
Abstract
Background:
Managing medications is a complex responsibility of family caregivers caring for end-of-life patients. This study characterizes caregivers with and without formal/informal support managing medications for patients who receive end-of-life care at home.
Aim:
To explore factors related to caregivers’ support with managing medications for end-of-life home hospice patients.
Design:
A convenience-sampled, cross-sectional telephone survey.
Setting/participants:
Computer-assisted telephone interviews were administered to 120 caregivers managing medications, who were referred by five Chicago-based home hospice services. We measured caregivers’ additional formal (paid) and informal (unpaid) support with managing medications, and caregiver/patient socio-demographic, relational, and health characteristics.
Results:
While 47 (39%) had no additional support with managing medications, 27 (22.5%) had formal support, 37 (31%) informal, and 9 (7.5%) both. Seven caregivers (19%) with formal and 13 (31%) with informal support reported disagreements concerning treatment plans. Caregivers lacking formal support tended to be racial/ethnic minorities, live with the patient in their home, or report greater emotional burden. Caregivers with formal support tended to report higher education/income, lower mutuality, or care for a patient with over 6 months’ hospice enrollment. Caregivers lacking informal support tended to be spousal caregivers, live with the patient, or have experience caring for another dying person.
Conclusion:
Our study suggests that high proportions of caregivers may not have support managing medications for patients receiving hospice care at home. More research should examine whether the observed variations in obtaining support indicate disparities or unmet needs among caregivers. Disagreement about treatment with formal/informal support also warrants further investigation.
Patients receiving hospice care at home represent a unique challenge to their families or loved ones, who want to care for them while allowing them to remain at home near the end of their lives.
Finding ways to better assist these caregivers is an important challenge both at the individual level (difficulty managing pain and symptoms) and the population level (aging of the population, cost and burden of caregiving, etc.).
This study describes the possible extent to which caregivers of hospice patients receiving end-of-life care at home may lack additional support with managing medications for the patients.
This study also identifies factors that may be associated with a lack of additional support (both informal/unpaid and formal/paid help) with medication management.
This study identifies potential characteristics that could be targeted for future interventions to help caregivers receive additional formal or informal support.
Our findings inform future research directions to determine whether the observed variations in having additional support are indications of disparities or unmet needs among caregivers of patients receiving hospice care at home.
Introduction
Over 20 million Europeans and 61.8 million Americans self-identify as caregivers of someone living at home,1,2 numbers which are expected to increase across the European Union (EU). 3 A survey of Organization for Economic Cooperation and Development (OECD) countries estimates that 8%–16% of the population serves as family caregivers. 4 Family caregivers are critical in optimizing health and quality of life for older patients. 5 Additional support from caregivers’ friends/family is their most common, “front-line” help.6,7 However, many report lacking additional support,5,8 particularly caregivers aged 65+ years. 1 Although the lack of informal (defined here as unpaid) support could be alleviated by formal (defined as professional/paid) services, their use is documented to be low, particularly in minority subpopulations and southern Europe.2,9–11 In the EU, patterns of caregiving and support are divided along geographic lines, with residents of northern Europe likelier to report greater and more formal support than those in southern Europe. 3 Low levels of support can adversely affect caregivers psychologically and physically, and their ability to care for patients.12,13
A review of end-of-life research in Europe found that caregivers report feeling overwhelmed, and needing additional support and information with multiple caregiving tasks. 14 In addition, caregiving is linked to caregiver health decline,15–18 and poverty 4 and low levels of support can exacerbate these declines.12,19 Caregivers’ health decline can also deleteriously affect their patient care. 20 For these reasons, clarifying the relationship between a caregiver’s additional support and their experiences in giving care is a research priority in the United Kingdom and elsewhere.21,22
Particularly concerning are family caregivers of patients receiving end-of-life care at home,23,24 prompting international calls for greater understanding of and assistance to them. 25 End-of-life caregiving presents not only grief with which to cope, but also complex responsibilities that pose physical and emotional stress26,27 and impede caregivers’ effectiveness.20,28 Among these responsibilities, medication management (e.g. adherence, administration, monitoring therapeutic and adverse effects) is particularly crucial to alleviating patients’ suffering. 29 Prior studies have found that effectively managing end-of-life medications requires complex knowledge and skills, and that caregivers report feeling underprepared to do so.30,31 Although hospice providers serve as primary sources of assistance with end-of-life patients,32,33 they report systematic barriers to facilitating caregivers’ medication management; 34 additional support beyond hospice may be necessary.
