
Abstract
Introduction
In the past decade, there has been a great deal of interest in the place where people die, with a view to improving choice and adequately planning care for terminally ill patients.1–3 Although about two thirds of people prefer to die at home,4,5 secular trends towards an institutionalised dying have been reported in many developed world regions.6–8 In England and Wales, the number of deaths at home nearly halved from 1974 to 2003. Projections suggested that if this trend continued, fewer than one in 10 people would die at home by 2030. 9 The present paper examines trends in place of death in England and Wales from 2004 to 2010 to determine whether there were any changes from previous trends.
Methods
Data source
The British Office for National Statistics (ONS) collects and analyses death registration information and makes this publicly available free of charge in annual tables with aggregated information. 10 These include data on place of death. We extracted data on all decedents in England and Wales from 2004 to 2010. Although the ONS has changed its coding for the 2010 datasets, the ONS team has kindly provided the 2010 data with the old coding to allow comparisons with previous years.
Outcome measure
Place of death was classified by the ONS in six main categories: (1) at home; (2) psychiatric hospitals; (3) inpatient hospices; (4) hospitals and communal establishments for the care of the sick (divided into National Health Service (NHS) and non-NHS facilities); (5) other communal establishments (which include aged persons’ accommodation, rehabilitation centres and other communal facilities, such as assessment centres, holiday homes and hotels, schools and prisons); and (6) other private houses and other places (called elsewhere). There were no changes in this classification during the seven-year period examined. For the purpose of this analysis, the category of NHS hospitals and communal establishments for the care of the sick was shortened to NHS hospitals and nursing homes (note, however, that this included NHS hospital palliative care units), and all deaths occurring in places other than home were called institutional deaths, except for deaths coded in the elsewhere category.
Analysis
We analysed trends in place of death by gender, seven age groups and separately for cancer and non-cancer deaths (cancer deaths identified through ICD-10 codes C00-D48).Yearly and seven-year changes were calculated in both percentages and absolute numbers of deaths. Proportions of deaths at home were standardised by age and gender according to the distribution in 1974 (to enable comparisons with standardised proportions previously calculated for 1974–2003). 9 . Since the data represent 100% of our population of interest and no sample was drawn, inferential statistics were not applied. 11
Results
More home deaths amongst fewer deaths
Between 2004 and 2010 over three and a half million people died in England and Wales. During this time period the annual number of deaths fell by 3.8%. Home deaths increased slowly but steadily, from 18.3% in 2004 to 20.8% in 2010. The increase was seen in both proportions and absolute numbers – the latter increased by 9.1% (Table 1). The rise was more pronounced in cancer than in non-cancer deaths (Figure 1) and was more evident when ageing was accounted for (age–gender standardised home death proportions were 20.6% in 2004, 20.7% in 2005, 21.3% in 2006, 22.0% in 2007, 22.5% in 2008, 22.9% in 2009 and 23.5% in 2010).
