
Abstract
Objective
To explore lived experience after young-onset stroke.
Design
This embedded qualitative analysis formed part of a larger, ongoing observational follow-up study of young-onset stroke. Using an open-ended prompt at the end of a structured questionnaire, participants were invited to share further insights on their life after stroke. These responses formed the dataset for this qualitative analysis. Two authors developed codes and themes using reflexive thematic analysis, guided by the Biopsychosocial Model, and Coping and Adaptation Theory.
Setting
Telephone, electronic, or postal follow-up assessments were conducted between 13 September 2024 and 13 May 2025 with individuals who had been admitted to the University College London Hospitals Hyperacute Stroke Unit 5–8 years earlier with ischaemic stroke or intracerebral haemorrhage and were aged <55 at the time of stroke.
Participants
Of 127 eligible participants, 80 responded (age range: 20–54 years; 33 females; 65 with ischaemic stroke; 15 with intracerebral haemorrhage).
Results
Four themes emerged: (1) persistent ‘hidden’ disabilities affecting daily life; (2) loss of sense of self and disruption of age-normative roles; (3) systemic gaps in stroke awareness and long-term support; and (4) emotional resilience developed in response to life disruption.
Conclusions
Young-onset stroke has profound and lasting effects, including ‘hidden’ disabilities that remain prevalent years later. Our findings emphasise the need for increased public awareness of young-onset stroke and call for a more holistic, long-term post-stroke care model that supports not only functional recovery but also the restoration of identity and life roles.
Introduction
Stroke is the second-leading cause of death and the third-leading cause of death and disability combined worldwide. 1 Although a high proportion of strokes are potentially preventable (as indicated by declining incidence in older adults), rates are increasing among younger adults.2,3
Previous studies have shown that both functional and non-motor impairments remain prevalent 6 months post-stroke in younger adults (<55 years), with high rates of fatigue (55%), sleep disturbances (46%), and reduced ability to participate in social roles and activities (47%).4,5 Depression and anxiety are also common, affecting 32% and 35% of younger stroke patients respectively. 5 Many of these individuals are in their most economically productive and demanding years of employment, yet 44% of working-age adults have not returned to the workforce 1.5 years post-stroke. 6 The resulting productivity losses are considerable, with premature death and lost working days estimated to cost approximately €12 billion annually across Europe. 7 In the United Kingdom, the total societal cost of stroke is approximately £26 billion per year. Notably, £20.6 billion of this cost is attributable to ongoing care, highlighting long-term support needs beyond the acute phase after stroke. 8
Despite this emerging trend, stroke research continues to focus largely on older populations.9–12 Furthermore, long-term disability is often described primarily in terms of motor and language impairments, with less attention paid to cognitive, emotional, and psychosocial consequences. Clinical guidelines increasingly emphasise the importance of patient-centred care, 13 although the evidence base informing these recommendations is largely derived from older stroke populations. The needs and priorities of younger stroke patients may be unique, focusing on family responsibilities, relationships, career pressures, and financial stability.13,14 Most of the existing literature on stroke in younger individuals has used quantitative instruments to evaluate outcomes, with limited qualitative data capturing long-term lived experience.15–17 This is a significant gap, given the lasting impact stroke can have on young people's lives. Qualitative research allows for a flexible, inductive exploration of meaning and experience, making it well-suited to understanding the daily realities of stroke from the perspective of younger adults and providing insights that may not arise through quantitative methods. 18
To address this gap, we established the University College London Young Stroke Systematic Evaluation Study (ULYSSES), a cohort study of individuals who were admitted to the University College London Hospitals Hyperacute Stroke Unit 5–8 years earlier with ischaemic stroke or intracerebral haemorrhage and were aged <55 at the time of stroke. In this embedded qualitative sub-study, we aimed to explore the long-term lived experience of young-onset stroke in the United Kingdom. This qualitative component was designed as a complementary approach to capture patient-reported lived experience alongside structured quantitative outcomes.
