
Abstract
Background:
Patient misunderstandings about prognosis may be related to lack of communication.
Aim:
This study aimed to examine prognosis discussions held with hospitalized patients for whom palliative care consultations were requested, and if prognosis discussions did not occur, to explore why not.
Design:
This was a survey conducted over the telephone from a convenience sample of health-care providers who requested palliative care consultations. Respondents were asked about whether prognosis had been discussed with the patient and the topics addressed.
Participants:
A total of 65 health-care providers who called to request a consultation from the palliative care team in a large academic medical center in the United States.
Results:
Of the 65 responses, 45 (69.2%) subjects reported that a prognosis discussion had occurred, while 15 (23.1%) reported that a prognosis discussion had not taken place. Among the surveys reporting a prognosis discussion, a majority of providers responded that most aspects of prognosis were discussed, with the exceptions of life expectancy, survival rates/statistics, and psychosocial concerns. When the prognosis discussion had not occurred, the most common reasons for omitting the prognosis discussion included difficulty in determining prognosis, the perception that the patient already knew his or her prognosis, and the belief that the prognosis discussion was better suited for a different specialty.
Conclusions:
The results of this study highlight the uncertainty that primary team providers in the academic hospital environment have with prognostication, which is a complex process for which this set of providers, composed primarily of medical trainees and nurses, may not have had sufficient training.
Patient misunderstandings regarding their projected survival have been linked to lack of health-care providers’ communication regarding prognosis, but it is not clear whether this is primarily related to complete lack of discussion or incomplete discussions.
There is a lack of data about the frequency of discussions of prognosis with hospitalized patients and the specific components of prognosis discussions.
This study demonstrated that certain aspects of prognosis discussions, including life expectancy, survival rates, and psychosocial concerns, were not covered in many prognosis discussions.
Reasons why discussion of prognosis did not occur included uncertainty regarding prognosis, the perception that the patient already knew the prognosis, and the belief that a prognosis discussion would be more appropriately held by a provider of a different specialty.
This study highlights the complexities and challenges of discussing prognosis.
The results of this study highlight the need for improved educational strategies that will foster the abilities of medical trainees and other providers to hold thorough and effective discussions of prognosis.
Background
Communicating prognosis, especially with patients suffering from life-limiting illness, can be a difficult process.1–4 While many patients with advanced or life-limiting illness need prognostic information, accept their disease, and make decisions regarding treatment, this information is often not conveyed to the patient effectively.2,4,5 The Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatments (SUPPORT) showed that patients with advanced (stage III or IV) non-small cell lung cancer overestimated survival when compared to physician estimates. 6 Patient overestimations of survival have been linked to lack of physicians’ communication of prognosis.1,7 These misunderstandings lead to adverse consequences, in which patients obtain more aggressive treatment than warranted, ultimately leading to increased morbidity.
However, communicating prognosis can be a difficult process for health-care providers. Failure to communicate patients’ prognoses may be related to fear of making patients unnecessarily upset or causing patients to lose hope, as well as reluctance to go against patients’ wishes, uncertainty regarding how to present prognostic information, and lack of confidence.3,8–11
Prognosis has become an important focus for palliative care providers. Indeed, one guideline for assessment of quality of palliative care in academic medical centers includes documentation of prognosis for patients within 48 h of admission to the hospital. 12 However, the extent to which these benchmarks are being followed is not well described.
This study aimed to examine whether prognosis discussions were occurring in hospitalized patients for whom palliative care consults were called and, if these discussions were occurring, to determine what aspects of prognosis were covered. In addition, we sought to explore what factors led to a lack of a prognosis discussion when this did not occur. The study was approved by the Institutional Review Board of the study site (IRB #07-11-06).
Methods
The study was conducted in a large academic medical center located in Cleveland, Ohio. A questionnaire was created and administered via phone or in person to any health-care provider who requested a consultation from the Palliative Care Service from August to September of 2011. The only exclusion criterion was if the caller had previously answered the survey. Consent was obtained directly prior to administration of the survey, and survey participants were given the option to not participate at any time. Consult requestors were given 48 h to complete the survey. During this time, attempts were made to follow up with the provider requesting the consult. Those who were reached were given the survey either by phone or in person.
