
Abstract
Background:
Medical care at night for patients with do-not-resuscitate orders and the practice patterns of the on-call residents have rarely been reported.
Aim:
To evaluate the after-hours physician care for patients with do-not-resuscitate orders in the general medicine ward.
Design:
Observational study.
Setting/participants:
This study was conducted at an urban, university-affiliated academic medical center in Taiwan. The night shift nurses consecutively recorded every event that required calling the duty residents. Patients with and without a do-not-resuscitate order were compared in demographics, reasons for calling, residents’ response, and nurses’ satisfaction. A standard report form was established for the nurses to record events.
Results:
From October 2009 to September 2010, 1379 inpatients contributed to 456 after-hours calls. do-not-resuscitate patients accounted for 256 (18.7%) of all inpatients, and 160 (35.1%) of all after-hours calls. The leading reason for calls was abnormal vital signs, which was significantly higher for patients with do-not-resuscitate orders compared to patients without a do-not-resuscitate order (64.4% vs 36.1%, p < 0.001). The pattern of residents’ responses showed a significant difference with more bedside visits for patients with do-not-resuscitate orders (p < 0.001). The nurses were usually satisfied with the residents’ management of both groups.
Conclusion:
Abnormal vital sign, rather than symptom, was the leading reason for after-hours calls. The existence of do-not-resuscitate order produced different medical needs and physician workload. Patients with do-not-resuscitate orders accounted for one-third of night calls and nearly half of bedside visits by on-call residents and may require a different care approach.
Introduction
The night shift is a time when on-site faculty supervision and nurse staffing ratios are reduced resulting in a different system of care at night compared to the day.1,2 There is some evidence that the medical events which occur at night are associated with poor clinical outcomes. 3 Studying nursing and beeper calls at night allows for researchers to understand the demand and need of inpatients at night. Unfortunately, such studies are rare in the literature. Studies focusing on paging patterns4,5 showed that interns were interrupted frequently during both sleep and patient encounter and that nurses’ perception was not in agreement with residents’ responses. 6 Another study investigating paging times showed that on-call days generate nearly five times of workload to physicians. 7 However, these studies focusing on the occurrence of paging provide incomplete information regarding physician workload. The unanswered questions regarding on-call residents’ workload are the sources of paging as well as workload produced after paging. To answer these questions, the demand of paging and behavior of on-call residents should be observed.
Palliative care (PC) is a continuous process, which typically begins with discussing advance care planning and end-of-life (EOL) care. 8 Patients who have do-not-resuscitate (DNR) orders are a particular population in a hospital, and their physical, social, and mental needs may be very different.9,10 With the progress in palliative medicine, patients are well cared for by specialist PC teams during the daytime. However, the treatment for inpatients may be suboptimal at night and outside the PC unit. In the general medicine setting, the medical needs of inpatients with DNR orders may be different from other inpatients and are less satisfactorily met at night with the current off-hours care system. Our study aims to investigate the physician care for inpatient at night and allows to compare between patients with and without a DNR order. It is hypothesized that patients with DNR order would generate different workload for after-hours physicians.
Methods
Study setting
This study was conducted at the National Taiwan University Hospital (NTUH), a 2000-bed, university-affiliated tertiary referral medical center in Taiwan. A hospitalist acute general medicine service was established in October 2009, and general medicine patients are admitted to this hospitalist ward from the emergency department (ED). The performance in caring for general medicine patients in this ward was demonstrated in our previous study. 11
Three working shifts, day, bridge, and night, were designed for the hospitalist ward and remained unchanged during the study period. Patients newly admitted from the ED were assigned to both day and bridge hospitalists. In general, all beds were fully occupied in the evening. The night shift was from 11 p.m. to 8 a.m. the following day, with the staff taking handoffs from the bridge shift (from 1 p.m. to 11 p.m.) and covering the whole ward overnight. Nurse practitioners were assigned to the day and bridge shift hospitalists, and residents were assigned to the night shift hospitalist. Residents were the first to whom night shift nurses reported inpatient problems and data. Each hospitalist, resident, and nurse practitioner had a mobile phone to communicate with each other.
