
Abstract
Background:
The majority of children and young people who die in the United Kingdom have pre-existing life-limiting illness. Currently, most such deaths occur in hospital, most frequently within the intensive care environment.
Aim:
To explore the experiences of senior medical and nursing staff regarding the challenges associated with Advance Care Planning in relation to children and young people with life-limiting illnesses in the Paediatric Intensive Care Unit environment and opportunities for improvement.
Design:
Qualitative one-to-one, semi-structured interviews were conducted with Paediatric Intensive Care Unit consultants and senior nurses, to gain rich, contextual data. Thematic content analysis was carried out.
Setting/participants:
UK tertiary referral centre Paediatric Intensive Care Unit. Eight Paediatric Intensive Care Unit consultants and six senior nurses participated.
Findings:
Four main themes emerged: recognition of an illness as ‘life-limiting’; Advance Care Planning as a multi-disciplinary, structured process; the value of Advance Care Planning and adverse consequences of inadequate Advance Care Planning. Potential benefits of Advance Care Planning include providing the opportunity to make decisions regarding end-of-life care in a timely fashion and in partnership with patients, where possible, and their families. Barriers to the process include the recognition of the life-limiting nature of an illness and gaining consensus of medical opinion. Organisational improvements towards earlier recognition of life-limiting illness and subsequent Advance Care Planning were recommended, including education and training, as well as the need for wider societal debate.
Conclusions:
Advance Care Planning for children and young people with life-limiting conditions has the potential to improve care for patients and their families, providing the opportunity to make decisions based on clear information at an appropriate time, and avoid potentially harmful intensive clinical interventions at the end of life.
Keywords
Currently, most childhood deaths occur in hospital, commonly in intensive care. Most children and young people (CYP) who die have a pre-existing life-limiting illness.
Decision-making about whether to continue or stop delivery of invasive intensive care interventions at the end of life presents complex moral and ethical dilemmas, especially in relation to CYP with life-limiting illnesses.
Advance Care Planning (ACP) is a process by which patient and family preferences for end-of-life care, including preferred place of death, can be considered.
This study provides an in-depth qualitative exploration of the experiences and perceptions of Paediatric Intensive Care Unit (PICU) senior doctors and nurses around the provision of care, including ACP, at the end of life to CYP with life-limiting illness.
The results offer insight into the complexity of decision-making and the difficulties faced with ACP for this population.
The study contributes to the growing evidence in favour of ACP to prioritise and facilitate patient and family choice at the end of life.
This study contributes to the growing evidence base in favour of timely ACP.
There is a need for education of healthcare professionals around recognition of life-limiting illness, palliative and end-of-life care and ACP.
ACP is described as a process with potential benefits for those involved in complex end-of-life care decision-making, specifically regarding the delivery of invasive life-sustaining treatment. Further research is necessary to explore the benefits and barriers to ACP from the perspective of patients and families.
Introduction
Around 70% of children and young people (CYP) who die in England have complex, life-limiting conditions and associated palliative care needs.1,2 The number of CYP living with these conditions is rising,3,4 making the end-of-life care for such patients an important issue to consider.
The death of a child is a profound, unique and devastating event.5,6 It is well recognised that for those with life-limiting illness, the delivery of integrated, holistic healthcare can improve patient experience at the end of life. Advance Care Planning (ACP) offers a means of eliciting patient and family choice to guide the delivery of such care during acute deteriorations in health and at the end of life.7,8 ACP is a formal process of discussion between an individual, their care providers and those close to them, which enables the recognition of preferences for care,9,10 and therefore allows patients and families to achieve some sense of control in their situation.11–13 The development of both a ‘child and family care plan’ and an ‘end-of-life care plan’ is recommended in the UK Together for Short Lives Standards. 14
The importance of recognising that a condition is life-limiting in nature, 15 starting discussions early and involving CYP (where possible) and their parents in decision-making is widely acknowledged.16–18 However, these discussions can be challenging, particularly at times when the child or young person’s condition is stable and initiating decision-making about end-of-life care may appear premature.11,19 There is also evidence that healthcare professionals may be more ambivalent about these difficult conversations than families.13,16 Lack of openness can have negative consequences for the quality of care delivered, resulting in fear of the dying process, lack of knowledge about local services, poor communication between family members and isolation of the bereaved. 20
Evidence is emerging to suggest that families facing the death of a child wish for well-coordinated healthcare, with the option of this care being delivered in the home environment.21–23 However, currently the majority of children who die, do so in hospital,2,4 most frequently in an intensive care environment.24–26 Paediatric Intensive Care Unit (PICU) is, therefore, an important setting in which to investigate current practice around ACP and the delivery of end-of-life care for CYP with life-limiting illness.