Additional support for caregivers has been described as important to effective medication management; 35 however, little is known about the formal or informal support caregivers receive to manage medications for end-of-life (as defined in the United States by the Medicare hospice benefit) patients at home. 36 The objective of this study is to characterize caregivers having or lacking additional formal/informal support with managing medications for elderly hospice patients, using key characteristics previously identified as barriers to caregiving and managing medications.34,37–39 Our findings may help identify subgroups of caregivers at greatest risk of lacking formal and/or informal support with medication management, and thereby inform the development of targeted interventions.
Methods
Study design/participants
The Institutional Review Board, an independent expert panel that reviews human subjects’ research for ethical compliance, approved this study (NUIRB#1511-006 and UICIRB# 2010-0930). From 2009 through 2012, we purposively selected five hospice agencies providing similar home-based end-of-life services in the greater Chicago areas based on ownership (one for-profit, four not-for-profit) and daily census (one with <100 patients, one with 100–200 patients, three with >200 patients). These hospice providers (namely, a nurse, social worker, chaplain, and physician) provide services tailored to the health and support needs of the patient/caregiver by visiting their home to provide comfort care. We approached these providers at each agency and asked for referrals of their patients receiving end-of-life care at home and the corresponding primary informal caregiver on record. We then contacted only the caregivers by phone to explain the study, obtain their consent, recruit them, and schedule telephone interviews with the caregivers within the subsequent week. Eligible caregivers had to (1) be unpaid, aged 18+ years, English-proficient, and self-identified as primary caregiver; (2) have medication responsibilities for a home hospice patient aged 60+ years; and (3) have no cognitive/sensory deficits precluding a telephone interview. Recruitment ended when we reached our sample size goal of 120 caregivers.
For this cross-sectional study, we analyzed data on enrolled caregivers who completed a 45-min, computer-assisted, telephone interview. Questions were administered verbally over the phone and entered directly into a computerized instrument in which entered data are stored real-time. At the study’s conclusion, clinical personnel at each hospice agency provided information on patient date of death (if deceased). Study investigator B.T.J. conducted all interviews and obtained informed consent for all participants immediately prior to