Night shift call recording
A standard night shift call record form was designed by our study group. The night shift nurses (working from 11 p.m. to 8 a.m.) were responsible for recording every event that required calling the duty residents. In order to minimize the bias of underreporting or overreporting, night shift nurses who participated in the study were informed that the record forms aimed to monitor the resident’s management and notify the day staff of important events. The on-call residents were blinded to the study design. To minimize the observation effect, the Institutional Review Board (IRB) of our institution agreed that only the night shift nurses required the informed consent.
Population and data collection
The IRB of NTUH approved the study (201006028R). This study was performed by prospective data collection with retrospective analysis. A standard night shift call record form was used for quality control purpose, and it consisted of time of call, classified call reasons, vital signs at calling, subsequent management of the physician, and the nurses’ satisfaction on the whole management process.
Advance care plans are scarcely noted in hospitalized patients in Taiwan. DNR is typically discussed after admission and is usually initiated by physicians when the patient’s clinical status becomes life-threatening or irreversible. If a patient has a DNR order that has been signed by himself/herself (or families) and by in-charge physicians, it is legal for physicians to withhold cardiopulmonary resuscitation in our country since 2000. Patients who had DNR codes during hospitalization in the hospitalist ward were included as the population of interest. Patients with DNR orders were labeled as “DNR” in green in the health information system of our hospital, whereas the remaining patients were not labeled in green. We were thus able to easily identify DNR patients when the calls were placed.
