general, recruitment was slow despite broad inclusion criteria and close collaboration between the researchers and the neurorehabilitation centre. A low recruitment rate is not unusual for feasibility studies of comparable interventions; recruitment rates of 30–38% have been reported.9,32,33 The main reason for non-participation in our study was the lack of two performance goals to work on. This was puzzling; however, it could be because enrolment took place very soon after discharge from hospital, and the stroke survivors may not yet have experienced many day-to-day performance issues. Another reason for non-inclusion was that no CO-OP therapist was available during different periods of the recruitment period. This was primarily related to organisational reasons, above all because only three interventionists were trained to deliver CO-OP. This is a lesson learnt for a future study where more attention will be given to organisational adjustments to ease recruitment.
Dose: Participants received a median number of six CO-OP intervention sessions, which is close to the planned maximum number of seven sessions. Stopping before the seventh intervention session was allowed, and 90% did so; the planned maximum number of sessions therefore seemed sufficient for most participants, making CO-OP a relatively inexpensive intervention. However, a future study may allow for an extended period to tailor CO-OP to each participant's individual needs.
Fidelity: The essential elements of CO-OP were delivered with a high degree of fidelity to almost all participants. The occupational therapists did not have a long experience with delivering CO-OP; they were supervised by the project leaders using video recordings of intervention sessions. According to Breitenstein et al., 34 frequent supervision is essential to ensure fidelity as it creates a structured space for clarifying method requirements, correcting misunderstandings early and reinforcing the core components of the intervention. Through feedback and guided reflection, supervisors helped practitioners maintain consistency and avoid unintended adaptations that could weaken the effect of the intervention. While the check of fidelity concentrated on what happened during the CO-OP sessions, it would also have been interesting to know how compliant the participants were concerning their homework. Although it is an intrinsic element of CO-OP that the participants should work on their goals between sessions, it remains unknown how much that took place. Such information could add to our understanding of how CO-OP leads to its intended outcomes, and it seems relevant to assess as part of a process evaluation in future studies.
In this feasibility study, CO-OP replaced the occupational therapists’ usual ways of addressing their clients’ performance issues. The protocol allowed them to supplement CO-OP with more traditional approaches, such as training of body functions, just as they would do during usual practice. This was the case in a small number of sessions. Since no control group participated in the study, we do not know whether the use of other approaches may have increased or decreased when CO-OP was applied. This could, with advantage, have been explored in the group interview with the occupational therapists.
Perceived value: CO-OP was, in general, perceived as meaningful from both participants’ and occupational therapists’ perspectives. However, in the group interview, the occupational therapists reported on participants who had expressed that it was difficult to participate in making the plans and expected that the occupational therapist would provide them with more specific instructions on what to do. In the CO-OP intervention, the therapist's role is to support client-centred learning and promote self-discovery of strategies. This contrasts with a more traditional professional–client relationship where the professional ‘knows best’ and leads the way. Some participants seemingly preferred the ‘old way’, and this emphasises the importance of a thorough explanation of the idea behind CO-OP during and after the educational session.
Potential outcomes: Both the COPM and the PQRS were able to detect significant changes from baseline to post-intervention, thus being sufficiently sensitive for research on the effectiveness of CO-OP. Because both instruments are therapist-led, data collection was ensured from all participants. According to the COPM manual, performance issues that have not yet been experienced in practice cannot be scored. 28 There were, among the 20 participants, all in all 10 performance issues identified through the initial COPM interviews that could not be scored at baseline, as the participants had not yet experienced the performance issue in practice. In these cases, it was not possible to compute a difference between baseline and post intervention. This could potentially impede the sensitivity of the analyses, and this potential problem should be considered in future studies; perhaps, the time schedule should be eased to allow the participants to spend a few extra days or a week performing their activities before scoring them.
No statistical difference was found between improvements in COPM performance of trained and untrained activities, as both improved significantly. This suggests that there was good generalisation and transfer to the untrained tasks. A scoping review by Houldin et al. supports this finding. 19 However, specific research into how well CO-OP supports transfer and generalisation is needed. The PQRS was chosen as a supplement to COPM, due to a wish to include an observation-based instrument and because it had been used in earlier CO-OP studies.6,35 However, the occupational therapists reported difficulties in using the PQRS, especially when some participants had non-observable performance issues. As recommended, 4 the occupational therapists therefore scored the PQRS after interviewing the participants. In this way, the scoring of the PQRS did not exclusively build on the professionals’ direct observation but on participant reports.
