
Abstract
Background:
Early integration of palliative care into the management of patients with serious disease has the potential to both improve quality of life of patients and families and reduce healthcare costs. Despite these benefits, significant barriers exist in the United States to the early integration of palliative care in the disease trajectory of individuals with serious illness.
Aim:
To provide an overview of the barriers to more widespread palliative care integration in the United States.
Design and data sources:
A literature review using PubMed from 2005 to March 2015 augmented by primary data collected from 405 hospitals included in the Center to Advance Palliative Care’s National Palliative Care Registry for years 2012 and 2013. We use the World Health Organization’s Public Health Strategy for Palliative Care as a framework for analyzing barriers to palliative care integration.
Results:
We identified key barriers to palliative care integration across three World Health Organization domains: (1) education domain: lack of adequate education/training and perception of palliative care as end-of-life care; (2) implementation domain: inadequate size of palliative medicine–trained workforce, challenge of identifying patients appropriate for palliative care referral, and need for culture change across settings; (3) policy domain: fragmented healthcare system, need for greater funding for research, lack of adequate reimbursement for palliative care, and regulatory barriers.
Conclusion:
We describe the key policy and educational opportunities in the United States to address and potentially overcome the barriers to greater integration of palliative care into the healthcare of Americans with serious illness.
Early integration of palliative care into the management of patients with serious disease has the potential to both improve quality outcomes for patients and families and reduce healthcare costs.
Despite these benefits, significant barriers exist in the United States to the early integration of palliative care in the disease trajectory of individuals with serious illness.
A number of studies have identified and discussed specific barriers to palliative care integration, yet we lack an organized synthesis of the data on barriers to palliative care integration across domains.
Barriers in the education domain are lack of adequate education/training and perception of palliative care as end-of-life care.
Barriers in the implementation domain are the inadequate size of the palliative medicine–trained workforce, the challenge of identifying patients appropriate for palliative care referral, and the need for culture change across settings.
Barriers in the policy domain are the fragmented healthcare system in the United States, need for greater funding for research, lack of adequate reimbursement for palliative care, and regulatory barriers, particularly in the nursing home setting.
Using the World Health Organization’s Public Health Strategy for Palliative Care framework, the barriers we identified may be best addressed with a multipronged approach.
Expansion of the palliative medicine–trained workforce and greater investment in palliative care research are critical to building the evidence base for palliative care integration and securing funding for palliative care services.
Establishment of guidelines to “trigger” palliative care consultation may facilitate earlier integration of palliative care for individuals across multiple settings and in varying disease populations.
Introduction
During the last decade, palliative care has been one of the fastest growing trends in US healthcare. The number of palliative care teams within US hospitals with 50 or more beds has nearly tripled since the year 2000 to more than 1700 programs serving approximately 6 million Americans in 2012. 1 This growth has occurred primarily in response to the increasing number of Americans living with serious and chronic illnesses and to the caregiving realities faced by their families. Approximately 90 million Americans are living with serious illness, and this number is expected to more than double over the next 25 years. 2 About 20% of all Medicare beneficiaries have five or more chronic conditions, and two-thirds of Medicare spending goes to cover their care. 3 This patient population is also the most likely to benefit from palliative care.
The dominant three palliative care delivery models in the United States are hospital palliative care, community palliative care, and hospice. Hospital palliative care teams either provide consultation to the attending physician or assume primary oversight of care, depending on the preferences of the referring physician. Consultations occur in the inpatient setting, the intensive care unit (ICU), and emergency department (ED). Community palliative care includes a range of delivery models designed to meet the needs of seriously ill individuals and their families, outside the inpatient or hospital setting. Palliative care may be provided in the patient’s home, a nursing home, an assisted living facility, or an outpatient clinic such as a physician’s office, dialysis unit, or cancer center. These care models are developing rapidly in an effort to meet the needs of the sickest and costliest patients—who may otherwise resort to 911 calls, ED visits, and hospitalizations for problems that could have been addressed safely and effectively in the community. Hospice care is a well-known and comprehensive delivery model of palliative care, but in the United States, it is limited to terminally ill patients who agree to give up insurance coverage for disease treatment. The Medicare hospice benefit (and those of other payer’s) defines hospice eligibility as appropriate for patients when two doctors certify a prognosis of 6 months to live if the disease follows its usual course, and the patient (or surrogate) agrees to forgo insurance coverage for disease treatment of the terminal illness.
The World Health Organization (WHO) considers palliative care to be “an approach that improves the quality of life of patients and their families through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial and spiritual.”4 –6 Early integration of palliative care into the overall management of patients with serious disease has the potential to improve quality outcomes for patients and families and to reduce healthcare costs.7 –19
Despite these substantial benefits, there are significant barriers in the United States to the early integration of palliative care in the disease trajectory of individuals with serious illness. Our objective is to provide an overview of the barriers to more widespread palliative care integration in the United States. We achieve this objective through a review of existing literature in combination with primary survey data from the Center to Advance Palliative Care (CAPC). We then outline the key opportunities on the US policy agenda for addressing these barriers to greater palliative care integration in the United States.
