
Abstract
Background:
There is a need to identify proactive, evidence-based interventions to support informal palliative caregivers. Mindfulness-based interventions, evidenced in the literature as providing physical and mental health benefits for diverse populations, may have application in the setting of palliative caregiving.
Aim:
To describe, evaluate and synthesise the peer-reviewed literature on the effects of mindfulness-based interventions for informal palliative caregivers.
Design:
A Systematic Literature Review according to the Preferred Reporting Items for Systematic Review and Meta Analyses guidelines and a Narrative synthesis.
Data sources:
The Cochrane Library, CINAHL, MEDLINE, PsycINFO and EMBASE databases, searched from inception to February 2014 and references of included studies.
Results:
A total of 13 articles, reporting 10 studies (n = 432 participants) were included. All studies were conducted in the last 5 years. Dementia caregivers were the most frequently researched population (n = 7). Results suggest that mindfulness-based interventions are feasible and acceptable to offer to informal palliative caregivers and may provide benefit, particularly in terms of reducing depression and caregiver burden and increasing quality of life. However, effects were not as robust as findings in the wider mindfulness intervention literature.
Conclusion:
This is the first systematic literature review on this topic. Results suggest both feasibility and potential benefit. Further qualitative research is required to explore the outcomes identified by informal caregivers themselves as the reduced magnitude of effect may suggest that we are not measuring the right outcomes in this context. This would inform more sensitive outcome measures for future intervention studies and guide the development and application of mindfulness-based models in this area.
Caring for a significant other with a palliative illness involves complex challenges that can negatively impact caregiver wellbeing.
There is a global concern to explore a broader range of caregiver support models, with a focus on proactive, preventative approaches.
Mindfulness-based interventions are evidenced as providing psychological and physical health benefits for diverse populations and may have application for informal palliative caregivers.
This is the first published systematic review of empirical research from around the world into the effects of mindfulness-based interventions for informal palliative caregivers.
We identified a small number of studies, with findings suggesting feasibility and potential benefit for reducing caregiver burden and depression and increasing quality of life.
However, effects were not as robust as identified in the wider mindfulness intervention literature, and the majority of studies focused on dementia caregiver populations.
Mindfulness-based interventions demonstrate some promise as a low-cost innovative approach to operationalise a fundamental principle of palliative care: holistic family caregiver support.
Further qualitative research and a focus on caregivers caring in the context of more rapidly progressing disease are warranted.
Introduction
Caring for a family member or friend with a palliative illness can be a positive and rewarding experience.1,2 However, caregivers also experience significant challenges as they take on the multifaceted, often unfamiliar roles to support complex care, in a setting marked by grief and uncertainty. The adverse effects on caregiver physical and psychological health, including increased rates of depression and anxiety, are well documented in the literature.3–6 These effects are reported to increase over the disease course, escalate as death approaches7,8 and can extend to bereavement.9,10 Caregiver strain has also been shown to adversely impact care recipient experience, as well as the sustainability of homecare. 11 Sustainable homecare, including the support of informal caregivers, is of increasing interest to governments around the world owing to the greater financial burden of in-patient palliative care on health expenditure. 12 With projected increases in people living longer with a greater level of disease burden, many of whom will require palliative and supportive care, informal caregiving in the home setting will gain increasing importance.
While there is a recognised imperative to provide informal caregivers with effective, evidence-based support,13–15 meeting this goal remains challenging. Rigorous caregiver intervention research to guide clinical practice is required,16–21 with emphasis on exploring a wider range of interventions to address diverse caregiver need, particularly within the psycho-social domains. 18 Proactive and preventative approaches, actively building on caregiver strengths and self-determination, are also advocated, rather than those that focus on treatment of informal caregivers in crisis. 22
Mindfulness-based interventions
Mindfulness-based interventions (MBIs) are empowering multicomponent interventions which aim to increase self-efficacy to respond to life stressors and may have application for informal palliative caregivers. Frequently delivered in a group setting, participants are taught, through meditation practice, how to cultivate attention on the ‘present moment’ rather than being swept away in past or future concerns. Participants learn to sit with and observe their changing field of thoughts, feelings and sensations without judging or seeking to alter the experience. 23 Mindfulness interventions are traditionally delivered over 6–8 sequential weeks lasting for 2.5 h. A silent retreat day is embedded in the later part of the programme. In addition, daily mindfulness practice (formal practice) is required, as well as informal practice, in which mindfulness is brought to daily life activities such as walking and communicating with others. Regular practice is considered important in order to cultivate skill and enhance benefit. There are now a diverse range of MBIs with varied protocols and adaptations for particular populations, for example, Mindfulness-Based Cognitive Therapy (MBCT) for depression and anxiety and Mindfulness-Based Cancer Recovery (MBCR) for cancer survivors. Underpinning intervention integrity is the requirement for skilled Mindfulness facilitators who have undergone extensive training and who have an established mindfulness practice themselves.