In order to analyze the night shift events and patterns, the management of the residents was classified as telephone order, immediate bed visit, or delayed bedside visit. Drug prescriptions could be made by the residents via the electronic prescription system anywhere in the hospital. The residents did not have to go to the nurse station for simple medication requests such as sleeping pills or drug refills. On-call residents, who were blinded to the study, decided by themselves whether an immediate (within 15 min) bedside visit was required. A bedside visit more than 15 min after a call was defined as a delayed bedside visit, as used in a previous study. 6 The actual time lag between the call and visit was recorded by the nurses.
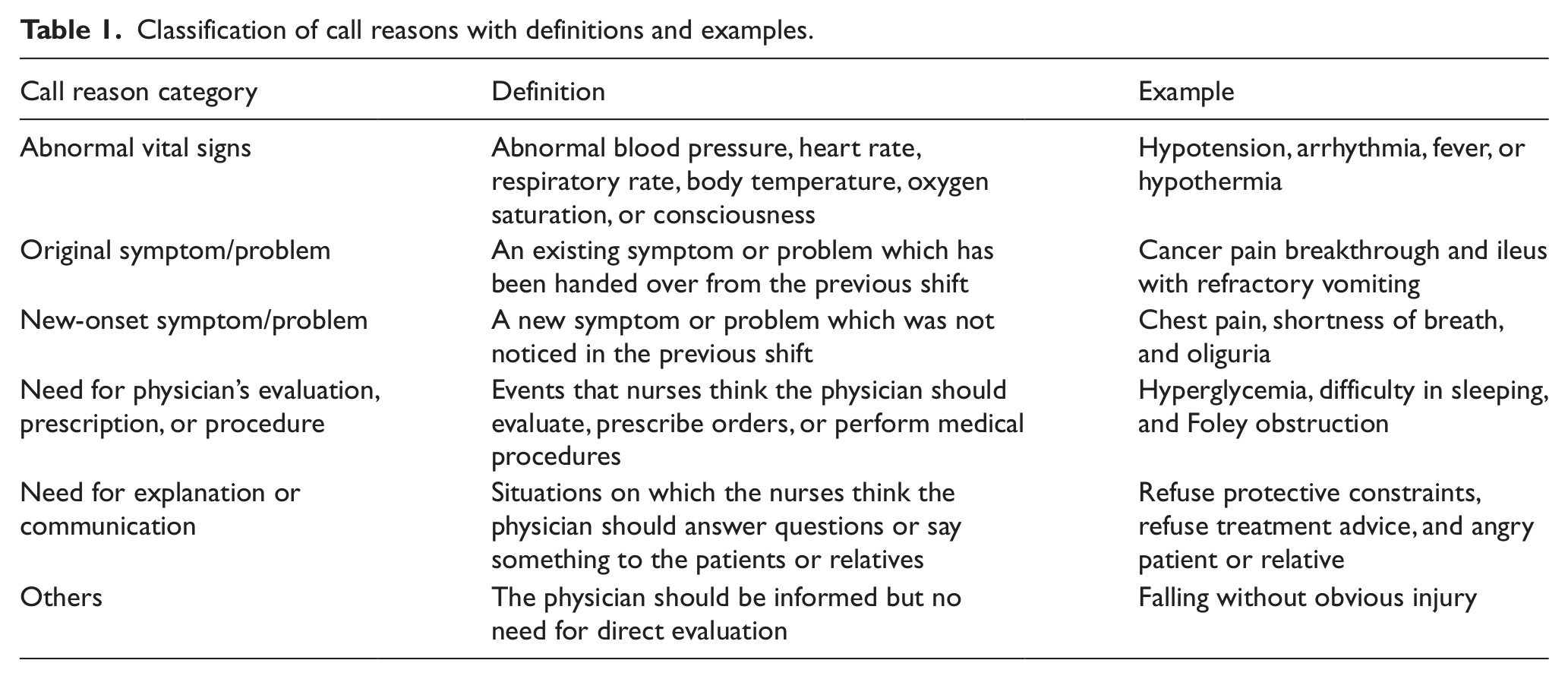
For analysis, the reasons for the night call were classified into six categories by the night shift nurses—(1) abnormal vital signs; (2) original symptom/problem; (3) new-onset symptom/problem; (4) need for physician’s evaluation, prescription, or procedure; (5) need for explanation/communication; and (6) others—in descending order of priority with the category of highest priority being recorded. The classifications, definitions, and examples are shown in Table 1.
Classification of call reasons with definitions and examples.
The night shift nurses who participated in our study were requested to complete informed consent process by the IRB of NTUH. The nurse’s satisfaction was measured using a Likert scale including five levels of satisfaction: very satisfied, satisfied, unsure, dissatisfied, and very dissatisfied. The night shift nurses completed the satisfaction scale within their shift.
Statistical analysis