The questionnaire included a section on demographics, with questions asking the respondent’s role on the team (i.e. attending physician, resident, advanced practice nurse (APN), etc.), specialty, years worked in health care, age, gender, and past experience with palliative care. For those who were residents, specialty represented the residents’ training program and not their current rotation service. The section on prognosis asked the respondent’s familiarity with the patient’s prognosis and whether a prognosis discussion was held with the patient during the patient’s current admission. Respondents who were present for the prognosis discussion were asked whether the following were discussed: the patient’s diagnosis, probability of a cure, extent/severity of disease, life expectancy, survival rates, statistics, effect of the patient’s disease on quality of life, treatment options, reassurance/hope, and psychosocial concerns. If probability of a cure and statistics were not included in the prognosis discussion, the respondent was asked why these topics were not included. If the caller was not present for the discussion, he or she was asked to provide contact information for the health-care provider who conducted the prognosis discussion. This contact information was used to reach the providers who conducted the discussion, and those who were successfully contacted were invited to participate in the survey. If the prognosis discussion had not occurred, the respondent was asked why the discussion did not take place.
Data collected from the surveys were entered into SPSS software, and frequencies tabulated for demographic data and survey responses. For questions that involved an open answer, responses were read independently by two of the investigators (A.C. and I.D.-B.) and coded as to major themes. These summaries were then compared and discrepancies resolved by repeated review of the raw data.
Results
The investigators attempted to enroll 101 requestors of palliative care consultations. Of these consults, 20 callers were unable to be reached for survey administration, while another 16 were respondents who had already answered the survey previously. A final sample of 65 surveys were included in the analysis (Figure 1). Of these, 33 (50.8%) respondents were present during the prognosis discussion and able to explain what had been discussed with the patient regarding the patient’s prognosis. Twelve (18.5%) of the respondents stated that the prognosis discussion occurred, but they were not present during the prognosis discussion. Five (7.7%) providers did not know whether the prognosis discussion had occurred, and 15 (23.1%) stated that the prognosis discussion did not occur during the patient’s current admission.
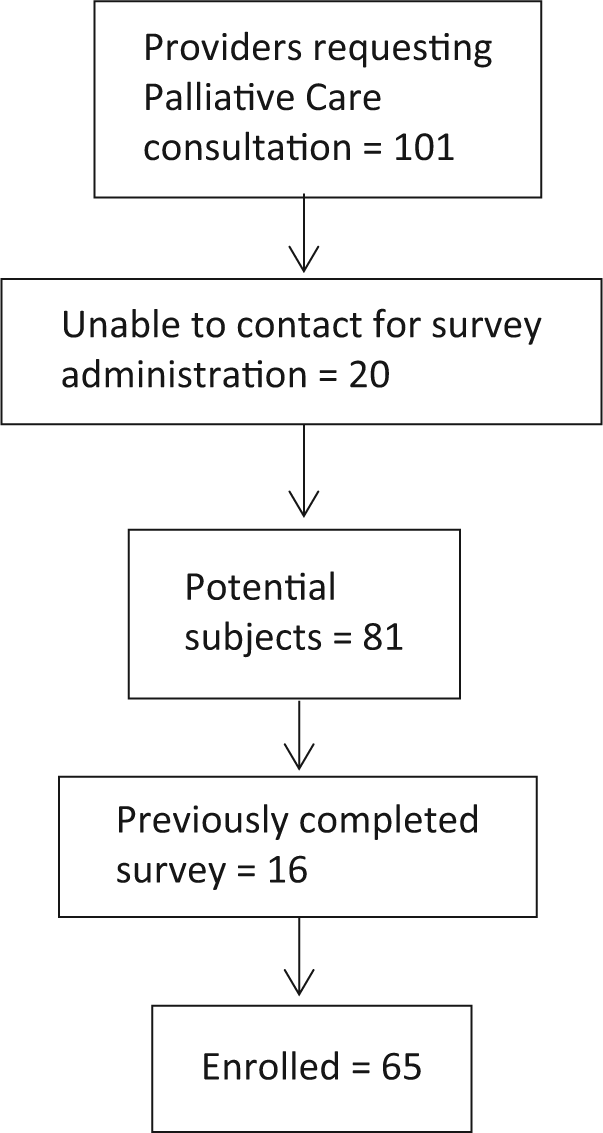
Sample enrollment.