the interview, including notification of the potential risk of distress. B.T.J. was prepared to provide verbal support over the phone; allow caregivers to take breaks, end interview, or withdraw from study; and contact hospice agencies for additional support if necessary. Fortunately, actual distress experienced was not documented among any caregivers, and many caregivers reported feeling less distressed after the interview.
Survey
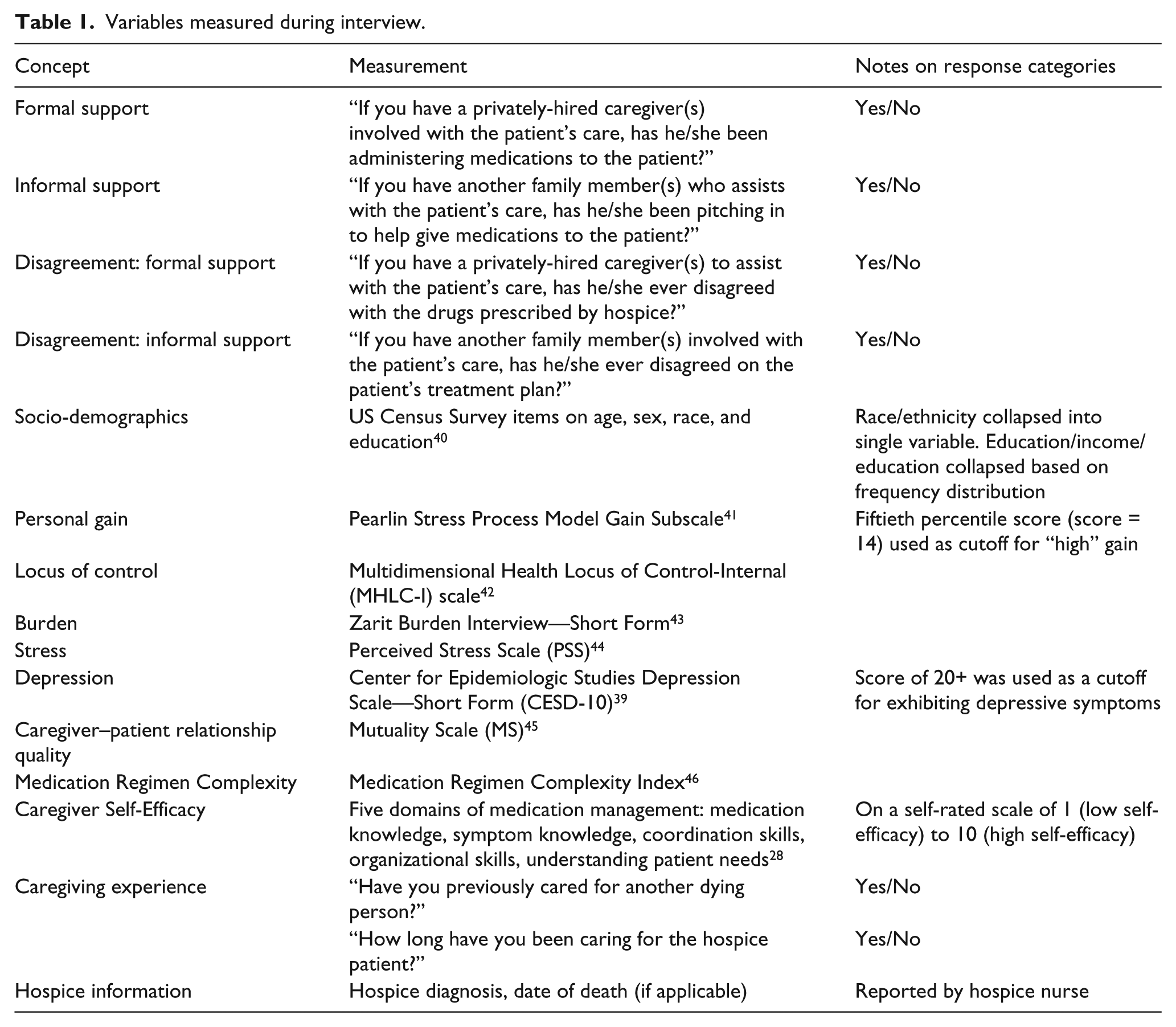
The survey assessed caregiver and patient socio-demographics, additional support, caregiver–patient relation, caregiving experience, caregiver’s psycho-emotional health, and medication management (Table 1). Where available, the survey included previously validated instruments.29,40–47 To assess feasibility and comprehensibility, we beta-tested the survey by conducting cognitive interviews with five eligible caregivers and used these results to refine survey administration.
Variables measured during interview.
Analysis
We conducted univariate analyses using frequency distributions for categorical variables, and means and standard deviations for continuous variables. Because few respondents had missing data, we compared a mode imputation 48 (imputing income data for five respondents and stress data for one) to a complete case analysis. Upon finding no noteworthy differences in our parameter estimates between the two methods, we opted to use mode imputation for our final results so as to maximize the reportable sample size. Our outcome was a constructed four-category variable reflecting each combination of Q1 and Q2 (see Table 1): (1) “no formal or informal support,” if no to both; (2) “only formal support,” if yes to Q1 and no to Q2; (3) “only informal support,” if no to Q1 and yes to Q2; and (4) “both formal and informal support,” if yes to both. Due to low sample size, we opted to collapse categories (2) and (4), as based upon our experience with this population we felt that caregivers with formal support were more likely to share characteristics than those with informal support. This resulted in three analytic subgroups: “no formal or informal support,” “any formal support,” and “only informal support.” Using SAS version 9.1, we conducted bivariate, generalized logistic regression to determine associations between having formal or informal support with medication management (compared to having no support) and each independent variable.
Results
For the overall study, 204 caregiver–patient dyads were referred and 144 were screened and determined as eligible to participate. Among them, 5 dyads completed beta-tests (see “Methods” section) and 19 were never interviewed due to dropout/loss to follow-up. Therefore, 120 (86.3% = 120/139) completed the survey (Figure 1).