Methodology
Framework: WHO’s public health model
Our analysis uses the WHO’s Public Health Strategy for Palliative Care 4 to frame our discussion of barriers to palliative care in the United States. The public health model postulates that in order to effectively integrate palliative care into a society, and change the experience of patients and families, the following components must be addressed: (1) education of healthcare workers and the public, (2) implementation of palliative care services at all levels throughout society, (3) appropriate policies, and (4) adequate drug availability. Our analysis will focus on policy, education, and implementation because drug availability is not a significant barrier in the United States to palliative care growth.
Working definitions
We used the following definitions in our discussion of barriers to palliative care in the United States:
Integrated palliative care. Integrated palliative care involves bringing together administrative, organizational, clinical, and service aspects in order to realize continuity of care between all actors involved in the care network of patients receiving palliative care. It aims to achieve quality of life and a well-supported dying process for the patient and the family in collaboration with all the care givers (paid and unpaid). 20
Barriers to integrative palliative care. Those that avoid bringing together administrative, organizational, clinical, and service aspects in order to realize continuity of care between all actors involved in the care network of patients receiving palliative care. 20
Data sources
Our analysis comprised both a review of existing literature, national/government reports, and survey data collected by CAPC. Details regarding these sources are as follows.
Literature search
We conducted a literature search of PubMed in March 2015. Our search terms included “barriers” and “palliative care,” and we included the literature published between 2005 and March 2015. We identified a total of 143 publications, and two authors screened the titles and abstracts for applicability. The following publications were excluded: 85 that were internationally based, 20 that were focused on the clinical treatment of patients, 11 that were tangential to the topic of barriers to integrated palliative care, 9 that were focused on the pediatric population, and 6 that were opinion pieces. We included an additional four articles and two books identified from the reference lists of included articles (Figure 1). We categorized the literature as either original research, review article, report, or book and indicated the population/setting in which the research was conducted and the type of barrier addressed by the document using the previously mentioned WHO public health model (Table 1).
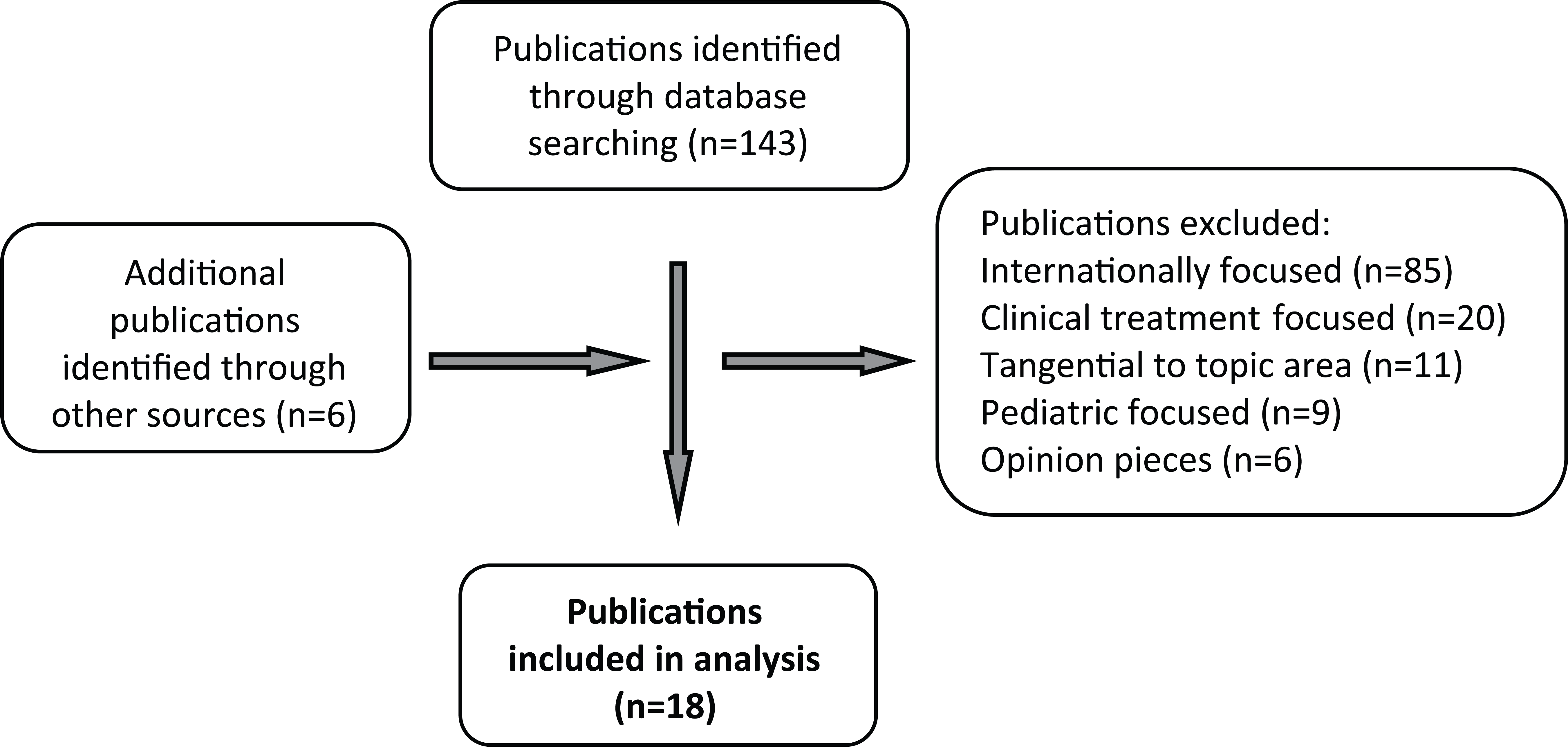
Flowchart of included and excluded publications.