Methods
Study design and setting
ULYSSES is a prospective, observational, hospital-based cohort study investigating the causes and consequences of stroke in young adults. 4
The cohort included consecutive young adults (<55 years old) admitted to the University College London Hospitals Hyperacute Stroke Unit between 1 January 2017 and 1 January 2020 with a clinical diagnosis of acute ischaemic stroke or intracerebral haemorrhage. The University College London Hospitals Hyperacute Stroke Unit provides specialised stroke care to an ethnically diverse population of approximately 1.6 million people from across five North Central London boroughs.
Ethical approval and informed consent
ULYSSES is a sub-study of the Stroke Investigation Group in North And central London (SIGNAL) registry. The SIGNAL registry was approved by the University College London Hospitals NHS Foundation Trust Governance Review Board as an ongoing service evaluation of a comprehensive clinical care programme (reference: 5-201920-SE). Additional ethical approval for long-term follow-up of registry participants was obtained from the London South-East Research Ethics Committee (reference: 24/LO/0368). Written informed consent was obtained from all participants included in this study.
Data collection
Data collection was conducted by a multidisciplinary team of trained female research practitioners, including two registered nurses (Siobhan McLernon, Charlotte Willett), one neurologist (Iryna Klopotovska), and two clinical research assistants (Raafiah Mussa, Mila Penzel). All team members had experience working with people with neurological conditions. Data collection was supervised by senior clinical academics with expertise in stroke research and qualitative methodologies (Siobhan McLernon, Calvin R. Moorley). No prior relationships were established between participants and the researchers before the interviews. The research team remained aware of their clinical backgrounds and personal perspectives throughout the research process.
Participants were invited to take part in a follow-up assessment 5–8 years after hospital discharge that included a quantitative component including validated measures covering domains such as anxiety, depression, fatigue, sleep disturbances, pain, sexual dysfunction, return to work, and cognitive impairment, and a qualitative component. At the end of the structured questionnaire, participants were invited to respond to a single open-ended prompt: ‘Please share any further experiences or feedback about your life or lived experience after stroke’. These responses were optional and unstructured, allowing participants to express their lived experiences. No additional prompts or probing questions were used. The questionnaire was piloted with three young people who had experienced a stroke, and feedback was received from a person with lived experience of young stroke to inform questionnaire wording and design.
Although the broader ULYSSES study is ongoing, with a target sample size of 552 participants, this qualitative sub-study was conducted as part of an interim analysis. At the time of analysis, 127 participants had been followed up, of whom 80 provided responses to the open-ended question regarding life after stroke. Analysis of the quantitative component is ongoing and will be reported separately.
Assessments were conducted primarily via telephone; however, postal and electronic questionnaires were also offered to maximise response rates and reduce participant burden by allowing individuals to complete assessments using their preferred method. These alternative approaches also improved accessibility for participants with communication difficulties or significant functional disability (i.e. modified Rankin Scale score 4–5). The same open-ended question was used across all modes of administration.
The open-ended spoken responses were recorded verbatim by the researcher in real time as part of the follow-up assessment and entered directly into an electronic data collection form; no audio recordings were made, and therefore, no transcription was required.
As part of maintaining rigour, the study team regularly reviewed free-text responses to monitor data quality and depth, and to refine codes and themes. Through this process, we identified recurring patterns across participants’ responses. This provided justification for conducting a qualitative analysis at this stage and for sharing the findings with the wider stroke research community, due to their urgent relevance to understanding life after young-onset stroke and in recognition of participants’ valuable contributions.
Data analysis
This study used a sequential inductive-deductive approach to reflexive thematic analysis. Initially, two researchers (Raafiah Mussa, Siobhan McLernon) analysed the data inductively using Braun and Clarke's reflexive thematic analysis framework 19 to identify patterns of meaning across participants’ responses. Themes were developed through close engagement with the data and through researchers’ interpretive and reflexive engagement with participants’ accounts.
