
Abstract

Background
Several international health and cancer organizations, including the American Society of Clinical Oncology, have called for all patients with advanced cancer to have access to palliative care (PC) services. The challenges associated with providing these services are significant, and ideal approaches to implementation are unclear. 1 Typically, subspecialists practice independently from one another, isolated in separate clinics. For frail cancer patients, this approach is hindered by care coordination confusion, late referrals, and additional burdens of time and travel demonstrated by high no-show rates in PC clinics. 2 In contrast, joint management with a few providers in disease-specific clinics has been successful. 3
Methods
At the University of Wisconsin, we conducted a prospective, observational quality improvement study evaluating the feasibility of integrating a PC provider to co-manage patients together with oncologists across a diverse group of academic oncology clinics. Feasibility was defined as >64% of patients completing at least 50% of every 6-week clinic visits with a nurse practitioner. 4
All English-speaking oncology patients with pathologically confirmed, incurable lung, gastrointestinal, breast, and head and neck cancers were eligible for participation. Patients were usually identified via a morning discussion between the PC practitioner and the oncologist and nursing staff as they reviewed the list of the day’s patients. The mere presence of the nurse practitioner in clinic often prompted referral, although patients with high-symptom burden or significant psychosocial distress were commonly referred unprompted. The PC nurse practitioner also reviewed the upcoming days’ clinic list with the oncologists when possible to identify potential patients and provide informal consultation. The aim was for the PC clinician to meet with patients and families within 1 month of study enrollment and every other visit (approximately every 6 weeks for patients on chemotherapy). To improve the oncologists’ knowledge about the PC providers’ skills and the intervention, we adopted two important strategies. First, the PC provider typically saw patients before, after, or concurrently with the oncologists, utilizing existing staff and rooms. Some patients were also seen in the infusion center to maximize the efficiency of an individual patient’s day if delays were anticipated in the clinic. Second, the PC provider sat near the oncologists in the workroom to facilitate face-to-face communication.