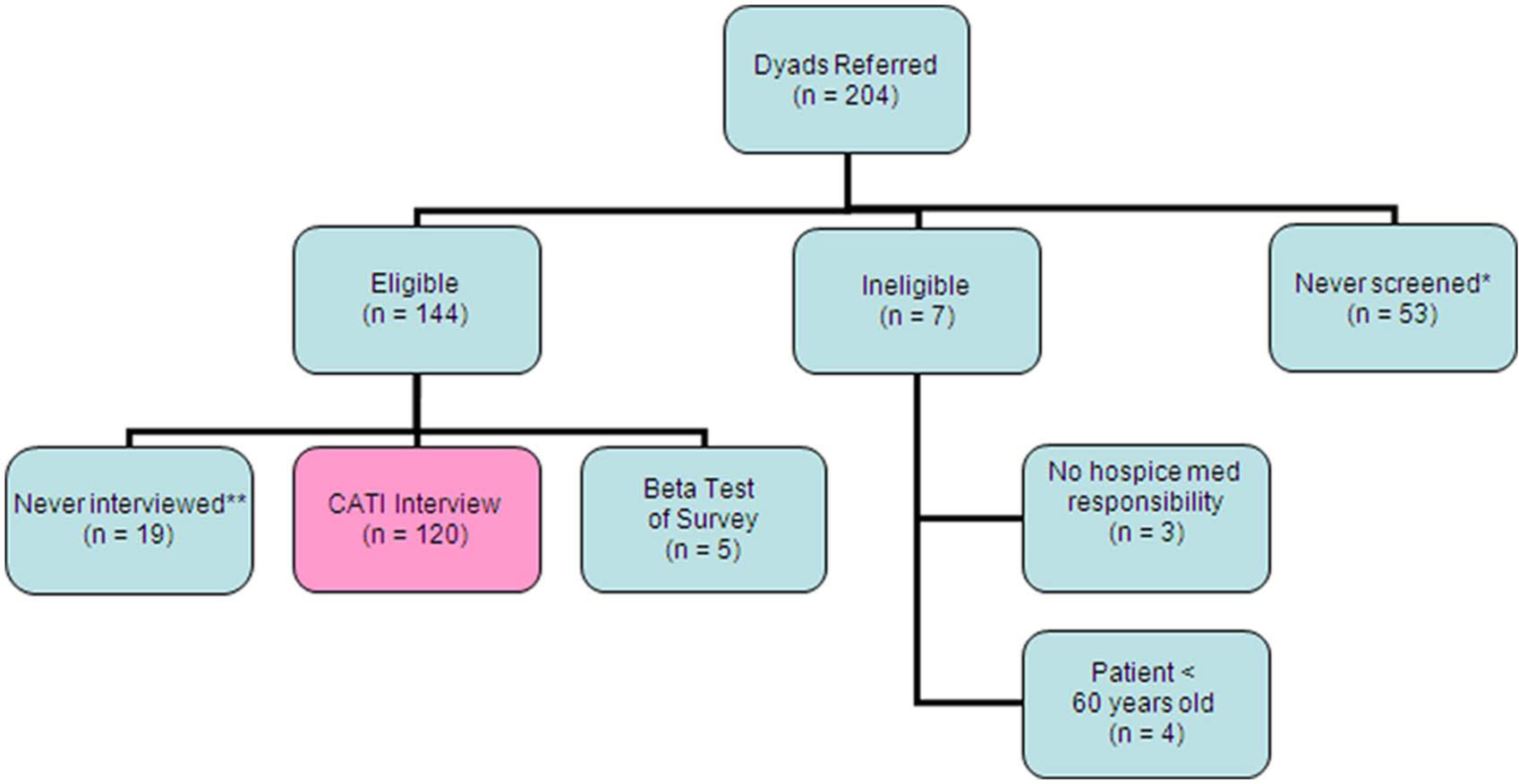
Diagram of dyads recruited/surveyed.