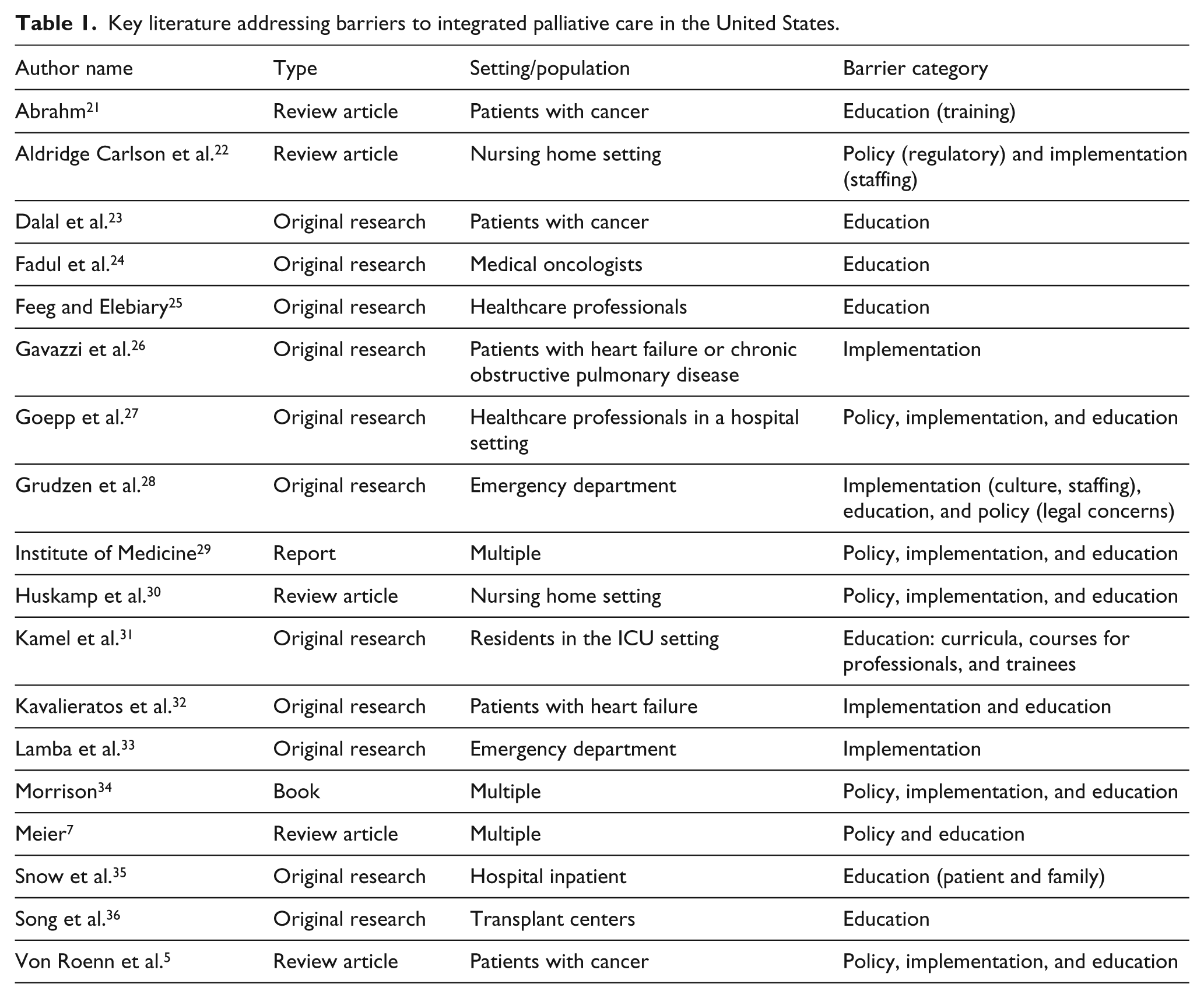
Key literature addressing barriers to integrated palliative care in the United States.