The provision of PICU services has increased since the 1960s with advances in sophisticated medical interventions and technology which have changed the care of critically ill or injured children. 27 PICU is an emotionally charged, high-pressure, highly technological environment. 28 Children admitted to PICU are the most seriously unwell, often with complex long-term conditions which are life-limiting in nature.24,26,29 PICU staff become responsible for managing end-of-life care, including the ACP process if these discussions have not previously taken place, once intensive treatment options have been exhausted. They are faced with complex and emotive ethical dilemmas, including the withdrawal or limitation of life-sustaining interventions, which is the most common mode of death in Northern European PICUs.25,26,28,30–33
ACP and end-of-life care decision-making in the PICU environment is particularly challenging for many reasons. PICU staff often have to proceed with these discussions during an acute deterioration in a patient’s clinical condition, at a time when family members have little time to adjust and may be experiencing the early stages of a bereavement reaction, including denial and anger. 34 Frequently, there are many teams of professionals involved. Situations where multi-disciplinary consensus opinion and ‘collective decision-making’ cannot be achieved can cause frustration among clinical colleagues and false hope for families. 35 Currently, there is a lack of consensus in approach and documentation of care plans,12,19,36,37 and evidence to support the benefits and perceived risks of formal ACP documents for patients, their families and healthcare professionals is lacking. 19
There is a need to enhance the evidence base for ACP for CYP. The aim of this study was to investigate current practice in ACP and how this might be improved, by exploring the experiences and perceptions of senior PICU medical and nursing staff who are frequently involved in managing end-of-life care for CYP.
Methods
Qualitative interviews
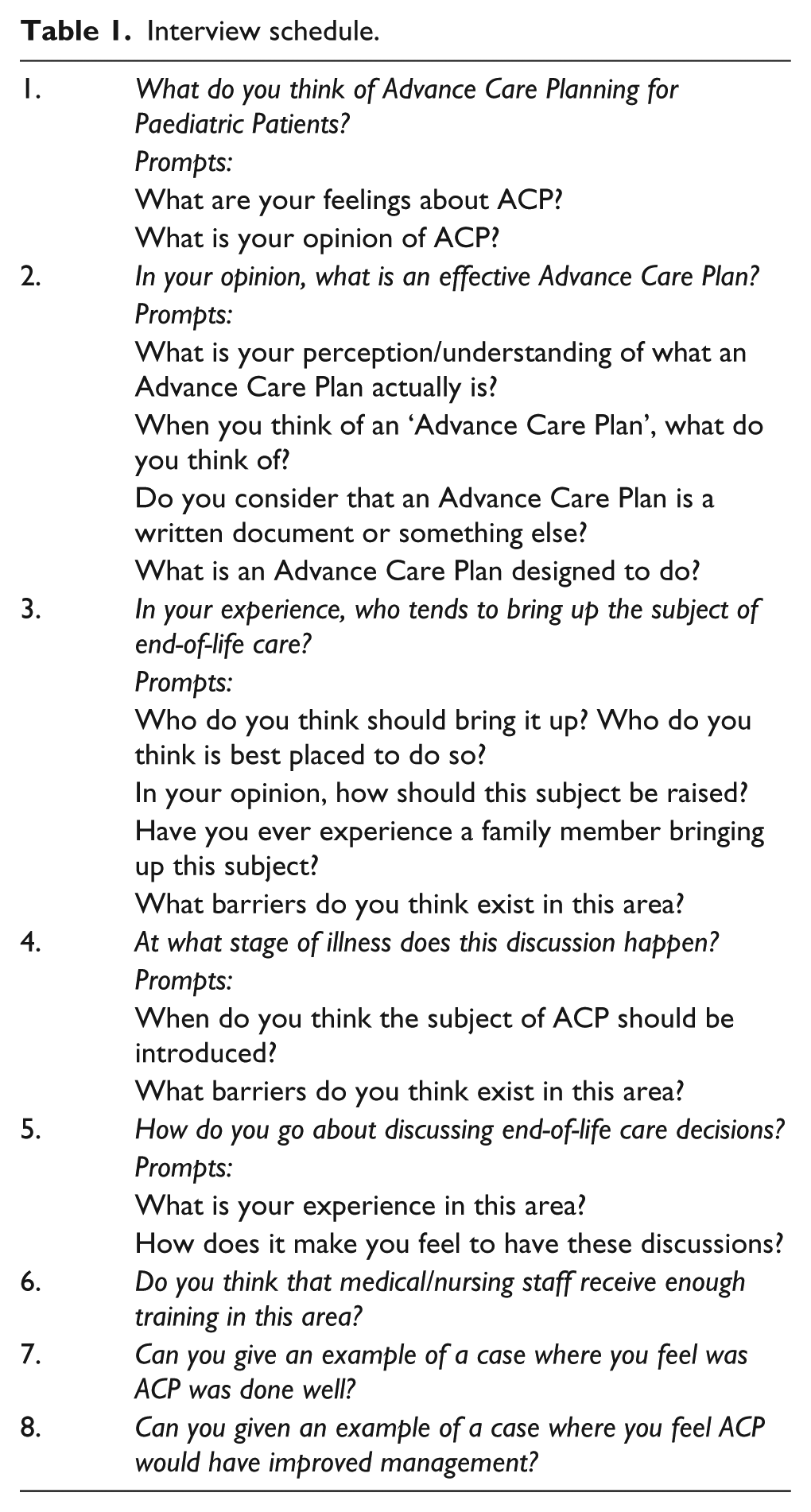
