
Abstract
Background:
Significant gaps in the evidence base on costs in rural communities in Canada and elsewhere are reported in the literature, particularly regarding costs to families. However, it remains unclear whether the costs related to all resources used by palliative care patients in rural areas differ to those resources used in urban areas.
Aim:
The study aimed to compare both the costs that occurred over 6 months of participation in a palliative care program and the sharing of these costs in rural areas compared with those in urban areas.
Design:
Data were drawn from two prior studies performed in Canada, employing a longitudinal, prospective design with repeated measures.
Setting/participants:
The urban sample consisted of 125 patients and 127 informal caregivers. The rural sample consisted of 80 patients and 84 informal caregivers. Most patients in both samples had advanced cancer.
Results:
The mean total cost per patient was CAD26,652 in urban areas, while it was CAD31,018 in rural areas. The family assumed 20.8% and 21.9% of costs in the rural and urban areas, respectively. The rural families faced more costs related to prescription medication, out-of-pocket costs, and transportation while the urban families faced more costs related to formal home care.
Conclusion:
Despite the fact that rural and urban families assumed a similar portion of costs, the distribution of these costs was somewhat different. Future studies would be needed to gain a better understanding of the dynamics of costs incurred by families taking care of a loved one at the end of life and the determinants of these costs in urban versus rural areas.
Although most large urban centers have specialized palliative care delivered at home and in hospitals, such services are less developed in rural and semi-rural areas.
Significant gaps in the evidence base on costs in rural communities in Canada and elsewhere are reported in the literature, particularly regarding costs to families.
Because of limited access to health care services and other issues, end-of-life patients in rural areas may have different patterns of health care resource utilization than their urban counterparts, and rural families may experience different financial burdens.
It is unclear whether the costs incurred by rural palliative care patients and their family and the sharing of these costs differ from those observed in urban areas.
This study demonstrates that rural and urban families assume a similar portion of the overall costs, but the distribution of these costs is somewhat different.
Rural families face expenses particularly related to prescription medication, out-of-pocket costs, and transportation.
Urban families face expenses particularly related to private home care, followed by out-of-pocket costs, medical equipment/aids, and prescription medication.
Such knowledge may help to inform policy makers in the areas of development or improvement of financial policies and programs to prevent pauperization among vulnerable families as a result of insufficient health care resources for dying people.
Introduction
In Canada, each province and territory must ensure that their health insurance programs meet the federal standards set out in the Canada Health Act, which ensures universally accessible and publicly funded health care services. 1 Palliative care falls within the scope of such health care services. Although most large urban centers have specialized palliative care delivered at home and in hospitals, such services are less developed in rural areas, due notably to a smaller patient population.
Rural individuals usually do not want to leave their homes or community during their final days of life,2,3 nor do their families want them to be long distances away during this time. 3 However, rural patients are less likely to die out of hospital than urban patients,2,4 and among those who die in hospital, some die in hospitals situated outside of their region of residence. 5 There are several major impediments to supporting home deaths in rural areas. 6 The likelihood of receiving any palliative care at home is significantly lower for persons in rural areas than for those in urban areas. 7 Rural residents are much more likely to receive non-professional home care services such as supportive care and meal preparation 7 and tend to receive fewer home visits by family physicians during end of life than those living in an urban area. 8 Long travel distances9–14 and driving challenges9,13 also contribute to the complexities of home visits by professionals in rural areas. Significant gaps in the delivery of health services to end-of-life patients in rural communities in Canada and elsewhere are reported in the literature. These gaps include a shortage of health care professionals6,10,12–15 and limited access to 24-h/7-day health care services,2,12,16–19 equipment,10,12,14 medications,10,12,15,18 respite and other support services for family caregivers,17,20 and funding for services.2,15
Rural residents have significantly lower physician consultation rates in their last year of life than their urban counterparts 21 and are more likely to be hospitalized for conditions that could have been treated by primary care providers,22–24 which might reflect the more limited access to primary care in rural areas as compared with urban areas.25,26 Palliative care patients residing in a rural area, particularly women, those who are younger and those with a parent or a relative other than a spouse or child as their primary informal caregiver, are more likely to make emergency department visits to address their needs, and these visits often result in hospitalization.2,27 The lack of 24-h palliative care coverage in rural areas often leads to reliance on hospital emergency room services at night when care is urgently needed. 18
Although larger rural areas may have hospitals with basic services, people usually have to travel to urban areas for specialized care and treatments,12,28,29 which is sometimes perceived as a barrier to benefitting from these services. 30 Rates of palliative radiotherapy consultation and treatment seem to decline with increased travel time. 31 Hence, the greater distance from home to the hospital or specialized center may reduce the likelihood of admission to hospital.32–34 However, when patients are admitted, the probability of being discharged declines with increasing distance to the hospital.32,33 The need to travel may impose increased financial burdens on the patients and their families,28,29,35–37 including various traveling expenses28,35,36 and loss of or reduction in income.35,36,38
Because of limited access to health care services and other issues, end-of-life patients in rural areas may have different patterns of health care resource utilization, and their families may experience different financial burdens than their urban counterparts. However, it is unclear whether the costs incurred by rural palliative care patients and their families differ from those observed in urban areas, or whether there exist differences between these groups with regard to the sharing of these costs.