MBIs are evidenced as providing many physical and psychological health benefits for diverse clinical and non-clinical populations,24–27 particularly in terms of reducing perceived stress, depression and anxiety. There is emerging research of mindfulness-based programmes for informal caregivers in other contexts. Following an 8-week Mindfulness-Based Stress Reduction (MBSR) intervention, informal caregivers of children with chronic disease had an overall reduction in stress symptoms of 32% and 56% in total mood disturbance. 28 In another study, informal caregivers of adults with chronic conditions had significantly greater reductions in anxiety post-intervention, in depressive symptoms (post and at 3-month follow-up) and significantly greater self-efficacy scores at 3 months post-intervention, than the control group. 29
These findings suggest that MBIs may be of benefit to informal caregivers caring in the context of an incurable advancing disease; however, the increased complexity and narrow window of engagement in this setting warrant careful consideration. To our knowledge, there are no published systematic literature reviews exploring this topic; therefore, we sought to systematically investigate the empirical literature and provide a synthesised overview of the effects of MBIs for Informal Palliative Caregivers.
Methods
The study was conducted and is reported here, adhering to the Preferred Reporting Items for Systematic Review and Meta Analyses (PRISMA) guidelines. 30 A Participants, Interventions, Comparisons, Outcomes and Study design (PICOS) review protocol was formulated at study outset with the collaboration of all research members. As this was a systematic review study, ethics approval was not required.
Eligibility criteria
We included primary peer-reviewed studies and thesis, reporting empirical data, on the effects of MBIs for informal palliative caregivers. No restrictions on language, study design, outcome measurements, or comparators were applied. Articles that did not report outcome data, such as study protocols, and conference abstracts that did not progress to full papers were excluded on the grounds that full study details were not able to be evaluated.
Population
An informal palliative caregiver was defined as someone who provided for the physical, emotional or practical support needs of a person with an incurable, progressive illness, based on social connection or kinship. Stage of patient disease was not specified, and illness type was inclusive of both cancer and non-cancer. Studies of professional staff or volunteers employed or managed by an organisation were excluded.
Types of interventions
An MBI was defined as a multicomponent intervention that aimed to teach participants, through meditation practices, how to cultivate attention on the present moment and the changing field of thoughts, feelings and sensations, with qualities of openness and non-judgement. The intervention was required to be delivered in a number of sessions over time, led by a mindfulness facilitator. It could be delivered either in a group or individual setting. No stipulations were put around home mindfulness practice or a retreat day. Adapted mindfulness programmes were included if mindfulness remained the core driver of the intervention and the additional elements did not conflict with the principle tenets of mindfulness. Studies investigating mindfulness as a state or trait, in the absence of a mindfulness intervention, were excluded.
Information sources
The following bibliographic databases were searched from their inception to February 2014: Cochrane Library, CINAHL, MEDLINE, PsycINFO and EMBASE, without language restrictions or search limits. References of included studies and citing articles were also screened to identify additional studies.
Search strategy
A sample of Cochrane Systematic Reviews on palliative care were subject to detailed analysis in respect to search terms used and consultations with CARE SEARCH, a leading Australian palliative care knowledge network occurred. A comprehensive search strategy was then developed and tested in January 2014, prior to running the final strategy. A strategy was formulated for each database separately, using a combination of controlled vocabulary and key words. The search was conducted on 6 February 2014. See Appendix 1 for the MEDLINE strategy. The full search strategy is available from the author on request.
Study selection
Upon removal of duplicate records, one reviewer (author L.J.) screened the title and abstracts of identified papers against the inclusion criteria. A reliability check was undertaken by two additional reviewers (authors T.S. and H.B.) who independently screened these records, with differences resolved by papers going to full article review. Full text records were retrieved for more detailed analysis against the eligibility criteria. Authors of conference abstracts were contacted to determine whether they had published full articles pertaining to this work. References of included studies and citing articles were screened and author searches undertaken to identify additional studies.
Data abstraction and analysis
A standardised data abstraction form was used, and for each study, data were extracted for: author, year and country; study design; caregiver characteristics; outcomes; mindfulness type and intervention protocol, as well as class attendance and home practice rates. The classification of mindfulness type was supported by author M.S., an experienced MBSR teacher and practitioner. A narrative synthesis was conducted, as the small number of studies, diversity of intervention protocols and disparate measures precluded a meta-analysis.
To assess the quality of included studies, the randomised controlled trials (RCTs), the randomised trial and wait-list controlled studies (n = 6) were assessed using the Cochrane Risk of Bias Tool. 31
This is a domain-based evaluation of potential bias, advocated by the Cochrane Collaboration, in preference of scoring a quality weight, common in traditional scale-based approaches, which, they argue, have not been well supported by empirical evidence. 32 Following the Collaboration’s recommendations, each study was assessed for the potential risk of bias across six domains: selection bias, performance bias, detection bias, attrition bias, reporting bias and other potential biases using the prescribed criteria and guidance. On the basis of this assessment, an indication of low, high or unclear risk was ascribed.