CAPC Registry data
We used primary data collected by the CAPC’s National Palliative Care Registry to exemplify the barriers identified in the literature review. The National Palliative Care Registry collects operational data on palliative care programs to promote standardization and improve the quality of palliative care in the United States and is the only data repository of its kind. The registry has been collecting information and reporting back to hospital-based palliative care programs since 2008, and during the past 6 years more than 1000 programs have participated. To be eligible to submit program data to the registry, hospital-based palliative care programs must meet the following eligibility criteria:
The palliative care program is part of a formally organized and legally constituted entity that primarily provides healthcare services, or a sub-unit of a legally constituted entity that may be, but need not be, health related.
The palliative care program has been providing palliative care services for at least 1 month.
The palliative care program provides care to patients at one or more locations within the broad continuum of care settings (e.g. hospital, home, office, long-term care, hospice, and nursing home).
The palliative care program representative(s) act in good faith in providing complete and accurate information reported on the survey.
This report uses registry data from 2012 to 2013 for 405 hospital-based palliative care programs throughout the United States. Specifically, we report responses from the following survey question: “What resource(s) would be most helpful to you in growing your palliative care program (consult and/or inpatient palliative care unit)?”
Results: barriers to palliative care integration in the United States
Our literature review resulted in 18 key papers which are summarized in Table 1. The barriers we identified from these papers are described in the following sections and are summarized by the WHO domains below:
Education-related barriers: Lack of adequate education and training for medical residents. Perception of palliative care as end-of-life care by healthcare providers and the public.
Implementation-related barriers: Inadequate size of palliative medicine–trained workforce. Challenge of identifying patients appropriate for palliative care referral. Need for culture change regarding palliative care across settings.
Policy-related barriers: Fragmented structure of the US healthcare system. Need for greater funding for palliative care research. Lack of adequate reimbursement and incentives for palliative care for complex patients. Regulatory barriers to greater palliative care integration in the nursing home setting.
Education-related barriers to palliative care in the United States
The WHO public health model identifies the domain of education-related barriers as curricula, courses for professionals and trainees, expert training, family caregiver training and support, and media and public advocacy. Our literature review identified numerous examples of lack of education and training being a primary barrier to greater palliative care integration in the United States. While palliative care is becoming more important in today’s health system, addressing health professionals’ lack of knowledge is crucial to more widespread integration.
Lack of adequate education and training for medical residents
A number of studies sought to identify the extent of palliative care knowledge of current US medical students or residents across numerous settings. The fairly consistent conclusion was that students in US medical schools had very little to no training in palliative care and did not feel confident to handle situations that required palliative care consultation.
For example, one study 31 evaluated residents in the ICU setting and surveyed them to assess their knowledge, skills, and perceived barriers toward palliative care in the ICU. This study found that the most common barrier identified by residents (19%) was discrepancies in goals of care between the medical team and patients/families. In addition, residents reported that a palliative care consult was most commonly obtained when the patient was terminally ill (23%) as opposed to further upstream in the course of illness. The authors suggest that resident teaching should focus on overcoming communication barriers with patients and their families and identifying the best method to teach palliative care in the ICU setting.
Similarly, a paper regarding the integration of palliative care into comprehensive cancer care recommended greater training of fellows and practicing oncologists in palliative care skills, including communication, and methods of preventing and treating compassion fatigue. 21 A qualitative study regarding provider perceptions of barriers to integrated palliative care similarly found that there was a need for organized educational services that crossed disciplinary lines. 27
Perception of palliative care as end-of-life care by healthcare providers and the public
A number of studies in our review discussed the perception of palliative care in the United States as equivalent to end-of-life care as a major barrier to greater upstream integration of palliative care in patients’ disease course. We considered this as an education-related barrier because it can be overcome with knowledge and understanding of palliative care both through clinical and professional training as well as through public health education. A recent review
5
concluded that the most significant barrier to the integration of palliative care at all stages in the treatment of patients with cancer is the largely clinician perception that it is end-of-life care. The authors noted that
an assessment of perceptions and experiences of palliative care providers indicated that some health care professionals viewed palliative care as being primarily focused on symptom control for terminal patients and that these professionals saw palliative care as a consideration only after all disease-modifying treatment had ceased.
5
They found that these misperceptions were also identified in multiple other studies.
One series of studies hypothesized that the perceived association between the names “palliative care” and “hospice” was a barrier to early patient referral. The studies aimed to determine whether a service name change from “palliative care” to “supportive care” was associated with earlier referrals of patients to palliative care services. In the first study, 24 the authors found that the name “palliative care” was perceived by 140 medical oncologists and mid-level providers as more distressing and reducing hope to patients and families compared with the term “supportive care.” Medical oncologists and mid-level providers significantly preferred the name “supportive care” and stated that they would be more likely to refer patients on active primary and advanced cancer treatments to a service named “supportive care.”