We carried out a study in urban regions of five Canadian provinces to evaluate all costs related to palliative care and how these costs were shared between the public health care system (PHCS), the family, and not-for-profit organizations (NFPO). 39 We replicated the same study concentrating on rural regions of four Canadian provinces. 40 This article compares the findings of the urban and rural studies in order to characterize cost differences in resources used by palliative care patients, the sharing of these costs, as well as the financial burden faced by families caring for palliative care patients. It should be noted that these studies were mainly descriptive and did not aim to investigate the determinants of costs.
Methods
Design, setting, and participants
The target population consisted of patients enrolled in a regional palliative care program and their main informal caregivers. Data on the urban sample were drawn from a study we performed in urban regions of five Canadian provinces, employing a longitudinal, prospective design with repeated measures. 39 Data on the rural sample were drawn from a replication of this study we conducted in rural regions of four Canadian provinces. 40 Rural areas were defined as geographic locations where access to secondary and tertiary health care services is complicated by distances from hospitals. 41 For the purpose of this article, we selected participants from the provinces common to the two studies: Nova Scotia, Quebec, and Manitoba. Details regarding the recruitment process are provided in Dumont et al. 39 and Dumont et al. 40 Both studies were approved by the Laval University Research Ethics Committee (Quebec) and by each participating site’s ethics boards.
Data collection
Data were collected in 2005–2006 for the urban regions and in 2009–2011 for the rural regions. Interviews were conducted every 2 weeks until either the patient’s death or upon patient and/or informal caregiver decision to end their follow-up. A 6-month follow-up was initially planned with participants, but upon completion of the 6-month period, patients/caregivers were invited to pursue their participation. The questions targeted the goods and services used related to the patient’s condition, and identification of who paid which costs.
Costing
The costing process of goods and services is described in Dumont et al. 40 At the time of the urban study, the Alberta values were retained as standard costs because of their availability and their completeness. In order to be consistent and to allow comparisons between the two studies, the Alberta values were also used in the rural study even though there were no rural study sites in Alberta. Cost values from 2010 were used in determining standard costs, except for personal expenses, which were provided by participants and adjusted according to the consumer price index for 2010. The urban study costs were re-estimated using the same values from 2010. (For more details on individual resources costing, see Appendix 1.)
Statistical analyses of costs
For patients with a follow-up longer than 6 months, data from the 6 months prior to death or to the end of their participation in the study were retained as the study was interested in costs occurring near death. The mean total cost per patient over the 6-month period was estimated using Lin et al.’s 42 non-parametric estimator method for each resource category and payer category. Statistical analyses were performed with SAS 9.2 (Cary, NC, USA) software. The bootstrapping technique was used to provide a 95% confidence interval of all the mean cost estimates. For more details on the statistical analyses, see Dumont et al. 40
Results
Study descriptive data and participant characteristics
The urban sample consisted of 125 patients and 127 informal caregivers. The rural sample consisted of 80 patients and 84 informal caregivers. Tables 1 and 2 compare the socio-demographic characteristics of rural and urban participants. Rural and urban patients differed significantly regarding their status on the Eastern Cooperative Oncology Group (ECOG) Performance Status scale 43 at the time of the first interview (p < 0.0001) and the total number of persons providing care and/or assistance to them (p = 0.0316). Rural and urban informal caregivers were significantly different regarding their gender (p = 0.0056) and age (p = 0.0244).