The data were analyzed using SPSS software (version 16; SPSS Inc., Chicago, IL, USA). We compared the basic demographic data, reasons for the night call, residents’ response, time to bedside visit, and nurses’ satisfaction score between patients with and without a DNR order. Subgroup analysis was done for all DNR night calls to compare characteristics between cancer patients and noncancer patients. Intergroup differences were compared using Pearson’s chi-square test or Fisher’s exact test for dichotomous variables and using the Mann–Whitney U test for continuous variables.
Results
Demographic data
From October 2009 to September 2010, a total of 1379 patients were admitted to the hospitalist ward. Among them, 258 patients (18.7%) had DNR orders during hospitalization. Table 2 depicts the demographic data and outcomes of all patients with DNR orders.
Demographics of the patients with DNR orders in the whole study cohort.

BMI: body mass index; CCI: Charlson comorbidity index; DNR: do-not-resuscitate; GHTD: go home to die; ICU: intensive care unit; LOS: length of stay.
Data are expressed as median (minimum–maximum) or number of cases (%).
Reasons for night shift calls
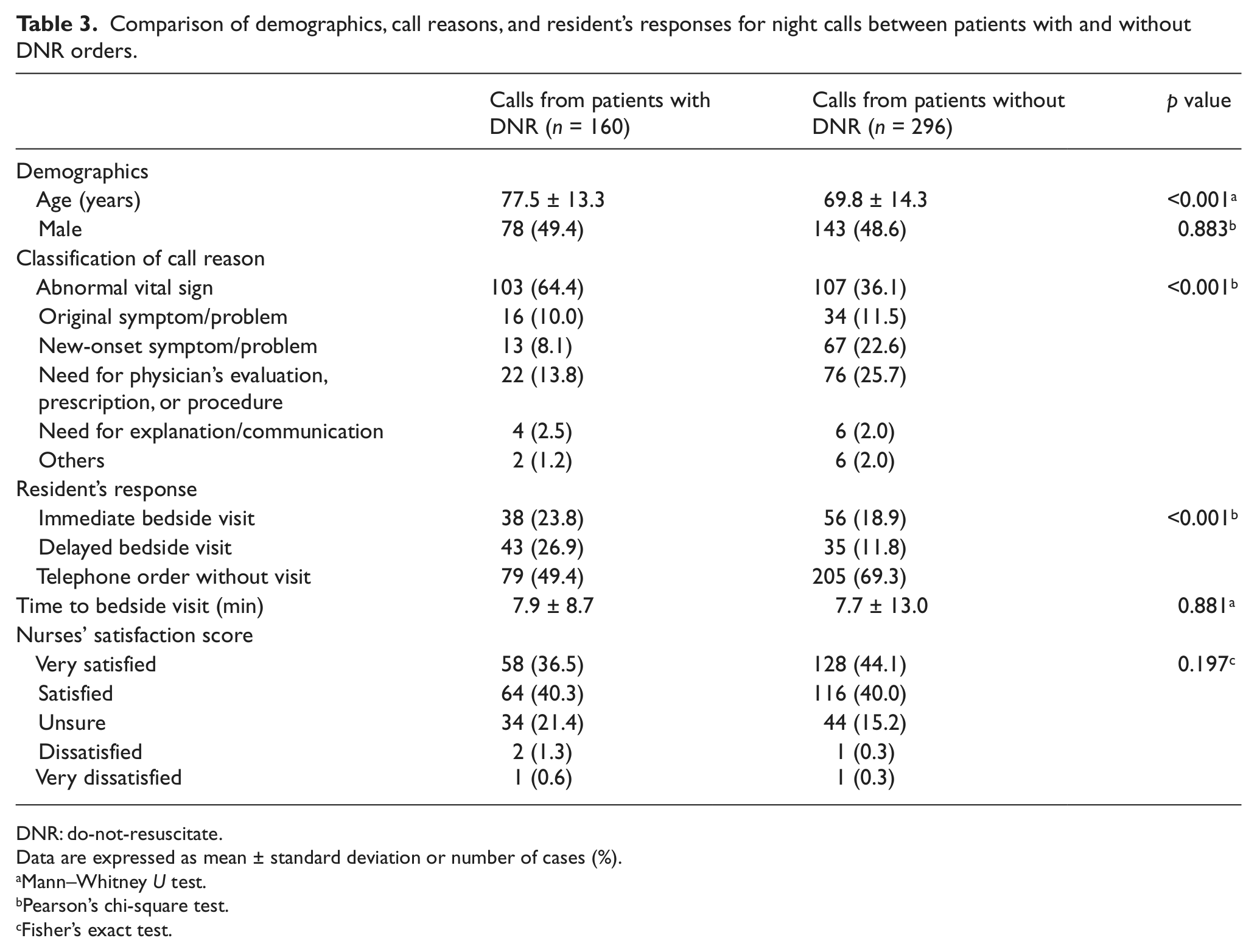
Within the 1-year study period, a total of 456 night calls to physicians were recorded. Table 3 shows the characteristics of the night calls with comparisons between patients with and without a DNR order.
Comparison of demographics, call reasons, and resident’s responses for night calls between patients with and without DNR orders.
DNR: do-not-resuscitate.
Data are expressed as mean ± standard deviation or number of cases (%).
Mann–Whitney U test.
Pearson’s chi-square test.
Fisher’s exact test.
Patients with and without a DNR order accounted for 160 (35.1%) and 296 (64.9%) of all calls, respectively. For both groups, the leading reason for the night calls was abnormal vital signs, which was significantly higher for the DNR group (64.4% vs 36.1%, p < 0.001). Compared to patients without a DNR order, patients with DNR orders had significantly fewer calls for symptoms or problems, regardless of whether they were original or new.