The studies incorporating a qualitative method of inquiry were assessed using the Critical Appraisal Skills Programme (CASP) 33 for qualitative studies. This tool involves assessing the qualitative study using a series of questions that take into account the following: the presence of clear research aims and appropriateness of the chosen methodology; participant recruitment strategy and data collection methods to address these aims; consideration of the relationship between the researcher and study participants; evidence of compliance with ethical standards, rigour of data analysis, clear statement of findings and contribution to existing knowledge and understanding in the subject area. The remaining pre–post studies were not evaluated with a specific tool, as they are acknowledged as inherently having a greater risk of potential bias due to their study design and lack of control group. Study inclusion was not dependent on the assessed level of bias risk or quality, as an inclusive approach of gathering in all the intervention research undertaken in this emerging field of enquiry was considered important.
Results
The search strategy identified 156 references. Following the removal of duplicate records (n = 41), 115 references were screened against the inclusion criteria by title and abstract. 67 records were excluded in this process – (n = 54) because participants were not informal caregivers and (n = 13) because the study was neither an MBI nor involved informal caregivers. In a reliability check for the application of the inclusion criteria, the agreement rate was 86.48%, with differences resolved through consensus. A total of 48 full text records were retrieved for more detailed analysis of which n = 35 were then excluded. From the 156 records retrieved from the search strategy, 13 articles met the criteria for review inclusion. Three articles by Fegg and colleagues34–36 reported on different aspects of the same primary study and were treated as one study. Two articles by Whitebird et al. one reporting the primary study and one detailing successful strategies for study recruitment and retention, were also treated as one study. As a result, 13 articles, reporting 10 primary studies, were included in the review. Search results are summarised in the PRISMA flowchart (Figure 1).
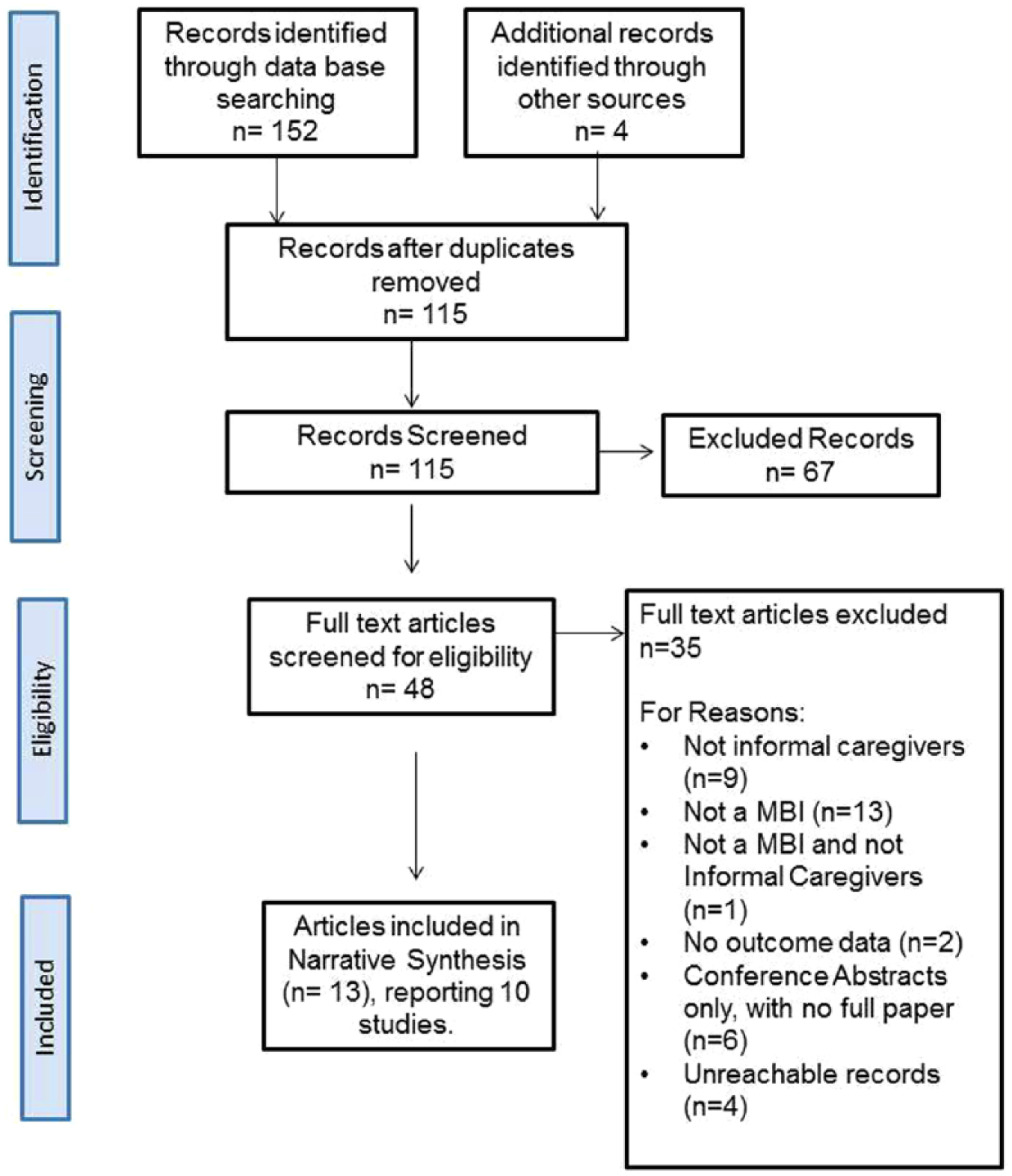
PRISMA flow diagram.