In actual clinical practice, the second study 23 found that the name change from “palliative care” to “supportive care” impacted referral rates. In this study, the authors examined the records of 4701 consecutive patients with a first palliative care consultation before and after a name change from “palliative care” to “supportive care” to determine the rate and timing of palliative care referral. They found that after the name change, there were a 41% greater number of palliative care consultations mainly as a result of a rise in inpatient referrals. In the outpatient setting, they found a shorter duration from hospital registration to palliative care consultation and from advanced cancer diagnosis to palliative care consultation occurred. These results suggest that the perception of palliative care as end-of-life care is a barrier to palliative care integration. Although some debate exists regarding the equivalence of the terms, “palliative care” and “supportive care,” 37 both supportive care in cancer and palliative care have their own origins, history, and background and may be primary, secondary, or tertiary. 38 In current practice, both approaches share mutual interests that have the potential to stimulate earlier integration in the disease process.
A number of studies surveyed physicians in various settings regarding barriers to palliative care integration finding that the perception of palliative care as end-of-life care was a significant barrier. For example, a survey of 155 physicians caring for patients with lung cancer found that 48% of physicians referred fewer than 25% of their patients for palliative care consultation. A major reason for this low referral rate was concern that a palliative care referral would alarm patients and families.5,39 Similar concerns regarding the expectations of patients and families were voiced in two other studies. In one study, a survey of 74 physicians found that the most commonly endorsed barrier to palliative care referral in the hospital setting was the patient and/or family’s perceived unrealistic expectations regarding disease prognosis. 35 In another study summarizing barriers to palliative care in the ICU, inflated expectations regarding critical care therapies and preoccupation with an unattainable level of prognostic certainly are two important barriers to earlier palliative care intervention. 40 A study of 74 clinicians across 27 lung transplant centers found that the misconception of palliative care as end-of-life care was a major reported barrier, along with uncertainty about patient prognosis and perception that palliative care precludes more aggressive treatment. 36 Similarly, survey respondents attending a national palliative care conference rated the top three barriers to greater use of palliative care and hospice as (1) physician’s reluctance to make referrals, (2) physician’s lack of familiarity with availability and suitability of hospice, and (3) association of hospice with death. 25