Following agreement on the preliminary themes within the research team, a deductive analytic process was undertaken in which the themes were interpreted and organised using a combined theoretical framework comprising the Biopsychosocial Model 20 and Coping and Adaptation Theory. 21 The theoretical frameworks were, therefore, not used to generate codes or themes during the initial inductive analysis, but rather to support interpretation, contextualisation, and development of a coherent understanding of participants lived experiences after young stroke. Further details on the study's theoretical framework and its ontological and epistemological positioning are provided in the Supplementary Material.
Reflexive thematic analysis emphasises researcher subjectivity as a resource rather than a limitation. Using this approach allowed us to remain aware of our perspectives (i.e. areas of familiarity and potential bias) while staying focused on the research question and remaining closely engaged with participants’ responses. Having two researchers involved facilitated discussion, reflexive interpretation, and refinement of themes. No qualitative software was used; coding was conducted manually using Microsoft Excel.
Results
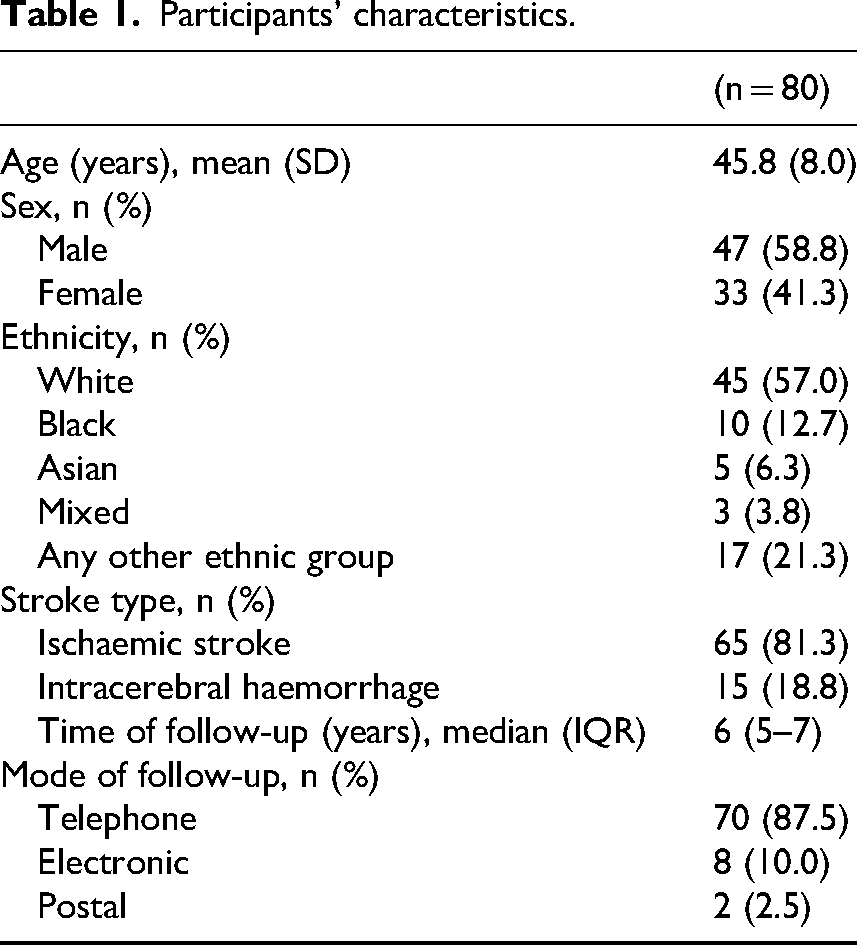
A total of 127 individuals who had a stroke at age <55 years and had previously presented to our service were contacted for follow-up between 13 September 2024 and 13 May 2025, of whom 80 participants responded to the open-ended prompt about their lived experience after stroke. Follow-up was conducted via telephone (n = 70), postal questionnaire (n = 2), and electronic questionnaire (n = 8). The age range was 20–54 years, and the mean age at time of stroke was 46 years (SD ±8.0). 33 (41%) participants were female. 65 (81%) participants had an ischaemic stroke, and 15 (19%) had an intracerebral haemorrhage. Median time to follow-up was 6 years (IQR 5–7). Participants’ characteristics are summarised in Table 1.