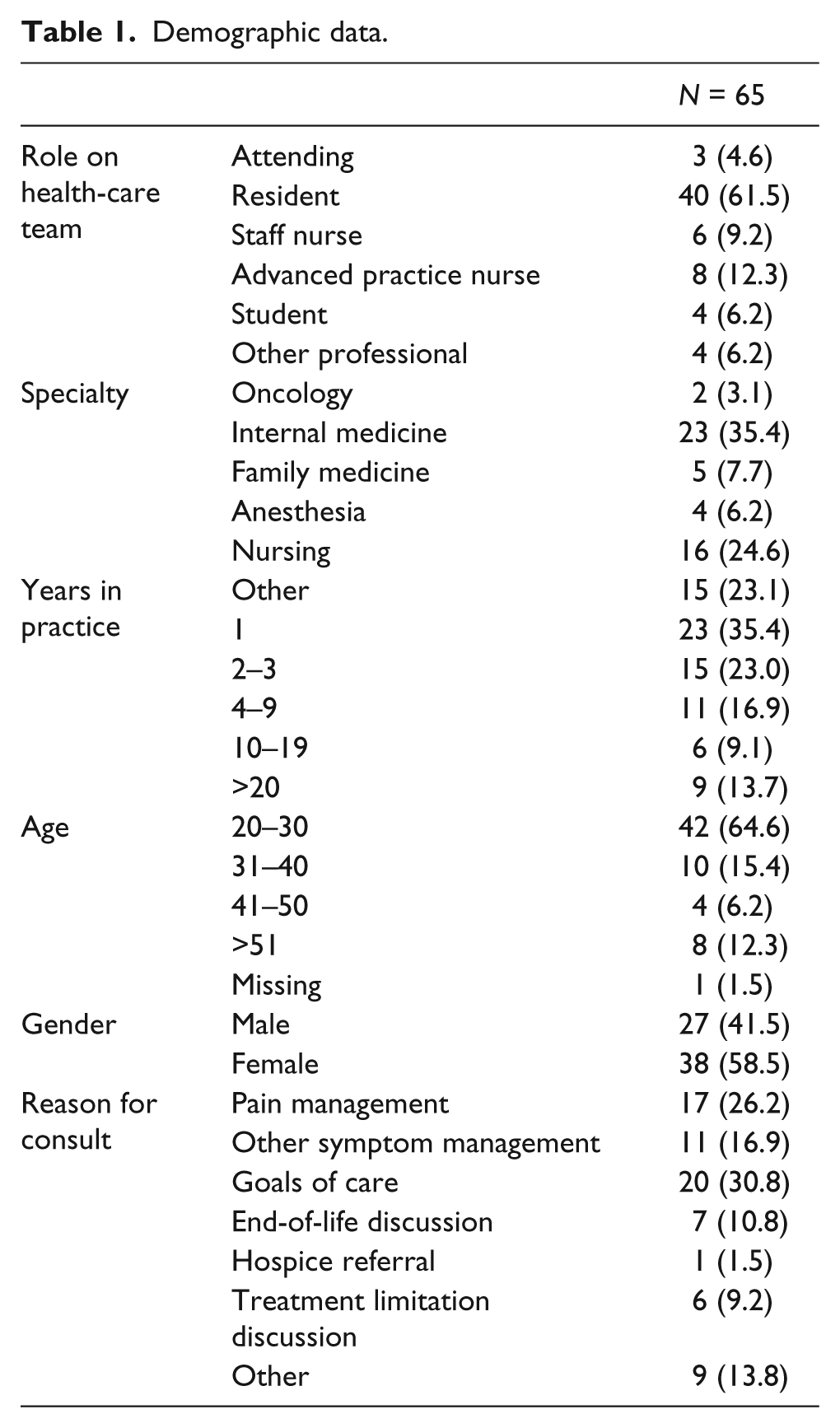
Demographic data are listed in Table 1. As can be seen, most respondents were residents (n = 40, 61.5%), and most were practicing in the specialty of internal medicine (n = 23, 35.4%). The majority (64.6%) of respondents were younger (20–30 years old) and female (n = 38, 58.5%). Primary reasons for requesting a consultation included pain management (n = 17, 26.2%), other symptom management (n = 11, 16.9%), and goals of care (n = 20, 30.8%).
Demographic data.