Socio-demographic characteristics of patients in rural and urban areas.
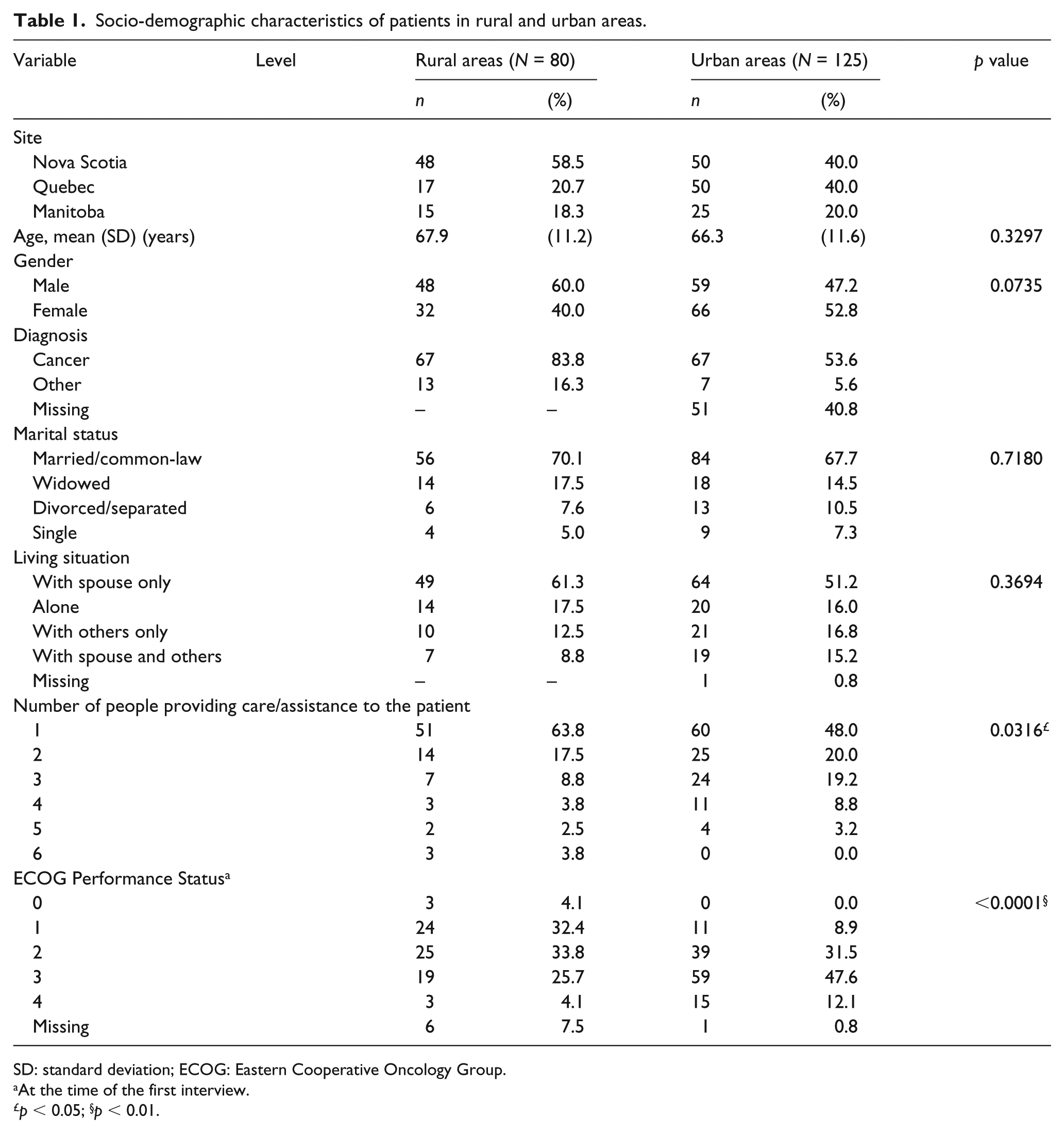
SD: standard deviation; ECOG: Eastern Cooperative Oncology Group.