Caregiver and patient characteristics
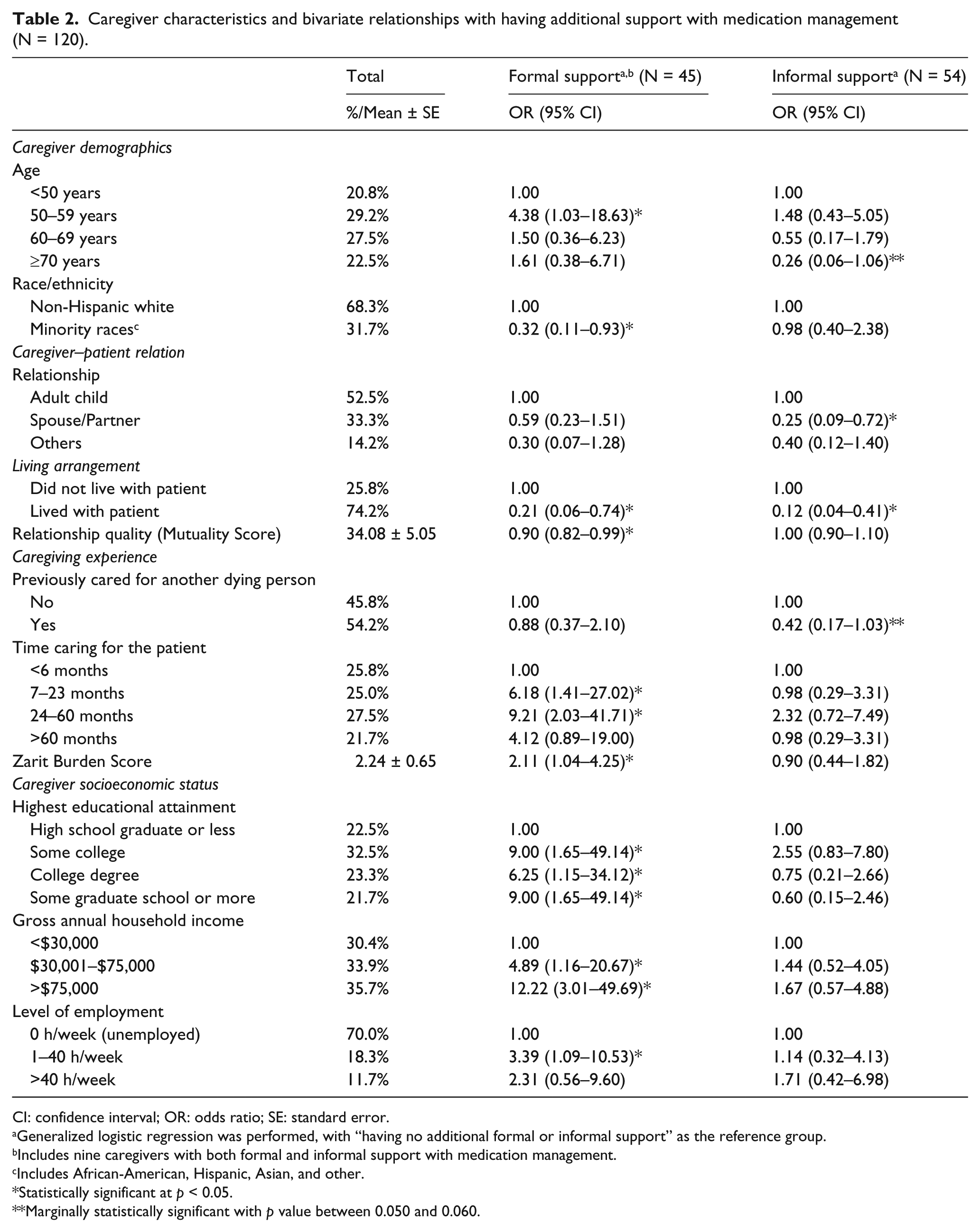
Among 120 participating caregivers, half were aged 60 years or older (Table 2) and most were female (83%) and non-Hispanic white (68%). Minority races included 20% black, 7% Hispanic, and 5% Asian/others. Slightly more than half were adult children and most lived with their patient. Slightly over half had previously cared for another dying person and almost half had been caring for the patient for 2 years or more. Over half did not have a college degree, nearly a third had an annual income of US $30,000 or less, and the majority of them were unemployed.
Caregiver characteristics and bivariate relationships with having additional support with medication management (N = 120).
CI: confidence interval; OR: odds ratio; SE: standard error.
Generalized logistic regression was performed, with “having no additional formal or informal support” as the reference group.
Includes nine caregivers with both formal and informal support with medication management.
Includes African-American, Hispanic, Asian, and other.
Statistically significant at p < 0.05.
Marginally statistically significant with p value between 0.050 and 0.060.