Participants’ characteristics.
Four themes representing the lived experience of young-onset stroke were formed: (1) persistent ‘hidden’ disabilities affecting daily life; (2) loss of sense of self and disruption of age-normative roles; (3) systemic gaps in stroke awareness and long-term support; and (4) emotional resilience developed in response to life disruption.
Theme 1: Persistent ‘hidden’ disabilities affecting daily life
Persistent ‘hidden’ disabilities (i.e. consequences of stroke that are not readily visible to other people) affecting daily life were a prominent theme, with many participants describing a range of hidden symptoms (often in addition to physical disabilities) that continued to impact their quality of life many years after their stroke event.
Fatigue was one of the most frequently reported ‘hidden’ symptoms and was described as unpredictable and debilitating, limiting the ability to socialise or complete basic activities of daily living: “I do my daily tasks in intervals as I do not have the strength or energy to perform them one after the other. I must sit for at least 15 minutes before I tackle the next.”
– Participant 482; female; 54 years old at time of stroke; ischaemic stroke; 6 years since stroke
Cognitive symptoms (mainly memory problems, difficulty concentrating, reduced processing speed, and challenges with multitasking) were also common and were described as frustrating, limiting, and affecting day-to-day functioning. “The main problem after stroke is reduced ability to concentrate. It doesn’t bother me every day, just when I am in a high-stress situation.”
– Participant 268; male; 28 years old at time of stroke; ischaemic stroke; 6 years since stroke
Several participants reported that cognitive difficulties affected their ability to concentrate and communicate in everyday and work-related situations, particularly when there was background noise or other distractions: “[I] would not be able to concentrate or talk on the phone if there was noise in the background.”
– Participant 329; female; 46 years old at time of stroke; ischaemic stroke; 7 years since stroke
Sensory changes were also frequently reported, including tingling in the limbs or face, pins and needles, noise and smell sensitivity, and feeling persistently cold. Some participants struggled in crowded settings or relied on noise-cancelling devices to cope: “There are a lot of food or drinks I used to love that I can’t stomach now. I used to love orange juice, now the smell makes me gag… [I am] so sensitive to noise and smells. I wear headphones a lot.”
– Participant 89; female; 24 years old at time of stroke; ischaemic stroke; 5 years since stroke
“[I experience] sensations of weird tingling in the left side of my face [that get] worse in cold weather, and in my arm and leg that have been present since stroke…”
– Participant 104; female; 45 years old at time of stroke; ischaemic stroke; 5 years since stroke
Others experienced ongoing pain, vestibular dysfunction (e.g. vertigo, problems with balance, poor coordination and orientation, particularly in tight or busy spaces), and visual disturbances (including double vision and peripheral vision loss), all of which significantly disrupted daily routines: “When I cycle now it is a bit more dangerous than before because I have a permanent blind spot and when I look at things, I can miss things on the left side of my periphery. Also, everything seems a bit dimmer than before.”
– Participant 361; male; 41 years old at time of stroke; ischaemic stroke; 6 years since stroke
Emotional and psychological symptoms were also commonly reported, with one participant describing: “…a constant daily battle on mental health…”
– Participant 338; male; 35 years old at time of stroke; ischaemic stroke; 7 years since stroke
Anxiety was prevalent and often related to a fear of recurrence. One participant shared how they had become more restrained or risk-averse since their stroke. “Before stroke [I] was very adventurous, but now [I am] more restrained… [I] approach life more carefully…”
– Participant 404; male; 39 years old at time of stroke; ischaemic stroke; 6 years since stroke
Another participant, who was a parent to a young child, described post-traumatic stress-like symptoms, including flashbacks and panic attacks relating to a fear of dying and the effect this would have on their young family. For some, these psychological effects did not arise immediately but surfaced years later. One participant, for example, reflected on how they had returned to work quickly after their stroke, only to find themselves confronting the trauma of what had occurred much later: “[I] remember being admitted and wanting to get out of hospital as soon as possible. [I] feel [I] didn’t deal with the trauma of what happened at the time of stroke. In hindsight, [I] realise [I] was very depressed after stroke… [I am] still dealing with the trauma of what happened.”