A qualitative interview study was conducted, to elicit rich contextual data regarding participants’ experiences and perspectives around caring for CYP with life-limiting illness in the PICU. The open approach and confidential nature of the interviews allowed participants to disclose freely their thoughts and describe their experiences. The interview was semi-structured and followed an interview schedule (Table 1), which comprised open questions and a series of prompts to guide the interview, but was not rigid or exhaustive, allowing flexibility to explore important themes that became apparent during each interview. It was informed by relevant literature and underwent minor modification according to emerging findings, throughout the interview process. Interviews were conducted until the point at which no new information (data saturation) was elicited around the main themes.
Interview schedule.
S.M. conducted the interviews following training in qualitative interview techniques as part of an MSc in Palliative Medicine, supervised by J.D. All interviews were conducted in a quiet room close to the PICU and were digitally recorded.
Setting
The study was conducted in the PICU of a tertiary referral centre children’s hospital in the United Kingdom (Birmingham Children’s Hospital), which, with over 1400 admissions per year and 28 PICU beds at the time of this study, is one of the largest PICUs in the United Kingdom. 38 Local admission criteria define that admission to the Neonatal Intensive Care Unit (NICU) occurs from labour ward or a postnatal ward only. Otherwise, all critically unwell neonates and children are admitted to the PICU.
The number of deaths in the PICU in 2010 was 73, which equates to one or two deaths per week, an expected number for a PICU of this size (Standardised Mortality Ratio (SMR) of <1 when adjusted for severity of illness).
At the time of the study, a local Paediatric Palliative Care Toolkit including a formal ACP document had just been developed and launched, but was not widely in use. 39
Participants
Consultants and senior nursing staff (including matrons, and those with leadership and managerial roles within PICU) were invited to participate in the study. Verbal and written consent to interview were obtained. Interviews were carried out between July and September 2011.