A large majority of respondents (n = 55, 84.6%) stated that they were familiar with the patient’s prognosis, while the remaining providers (n = 10, 15.4%) indicated that they were not familiar with the patient’s prognosis. Of those who responded that they had been present for the prognosis discussion (n = 33), 90.9% stated that they were familiar with the patient’s prognosis. Most of the respondents present for the discussion were also the providers who had conducted the discussion (n = 21, 63.6%); the remaining providers (n = 12, 36.4%) had been present for the discussion but did not conduct the discussion themselves.
As expected, there were some differences between physician and nurse respondents. Eight of the nine respondents who had more than 20 years of experience were nurses. Although the APNs reported having held a prognosis discussion with similar frequency as residents (3/6 for APNs and 16/33 for residents), none of the three staff nurses did.
Table 2 lists the aspects of prognosis that were covered during the discussion, showing totals for all providers who were present for the discussion (n = 33) and also for the subset of providers who conducted the discussion themselves (n = 21). After examination of the data, discussion about survival rates and statistics were combined into one category because the categories were considered too similar, and all the respondents who did not discuss survival rates also did not discuss statistics. A large majority of providers had discussed most of the topics listed within the survey, including the patient’s diagnosis, probability of a cure, extent/severity of disease, the effect of the patient’s disease on quality of life, treatment options, and reassurance/hope. Topics discussed less often included life expectancy, survival rates/statistics, and psychosocial concerns. The distribution of topics that were discussed versus not discussed was similar between those present for the discussion and those who conducted the discussion. In response to the question “If you did not use statistics in your discussion, why not?,” reasons included the provider’s lack of knowledge/uncertainty regarding the exact statistics, the belief that statistics would better be provided by someone else, and the idea that statistics were not useful or relevant to the situation.
Topics discussed.
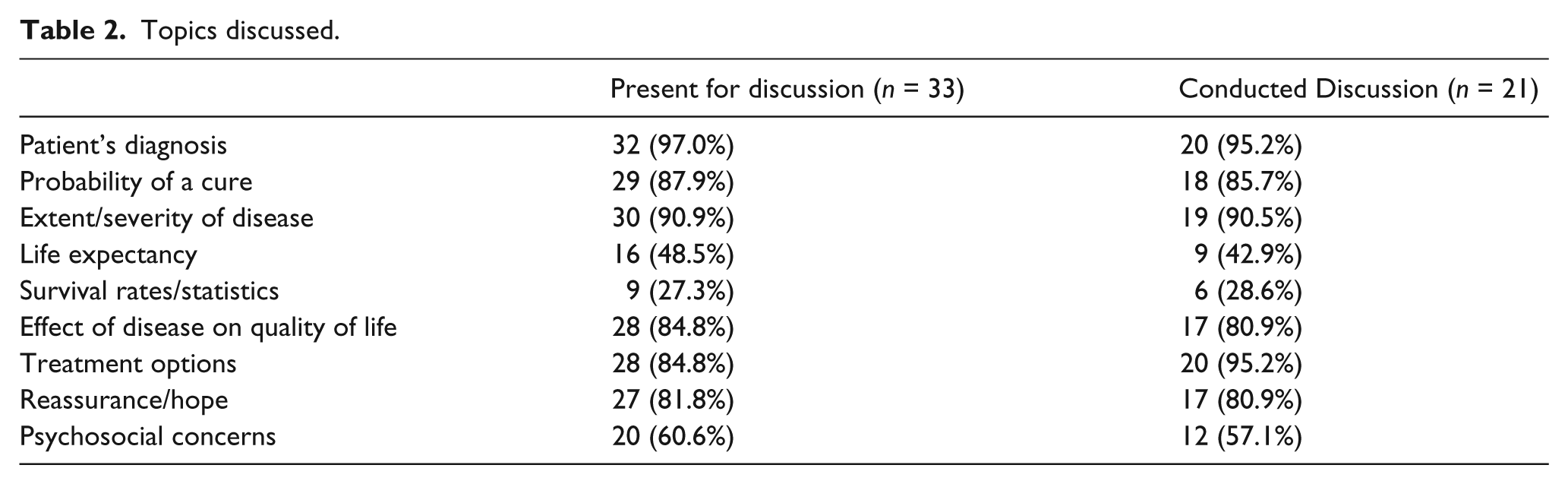
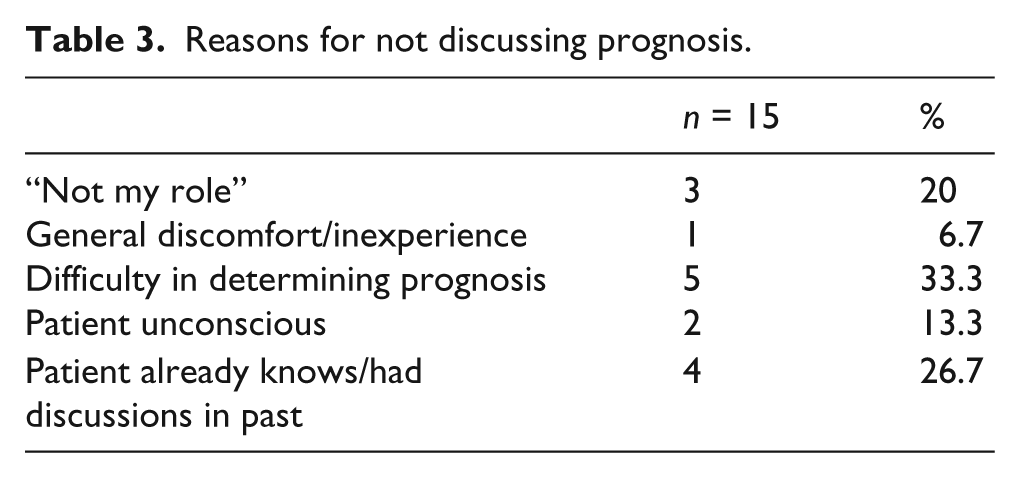
Table 3 lists reasons why the prognosis discussion was not held in 15 cases. For those providers who responded that the prognosis discussion had not occurred, the most common reason was difficulty in determining the patient’s exact prognosis. Other reasons included the belief that the patient already knew his or her prognosis because he or she had many prognosis discussions before admission, the thought that the prognosis discussion was better suited for a provider from a different specialty, inability to have the discussion because the patient was unconscious or delirious, and general discomfort/inexperience with the prognosis discussion.
Reasons for not discussing prognosis.