At the time of the first interview.
p < 0.05; §p < 0.01.
Socio-demographic characteristics of informal caregivers in rural and urban areas.
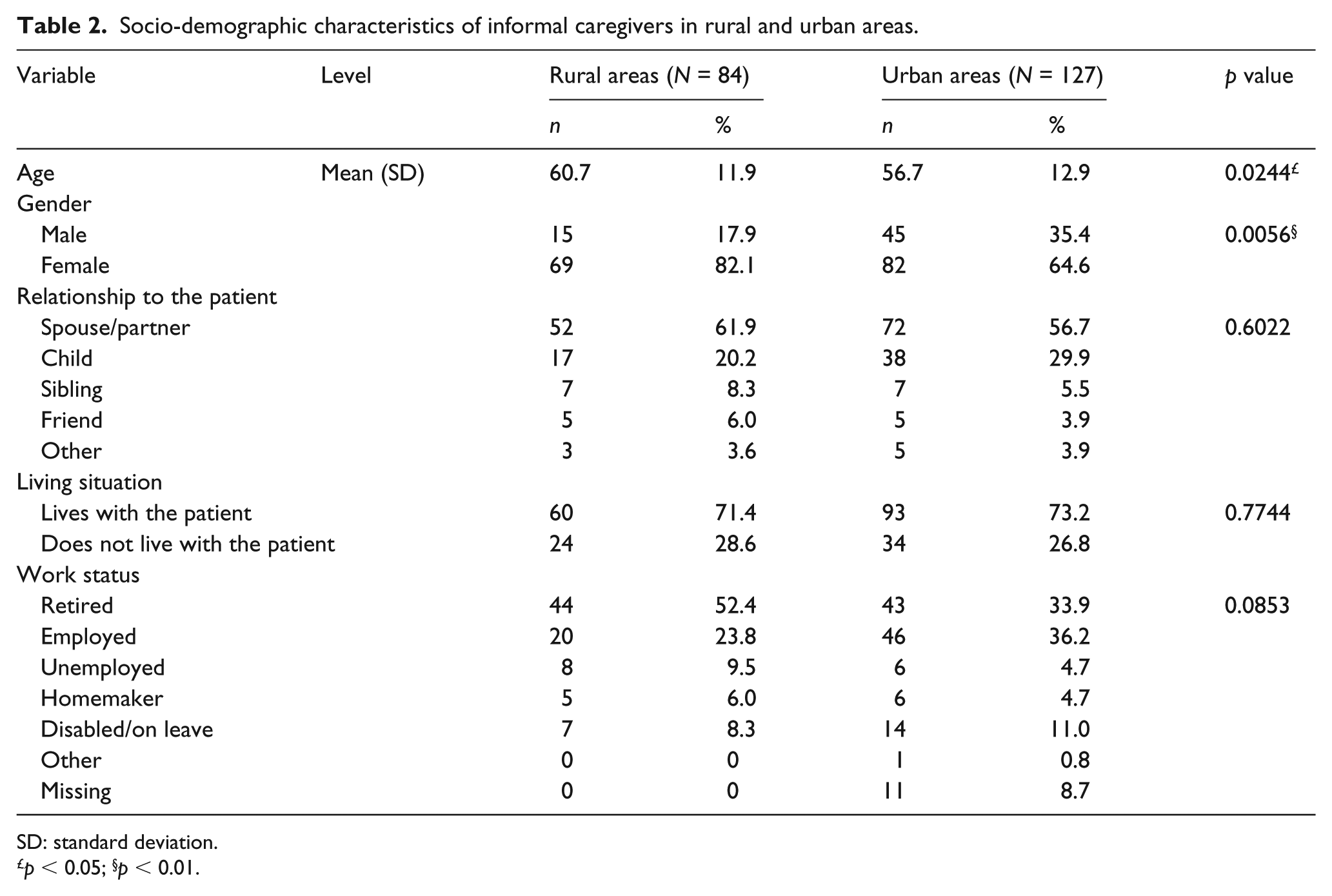
SD: standard deviation.
p < 0.05; §p < 0.01.
The data included for analyses covered a median length of 101.0 days (Q1: 51; Q3: 179) for the urban sample and a median length of 163.5 days (Q1: 64; Q3: 182) for the rural sample. About 88.8% of the urban patients and 55.0% of the rural patients died during their participation in the study.