Data analysis
Interviews were transcribed verbatim and anonymised. Participants were allocated identifiers according to their professional group (doctor = D, nurse = N). S.M. then undertook a detailed familiarisation process with the data, followed by the identification of summary statements (open codes) that described every element of the interview. The themes emerging from this list of open codes were consolidated and divided into broad overarching categories, and from this list of categories, a final coding framework was derived. The transcripts were then reviewed and every section of each interview colour coded to an allocated category, to produce an organised dataset. 40 For the purposes of this study, this process was completed manually, without the use of qualitative data analysis computer software.
A selection of transcripts were reviewed and independently coded by J.D. in order to decrease lone researcher bias and increase the validity of the study. The coding frameworks from these analyses were compared, allowing further development of categories and themes41,42 and a plan to present the themes in a systematic way to reflect phases of illness towards the end of life.
Ethical approval
The research protocol was granted ethical approval from The Birmingham East, North and Solihull Research Ethics Committee in June 2011 (REC reference: 11/WM/0157).
Findings
A total of 14 semi-structured interviews were carried out between August and October 2011. All individuals who were invited to participate agreed to do so. The sample comprised eight PICU consultant and six senior nurses (bands six and seven), all of whom have experience of end-of-life care and ACP for paediatric patients with life-limiting illness. Years of experience in these roles at the PICU ranged from 2 to 26 years.
Four main themes emerged: recognition of the child’s illness as ‘life-limiting’; ACP as a multi-disciplinary, structured process; the value of ACP and adverse consequences of inadequate ACP.
Recognition of a life-limiting illness trajectory
Lack of diagnostic precision provides an obstacle to undertaking ACP. In paediatrics, clear diagnoses frequently cannot be applied, with some complex metabolic and neurodegenerative conditions being particular to just one child. Participants described recognition of the child’s illness trajectory as a key barrier to initiating ACP. Participants described a need for earlier recognition of life-limiting conditions in order to permit earlier ACP, rather than waiting until all therapeutic options had been exhausted:
it’s almost like relapsing remitting MS [multiple sclerosis], they get relapsing remitting ICU and their relapses occur more frequently and last longer. (D1)
Participants described experiences where gaining consensus among the healthcare professionals involved had been a significant barrier to the ACP process. Different clinical judgements, including management of clinical risk and expectations around what can be achieved through medical intervention, all contributed, as well as different ethical and moral attitudes:
we can be a lot more proactive given the opportunity, but often we’re just trying to, er, persuade our colleagues who are providing care at the time, long before I see admission [to PICU], to raise the point. (D4) before you can convince any parents, you have to convince the other specialties. You have to bring them on board. If they’re not on board, you have no chance, or your chances with the family are much much less. (D7)
Nursing staff were described as most frequently being the health professional who identified deterioration in a child’s condition towards the end-of-life phase. Occasionally, it was parents who raised the issue of end-of-life care, in particular where they had witnessed their child having multiple admissions to PICU involving invasive treatments or resuscitation:
often the nurses are way ahead of us, often the nurses are the people who suggest it … And sometimes it’s us who realise. Sometimes it’s the specialty consultants realise enough is enough. It’s rare for the families to suggest it, but I have had families suggest it to me. (D1) parents who have seen their children having very umm, frightening events, life threatening events, cardiac arrest, the parents that have witnessed a number of cardiopulmonary resuscitations, they’ll get to a point where they can’t watch it anymore. (D2)
ACP as a multi-disciplinary, structured process
ACP was unanimously considered to be a ‘good idea’ or ‘essential’ among participants. All recognised the multi-disciplinary, dynamic nature of the process. Multiple barriers to successfully managing the process were identified, including time constraints, conflicting clinical demands and lack of formal training in communication skills. In the PICU setting, a lack of established rapport with the family before having to raise the issue of end-of-life care for the first time during acute situations, including resuscitation, was identified as causing particular difficulty:
it’s very difficult for us, because it is usually in the acute settings, unusual that we even get an opportunity to speak to them before the breathing tube goes down. (D5) It [ACP] should have happened before they came to ICU, for a lot of children. And I know the challenge is that we never know when that end is going to be, but if the families have had no preparation that this is likely to take place, it’s even harder. (N3) worst case scenario … would be [discussing end-of-life] right in the arrest situation … then you try to give parents the heads up about that, actually this is not really going to be a successful resuscitation, and to try to prepare them … in a very short space of time. Umm, depending on the parents that might be with them watching at the bedside. (D2)