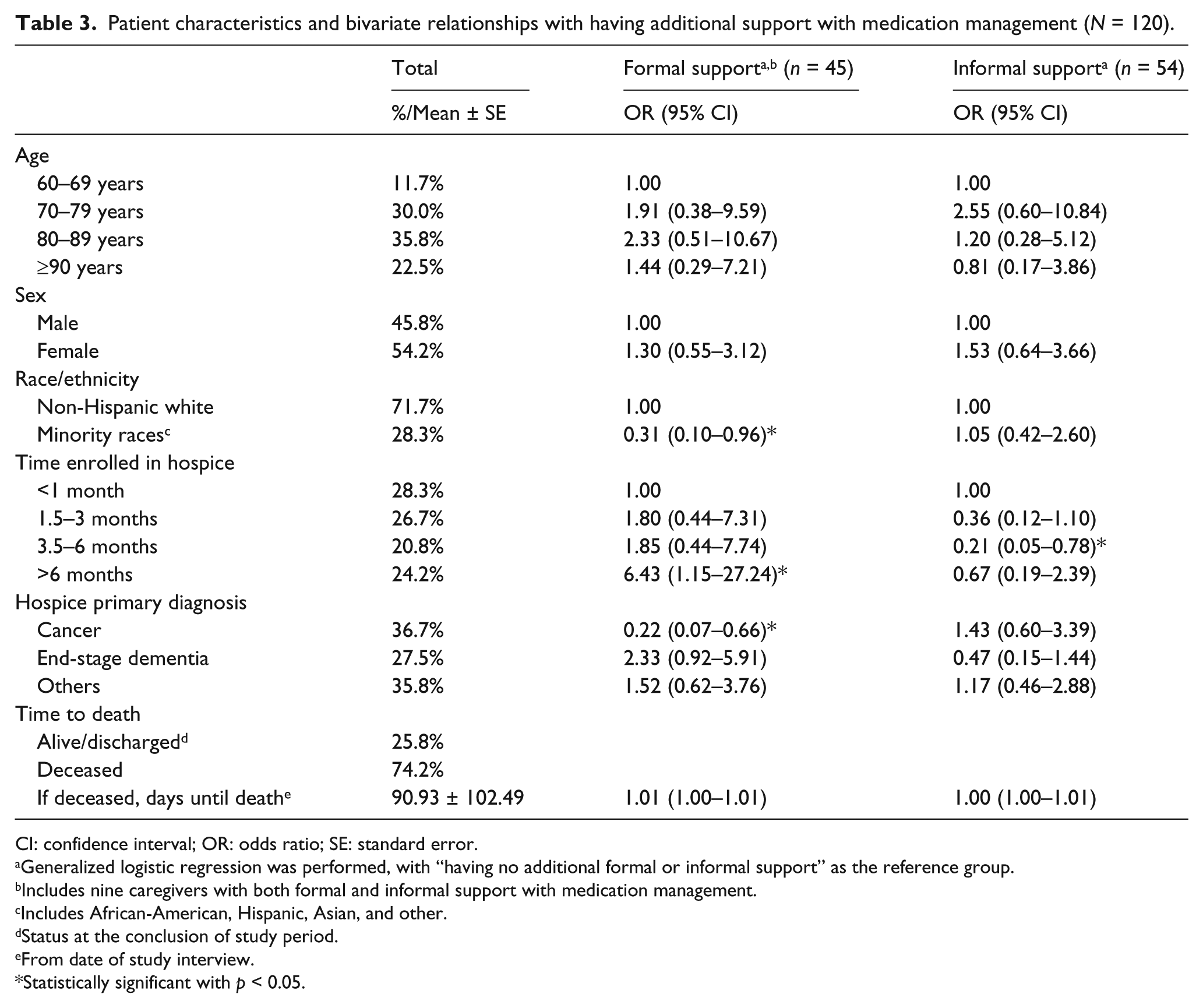
Most respondents were caring for a patient who was at least 80 years old, female, and non-Hispanic white (Table 3). Minority races of patients included 20% black, 7% Hispanic, and 2% Asian/others. Over one-third cared for a cancer patient and over one-quarter for someone with end-stage dementia.
Patient characteristics and bivariate relationships with having additional support with medication management (N = 120).
CI: confidence interval; OR: odds ratio; SE: standard error.
Generalized logistic regression was performed, with “having no additional formal or informal support” as the reference group.
Includes nine caregivers with both formal and informal support with medication management.
Includes African-American, Hispanic, Asian, and other.
Status at the conclusion of study period.
From date of study interview.
Statistically significant with p < 0.05.