These studies illustrate that the misperception of palliative care as end-of-life care and as not compatible with ongoing treatment is a significant barrier to palliative care integration in the United States. To address this barrier, better education about palliative care, for both healthcare providers and the public, could potentially result in greater use and earlier integration of palliative care services for patients with serious illness. These opportunities and initiatives are discussed in the “Options to expand integrated palliative care in the United States” section.
Implementation barriers to palliative care in the United States
The WHO public health model identifies the domain of implementation-related barriers as those related to opinion leaders, trained manpower, strategic and business plans (including resources and infrastructure), and the existence of standards and guideline measures. 4 Our literature review identified a number of significant implementation barriers to greater integration of palliative care in the United States.
Inadequate size of the palliative medicine–trained workforce
A major barrier facing the expansion of palliative care services in the United States is the lack of palliative medicine–trained physicians, nurses, social workers, and other disciplines. Where there is approximately one cardiologist for every 71 persons experiencing a heart attack and one oncologist for every 141 newly diagnosed cancer patients, there is only one palliative medicine physician for every 1200 persons living with a serious or life-threatening illness. 41 A recent analysis by the American Academy of Hospice and Palliative Medicine’s Workforce Task Force estimated that the gap between the current supply and the hypothetical demand for hospice and palliative medicine–trained physicians to reach mature staffing levels was 2787–7510 full-time equivalents, which equates to 6000–18,000 individual physicians, depending on what proportion of time each physician devotes to hospice and palliative medicine practice. 42
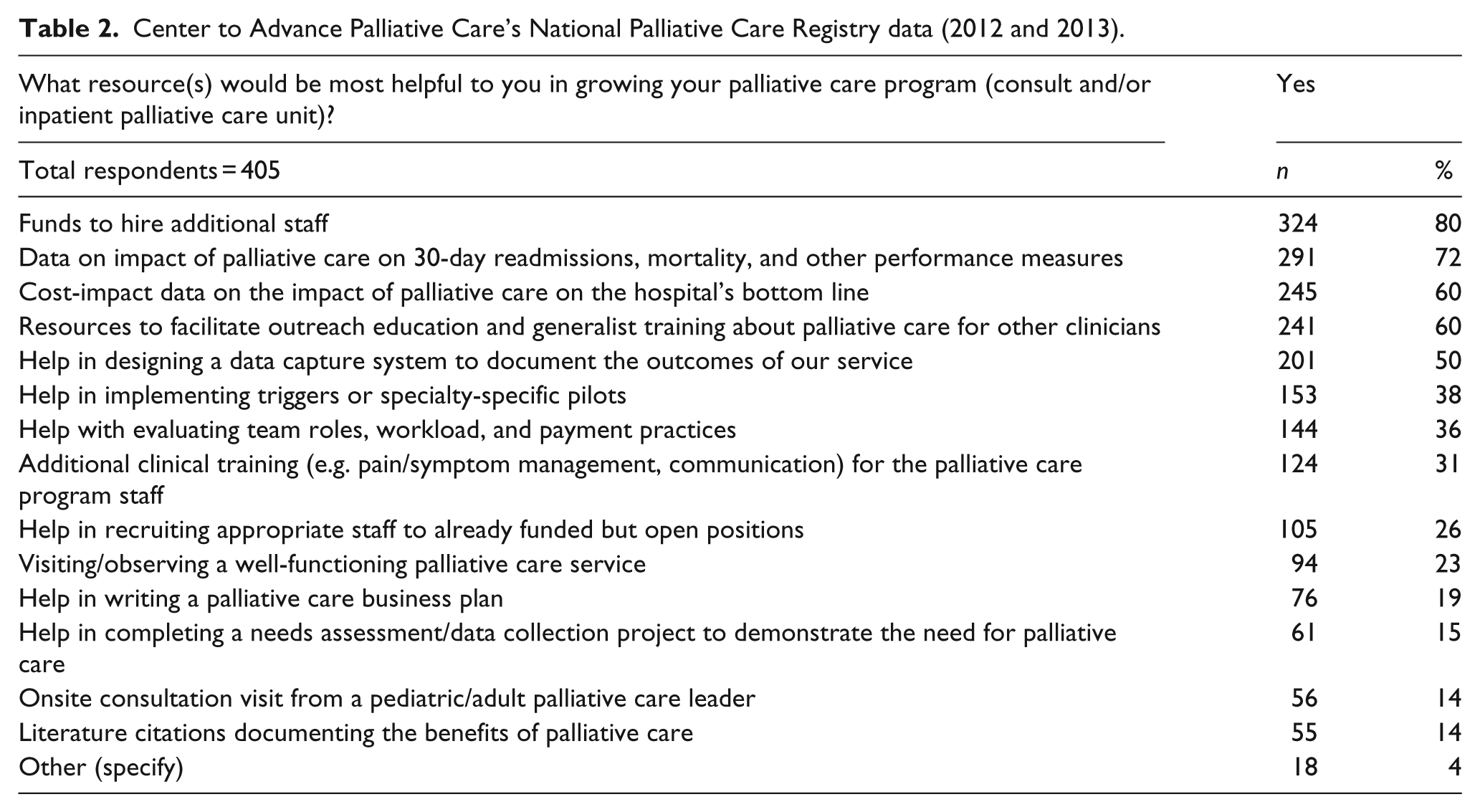
Primary data collected by the CAPC’s National Palliative Care Registry suggest the significance of this barrier to greater integration of palliative care in the United States. Our analysis of the annual program data for years 2012 and 2013 from 405 hospital-based palliative care programs nationwide finds that the barrier most often cited as hampering palliative care program growth is the need for additional staff (Table 2). Registry data show that 80% of programs report the need for funds to hire staff as the number one barrier to palliative care expansion. In addition, even when funds are available to hire palliative medicine–trained professionals, 26% of programs report difficulty recruiting appropriate staff to already funded but open positions, also a significant barrier to the expansion of their program.
Center to Advance Palliative Care’s National Palliative Care Registry data (2012 and 2013).
Analyses of registry data from years 2012 and 2013 also show that higher staffing levels in hospital-based palliative care programs are a key determinant of higher palliative care penetration in the hospital (i.e. serving more patients in need). 1 Figure 2 shows the mean palliative care service penetration for palliative care teams, from the lowest to the highest quartiles in terms of staffing.
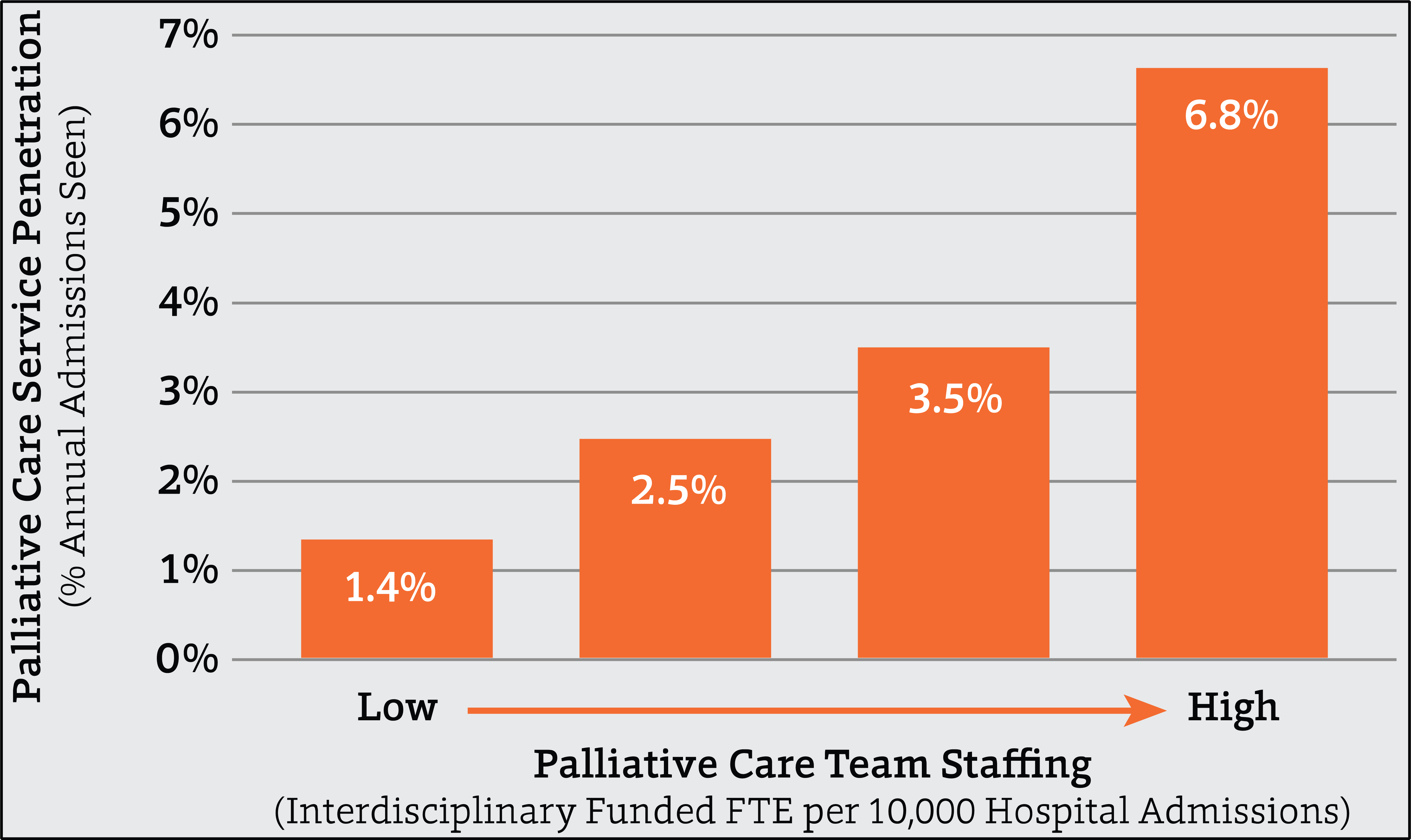
Impact of staffing on reaching patients in need.