It was felt that ACP discussions should ideally occur before admission to PICU, with clinicians who are familiar to the family. However, PICU staff can make useful contributions to these discussions by explaining the implications of a PICU admission and the potential burden of intensive therapies:
I think it’s the person who knows the family best. They are the people who should do that, whether it’s the community nurse, whether it’s their GP, or whether it’s their general paediatrician. Whoever knows them best and has the best relationship, is the person who should initiate that conversation. (N3) we get called in as intensive care doctors to help, er, the people who are managing the case long before a critical episode long before a critical episode to talk through what a resuscitation would involve and what the treatment we provide involves. And that, um, … parents will often agree in that situation that what we’re contemplating doing is abhorrent in some way; you know it’s just a step too far. (D4)
The use of a formal document in ACP was generally regarded positively by participants, with perceived benefits including the provision of a framework for discussions, empowering both healthcare professionals and parents to agree a care plan which reflects the family’s wishes:
I’m going to see somebody on the ward that’s collapsed and you’re considering whether they need ICU, you know, to look in their medical records, you see the [ACP], and you can quickly identify rather than going through tons of medical notes to find out what’s happening. (N5)
The value of ACP
Among medical staff, ACP was considered important to allow plans to be made in anticipation of different clinical scenarios. Nursing staff placed more emphasis on offering choice in terms of place of death, and the opportunity to carry out pre-bereavement work, as well as the introduction of other healthcare teams including hospice and community teams and the chaplaincy team when cultural and religious concerns were a priority:
Sometimes they have quite specific needs that they, or specific wants, they want to, and you can’t always facilitate them if you don’t … know in advance. (N5) if we want to get this child home, you know, we bring the community teams in, meet the teams. If you want to take your child afterwards to a hospice, let’s go … let’s go to the hospice, let’s go and see the bedroom, let’s go and … it’s just all about preparing them and getting the, to … just so that they’re not frightened by – you know, new faces or different people. (N6)
A strong theme for both medical and nursing participants was the need for ACP in order to make best interest decisions:
I have seen however many mothers here as well, who have never even held their baby, and the baby’s stuck here with their chest open for three weeks, and then we finally withdraw care and they still haven’t even held their baby. (D5) I don’t think the meaning of life sustaining treatment is always explained very well. How invasive it is and how uncomfortable, and how it takes you away from your normal environment, it takes you away from family interaction … lots of things we do carry significant risk of complications, and you should only really do them if, at the end of it, it is going to improve someone’s quality of life. (D8)
Participants were all able to recall instances where ACP discussions had resulted in achieving a peaceful terminal phase of illness and death in a preferred place of care. Positive feedback had been given by parents at subsequent bereavement meetings:
I do believe it’s helping. Well I know it is because I’ve seen parents coming back to us and talking about it, and saying how they feel it’s, it’s helped them. (N2) When he died I think it was all as sort of planned and predicted and … Yeah, the family were grateful, which is usually a good sign. (D3)
It was recognised, however, that acute clinical deteriorations often cause a crisis where even the most detailed ACP does not prevent a last-minute deviation from the plan:
if they make an ACP they may still change their mind right at the very end, um … But at least they will have had the opportunity to sit down and seriously think about what they want for their child. (N3)
Adverse consequences of inadequate ACP
Participants described situations where the admission of a critically unwell child with life-limiting illness to PICU had led to distressing consequences for the patient, their family and the staff involved in their care. It was felt that the expectations of both families and medical colleagues of what could be achieved through a PICU admission are on occasions poorly considered and can be unrealistic:
We definitely get exposed to when that whole process has gone wrong because children come here to die you know. Or come here with a life-threatening, you know, a development in their illness that could have been anticipated better and planned for in a different way. (D8) I know the challenge is that we never know when that end is going to be, but if the families have had no preparation that this is likely to take place, it’s even harder. (N3) So I think there are many examples in my head and in my career where we have over-medicalised the end-of-life and families have clung on to the medical management rather than the holistic palliative care management of children, such that they feel that they’re failing their child if they don’t ask for everything. (D1)