– Participant 552; male; 49 years old at time of stroke; intracerebral haemorrhage; 6 years since stroke
Some participants mentioned that their personality had changed to become more introverted or that they could no longer ‘mask’ their feelings as they once had: “I think the stroke made me lose my ability to mask my feelings. I'm more irritable when things are loud, or things don’t go to plan. If the pain is too much, I sometimes just shut down.”
– Participant 89; female; 24 years old at time of stroke; ischaemic stroke; 5 years since stroke
In addition to some participants describing shutting down as a psychological coping mechanism, others described the physical impact of the body shutting down due to stroke: “[My] body is shutting down and getting worse over the last years in particular, like a broken car.”
– Participant 172; male; 46 years old at time of stroke; intracerebral haemorrhage; 7 years since stroke
In some cases, despite complete physical recovery, individuals still reported hidden disabilities that impacted their well-being and affected aspects of working life, such as difficulty with processing, language, and speech: “When I can’t get the words out, I get really upset with myself.”
– Participant 532; male; 51 years old at time of stroke; ischaemic stroke; 5 years since stroke
Over time, the accumulation of such difficulties, particularly when poorly understood by others, contributed to emotional burden, diminished self-esteem, and feelings of isolation. Some participants expressed a sense of low self-worth: “I can’t think for myself. I constantly feel like that I don’t matter. I have things on my mind, but I have trouble saying them. They can’t come out.”
– Participant 322; female; 53 years old at time of stroke; ischaemic stroke; 8 years since stroke
Theme 2: Loss of sense of self and disruption of age-normative roles
Several people shared that they were no longer able to return to work due to ongoing physical or cognitive impairments. These disruptions to employment were often accompanied by financial stress and a sense of purposelessness, with one individual stating they felt as though they had ‘wasted’ their life. One participant who had adapted to a life on long-term disability benefits described feeling like they were as follows: “…on the outside looking in…”
– Participant 174; male; 53 years old at time of stroke; ischaemic stroke; 6 years since stroke
Some participants described being physically mobile but emotionally withdrawn, saying they no longer recognised themselves. Others reported becoming more reclusive: “I died the day I had stroke… it's not me anymore. I don’t want to go out. I am terrified. I am not me… I am now a recluse and don’t go out anymore.”
– Participant 53; female; 50 years old at time of stroke; ischaemic stroke; 5 years since stroke
One individual shared that one of the hardest parts of stroke recovery was not being able to socialise with others as they had before: “After stroke, I feel awkward in the same socialising activity… I don’t know how to explain it properly. I try to do everything the same, but it seems weird for me…”
– Participant 268; male; 28 years old at time of stroke; ischaemic stroke; 6 years since stroke
Some reported feeling increasingly isolated as they watched peers progress through age-normative milestones or roles that they were not able to partake in. One participant noted a change in how they were treated within their social circle, highlighting how shifts in social dynamics can compound feelings of loss: “…people changed towards me [and] treated me differently.”
– Participant 415; male; 51 years old at time of stroke; ischaemic stroke; 6 years since stroke
Other participants described a longing to return to the person they once were: “I wish I could be me again and swing my hips and go out… I am recluse… I don’t wish stroke on my worst enemies.”
– Participant 53; female; 50 years old at time of stroke; ischaemic stroke; 5 years since stroke
Overall, feelings of isolation, altered identity, and a sense of being fundamentally changed were common, even years after the event.
Theme 3: Systemic gaps in stroke awareness and long-term support
While the acute phase of stroke care was generally perceived as prompt and effective, several participants reported feeling unsupported or even dismissed by the healthcare system during the long-term recovery process, often describing being left to navigate ongoing symptoms largely on their own: “I would just like to thank the NHS for all their help on the day I had the stroke and the following days in hospital. I do feel the aftercare offered was virtually non-existent however and this is basically the first time I have spoken to anyone from the NHS (GP excepted) about how I feel.”