In addition to the hospital setting, a recent study 22 of barriers to greater palliative care integration in the nursing home setting found that the most immediate barrier to improving access to palliative care in nursing homes is inadequate training and numbers of staff. Nursing homes face a significant labor shortage and high turnover because of the difficulty of the work, inadequate pay, low respect, and demanding paperwork and regulatory requirements.43,44 The adequacy of nursing home staffing is a significant issue in the United States, and strong evidence supports the relationship between increases in nurse staffing ratios and avoidance of critical quality of care problems. 45 Nursing homes tend to have lower proportion of registered nurses (RNs) than other healthcare settings, 43 and RNs working in nursing homes often have administrative and supervisory duties and deliver little direct patient care. It has been suggested that a stronger physician presence and oversight of physicians trained in palliative care are needed to improve access and quality of palliative care in the nursing home setting. 44
There are two principal reasons for the shortage of palliative medicine providers across disciplines and settings. First, palliative medicine is a new specialty, formally recognized in 2007. Thus, although the number of training programs is increasing, as of 2014 there were only 115 Accreditation Council for Graduate Medical Education (ACGME)—accredited hospice and palliative medicine fellowship training programs in the United States 46 —collectively producing approximately 280 new palliative medicine physicians annually, which does not even replace the number of hospice and palliative medicine physicians who retire each year. 42 Second, Medicare funding, which currently supports the majority of post–medical school residency training for physician specialties in the United States, does not support palliative medicine specialty training. This is a consequence of the 1997 Balanced Budget Act’s cap on Medicare-funded graduate medical education slots. The majority of academic medical centers, the site of training for medical students, residents, and fellows, currently are at or exceed their graduate medical education residency cap in terms of numbers of slots receiving Medicare graduate medical education funding. As a result, Medicare funding is unavailable for training palliative medicine physicians, and current palliative medicine fellowship training programs are inadequately supported by scarce philanthropic funding.
Challenge of identifying patients appropriate for palliative care referral
Greater integration of palliative care in the United States is also hampered by the substantial challenge of identifying and referring patients appropriate for palliative care consultation in a timely manner. Although this barrier relates both to the misperception of and lack of workforce training in palliative care, a literature review suggests that it is also a type of implementation barrier to the expansion of palliative care in the United States. The challenge of identifying patients appropriate for palliative care referral is present for both patients (and their families) and providers47 –49 as demonstrated in a number of studies.