Formal/informal support and disagreements
About 39% had no additional formal or informal support with managing the patient’s medications (Table 4). Almost equal proportions had any formal support (30%) and only informal support (31%) with medication management, and nine respondents (7.5%) had both formal and informal support. Furthermore, 19% of respondents with formal support and 35% of those with informal support reported experiencing disagreement with their additional support regarding the patient’s hospice treatment plan.
Caregivers’ additional formal/informal support with medication management for home hospice patients (N = 120).

Includes nine subjects with both formal and informal support with medications.
Associations with formal support
Compared to those below 50 years of age, respondents who were 50–59 years of age tended to have formal support (p = 0.046) (Table 2). Respondents who were racial/ethnic minorities or living with the patient tended to lack formal support (p = 0.036 and p = 0.015, respectively). Having formal support was also associated with lower mutuality score (p = 0.027) and longer duration caring for the patient (7–23 months, p = 0.016; 24–60 months, p = 0.004; compared to under 6 months).
Having formal support was associated with higher education attainment (some college, p = 0.011; college degree, p = 0.034; some graduate school or more, p = 0.011; compared to “high school graduate or less”); and higher gross annual income ($30,000–$75,000, p = 0.031; > $75,000, p < 0.001; compared to “≤$30,000”). Respondents working 40 or fewer hours weekly tended to have formal support compared to respondents who were unemployed (p = 0.035).
Similar to caregiver race/ethnicity, respondents caring for minority patients tended to lack formal support (p = 0.042) (Table 2). Respondents who were caring for patients with hospice enrollment over 6 months tended to have formal support (p = 0.012) relative to those with patients enrolled for 1 month or less. Finally, respondents caring for a patient with cancer tended to lack formal support (p = 0.007). Caregiver self-efficacy in medication management and medication regimen complexity was not statistically associated with having formal support.
Associations with informal support
Compared to those below 50 years of age, respondents who were over 70 years of age tended to lack informal support (p = 0.0597, marginally significant) (Table 2). Compared to adult children, spouses/partners tended to lack informal support (p = 0.010), as did respondents who lived with the patient (p < 0.001). Finally, compared to respondents caring for patients with hospice enrollment shorter than 1 month, those with patients enrolled in hospice between 3 and 6 months tended to lack informal support (p = 0.020) (Table 3). Caregiver self-efficacy in medication management and medication regimen complexity were not statistically associated with having informal support.
Discussion
This descriptive study found characteristics associated with the presence or absence of formal/informal support for caregivers managing medications for elderly home hospice patients. Not only did a large proportion of participating caregivers (~40%) report no additional support with medication management, but many characteristics (such as racial/ethnic minorities and low socioeconomic status) previously identified as barriers to caregiving tasks and managing medications34,37–39 were inversely associated with having support with medication management. Other factors (low caregiver self-efficacy, greater number of medications) previously linked with worse patient pain/quality of life17,38 were not associated with additional support, which may indicate an unmet need for caregiver support with medication management.49,50 The most pronounced finding regarding length of hospice enrollment was that caregivers of patients with more than 6 months of enrollment tended to hire formal support (unadjusted odds ratio = 6.43; p = 0.012) compared to caregivers of patients in hospice for 1 month or less. A potentially related finding in this study is that caregivers of cancer patients tended to lack formal support, perhaps due to shorter post-enrollment survival. Finally, even among participants reporting some sort of additional support, notable percentages (19% of those with formal and 31% of those with informal support) reported disagreements with that additional support.
These findings complement the results of other studies in the field, although to our knowledge this is the first study to look at support with medication management specifically. Others have reported lower percentages of caregivers (ranging from 15% to 20%) lacking additional support with unspecified caregiving tasks;6,7 our larger finding therefore suggests that fewer caregivers may rely on support for medication-related duties. 12 At the same time, the association between formal support and duration of hospice enrollment reflects prior evidence that formal support tends to supplant informal support over time due to increasing caregiver burden and the patient needs exceeding the caregiver’s capacity to provide care.6,7 In light of several international data sets 51 reflecting widespread preference on the part of caregivers for additional support/guidance, this may indicate an unmet need. Our findings characterizing caregivers with and without additional support suggest that caregivers with difficulty managing medications may share similar characteristics with caregivers not accessing additional support. For example, we found that racial/ethnic minority caregivers tended to lack formal support and association, consistent with previous research,10,52 this potentially reflects cultural differences regarding use of formal care or disparities in income/resources to obtain paid services. Furthermore, this study did not find that racial/ethnic minority caregivers tended to have informal support to compensate, raising possible concerns about the adequacy of support minority caregivers are receiving. Finally, the prevalence of disagreement we found between primary caregivers and additional support may undermine the assumption that merely having additional support necessarily provides a benefit for caregivers and patients. Disagreements may adversely affect caregivers’ psycho-emotional health 53 and ability to care for the patient.