Results
Seventy-three patients were enrolled in the program from March through May 2013. The patients were predominantly Caucasian (96%), typical for our population in Wisconsin. In all, 68% of patients were female and the median patient age was 58 years (range 32–90 years). Feasibility metrics were met: 86% of patients attended at least 50% of scheduled every 6-week visits and nearly half of patients attended at least 75% of scheduled visits. When patients had an appointment scheduled, only 4/799 (0.5%) patients missed their clinic visit with the nurse practitioner. Despite being near the end of life, median survival of 6.7 months (Figure 1), the patient’s quality of life (Functional Assessment of Chronic Illness Therapy–Palliative Care (FACIT-PAL)) and symptom burden (Edmonton Symptom Assessment System (ESAS)) were stable between baseline and 3 months with a non-significant decline at 6 months. Caregiver burden was also stable during the 6-month follow-up using Caregiver Reaction Assessment (Table 1). During the 6-month study period, 33% of patients died. In all, 23% (17/73) of patients were admitted to the hospital. Of interest, no patient on the study was admitted to an intensive care unit (ICU); 14% of patients received chemotherapy in the last 30 days of life.
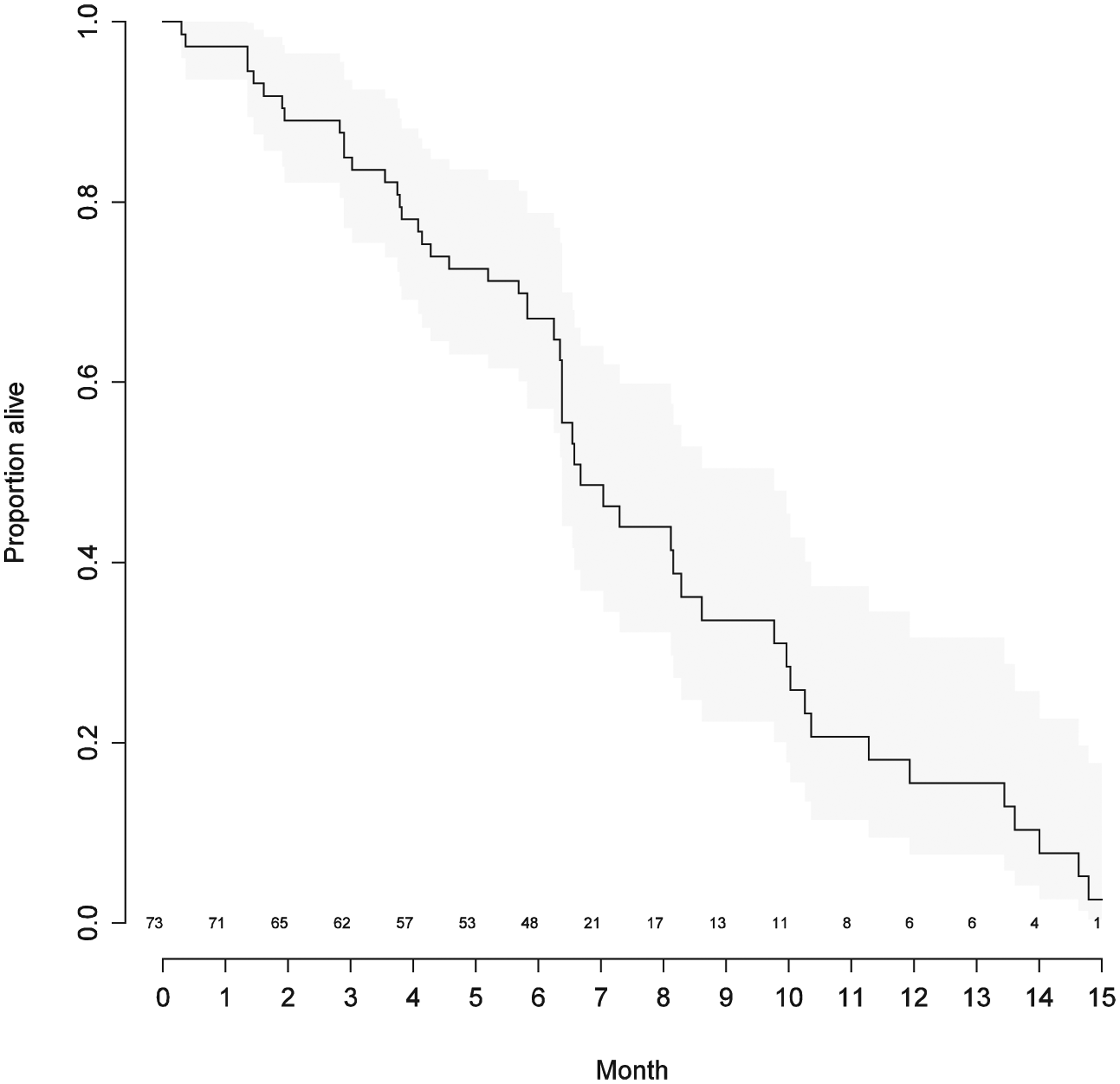
Kaplan–Meier curve (95% confidence interval) of overall survival for patients co-managed by oncology and palliative care.
Patient quality of life and symptom burden, caregiver distress.
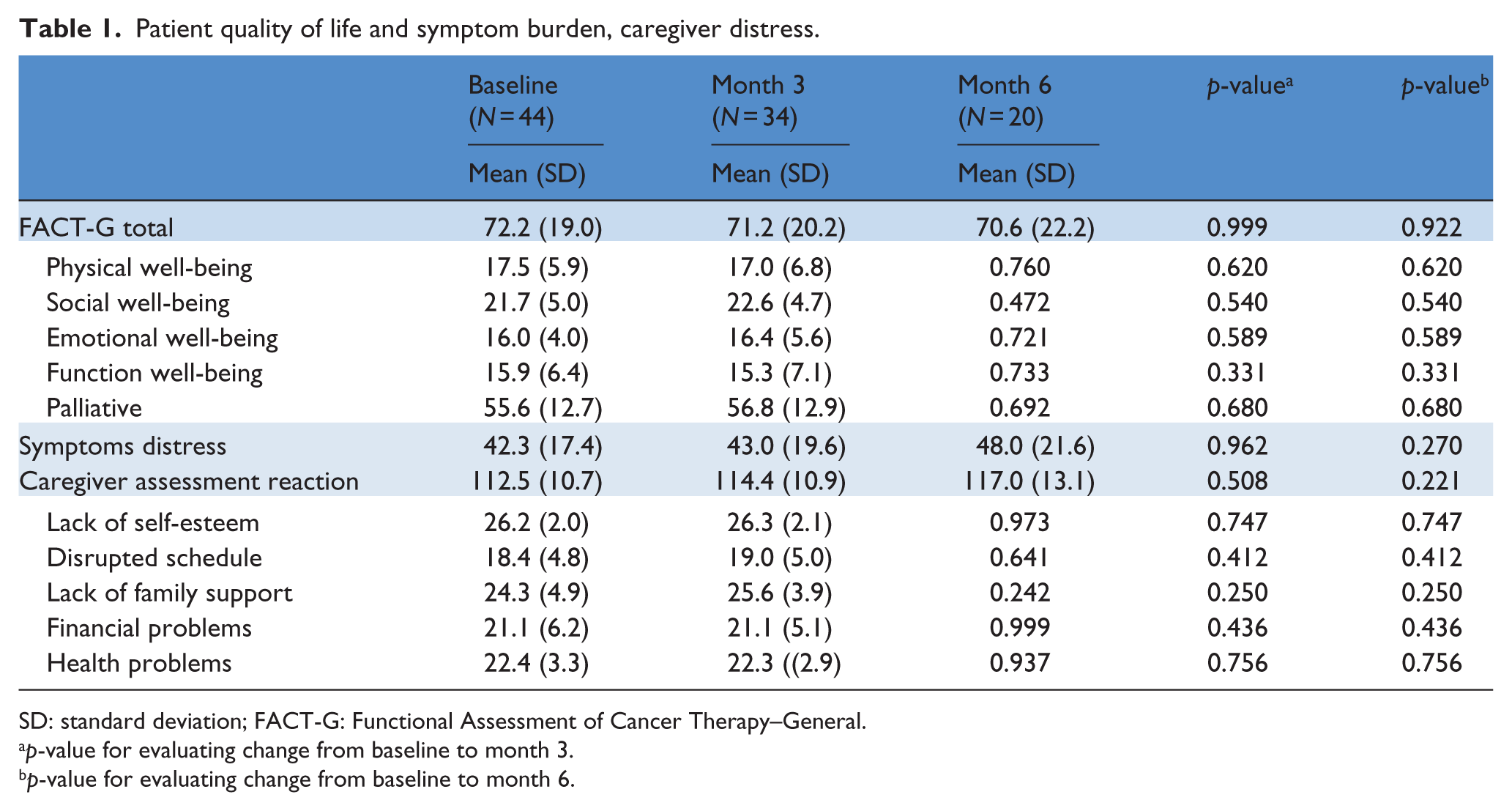
SD: standard deviation; FACT-G: Functional Assessment of Cancer Therapy–General.
p-value for evaluating change from baseline to month 3.
p-value for evaluating change from baseline to month 6.
Discussion
A model like ours of “embedding” the PC provider directly into the oncology clinic appears to facilitate the early adoption of PC by reducing barriers for both the referring oncologists and the patients. Our findings are consistent with the other inpatient concurrent care models showing improvement in health system outcomes and was well accepted by providers. 