Some strengths and limitations of the study should be addressed. Among the strengths, the study was conducted based on, and in accordance with, a published protocol (21), thus ensuring research transparency. No participants dropped out after inclusion, which indicates that they found CO-OP acceptable and relevant. Both quantitative and qualitative data represented the views of participants and occupational therapists and led to broad perspectives on feasibility aspects. Among the limitations, the lack of a control group precludes causal inference, as observed changes in COPM and PQRS scores from baseline to post-intervention may reflect factors other than the CO-OP intervention itself. However, given the feasibility design of the study, effectiveness testing was not a primary objective. Consequently, statistical adjustments for multiple comparisons were not applied, and findings should be interpreted as preliminary and hypothesis-generating.
Another study limitation was that the study was conducted in just one rehabilitation setting with three interventionists delivering the intervention; this increased the risk of not uncovering all challenges. The occupational therapists were responsible for both delivering CO-OP and collecting data. A future full-scale study should have blinded assessors who are not involved in delivering the intervention to ensure unbiased data and independent evaluation of fidelity. The use of occupational therapists’ self-reported adherence to the delivery of the essential CO-OP elements introduces a risk of social desirability bias: the tendency to present one's performance in a favourable light. 36 Such bias can lead clinicians to overestimate adherence to protocol elements or underreport deviations and should be taken into account in future studies where observation-based fidelity checks, as recommended in the CO-OP approach toolkit, should be considered. 4
In conclusion, applying CO-OP to stroke survivors in a Danish municipal neurorehabilitation centre proved feasible. The recruitment period was longer than anticipated, due to organisational issues; these project-inflicted issues are not expected to impede the application of CO-OP in daily practice. Important learnings from the feasibility study should be applied in a future study of effectiveness: To achieve the required sample size within a reasonable recruitment period will require additional strategies, including high availability of CO-OP therapists and time for trying out activities before COPM assessment. Also, it could be considered to include a wider study population to reflect the client base in Danish municipal neurorehabilitation. CO-OP was delivered with a high degree of fidelity; it was perceived as meaningful among both occupational therapists and participants, and the participants improved their occupational performance.
Clinical messages
The Cognitive Orientation to daily Occupational Performance approach was feasible to deliver with high fidelity and perceived meaningfulness.
Findings indicate potential benefits and warrant a full-scale effectiveness study.
The Canadian Occupational Performance Measure and the Performance Quality Rating Scale appeared sensitive to change in trained and untrained activities.
Supplemental Material
sj-docx-1-cre-10.1177_02692155261465889 - Supplemental material for Feasibility of applying the Cognitive Orientation to daily Occupational Performance (CO-OP) approach in a Danish municipal neurorehabilitation context
Supplemental material, sj-docx-1-cre-10.1177_02692155261465889 for Feasibility of applying the Cognitive Orientation to daily Occupational Performance (CO-OP) approach in a Danish municipal neurorehabilitation context by Tove Lise Nielsen, Helene Polatajko, Mette Brandi, Helene Windstrup Holst-Stensborg and Louise Moeldrup Nielsen in Clinical Rehabilitation
Footnotes
Acknowledgements
We thank the participants of the study as well as the occupational therapists who delivered the CO-OP intervention and collected data. Finally, we thank the occupational therapist students who assisted with the transcription of interview data.
Ethical considerations
The Regional Ethics Committee responded that no approval was required as the study was classified as a quality assurance project (J. nr. 1-10-72-1-21). The study was approved by the local Data Protection Committee at VIA University College (J. nr. 394562).
Consent to participate
All participants received oral and written information prior to inclusion in the study. Written consent was obtained from all participants, and anonymity and confidentiality were secured.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Research Foundation of the Danish Occupational Therapy Association (grant number FF1/21-R169-A3906).
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: However, Dr. Polatajko, the creator of the approach, has two books published on the topic and gives workshops on the topic.
Data availability
Data analysed and reported in this study are shared upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.