– Participant 390; male; 53 years old at time of stroke; ischaemic stroke; 7 years since stroke
Some participants reported receiving little to no long-term follow-up, with particularly limited access to support for ongoing psychological challenges: “I feel very strongly that stroke patients do not receive enough support in respect of the mental issues associated and required to help overcome obstacles that are vital to recovering from the stroke… patients should be helped acknowledge that there is a mental battle to be had towards recovery as much as physical. Physiotherapy should be accompanied by psychology and lessons in overcoming mental trauma.”
– Participant 400; male; 53 years old at time of stroke; intracerebral haemorrhage; 6 years since stroke
Some participants noted that most available information was geared towards older adults and signalled that stroke information for all ages is needed: “In general, I believe there is enough information about stroke, but all information [is] about old people and not enough about stroke in young people.”
– Participant 23; female; 31 years old at time of stroke; ischaemic stroke; 8 years since stroke
Overall, these accounts reflected a consistent perception of fragmented and insufficient long-term systemic care, with many participants emphasising the need for ongoing support that addressed the wide-ranging and persistent impacts of stroke.
Theme 4: Emotional resilience developed in response to life disruption
Despite ongoing physical, cognitive, or emotional challenges, many participants described a shift in perspective, expressing gratitude for survival and a renewed appreciation for life. This response shift often reflected a reframing of expectations and the development of a “new normal,” where participants acknowledged their limitations but focused on progress and recovery. For example, a participant described that despite them and their partner being worried about the future and experiencing anxiety, they stay optimistic and are grateful that they are not worse off: “The stroke has changed me. I'm more reserved and my anxiety overtakes me… but how lucky I am that I'm still here. I’m lucky to be here for my family, my daughters…”
– Participant 338; male; 35 years old at time of stroke; ischaemic stroke; 7 years since stroke
With optimism came resilience and determination to recover: “I spent 2 weeks in hospital, very immobile. Once I returned home, I was determined to return to normal. My only problem I had was my balance, however, I persevered and within 3–4 months, I returned to my work as a hairdresser and Pilates instructor.”
– Participant 552; male; 49 years old at time of stroke; intracerebral haemorrhage; 6 years since stroke
Not all experiences were characterised by ongoing difficulties; some participants described a full recovery and expressed gratitude for the care they received: “I have fully recovered; the care I received was excellent; because of the stroke the hole in my heart was discovered and repaired—so maybe I should see it as a lucky outcome!”
– Participant 485; male; 54 years old at time of stroke; ischaemic stroke; 6 years since stroke
Several participants described healthier habits, increased self-awareness, or a more mindful approach to living as outcomes of their recovery: “I recovered fully and would say that as a result of the stroke, it has changed my outlook on life in a very positive way. Do more, look after myself more etc. For me it had very little mid- or long-term impact if any, which I think was quite lucky!”
– Participant 158; male; 23 years old at time of stroke; ischaemic stroke; 6 years since stroke
Several individuals spoke about easing themselves back into former activities, maintaining a positive mindset, or setting new goals for recovery: “Stroke is a life changing event. You have to push yourself to get better… don’t let it drag you down.”
– Participant 415; male; 51 years old at time of stroke; ischaemic stroke; 6 years since stroke
In some cases, post-stroke mental health was seen as a necessary battle: “I am convinced that without the mental positivity battle, I would not have recovered as well as I have. Yes, I still carry scars, but it has not been without a fight.”
– Participant 400; male; 53 years old at time of stroke; intracerebral haemorrhage; 6 years since stroke
Others highlighted the importance of connection with family, peers, or support networks, which helped foster a sense of meaning and belonging post-stroke: “…the stroke on a good note has allowed me to connect with a lot of family members or people who’ve had strokes.”
– Participant 89; female; 24 years old at time of stroke; ischaemic stroke; 5 years since stroke
Overall, participants expressed a deep sense of gratefulness for having survived, with many framing the stroke as a turning point or ‘wake-up call’ that led to personal growth, lifestyle changes, or a renewed appreciation for life.