Discussion
This study of health-care providers, predominantly medical trainees and nurses, requesting palliative care consultation examined the aspects of prognosis discussed. While a majority of providers believed a prognosis discussion had occurred during their patient’s current hospital admission, some key aspects of prognosis were often not covered during these discussions. Moreover, several providers did not discuss the patient’s prognosis at all.
Life expectancy is a necessary component of prognostication used in formulating goals of care and is a topic that many patients and families expect to hear about toward the end of life.13,14 However, life expectancy and survival rates were not discussed in a substantial portion of prognosis discussions. Investigation was done using the open-ended question “If you did not use statistics in your discussion, why not?” The main theme in response to this question was lack of knowledge or uncertainty of the provider. It appeared that many providers did not supply statistics because they were not confident about probabilities related to the patient’s diagnosis. This answer supports the recognized complexities of prognostication. Forming an accurate prognosis can be difficult for many reasons. Many providers are inadequately trained in prognostication, trainees (i.e. residents) may have had limited experience with a particular disease, and few guidelines exist for communicating prognosis.10,11 Moreover, several studies have reported that physicians can be inaccurate when attempting to provide prognosis details, with some studies showing that physicians overestimate prognosis and others showing that they underestimate prognosis.15 –17 Many tools are available to assist with prognostication, but they vary in terms of accuracy and simplicity.18–20 With these barriers, health-care practitioners continue to be uncertain about a patient’s prognosis, making it difficult to discuss exact probabilities of various outcomes.
Another theme regarding use of statistics was that providers felt other specialties were better qualified to discuss statistics with patients. While providers may feel that specialists are more knowledgeable about survival rates, there is evidence that at least in oncology, clinical expertise of providers is not associated with better communication and increased understanding among patients. 21 A systematic review of prognosis discussions in cancer patients showed variable results in terms of whether oncologists provided accurate prognostic information to patients. 1
The final theme in respondents’ answers was that statistics were not relevant to the situation. Looking at survey response data, it appears that many physicians with this answer had consulted the palliative care team for pain. As noted by Van Mechelen et al. 22 in their recent review, there continues to be wide variability in the population receiving palliative care, including patients with complex symptom management needs who do not have a terminal illness. In these cases, life expectancy or survival rates may not be particularly relevant.