Participants described the moral and emotional distress associated with the provision of care and interventions that were not felt to be in the best interests of the patient or their family:
we get faced with decisions that are out of our control, someone else has decided actually, either between the family and the team, the medical team, the nursing team, they have decided that this child needs to come to ICU, and it is taken out of our hands. (D8)
The number of deaths in the PICU (the setting for this study) was 73 in 2010, equating to one or two deaths per week (the expected number for a PICU of this size when adjusted for the severity of illness
38
). The emotional impact of witnessing death so frequently on staff was described, but was more widely recognised and managed by nursing staff compared to their medical colleagues:
death is difficult and it is emotive and upsetting but at the same time, it is unavoidable, we have to deal with it. (D8) when I was a registrar it was easier for me because I had to just sit and have a debrief with my … consultant, as I love to cry. But now, I have to be this brave person and it’s very … very difficult. (D6) It’s not real life what’s going on in there, it’s just so horrendous what is happening every single day … so ‘No, you’re not doing it today. You’ve done it a couple of times recently and that is enough’. Because if you do it too often you have to leave. You have to protect yourself. (N2)
Emergent themes
In addition to the main themes described, an additional theme regarding transitions in care began to emerge during some of the later interviews. The challenges associated with managing CYP at ‘transition’ stages – babies moving from neonatal ICU to PICU, and those who make the transition to adult palliative care services – were described:
These teenagers that are the cross over … I don’t think paediatric and adults viewpoints on who they admit to ITU necessarily match at the moment. (N5)
Situations where the patient was a young person with capacity who wished to be involved in his or her own care planning, including difficult scenarios where the opinion of the CYP differed from that of his or her parents, were also described:
She herself had her own end-of-life care programme for her in another hospital. Unfortunately when she deteriorated, the parents diverted to us … we didn’t know about the end-of-life care plan. At the very best we knew from the way she looked that she had a life-limiting illness, but she was intubated. She woke up and she was extremely angry with the parents. Extremely angry. (D7)
Discussion
Summary of the main findings
This study provides an in-depth exploration of the experiences and perceptions of PICU staff regarding ACP for CYP with life-limiting illness and contributes to the growing evidence base in favour of timely ACP. ACP was identified as having multiple potential benefits including the provision of an opportunity to discuss with families their concerns and wishes for end-of-life care, before an acute deterioration in the patient’s clinical condition. It was perceived as a valuable process which supports decisions being made in partnership with patients and families, towards the delivery of continuous holistic care in a preferred place. ACP was felt to have contributed to ‘good’ deaths, with evidence for this existing in the form of positive feedback from parents at bereavement meetings following the child’s death. Conversely, deaths were described in which ACP had been lacking or inadequate, resulting in what was felt to have been substantial distress for the patient, the family and the staff involved. Similar themes have been reported in a recent study of the perspective of paediatric professionals from a range of specialties. 43
Benefits of the ACP process for healthcare professionals were also described, particularly around the ethical dilemmas that professionals experience around the delivery of invasive intensive life-sustaining therapies at the end of life. These dilemmas can cause moral distress, which arises when a sense of moral responsibility is not acted on due to internal (personal) constraints or external (contextual) barriers. 28
Strengths and limitations
This study used rich qualitative data to explore this increasingly important area of practice. Key strengths are the interdisciplinary nature and the rich data elicited from qualitative interviews with both medical and nursing staff. However, it was conducted within one PICU in England and included a relatively small number of participants. Ideally, further interviews across a number of PICU settings would be conducted to confirm data saturation, therefore caution is needed when extrapolating findings to other settings. PICU is an important setting from which to consider ACP for CYP with life-limiting illness; however, research with clinicians in other specialist and generalist settings, national and international, with varying years of experience would inform the process further. Investigation of the end-of-life decision-making process and evaluation of ACP processes and documents from the perspective of CYP and their families is also vital. Recent research suggests that family experiences vary greatly, but that decision-making in partnership with families is imperative.44,45
Implications for practice
The findings identified a need for specific training around palliative and end-of-life care and ACP. This includes training to develop the advanced communication skills associated with delivering this care. A work environment that allows time to have these conversations, while managing conflicting clinical demands, is also needed.