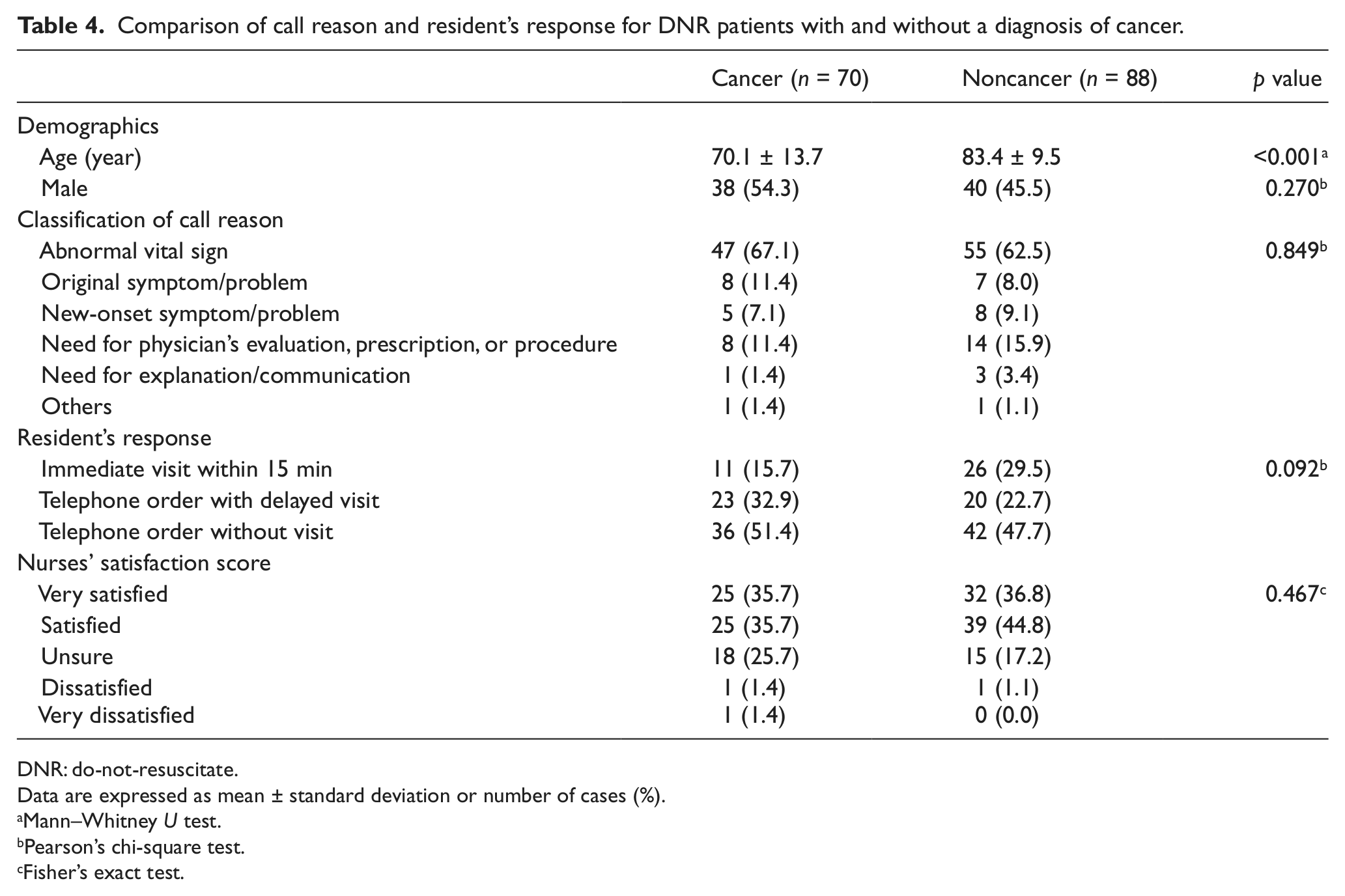
Among 158 calls from patients with DNR orders, 70 (44.3%) were from patients with history of cancer. When comparing cancer and noncancer patients, there was no significant difference between call reasons (Table 4).
Comparison of call reason and resident’s response for DNR patients with and without a diagnosis of cancer.
DNR: do-not-resuscitate.
Data are expressed as mean ± standard deviation or number of cases (%).
Mann–Whitney U test.
Pearson’s chi-square test.
Fisher’s exact test.
On-call resident’s response and nurses’ satisfaction
The percentages of bedside visits were 50.6% and 30.7%, and the percentages of immediate visits within 15 min were 23.8% and 18.9% for patients with and without a DNR order, respectively. Telephone orders without visits occurred in 49.4% of night calls for patients with DNR orders but 69.3% for patients without a DNR order. Overall, the pattern of the residents’ responses showed a significant difference between patients with and without a DNR order (p < 0.001), with more bedside visits for the former.
Of all 172 bedside visits, patients with and without a DNR order accounted for 81 (47.1%) and 91 (52.9%), respectively. Regarding direct patient care workload, it was similar between the DNR and non-DNR groups although the former was a minor subpopulation.