Study origins and designs
All studies (n = 10) were conducted in the last 5 years. Seven studies were conducted in the United States (n = 7) and one study each from Germany, Spain and Iran. There were a range of study designs, six of which used a control condition. A total of 28 different outcomes were measured, the most common being depression, anxiety, perceived stress, caregiver burden and mindfulness. Diverse measurement scales were used across studies, to assess these constructs. Seven studies employed follow-up measures, ranging from 1 to 6 months post-intervention. Only one study measured outcomes at a more distant time point of 1 year. Two of the 10 studies had a qualitative component.35,37 Study descriptions and findings are reported in Table 1.
Data extraction table for included studies.
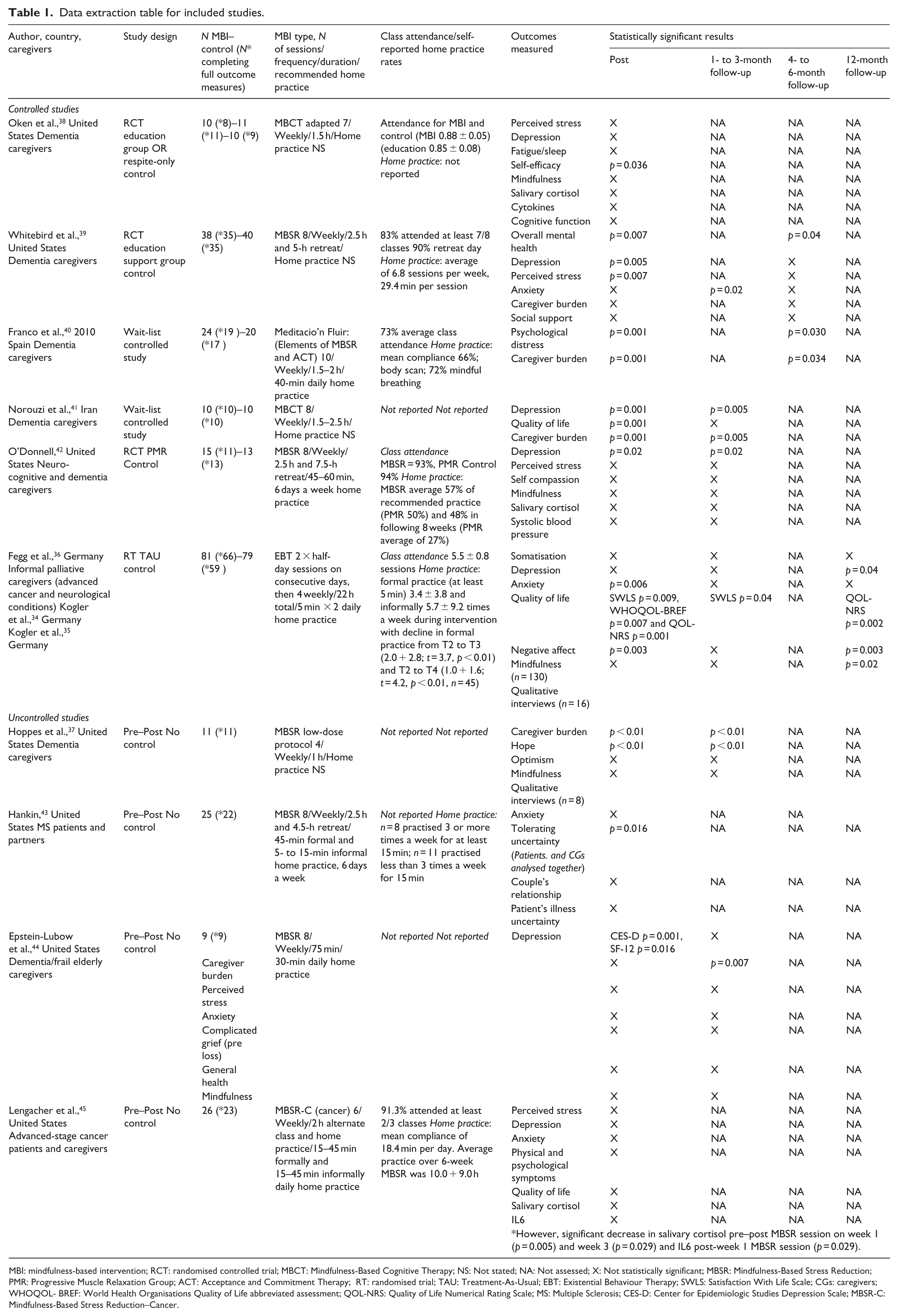
MBI: mindfulness-based intervention; RCT: randomised controlled trial; MBCT: Mindfulness-Based Cognitive Therapy; NS: Not stated; NA: Not assessed; X: Not statistically significant; MBSR: Mindfulness-Based Stress Reduction; PMR: Progressive Muscle Relaxation Group; ACT: Acceptance and Commitment Therapy; RT: randomised trial; TAU: Treatment-As-Usual; EBT: Existential Behaviour Therapy; SWLS: Satisfaction With Life Scale; CGs: caregivers; WHOQOL- BREF: World Health Organisations Quality of Life abbreviated assessment; QOL-NRS: Quality of Life Numerical Rating Scale; MS: Multiple Sclerosis; CES-D: Center for Epidemiologic Studies Depression Scale; MBSR-C: Mindfulness-Based Stress Reduction–Cancer.