Discussion
Our findings extend existing knowledge about young-onset stroke by providing insight into lived experience after hospital discharge, particularly persisting symptoms and the lack of age-appropriate support. Few qualitative studies have focused exclusively on recovery 5–8 years post-stroke.15–17,22–24 Examining this later stage with a relatively large and diverse sample highlights ongoing physical, cognitive, and psychosocial impairments well beyond the acute phase, with some participants reporting symptoms that worsened or accumulated over time. These long-term challenges are often overlooked in clinical care and research, particularly in younger individuals who are assumed to have ‘recovered’.
Many participants experienced a high burden of persistent, often ‘hidden’, non-motor outcomes, including fatigue, cognitive impairment, emotional lability, sensory disturbances, sexual dysfunction, pain, and bowel and bladder dysfunction. These findings highlight limitations of conventional outcome measures (such as the modified Rankin Scale), which overlook the broader impact of stroke on quality of life.25,26 In line with the Biopsychosocial Model, these ‘hidden’ disabilities negatively affected emotional well-being, social roles, and overall life satisfaction. 20
The variation in outcome timing and trajectory challenges current stroke service provision, which typically concentrates on the acute phase. National Institute for Health and Care Excellence guidelines recommend follow-up at 6 months, 13 yet our findings suggest that assessment and rehabilitation should be extended well beyond this, consistent with evidence of neuroplasticity and adaptation beyond the early ‘critical window’. 27
The persistence of ‘hidden’ symptoms significantly impacted participants’ social relationships and ability to engage in activities central to their identity. Symptoms were often misunderstood or dismissed by others, adding to psychological distress, self-stigma, and social isolation. Several participants became more aware of their impairments when unable to participate in valued leisure, work, and social activities, contributing to a sense of loss and withdrawal. These experiences align with previous studies, where individuals reported distancing themselves from others either to avoid reminders of their former selves or to protect loved ones from the burden of their new limitations and changing relationship dynamics.16,22 Similar patterns have been observed in people with acquired brain injury, where changes in self-perception and social functioning lead to social withdrawal. 28 These findings also align with Charmaz's ‘loss of self’ concept, 29 whereby individuals with long-term illnesses struggle to construct new, equally valued identities, causing them to lead a more restricted life, experience social isolation, and fear becoming a burden to others. Indeed, many participants described withdrawing from social connection because these interactions served as painful reminders of lost lives, roles, and relationships. Together, these findings highlight the importance of interventions that address not only physical, cognitive, and emotional symptoms but also the social consequences of stroke, including loneliness, isolation, and identity disruption.
Furthermore, stroke often resulted in a departure from planned life trajectories in relationships, parenting, employment, or social life, creating profound identity shifts. These findings align with Lazarus and Folkman's Coping and Adaptation Theory, which highlights the role of cognitive appraisal in adjusting to chronic illness. 21 Participants grieved not only physical loss but also struggled to adapt to versions of themselves no longer aligned with personal or societal expectations. Rehabilitation should, therefore, include interventions designed for younger adults that promote community reintegration, and, where possible, return to pre-stroke roles and identity. 13
Unemployment and financial strain were common, potentially affecting sense of self and quality of life, consistent with previous studies showing that some young people associate self-worth with productivity.6,22,30,31 Employment provides routine, social interaction, and meaningful contribution, all of which are central to personal identity.16,32,33 For some, returning to work represents a return to the pre-stroke self, allowing minimisation of the stroke's significance. 32 Barriers to return to work, including cognitive deficits, fatigue, and inadequate workplace support, are potentially modifiable through tailored vocational rehabilitation.6,32,34 In the United Kingdom, 15% of stroke patients experience workplace discrimination or missed promotions, and one in ten report unsupportive employers. 35 Insufficient understanding of the hidden effects of stroke often leads to insufficient reasonable adjustments.36,37 Tailored vocational support should, therefore, be central to post-stroke care for working-age adults.