Outcome data
The overall mean total cost per patient for a 6-month participation in a palliative care program reached CAD26.652 ± 1.704 in urban regions, as compared to CAD31,018 ± 1159 (16.4% higher) in rural regions. Tables 3 and 4 depict the distribution of these costs by resource and payer categories.
Mean total cost per patient incurred by each part for each resource category a in rural areas.
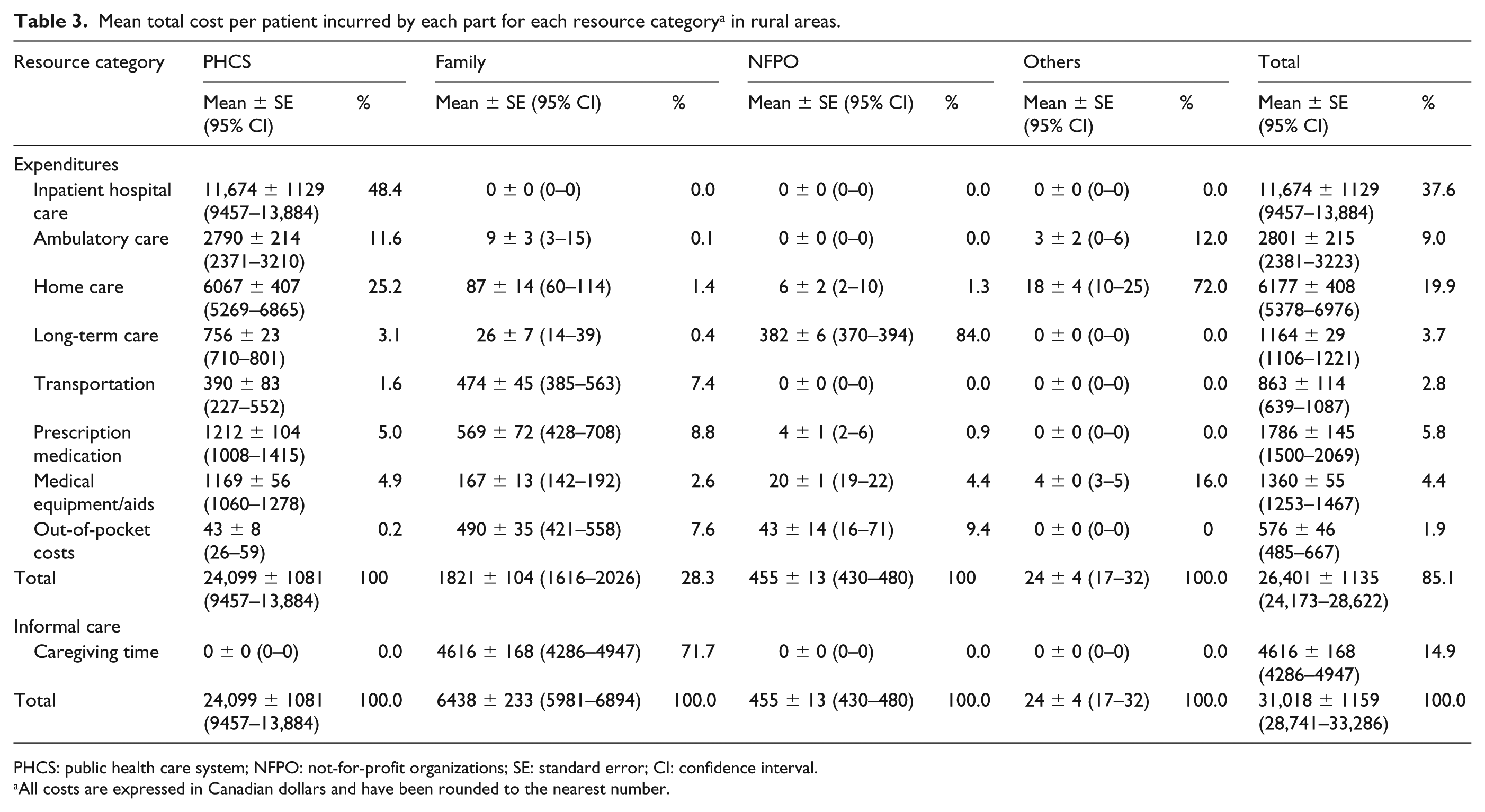
PHCS: public health care system; NFPO: not-for-profit organizations; SE: standard error; CI: confidence interval.