Place of death in England and Wales 2004–2010 a
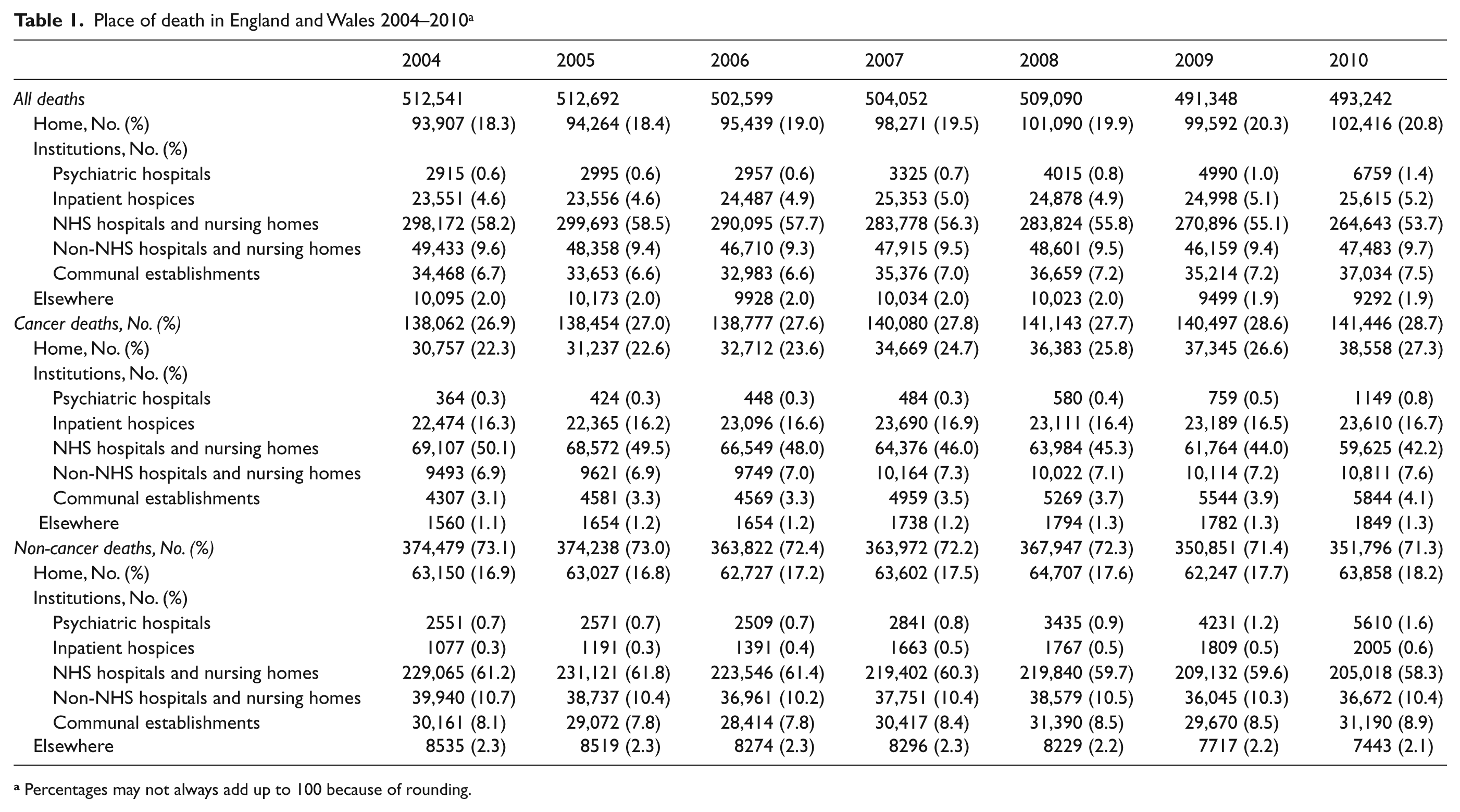
Percentages may not always add up to 100 because of rounding.
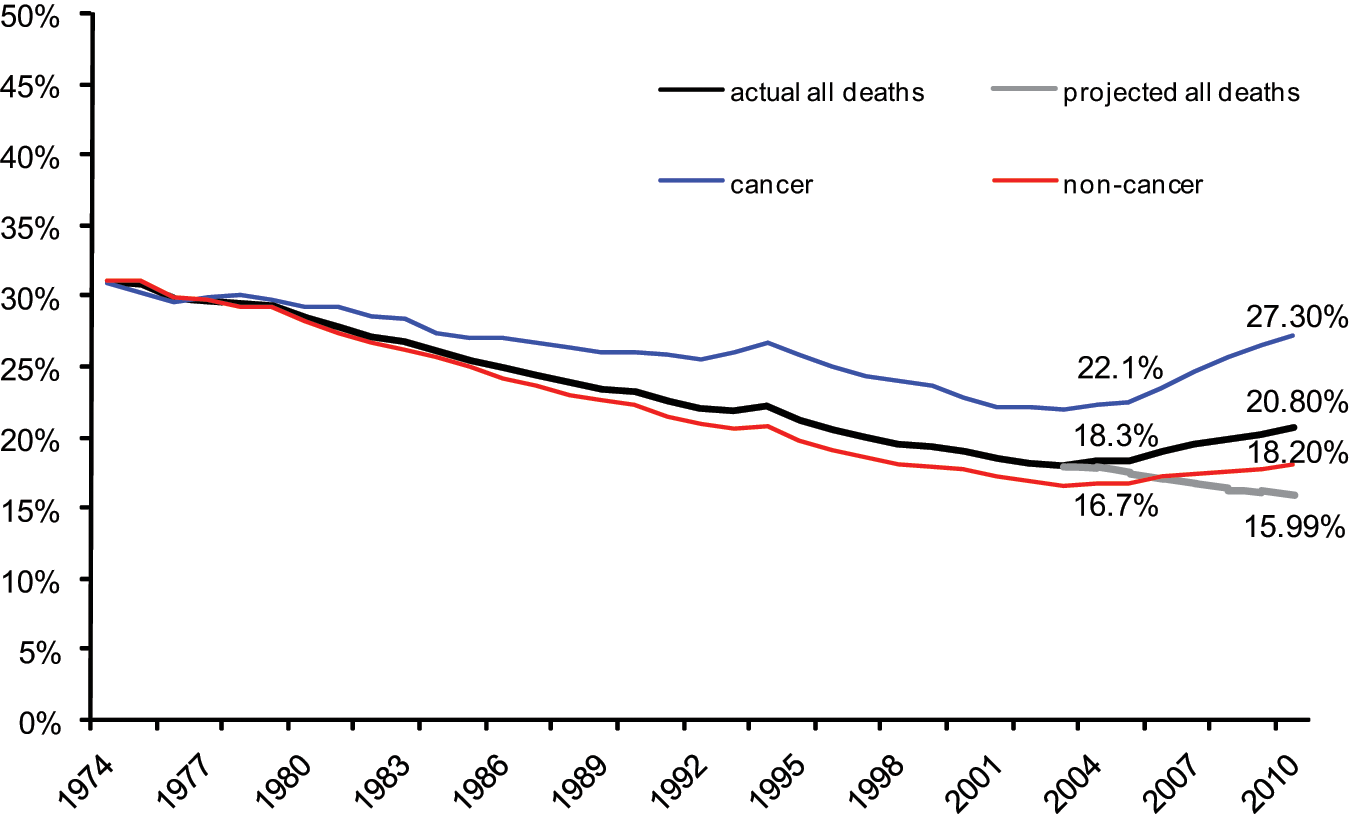
Proportion of home deaths in England and Wales 1974–2010. Actual place of death provided by the Office for National Statistics; 1999–2003 based projections by Gomes and Higginson. 9 Percentages shown within the graph refer to 2003 (actual data for all deaths, cancer and non-cancer deaths) and to 2010 (including both actual and projected data).
As home deaths increased, there was a reduction in the proportion of deaths in hospitals and nursing homes (4.5% in NHS facilities, while there was a 0.1% increase in non-NHS facilities). This was seen in both cancer and non-cancer, except for cancer deaths in non-NHS facilities (Table 1). We also observed a small increase in the proportion of deaths taking place in other communal establishments, although the increase was small and difficult to interpret, as this category included a wide variety of places. The proportion of deaths taking place in inpatient hospices increased slightly in both cancer and non-cancer (0.4% and 0.3%, respectively). The overall proportion of institutional deaths decreased by 2.4%, but because of the fall in the overall number of deaths the decrease in absolute numbers was greater (6.6%; from 408,539 in 2004 to 381,534 in 2010).