While many participants described persistent long-term impacts of stroke, some reported what they perceived as a full recovery or little to no ongoing impact, with such responses characterised by emotional resilience through adaptation, identity reconstruction, and reframing. This psychological adjustment was closely linked to self-efficacy, which influences motivation, coping, and engagement in rehabilitation and is increasingly recognised as essential to meaningful recovery. 35 Accordingly, support services that facilitate return to work and participation in meaningful activities should be more readily available, particularly for younger stroke patients navigating ongoing vocational and social challenges.
Our study has strengths and limitations. It addresses a key gap by exploring long-term recovery from the perspective of individuals with young-onset stroke. The open-ended prompt allowed participants to discuss personally meaningful challenges. However, retrospective accounts may be affected by recall bias or response bias (i.e. individuals with more ongoing difficulties being more likely to participate with detailed free-text responses). In addition, experiences may differ from non-responders, possibly under- or overestimating the true extent of the problem. As this study reports an embedded qualitative component of a larger cohort study, detailed clinical demographic data were not collected, limiting our ability to explore the influence of clinical characteristics on reported lived experiences.
In conclusion, younger stroke patients face long-term, complex challenges extending well beyond the acute phase of recovery, involving ‘hidden’ disabilities, disrupted identities, gaps in support systems, and ongoing adaptation. Guided by the Biopsychosocial Model and Coping and Adaptation Theory frameworks, our findings emphasise the need to strengthen secondary rehabilitation and improve long-term follow-up, with a need for more holistic and better coordinated care that supports recovery of identity, meaning, and life roles, that can be sustained over time. Collectively, these measures may help support not only clinical recovery but also psychosocial reintegration, identity restoration, and long-term well-being post-stroke.
Hidden cognitive, emotional, and psychosocial difficulties may persist for many years after young-onset stroke. Long-term follow-up should extend beyond physical recovery to include psychological, social, and vocational needs. Stroke-related changes in identity and social participation remain important long-term rehabilitation concerns. Younger stroke patients may benefit from age-appropriate peer and community support.
Supplemental Material
sj-docx-1-cre-10.1177_02692155261467644 - Supplemental material for A qualitative study of lived experience 5–8 years after young-onset stroke: UCL Young Stroke Systematic Evaluation Study (ULYSSES)
Supplemental material, sj-docx-1-cre-10.1177_02692155261467644 for A qualitative study of lived experience 5–8 years after young-onset stroke: UCL Young Stroke Systematic Evaluation Study (ULYSSES) by Raafiah Mussa, Siobhan McLernon, Calvin R. Moorley, Iryna Klopotovska, Hatice Ozkan, Mila Penzel, Charlotte Willett, Robert Simister, Arvind Chandratheva and David J. Werring in Clinical Rehabilitation
Footnotes
Acknowledgements
The authors would like to thank all the participants for sharing their lived experience of stroke. We are also grateful to Yee Chin Lee, Riham Muhammed, and Diana Wong Ramos for their valuable contributions in supporting and facilitating this study.
Ethical approval and informed consent
ULYSSES is a sub-study of the SIGNAL registry. The SIGNAL registry was approved by the UCLH NHS Foundation Trust Governance Review Board as an ongoing service evaluation of a comprehensive clinical care programme (reference: 5-201920-SE). Additional ethical approval for long-term follow-up of registry participants was obtained from the London South-East Research Ethics Committee (reference: 24/LO/0368). Written informed consent was obtained from all participants included in this study.
Author contributions
RM, SML, CRM, HO, RS, AC, and DJW contributed to study concept or design; RM, SML, IK, MP, and CW contributed to a major role in the acquisition of data; RM, SML, and CRM contributed to analysis or interpretation of data. All authors revised the manuscript for content and approved the final version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The SIGNAL registry was funded by the National Institute for Health and Care Research UCLH Biomedical Research Centre.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Due to the sensitive nature of the qualitative data and participant confidentiality, the full dataset cannot be shared. Relevant excerpts supporting the study's findings are included within the article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.