All costs are expressed in Canadian dollars and have been rounded to the nearest number.
Mean total cost per patient incurred by each part for each resource category a in urban areas.
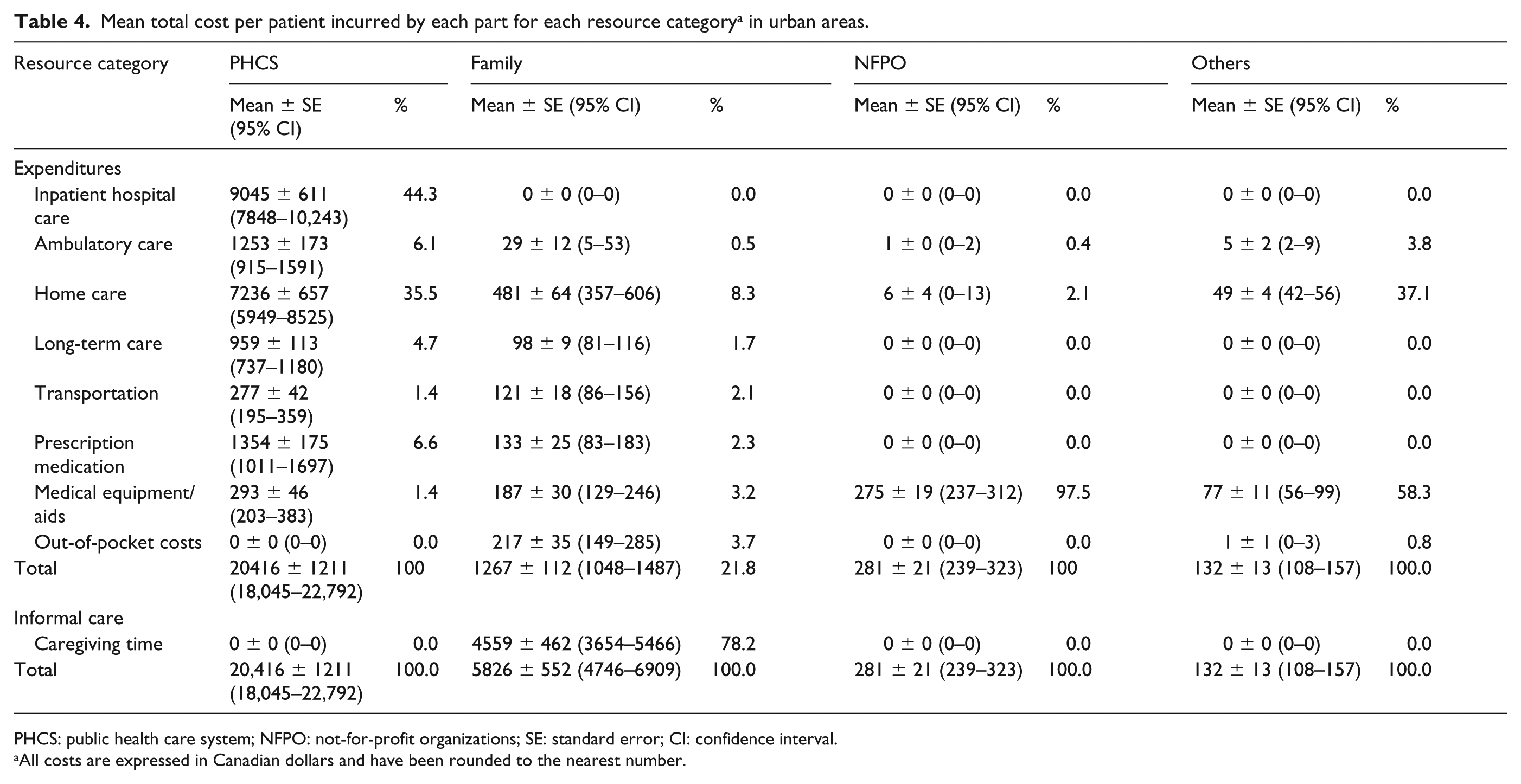
PHCS: public health care system; NFPO: not-for-profit organizations; SE: standard error; CI: confidence interval.