A total of 449 nurse satisfaction reports were used for analysis (7 were excluded due to missing data). The nurses scored “very satisfied” in 36.5% and 44.1% for patients with and without a DNR order, respectively. In general, the nurses were satisfied with the residents’ management, and there was no significant difference between the two groups (Table 3).
Time distribution of night shift calls
Figure 1 depicts the distribution of the 456 calls on an hourly basis throughout the night shift. Two peaks of the night calls, at 1–3 a.m. and 6–8 a.m., were noted. The variation seemed to be more prominent for patients without a DNR order than patients with DNR orders, although there was no significant difference.
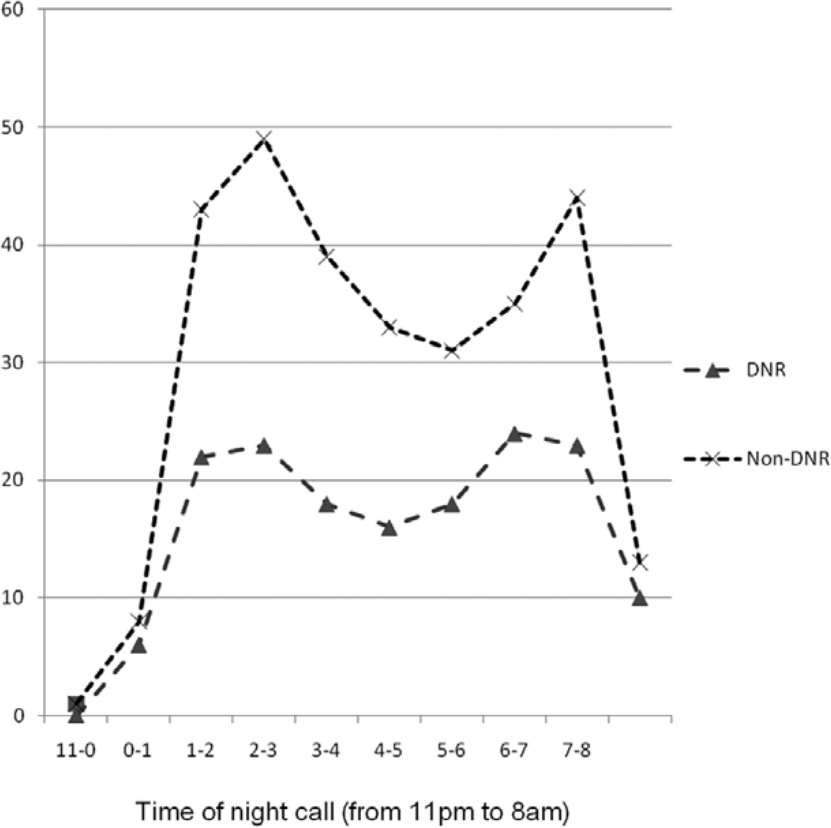
Time distribution of night calls to physicians.
Discussion
Abnormal vital sign was the leading reason for after-hours calls whether patients had DNR or not. To the best of our knowledge, this is the first report on after-hours calls to physicians comparing patients with and without DNR. The most valuable finding is that the reasons for the calls to the residents at night were significantly different between patients with and without a DNR order, with more urgent calls for abnormal vital signs for the former. The behavior patterns and workloads of the on-call residents were also different, and these findings may be valuable in improving resident care at night.
Patients with DNR orders were a minority of the patients in the general medicine ward; however, they accounted for one-third of night calls and half of direct patient care workload. This finding is important for researchers because we usually assume that patients with DNR orders require fewer medical interventions. After discussing DNR and EOL issues, we also assume that patients and relatives have an insight into terminal or near-terminal conditions and demand conservative, noninvasive, and symptom-oriented treatments after signing DNR consent. However, we may be neglecting the need for mental support and bedside visits just for the comfort and reassurance of continuing care. When vital signs worsen, which accounted for 64.4% of night calls in our study, the patients and relatives may still need supportive visits. These psychological needs are similar to the patients without a DNR order. There were fewer symptoms requiring night calls for patients with DNR orders compared to those without a DNR order, which indicates fair pain and symptom management for the former group in the study ward. However, if unexpected pain, dyspnea, or delirium occurs, evaluation and prescriptions by the residents are still mandatory. Finally, death can occur at any time. All the aforementioned needs contributed to the reasons for the night calls for patients with DNR orders in this study, and they were a significant source of night shift workload for both nurses and residents.