Participants
Across the 10 studies, there were 432 caregiver participants. Dementia family caregivers were the most frequently researched population (n = 7/10 studies). Patient–carer dyads were included in two studies.43,45 Caregivers were predominantly female, White, caring for spouses or partners. Across studies, the age of participants ranged from 28 to 88 years. Length of time caregiving was under-reported across studies, with the exception of two studies39,42 who identified participants as being long-term caregivers (4+ years). Participant characteristics are summarised in Table 2.
Study participant characteristics.
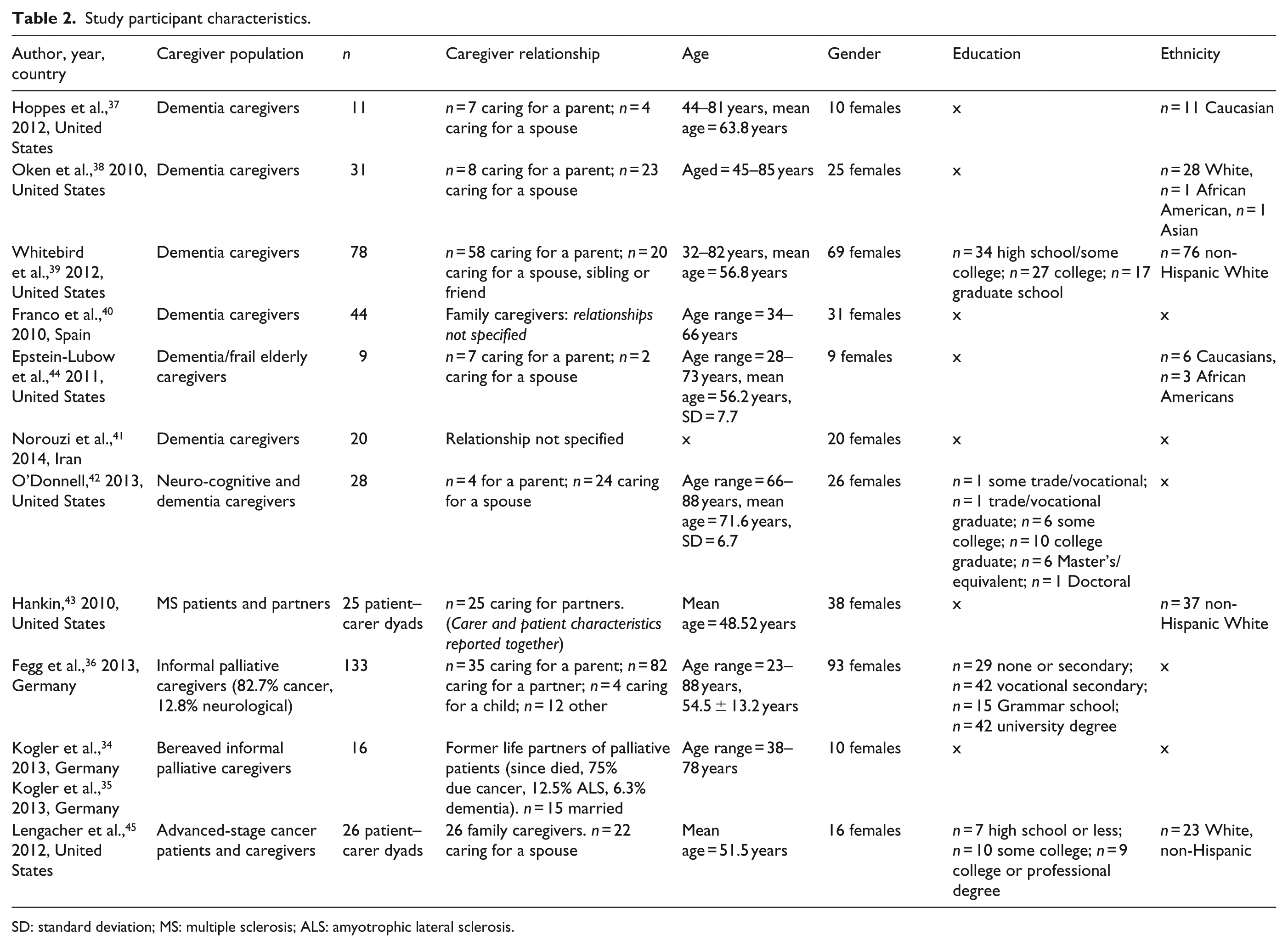
SD: standard deviation; MS: multiple sclerosis; ALS: amyotrophic lateral sclerosis.