All costs are expressed in Canadian dollars and have been rounded to the nearest number.
The mean total cost per patient attributable to inpatient hospital care was 29.1% higher in rural regions than in urban regions. Over the course of the study, about 47% and 55% of patients were hospitalized in urban and rural areas, respectively. Urban patients had a total number of days spent in hospital averaging 8.40 (standard deviation (SD) = 0.53), while rural patients had a total number of days spent in hospital averaging 10.94 (SD = 1.03). Costs related to medical equipment and aids were 63.3% higher in rural regions. Those related to prescription medication were higher by 20.1% in rural regions. Home care costs were 25.8% higher in urban areas, while caregiving time costs in both rural and urban areas were similar.
Main results
The PHCS assumed 76.6% and 77.7% of the mean total cost per patient in the urban and rural areas, respectively. Most of the PHCS costs were attributable to inpatient hospital care. A greater portion of the PHCS costs was attributable to home care in urban areas as compared to rural areas (35.5% vs 25.2%), while a greater portion of PHCS costs was attributable to ambulatory care (mainly in emergency rooms) in rural areas as compared to urban areas (11.6% vs 6.1%).
The family paid 20.8% and 21.9% of costs in the rural and urban areas, respectively. The most important family cost component was caregiving time in both rural and urban areas. When excluding caregiving time costs, rural families faced expenses that were 43.7% higher than those of urban families. Most of the family expenses in the rural areas were attributable to prescription medication (31.2%), out-of-pocket costs (26.9%), and transportation (26.0%), while in the urban areas, family expenses were mostly attributable to private home care (38.0%), followed by out-of-pocket costs (17.1%), medical equipment/aids (14.8%), and prescription medication (10.5%).
Some informal caregivers absorbed indirect costs related to work absences. In urban and rural areas, respectively, the working informal caregivers missed an average of 32.35 (SD = 5.98) and 41.42 h (SD = 9.58) from work in order to carry out their caregiving responsibilities, which represents a difference of 21.9%. This difference was significant (p < 0.0001).
Discussion
The mean total cost per patient participating in a palliative care program over a 6-month period was 16.4% higher in rural areas as compared to urban areas, and the cost difference was greater for the PHCS than for the family. The portion of costs assumed by the PHCS and the family was similar among the urban and rural areas, but the distribution of these costs was somewhat different.
A greater percentage of the PHCS costs was attributable to inpatient hospital care in rural areas as compared to urban areas. This is consistent with the literature indicating that rural patients are more likely to be hospitalized at the end of life than their urban counterparts.5,44 Ambulatory care accounted for a greater portion of the PHCS costs in rural areas as compared to urban areas. This is consistent with findings of a Canadian study revealing that a greater proportion of rural residents report receiving care in emergency departments or outpatient clinics, which may reflect differences in the organization or the provision of health services, as well as disparities in the availability of health care resources as compared to urban areas. 45 Home care costs accounted for a lower portion of costs in the rural sample as compared to the urban sample. This is consistent with findings of a study by Goodridge et al. 7 revealing that patients living in rural/remote areas are less likely than those living in urban areas to receive any home palliative care. This difference may be attributable to more limited access to palliative care at home in rural areas as compared to urban areas. 7
Surprisingly, the costs related to informal caregiving time were similar between rural and urban areas. This differs from findings from prior studies indicating that rural residents are more likely to rely on informal supports, while those in more urban areas tend to have more supports available to them and/or use more formal support services.46,47 It is possible, however, that some potential confounding variables such as age and gender of the informal caregivers, as well as the number of informal caregivers, may have affected these results.
Rural families absorbed more indirect costs related to work absences. They also faced more costs related to prescription medication, transportation, and out-of-pocket expenses than urban families. The financial burden sustained by families that was associated with expenses otherwise covered in hospital is identified as a major barrier in maintaining palliative care patients at home within rural areas.2,20 As well, for some families, the costs and time commitments of commuting to urban areas for specialized palliative care can create an insurmountable barrier due to the financial burden alone. 48 Because of these issues, rural patients may not access all of their required end-of-life care services 36 and attain the level of care and services dispensed in urban areas. 49 Other studies have also identified financial constraints as factors that may interfere with seeking care 50 and affect treatment choices. 18 Older rural patients with advanced cancer perceive their lack of access to specialized care services as resulting in limited choices with regard to their location of care/death. 16 As well, although a home death is often the preferred option, when individuals live long distances from specialized health care providers 51 and when the additional supports necessary to enable death at home are unavailable, 18 an institutional death in hospital may be accepted and expected.