Home deaths increase for the first time in the very elderly
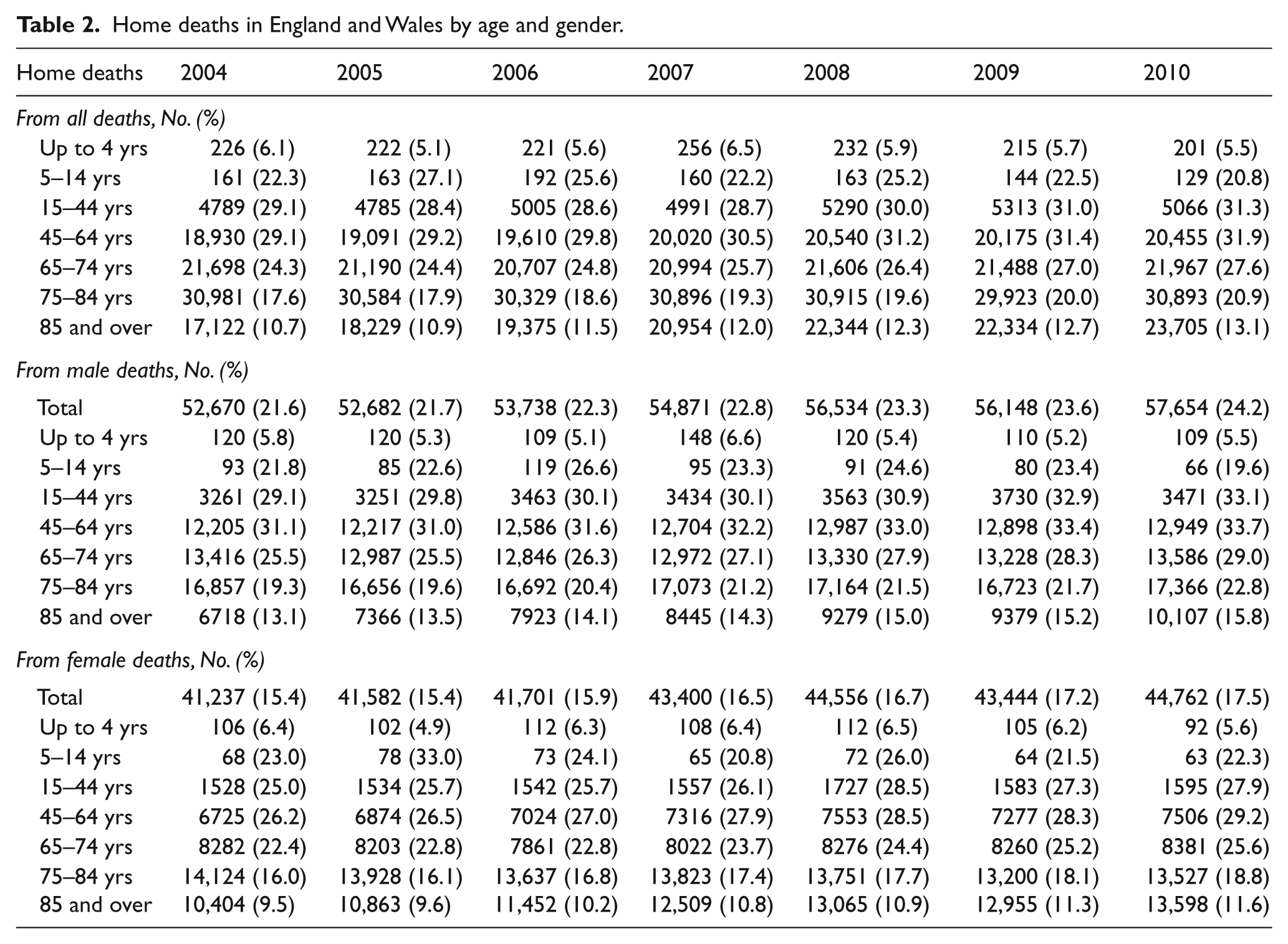
The number of home deaths increased for both genders and across age groups except for those younger than 14 years and for those aged 65–84, but only up to 2006 (Table 2). In those aged 85 and over the number of home deaths increased from 17,122 in 2004 to 23,705 in 2010. Proportions also rose from 10.7% to 13.1%. Notwithstanding, those aged 85 and over died less often at home over the seven-year period than the other adult age groups.
Home deaths in England and Wales by age and gender.
Comment
Trend reversal and explanations
What seemed to be an enormous task has happened – the reversal of the British longstanding trend towards an institutionalised dying. From 2004 onwards, it became more common for people in England and Wales to die at home. Although still recent, this trend is shown in both proportions and numbers (despite the decrease in overall numbers of deaths) and is sustained throughout the seven years examined. There were no methodological changes to affect the way home deaths were recorded prior to and after 2003. The actual figures clearly deviate from the projected figures based on a continuation of past trends (Figure 1). This suggests that the trend reversal is real.