MBIs delivered
The type of MBI delivered included MBSR (n = 6), MBCT (n = 2), an Acceptance and Commitment Therapy–based model (n = 1) and one Existential Behaviour Therapy (EBT) approach with mindfulness as its core driver. Nine of the 10 studies used a face-to-face group-based format. Mindfulness protocols varied from four to ten weekly sessions of variable length (1–2.5 h) and were marked by a range of daily home practice requirements (10–45 min). Three studies retained the ‘retreat day’, a key feature of the MBSR protocol,39,42,43 but duration varied (4–7.5 h). Five of the 10 studies reported the facilitator’s mindfulness qualifications and established self-practice, with varying degrees of clarity.
Class attendance, home practice and study retention rates
Six studies reported class attendance rates, ranging from 73% to 93%. Self-reported home practice rates varied across studies; however, in general, this was significantly less than the recommended amount with a further reduction in home practice at follow-up time points. Kogler et al.34,35 stated that there was a low compliance rate with the recommended amount of formal practice, but higher informal mindfulness practice. Retention rates of participants to full outcome measures appeared high across all studies ranging from 73.35% to 100%.
Quantitative outcomes
Depression
Five of seven studies found a significant effect for depression, including two RCTs and a randomised trial. Four studies found that this significant effect occurred post-intervention,39–42,44 with two studies also finding a significant effect at 1- to 3-month follow-up.41,42 One study found that a significant effect for depression emerged at 12-month follow-up. 36
Quality of life
Two out of three studies found a significant effect for quality of life post-intervention: Norouzi et al., 41 in a wait-list controlled study, and Fegg et al., 36 in a randomised trial. Fegg et al. 36 also found significant effects at 1- to 3-month and at 12-month follow-ups.
Caregiver burden
A significant reduction in caregiver burden was found in four out of five studies. Three studies identified this significant effect both post-intervention and at follow-up time points: Hoppes et al., 37 in a pre–post study, and Franco et al. 40 and Norouzi et al., 41 both wait-list controlled studies. The pre–post study by Epstein-Lubow et al. 44 found that a significant effect emerged at 4- to 6-month follow-up. In the study by Whitebird et al., 39 both the MBI and the education/support group control condition had a statistically significant effect on caregiver burden.
Anxiety and perceived stress
Two out of five studies found a significant effect for anxiety – one study, a randomised trial by Fegg et al., 36 at post-intervention compared to a treatment as usual control and in an RCT by Whitebird et al. 39 at 1- to 3-month follow-up compared to an education/support group control. One out of five studies found a significant effect for perceived stress at post-intervention, but not at 3- to 6-month follow-up. 39 In the RCT by Oken et al., 38 a statistically significant effect for perceived stress was identified in both the MBI and the education/support group control, but not the respite control. Similarly, in the RCT by O’Donnell, 42 a significant decrease in perceived stress was identified in both the MBI and Progressive Muscle Relaxation Control.
Mindfulness
One out of five studies measuring mindfulness identified a significant effect. In comparison with a treatment-as-usual (TAU) control, Fegg et al. 36 found that a significant effect emerged at 12 months post-intervention. O’Donnell 42 found that both the MBI and the Progressive Muscle Relaxation Control Group had a statistically significant increase in mindfulness at both post-intervention and at 2-month follow-up.
Other statistically significant results
Significant effects, both post-intervention and at follow-up, were also found for hope, overall mental health and psychological distress. A significant effect for self-efficacy post-intervention for dementia caregivers compared to control conditions of a respite and education/support group and ‘tolerating uncertainty’ in multiple sclerosis patients and caregivers analysed together were also identified. The remaining outcomes of interest yielded no significant effects (see Table 1 for results).
Qualitative results
Two studies incorporated a qualitative component of inquiry.35,37 Hoppes et al., 37 as part of their mixed-method, parallel design study, interviewed 8 of the 11 dementia caregivers who undertook an adapted low-dose MBSR protocol, at 1-month follow-up. Inquiring into the perceived effect of the intervention, four recurrent and related themes were identified: Increased acceptance of the care recipient’s illness, as well as enhanced acceptance/less judgement towards self and family; increased sense of presence; increased sense of peace and reduced stress; and decreased reactivity, particularly in terms of response to difficult care recipient behaviour.
Kogler et al.34,35 interviewed 16/81 former caregivers of palliative care in-patients who received the active intervention of EBT in a randomised trial (n = 130). Interviews were conducted 12 months after the last MBI; at this time, all participants were bereaved. Inquiring into the helpful aspects of the EBT intervention, two main categories of benefit were identified: social support and self-regulation. The theme of social support encompassed the benefits of interacting with others with shared experiences and included the subthemes of ‘self-disclosure’, ‘comparison to others’ and ‘setting of support’. The theme of self-regulation related to the strategies people used to deal with difficult experiences without becoming overwhelmed by them and included the subthemes of ‘mindfulness and acceptance’ which was defined as being aware of current experience with an attitude of acceptance, ‘focusing on the positive’ which included positive evaluation of dying, remembering pleasant experiences and searching for sources of strength and ‘orientation towards new goals’ which comprised conscious activities, living on one’s own and taking care of oneself.