The publicly funded Canadian health care system ensures universal access to necessary medical and hospital care and the Canada Health Act identifies accessibility as one of its five fundamental principles. Therefore, financial means should not be a condition for accessing necessary medical and hospital care. 45 Patients, particularly the elderly, usually greatly value being able to access local care as much as possible.38,52 On the other hand, most patients accept that some degree of traveling is an inevitable part of rural life. 52 The feasibility of providing specialist care in rural communities is also questionable due to limited time and resources, as well as the challenges related to maintaining expertise where patient numbers are small. 53 Primary care professionals are seen as having a key role in delivering palliative care in rural areas, 54 as well as in supporting families providing care for rural palliative care patients. 19 The support from generalist care providers through after hours telephone support is an example of initiatives that have proven to be efficient and effective in avoiding hospitalization and emergency department visits. 55 Moreover, access to specialist multidisciplinary palliative care consultation by videoconferencing has the potential of reducing travel time and expenses for rural cancer patients and their families. 56
Given that rural areas have their own specific needs, caution is advised in applying urban models of palliative care to rural settings.3,14,45 Instead, palliative care approaches need to be tailored to individual rural communities by being responsive to their unique strengths and challenges.14,18
Limitations
Because of the descriptive nature of the study design and the use of a non-parametric estimator method to calculate mean costs, it was not possible to evaluate the effect of potential confounding variables that could explain some differences in the study results observed between the two groups. In particular, rural and urban patients differed significantly regarding their status on the ECOG Performance Status scale at the time of the first interview, and a greater number of urban patients had two or more informal caregivers. Rural caregivers were older than their urban counterparts, and more rural caregivers were female. Further studies are needed to explore the effect of such variables on costs occurred by urban and rural palliative care patients and their families.
Patients in the urban and rural studies were recruited in different settings, by different research assistants, which may have had an impact on the selection of participants. As well, urban patients tended to participate in the palliative care program for a shorter period of time than rural patients and were recruited closer to the time of their death. Lin et al.’s method made it possible to attenuate the effect of this discrepancy by giving more weight to data gathered near the end of the follow-up for patients who did not die during the study period and therefore that are closer to their subsequent time of death. However, the cost estimations obtained using such a method may be slightly different from reality.
Another limitation of this study includes the years separating the urban and rural studies. Shifts in policy or social programs and health care system coverage may have occurred over time. As well, even if the response rate in both areas (36% and 35%, urban and rural, respectively) appears relatively good for studies among palliative care patients, this low level of response rate constitutes a methodological limit. Moreover, the study did not take into account provincial or regional differences in policy or social programs, which may affect the generalizability of the findings. Only adult patients enrolled in palliative care programs, who are mainly cancer patients, were targeted. Finally, a study of actual costs may not reveal all needs, leading to an underestimation of costs.
Conclusion
Despite the fact that rural and urban families assumed a similar portion of the overall costs, the distribution of these costs was somewhat different. Rural families faced more costs related to prescription medication, out-of-pocket expenses, and transportation while urban families faced more costs related to formal home care. The amount of informal caregiving time was similar among rural and urban families. Future studies would be needed to gain a better understanding of the dynamics of costs incurred by families providing care for a loved one at the end of life, as well as the determinants of these costs in urban versus rural areas. Other studies might also explore unmet needs of rural palliative care patients and their informal caregivers in order to compare their situation to that experienced by their urban counterparts. These future studies could also examine the potentially differing needs of urban and rural palliative care patients. Further research might also investigate best-practice methods of hospice and palliative care service delivery (e.g. shared care) in rural areas.
Footnotes
Declaration of conflicting interests
The authors declare that they have no conflicts of interest.
Funding
Results presented in this article were drawn from two studies funded by the Canadian Institutes for Health Research (grant nos 123695, 178960).