Another topic that was not included in several prognosis discussions was psychosocial concerns. Acknowledging the patient’s emotional concerns is an essential part of the prognosis discussion.13,23 Thus, it is concerning that many respondents did not address this matter. Studies have addressed physicians’ opinions of psychosocial issues and barriers that prevent them from incorporating psychosocial factors into practice. A report of qualitative interviews with 20 physicians practicing specialties in which palliative care was relevant showed that while most physicians interviewed felt that psychosocial factors played an important role in care of patients, there was variation in attitudes. 24 Lack of training and time constraints prevented some from addressing psychosocial factors.
While most respondents stated that they had addressed hope or reassurance in some manner, a few said that they had not discussed this topic in any way. One respondent commented that while reassurance had been discussed, “you can’t tell a patient with terminal illness that they still have options.” It may be that some providers are reluctant to discuss hope for fear of inflating patients’ expectations. Nevertheless, hope can be addressed in different ways. A few respondents to the survey commented that while they tried to be realistic, they also tried to offer hope to patients by saying that addition of palliative care could improve quality of life in their remaining days. Literature on communication at the end of life suggests that giving patients and families realistic methods of handling their futures while treating them with compassion allows them to prepare for the worst without losing hope. 25
In the 15 cases in which prognosis was not discussed, the most common reason for why prognosis was not discussed by surveyed providers was that the provider had difficulty in determining the patient’s prognosis. The next most common answer was that the patient was already aware of his or her prognosis because discussions had occurred in the past as an outpatient. Indeed, prognosis discussions benefit from multiple conversations with one provider as part of a long-term patient–provider relationship. However, patients may still benefit from additional prognosis discussions as an inpatient. Hospitalizations could be signaling a worsening of the patient’s chronic issue, such as discovery of cancer metastases, or could be from a new condition. It is likely that patients in these situations would need additional prognosis discussions. Moreover, some studies show that prognosis becomes more accurate as a patient is closer to death, and so patients with terminal illness may benefit from supplemental discussions regarding prognosis as they near the end.17,26 Patients’ prognoses may change for the better rather than for the worse. In one case during this study, the prognosis of the patient had changed as the survey was being administered to the patient’s health-care provider; the patient’s biopsy showed that the patient’s cancer type was one that was more treatable than originally anticipated. Thus, even within the hospital admission, the patient’s prognosis can change, requiring updated discussions.
There were several limitations in this study. In addition to a relatively small sample, the convenience sample consisted of health-care providers, primarily residents, who requested palliative care consultation in a large teaching hospital located in an urban area in the United States. Thus, the sample may not represent more experienced providers, the attitudes of those who do not request consultations, or the practices in smaller community facilities. In particular, practitioners who provide both inpatient and outpatient care for their patients, in contrast to the pattern found in many academic centers, may exhibit different behaviors regarding discussion of prognosis with patients with whom they have a long-standing relationship. In addition, the survey findings may not reflect the views of providers from other countries, where views and practices regarding prognosis discussions may differ from those in the United States. Finally, we obtained no clinical data about the patients, and information about patient condition (e.g. presence or absence of metastatic disease) may have shed more light on findings.
In conclusion, it appears that in the sample studied, prognosis was not consistently addressed with all patients, and certain key topics often were not covered during prognosis discussions. Uncertainty was the strongest theme in reasons for not discussing prognosis. This is consistent with current literature suggesting that prognostication is difficult for providers, many of whom have not had much guidance in the process of determining a patient’s prognosis. Palliative care physicians, who have specialized training and experience with prognostication and delivering prognostic information to patients, may be an essential resource to health-care providers who have difficulty navigating through this complex process. In addition, our findings point to the need to develop educational strategies to better prepare trainees for the difficult task of talking with patients and families about all aspects of prognosis and evaluating the effectiveness of these conversations.
Footnotes
Acknowledgements
The authors would like to thank the Palliative care team at University Hospitals Case Medical Center for their support and cooperation. This study of human participants was approved by the Institutional Review Board of University Hospitals Case Medical Center.
Declaration of conflicting interests
No authors had any conflicts of interest influencing the content of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.