The attitude toward the patients with DNR orders did not appear to change because of DNR consent itself. In addition, it is natural for nurses to call duty physicians when the idea of “calling is necessary for unstable conditions” is so firmly rooted in their minds. The fact that two-thirds of the calls for patients with DNR orders were due to abnormal vital signs has important clinical implications and suggests a way to decrease avoidable calls at night. It appeared as though pain and symptom management were performed well. However, our results may suggest that we can discuss the issue of managing abnormal vital signs more with the nursing staff. First, we should have a consensus on the use of fluid resuscitation, blood transfusions, and vasopressors. We should even discuss whether bedside monitoring is appropriate or what to do when a monitor sounds an alarm. Is a fast heartbeat harmful or just a mirror of stress and anxiety to which we should pay attention? Is a slow heartbeat dangerous or a reflection of being comfortable? Should we do routine workup for fever or just give antipyretics and relieve the associated symptoms? All these points may be helpful when the nursing staff face changing conditions. In addition, fewer routine checkups may alleviate the anxiety of the patients and relatives. In our study, the two peaks of night call distribution shown in Figure 1 reflected the nursing round pattern at night. 12 While routine checkups are mandatory for general patients, is it necessary to closely monitor patients with DNR orders during sleep? If we communicate more and reach a consensus, the nurses will be more likely to feel at ease without doing routine round and checkups at night.
Second, we should facilitate communication between nurses and physicians, especially during off-hours. 13 Nurses could be included in the PC and EOL discussions or, at least, the nurses could be made aware of how we plan to handle abnormal events. Without these steps, the patients and relatives may become confused with the inconsistent attitudes of the nurses and physicians. Such internal communication takes time but is always worthwhile.
With regard to the residents’ responses, 50% of after-hours calls for patients with DNR orders required immediate or delayed bedside visits by on-call residents. Again, the workload for the residents appeared to be much higher than for patients without a DNR order who needed only 30% bedside visits. When nurses called the residents for a patient with DNR order, it could only be handled by telephone order or electronic prescription system half of the time. When analyzing all bedside visits made by the residents, half were for patients with DNR orders and half for patients without DNR, although the former group accounted for 18.7% of the ward. From this point of view, it is reasonable to assume that the workload for night staff will rise substantially if the number of patients with DNR orders increases. In a previous survey in Japan, Morita et al. 14 pointed out that the number of nurses and the number physicians were significant determinants of family satisfaction. A question that researchers should study is how to predict the necessary level of manpower required to care for patients with DNR orders.
This study has several limitations. First, the reasons why the patients called the night shift nurses were not studied. In a previous study, the reasons were different from those causing nurses to call doctors. 15 The nursing need for patients with DNR orders is also an important issue. However, we only focused on the need to call an on-call resident, so the response patterns could be studied. Second, we only surveyed the need for resident care at night for patients with DNR orders, which cannot be generalized to the daytime. Care at night aims to provide the best possible sleeping environment for the patients. 16 Night call studies are thus valuable because they reflect the real needs for the patients at night, without being confounded by daytime activities. To improve nighttime problems and design effective care in a hospital, it is critical to gather frontline information at night. 2 Third, patients with DNR orders in a general medicine setting may be different from those in a specialist PC unit. However, the subgroup analysis showed that cancer and noncancer patients had similar reasons for night calls. Therefore, we believe that the results are representative.
The medical need for the patients with DNR orders was different at night, but we have not yet designed a patient-centered, after-hours PC system in the hospital. Therefore, we can hardly say that PC at night is as good as that in the day. In order to minimize the inequity of day-and-night PC, potential solutions are to facilitate handoff communication, to improve doctor–nurse communication, and to introduce mandated 24-h coverage by specialist PC teams or hospitalists with PC training. 17
Conclusion
Our study unveils the picture of medical care delivery at night in the general medicine setting. The DNR status increased medical need at night and on-call residents’ workload. Patients with DNR orders were a minority of the patients in the general medicine ward but accounted for one-third of after-hours calls and nearly half of direct patient care workload by on-call residents. The medical need at night for patients with DNR orders may require a different care model. Therefore, further studies into after-hours PC are warranted.
Footnotes
Declaration of conflicting interests
None.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.