Risk of bias and quality appraisal of included studies
Among the six studies assessed using the Cochrane risk of bias tool, 31 generally there appeared to be a low risk for attrition and reporting bias, with the greatest potential risk associated with a lack of blinding. Under-reporting of methodology resulted in the determination of unclear risk for many bias domains. Studies incorporating a qualitative method of inquiry35,37 were assessed for quality using the CASP checklist for qualitative studies. 33 Both studies had clearly articulated research aims, and the use of qualitative methodology was appropriate to address these. Both studies were judged to be ethically conducted, used appropriate recruitment strategies, methods of analysis and provided a clear statement of findings which help to advance understanding of the effects of mindfulness training for informal palliative caregivers. In terms of potential bias, however, Hoppes et al. 37 provided little description of the data collection process, and both studies fell short of demonstrating reflexivity.
Discussion
This is the first published systematic review, to our knowledge, of empirical research investigating the effects of MBIs for informal palliative caregivers. Our review found that in comparison to the Mindfulness research for patient populations, which extends over 40 years and increases exponentially each year, the evaluation of MBIs in the setting of informal palliative caregiving is a relatively new field of inquiry (n = 10). Drawing definitive conclusions from the studies reviewed is difficult. Effects were not always consistent across studies, which may reflect the diverse interventions, caregiver populations, study designs and use of disparate measures. Based on interview data, intervention attendance and study retention rates, MBIs appear feasible and acceptable to offer in the context of informal palliative caregiving. Findings also suggest that MBIs may offer benefit for informal caregivers across a range of outcomes, with results more consistent for reducing depression, caregiver burden and increasing quality of life. Qualitative results identified the perceived value of social support, self-regulation, increased acceptance of the illness, self and others, increased sense of presence, peace and reduced stress and reactivity. Studies reported no evidence of harmful effects. As identified in mindfulness studies in other contexts, there was a dilution of effect over time. 46 As most studies reported a decreased rate of practice over time, exploring ways to support ongoing mindfulness practice beyond the end of the intervention is one strategy and supported by the qualitative data.
MBIs
In terms of the MBIs, the majority of studies (9/10) utilised a face-to-face group delivery format; however, the range of interventions and protocols were quite diverse. There was no evidence to suggest that any one MBI was more effective. Emerging research outside the palliative care context is exploring how variance in mindfulness protocols, such as the number, frequency and duration of sessions, impacts intervention outcomes. Other delivery formats such as telehealth and online platforms 47 are also being evaluated with preliminary findings showing comparable benefit to traditional face-to-face group formats.48,49 This work will be of interest to researchers in the setting of informal palliative caregiving where participants are likely to experience challenges accessing MBIs due to scheduling difficulties, time constraints and not wanting to impact the care recipient by leaving them alone or in respite care. For rural caregivers, travel time and distance are also likely to inhibit access.
Caregiver populations
Seven of the 10 studies included in this review targeted dementia caregivers. More studies are required to explore the experience and effects of MBI for caregivers of patients with more rapid disease trajectories. Issues regarding format, timing, effective engagement, retention and perceived challenges in the setting of more rapidly progressing disease remain unclear.
An important consideration when targeting advanced disease caregivers is how to support participants at different junctures on the end of life caregiving and bereavement journey. Fegg et al. 36 found that a high percentage of their participants were in bereavement (54.9% at baseline and 69.9% at pre-treatment). This study reported that the mixed group composition of active and bereaved caregivers was viewed positively by participants, and while there are obvious complexities to address, the authors point out that it is often in the transition from end of life caregiving to bereavement that people require the most support. 36 This may point to the need to explore adapted mindfulness programmes tailored to address specific areas of need or challenge commonly faced by informal palliative caregivers, as has occurred for other clinical populations such as MBCT for anxiety and depression relapse.
The two studies incorporating patient–caregiver dyads43,45 reported the least significant effects, compared to the remaining eight caregiver only studies. This may indicate that caregivers require support independent from the care recipient or to talk more openly with others in a similar caregiving situation.