5 The ability for formal and informal face-to-face communication between providers in the workroom and in the patient room provided oncologists with direct knowledge of the practice style and value brought to bear by the PC provider seemed to diminish provider-side referral barriers. As these professional relationships developed, the oncologist’s comfort level with recommending and facilitating PC consultations was noticeably enhanced. While no formal satisfaction surveys were completed among referring oncologists, we received many comments of support regarding the intervention including one who commented, “[The PC provider] has been the best addition to my clinic. I’m not sure how I functioned without [her].” We also noticed an increasing shift of responsibility for certain tasks, such as symptom management and certain serious discussions, from the oncologist to the PC provider over time as trust increased. This quality improvement project highlights that high rates of patient engagement, with exceedingly low no-show rates, are possible even at the nascent beginning of an ambulatory PC clinic with careful coordination. The benefits seen in terms of enhanced communication included better prognostic awareness and alignment of goals of care with patient wishes, as demonstrated by low admission rates and no patients or families requesting critical care intervention.
Additionally, the nursing staffs, who practice in stable dyads with the oncologists, were vital advocates with their oncology partners and the patients. With time and acceptance, the PC provider was able to build a more structured schedule with patients to improve clinical efficiency, while maintaining capacity for same-day appointments. In summary, we believe that PC nurse practitioners can be integrated into an oncology practice to create a successful joint management model.
Footnotes
Acknowledgements
Kathy Van Veldhuisen NP for tireless effort in the care of her patients and in the development of the ambulatory palliative care (PC) clinic.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Dr Campbell is supported by the Cambia Foundation’s Sojourn’s Scholar Award. This project was supported by a grant from the University of Wisconsin Medical Foundation and Physicians Plus Insurance Corporation. This funding source had no role in the design and conduct of the study; collection, management, analysis, or interpretation of the data; and preparation, review, or approval of the manuscript for publication.