Changes in the demographics of dying did not explain the increase of home deaths. In fact, the ageing of the population (with increased numbers of deaths from older people, a group found to be less likely to die at home) exerted influence in the opposite direction. Other factors associated with death at home are likely to have played a role. 2 It is possible that the British policy push towards enabling more people to die at home, including the government end-of-life care programme (established in 2004) and the national end-of-life care strategy (published in 2008) may be responsible for the trend reversal, alongside other factors. 12
Comparison with other countries
Britain is no longer part of the group of world regions with trends towards a greater institutionalisation of dying (e.g. Italy, Greece, Japan, Taiwan)6,7,13,14 and it joins countries where home deaths have been increasing for some years, such as the USA (since the 1980s) and Canada (since 1994).15–17 The British trend also differs from the Belgian and the South Australian trends.18,19 In these countries, the main shift has been from hospitals to nursing homes hence it did not involve home deaths. In England and Wales, since the categories NHS and non-NHS hospitals and nursing homes include both hospitals and nursing homes, a shift from hospitals to nursing homes remains hidden, if it existed. ONS data from 2010 onwards with a new coding separating hospital and care home deaths will allow investigation of these shifts.
It is important to note that the proportion of home deaths remains low and below that reported in the USA, Canada and other European countries (e.g. the Netherlands). 20 The most recent figure (20.8%) is still far from meeting the preferences for the majority of people who wish to die at home.
It is also important to note that whilst in some countries the overall numbers of deaths have been increasing (e.g. Germany, Canada), in Britain they have been decreasing, but are expected to rise substantially in the near future.9,21 This may affect how the trend behaves from now onwards in light of an increased demand for end-of-life care. Also important is the fact that although home deaths increased for the first time in the very elderly, the age differences previously identified have been maintained.9,22 In Britain, the very elderly continue to have fewer chances to die at home, but this is not a universal fact – the inverse seems to happen in the USA, at least for cancer patients. 23
Need for evidence
As death is shifting back home in a number of countries, it is imperative to find ways to monitor more closely trends in place of death both nationally and internationally. Death registration data usually take a few years to become available. In addition, the healthcare implications of the rising numbers of home deaths should be considered with great care.
Firstly, not all people with a terminal illness have an equal chance of dying at home. For example, people living in deprived areas are less likely to die at home.2,22,23 It is important to ensure that inequities are reduced and that home deaths increase not only in groups known to have increased chances of dying at home. The reality may be somewhat different in non-cancer (as suggested in Figure 1).
Secondly, as the number of home deaths increases across nations, it becomes more urgent to examine at what quality and secondly at what cost do people die at home. Presently, there is little evidence that patients who die at home and their relatives experience better care than those who die in institutions, such as hospitals, hospices or nursing homes, apart from Teno et al.’s 1 nationwide mortality follow-back survey in the USA back in 2000. There is a dearth of comparative studies on the associated costs. A population-based survey with bereaved relatives – the QUALYCARE study – is examining variations in outcomes and costs for cancer patients dying in different settings in London, Britain. 24 It is crucial to investigate to the same level of detail the experiences of people dying from non-cancer conditions. Such information is vital to develop investment plans and services that meet the increased end-of-life care needs of ageing populations and ensure the best possible outcomes of care for terminally ill patients and their families wherever they wish to be.
Footnotes
Acknowledgements
We thank our funders, Cicely Saunders International and the ONS, for supplying the mortality data (special thanks to Vanessa Fearn, Di Goodwin and Claudia Wells). We also thank the anonymous reviewers for their insightful comments.
Funding
This work was supported by the charity Cicely Saunders International [grant code MMSTCYR] and is a result of a long-term project on place of death led by Gomes and Higginson.
Conflict of interest
All authors declare that they had support from Cicely Saunders International for the submitted work. Cicely Saunders International did not have any role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, or approval of the manuscript. Authors have also received funding in the past five years from the UK Department of Health for conducting end-of-life care research. Although unlikely, it is possible that this organisation may gain or lose financially from the publication of this manuscript. The authors declare that they have no other relationships or activities that have influenced the submitted work.