Our results suggest several ways in which hospice providers can target interventions to alleviate lack of support and/or potentially improper medication management. Subpopulations characterized by both medication management difficulty and lack of access to additional support (e.g. racial/ethnic minorities) should be targeted for additional intervention by hospice support teams. Targeting caregivers with low self-efficacy and those managing complex medication regimens may also be necessary to ensure adequate support with medication-related tasks. More efforts may also need to ensure that caregivers of cancer patients, whose late entry into hospice 54 may restrict opportunities to obtain formal support, are adequately supported with managing medications. 17 Finally, hospice providers may need to actively assess potential disagreements between caregivers and formal/informal support and to effectively intervene if disagreements are identified. Future research may need to consider disagreement as an important mediating factor in caregiving processes.
It is interesting to note that we find that caregivers reporting lower mutuality scores (poorer relationships) tend to hire formal support to manage medication. While reasons underlying this association cannot be determined within this study, such findings suggest practice implications for providers. For example, formal support may reflect certain underlying caregiver–patient relationship dynamics to which hospice providers may need to pay special attention while coordinating care with caregivers and delivering services to patients in private residences.
Regarding limitations, given the cross-sectional study design and the lack of multivariate regression analysis, the observed associations between variables should not be interpreted as causal. Both formal and informal support were measured crudely with dichotomous variables; therefore, we could not examine the amount of time/additional support, qualifications of formal/informal support, or the amount and type of care provided by the additional support to caregivers in managing medications. Our convenience sample, predominantly white, female, educated, and having higher income, cannot be generalized to other populations. Our small sample size may have contributed to non-significant or marginally significant findings observed in the study.
Family caregivers play a key role in caring for patients who elect to receive hospice care at home near their end of life. Effective medication management, in particular, is important for adequate pain and symptom control for these patients. Our study suggests that high proportions of caregivers may not receive additional support to perform medication responsibilities and, among caregivers with additional support, sizable proportions may encounter disagreements concerning treatment plans with their support. As the current population ages across a number of countries, caregivers are projected to have even less access to informal support than previous generations,55,56 underscoring the need to ensure adequate access to formal support that is of high quality, acceptable, and substitutable for informal support. Future studies will need to replicate our findings and examine whether the observed variations in having formal/informal support are indications of systematic disparities or unmet needs.
Footnotes
Acknowledgements
The authors would like to express gratitude to all the participating hospice organizations (Horizon Hospice and Palliative Care, Midwest Palliative and Hospice CareCenter, Seasons Hospice and Palliative Care, Northwestern Memorial Palliative Care and Home Hospice Program, Rainbow Hospice and Palliative Care, and Presbyterian Homes), care providers, and informal caregivers for their valuable insights and support in this study. They are also grateful to Drs Celia Berdes, Chih-Hung Chang, Linda Emanuel, Joshua Hauser, Judith Kasper, Judith Paice, Simon Pickard, Robert Schrauf, and Whitney Witt for their assistance during the early stages of the study. The authors further thank Ms Janie Urbanic for her research assistance, as well as Christopher Lyttle and Raymond Kang for their data management support. Institutional Review Board approvals were obtained from Northwestern University and the University of Illinois at Chicago. This study was conducted in compliance with the STROBE guidelines for observational studies.
Declaration of conflicting interests
No competing financial interests exist. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health, the National Institute on Aging, the Centers for Disease Control and Prevention, or the National Center for Health Statistics. The sponsor—National Institute on Aging—has no role in the design, methods, subject recruitment, data collection, analysis, or preparation of this article.
Funding
At the time when this research was conducted, Dr Denys T Lau was affiliated with the University of Illinois at Chicago, College of Pharmacy. This work was supported by the United States National Institute on Aging (Grant Number K01AG027295 to Principal Investigator: Denys T Lau).