ACP was described as a dynamic, multi-disciplinary process that should be carried out by the healthcare professionals who know the patient and their family best, preferably before an acute deterioration in the patient’s clinical condition requiring resuscitation and intensive care. Understanding of this process and the importance of early identification and acknowledgement of the life-limiting nature of a condition requires promotion. It remains a common concept among healthcare professionals that ‘active’ treatment and ‘palliative’ treatment exist in two distinct mutually exclusive phases and that transition into the ‘palliative’ phase might deny patients life-sustaining ‘active’ treatment.46,47 However, earlier and more effective integration of palliative care can deliver better outcomes for patients and their families. 48 Formal ACP documents can provide structure to ACP discussions. 37 With ongoing advances in medical technology and life-sustaining therapies, more research, policy and guidance is necessary around the close relationship between ACP and discussions and decisions regarding withholding or withdrawing these therapies and interventions.
Death remains a taboo subject, preventing ACP conversations. 49 Additionally, death in childhood is against the cultural norm in developed countries. 5 Hence, ACP for CYP is a long way from being established as a concept in the public domain. 13 Furthermore, the effects of diversity, faith and multiculturalism have an impact on patient and family expectations and the ability to discuss death. 50 There is a need to increase awareness of life-limiting conditions and the implications for families within society as a whole in order that families who are faced with their child’s life-limiting illness come to expect an opportunity to participate in ACP as part of care.
Recommendations for further exploration in future studies include the challenges associated with ‘transition’ stages, situations where the patient is a young person with capacity who wishes to be involved in his or her own care planning, and the effects of diversity and multiculturalism around end-of-life care choices.
Conclusion
Delivering care in the best interests of CYP with life-limiting illness, and their families, is one of the most complex, emotive and ethically challenging scenarios for clinical medicine, and all the more so in the intensive care setting. The motivations for improvement are numerous, in particular to ensure the best possible care, with respect for autonomy and choice. Healthcare professionals have a responsibility to work in partnership with patients and families to ensure that preferences for care are recognised and prioritised. Improved training of healthcare professionals to enable earlier recognition of patients for whom ACP would be appropriate is necessary. Collaborative multi-disciplinary team-working between healthcare professionals across settings, and a formal ACP document, may facilitate the process. There is much to learn from work being carried out in paediatric settings, particularly around actions which have the potential to empower patients and families and contribute to societal understanding of the importance of ACP.
Footnotes
Acknowledgements
The authors would like to thank Dr Fiona Reynolds and Dr Adrian Plunkett, PICU Consultants, Birmingham Children’s Hospital, for assisting with study design. Dr Mitchell and Prof. Dale designed the study. Dr Mitchell was responsible for carrying out the interviews and analysing the data, with Prof. Dale for interpretation of the data. Dr Mitchell drafted the article. Prof. Dale revised it critically for important intellectual content. Both authors have approved this version for submission.
Declaration of conflicting interests
The authors have no competing interests to declare.
Funding
This study was carried out with the support of a Practitioner’s Allowance Grant from the Royal College of General Practitioners Clinical Innovation and Research Centre (SFB-2011–2024).
Licence for publication statement
The corresponding author (S.M.) has the right to grant on behalf of all authors and does grant on behalf of all authors, an exclusive licence (or non-exclusive for government employees) on a worldwide basis to permit this article (if accepted) to be published in Palliative Medicine and to exploit all subsidiary rights, as set out in our licence.