Measuring the right outcomes
While the findings of studies reviewed suggest benefit, the strength of the evidence is weaker than reported in the larger body of mindfulness intervention literature, where there is now robust evidence to support significant effects of MBIs for a variety of psychological and physical health domains. 24 The studies included in this review generally had small sample sizes and were likely underpowered. In addition, in the setting of caring for a significant other with a terminal illness, where stress, and frequently distress, increases over the disease course and escalates as death approaches, 7 there may not be the magnitude of symptom reduction identified in other settings and perhaps nor is it realistic. Alternatively, we may not yet understand the experience of learning Mindfulness while providing informal palliative care and as a result may not be measuring the right constructs. This highlights the role for qualitative research inquiries to more richly explore the perceived effects identified by informal palliative caregivers themselves, which may be missed if we presuppose particular outcomes. Only 2 out of 10 studies included in this systematic literature review incorporated a qualitative aspect of inquiry. A qualitative approach could inform theoretical model development, which is currently identified as a gap in the literature, and guide the selection of more sensitive or appropriate outcome measures. Malpass et al.’s 50 meta-ethnographic review of qualitative research on patient’s experience of mindfulness interventions indicates that people experience a perceptual shift in how they related to their illness and a transformation of their sense of self and personal agency. 50 This points to the need to more fully understand how caregivers experience mindfulness training and practice, in order to inform the design of appropriate studies to test MBI’s potential benefit.
Mechanisms of action
As with the wider mindfulness literature, understanding about the active components of the MBIs effecting change is still emerging. The significant effects identified for MBI groups, compared to treatment as usual or wait-list control groups suggest symptom improvement is unlikely to be due to the passage of time. Qualitative data identified that the group environment and peer learning and support are important mechanisms of change; however, the fact that MBI participants had statistically significant improvements in psychological symptoms compared to comparable control conditions matched for time spent with the facilitator, group setting and home practice suggests that other elements specific to the MBI are in play. Five studies assessed for increased mindfulness, using five different measurement scales, yet only one study found a significant increase in mindfulness. This may suggest that the mindfulness measures used were not sensitive enough to detect changes in this setting or alternatively other factors are moderating the effects of the MBI intervention. Understanding the active therapeutic components of these programmes is clearly a critical area for future study.
Study designs
Despite the well-documented challenges of conducting prospective intervention research in palliative care, all the studies included in this review adopted a prospective approach, seven of which undertook follow-up measurements beyond post-intervention. The range of study designs employed was encouraging and included six controlled studies. While the pre–post designs without control groups may have a heightened risk of bias, they have an important role to play in new fields of inquiry, in terms of working through logistics of engagement, implementation, and assessment with the view to inform larger, more rigorous clinical trials. 38
The generalisability of results of the studies reviewed is impacted by having small, convenience-based, homogeneous samples. Recruiting representative samples is a common methodological challenge in conducting both palliative caregiver intervention research 51 and mindfulness research and remains important to address. Future research would also be advised to report reasons for declined study participation to help inform better design, and the use of similar instruments across studies, to measure outcomes, would enable larger analysis and comparison. More explicit description of methodologies and interventions would also enable higher quality assessment. Facilitators’ holding a recognised qualification and an established mindfulness practice is considered fundamental to the integrity of MBSR and its derivative approaches, yet only 5 of the 10 studies reported this.
Strengths and limitations of this review
This study did not include grey literature and as such there may be publication bias against negative results. However, this review was conducted using a systematic methodology as advocated in the PRISMA guidelines. Three authors independently assessed the articles for inclusion using a pre-specified study protocol, anchored in a comprehensive and tested search strategy. This review was also inclusive of papers published in all languages, enabling a view into the world-wide literature.
Given the emergent nature of the research field, we chose to adopt an inclusive approach in which the findings of all studies meeting the review inclusion criteria were reported and discussed. We employed the risk of bias tool and the CASP checklist for qualitative studies to orientate readers to some key methodological considerations, rather than seek to exclude articles on the basis of quality metrics. Furthermore, this review is not making recommendations for clinical practice as the small number of studies with diverse measures and methodologies precludes definitive conclusions at this point in time. Therefore, in this instance, weighing study quality is less critical. The task, instead, becomes one of describing the findings, identifying the key learnings and the issues that require further attention.
Into the future, palliative care services throughout the world will be challenged to demonstrate an ability to more readily translate the central ethos of providing effective holistic family centred care, into practice. Exploring more innovative, proactive approaches that empower caregivers themselves to cultivate a sense of resilience and wellbeing as they take on the complex task of supporting a family member or friend at end of life is also recommended. This review has attempted to pull together the international learning around the effects of MBIs as a potential approach in this setting.
Conclusion
The aim of this review was to systematically identify, evaluate and synthesise the findings of empirical peer-reviewed studies exploring the effects of MBIs for informal palliative caregivers. We identified a small number of studies (n = 10) with results suggesting that mindfulness interventions are feasible and offer potential benefit to caregivers in this context. The empowering, participatory approach may offer caregivers a proactive way to manage the stress associated with providing care to a significant other during a terminal illness and in bereavement, reducing depression and caregiver burden, enhancing quality of life and a sense of self-efficacy. However, in terms of informing guidelines for clinical practice, there are many questions research has yet to answer. The needs and experiences of caregivers of people with more rapid disease trajectories is an important area for future research. Qualitative inquiry would also elucidate a wider range of potential effects, from the experience and perspective of the caregiver himself or herself. This would assist in defining the mechanisms of action and help to inform the selection of outcome measures for larger, more robust intervention studies.
Footnotes
Appendix 1
Medline search strategy February 2014.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.