For example, a public opinion poll of 800 adults conducted in 2011 by CAPC and the American Cancer Society reported that once informed, the vast majority (94%) of those polled wanted palliative care for themselves or a loved one in the face of a serious illness, felt it was important that patients and their loved ones were educated about palliative care, felt it was important that all hospitals offered palliative care services, and believed that palliative care services should be covered by health insurance. Three main barriers to the receipt of palliative care were identified: 47 (1) a lack of awareness of palliative care services among respondents, (2) the tendency of clinicians to equate palliative care with end-of-life care (as previously described), and (3) lack of adequate reimbursement for palliative care services by insurers. A separate poll, 48 surveying 500 US board–certified physicians, acknowledged concerns about incorporating palliative care, including the concern that introducing palliative care could interfere with therapy directed at extending life as long as possible (42%), inadequate patient resources (78%), issues related to reimbursement (82%), and a shortage of palliative care physicians and services (78%). In addition, this survey identified gaps in the education of physicians in palliative care during medical school based on physician age. The majority (73%) of physicians aged 39 years or younger reported exposure to palliative care during medical school, while only 36% of those aged 40–49 years, 23% of those aged 50–59 years, and 6% of those aged 60 years or older were exposed to palliative care during training.
The need to better identify patients appropriate for palliative care is exemplified by results of a survey of almost 170 patients with advanced cancer that evaluated both unmet needs for and interest in palliative care services. 50 More than 60% of patients reported unmet needs, primarily characterized as psychological/emotional or symptom-specific, and both were significantly associated with self-perceived need for palliative care services. The presence of these needs, however, was not associated with the likelihood that patients would initiate a request for services. This finding underscores the need for physician-initiated discussions of palliative care because patients were willing to proceed if it was suggested by their oncologist. Another study of patients with cancer, conducted at Mount Sinai Hospital, found that using standardized criteria for palliative care consultation for oncology in patients markedly increased the number and impact of palliative care consultations for this population, resulting in substantial reductions in 30-day readmissions and hospital mortality. 51
In the ED setting, the lack of clear guidelines regarding the identification of patients appropriate for palliative care consult was considered a major barrier to greater integration of palliative care by ED physicians. In a survey of 30 ED physicians at an urban, level-1 trauma center, respondents identified two major barriers to ED palliative care provision: lack of 24-h availability of a palliative care team and lack of access to complete medical records.
33
The authors noted that
Almost all respondents agreed they would initiate a palliative care consultation for a hospice patient in respiratory distress, and the majority would consult for massive intracranial hemorrhage, traumatic arrest, or metastatic cancer. However, inpatient triggers like frequent readmits for organ failure issues, e.g. dementia, congestive heart failure, and chronic obstructive pulmonary disease were rarely chosen for an ED palliative care consultation.
The authors concluded that outlining ED-specific triggers may help streamline the palliative care consultation process.
The need to establish clear triggers for referral to palliative care consultation was also evidenced in the study of patients with heart failure.26,32 One recent study 32 found that providers had limited knowledge regarding what palliative care is and how it can complement traditional heart failure therapy to decrease heart failure–related suffering. This study also identified several potential barriers to palliative care integration: the unpredictable course of heart failure, lack of clear referral triggers across the heart failure trajectory, and ambiguity regarding what differentiates standard heart failure therapy from palliative care.
Need for culture change regarding palliative care across settings
A number of barriers discussed in this report relate to the need for greater understanding and acceptance of palliative care as an upstream service in conjunction with ongoing medical treatment. One implementation-related barrier found in a recent qualitative study of hospital administrators suggests that a similar type of culture change is needed for greater implementation of palliative care in the ED. 28 In this study, semi-structured interviews were conducted with 14 key informants, including hospital executives, ED directors, and palliative care directors at a tertiary care center, a public hospital, and a community hospital. Qualitative analyses revealed that barriers to integrating palliative care and emergency medicine from the administrative perspective included the ED culture of aggressive care, limited knowledge, palliative care staffing, and medicolegal concerns. Incentives to the delivery of palliative care in the ED from these key informants’ perspective include improved patient and family satisfaction, opportunities to provide meaningful care to patients, decreased costs of care for admitted patients, and avoidance of unnecessary admissions to more intensive hospital settings, such as the ICU, for patients who have little likelihood of benefit. Therefore, although the hospital administration had great interest in integrating palliative care and emergency medicine to improve quality of care, patient and family satisfaction, and decreased length of stay for admitted patients, palliative care staffing, medicolegal concerns, and logistic issues were significant perceived barriers.
Policy-related barriers to palliative care integration in the United States
The WHO public health model identifies the policy components required for effective palliative care integration as including palliative care as part of national health plans, policies, and regulations; funding and service delivery models that support palliative care delivery; and the existence of an essential medicines policy. 4 The results of our literature review identified numerous policy-related barriers to greater implementation of palliative care in the United States.
Fragmented structure of the US healthcare system
As described in a recent Institute of Medicine report, 29 the healthcare payment system in the United States rewards the volume of medical procedures and therapies provided and typically neither recognizes nor pays for the day-to-day, long-term services that are needed for people with serious illness. In the United States, the traditional model of medical care has been dichotomous, with curative or disease-modifying treatment offered initially and comfort care through hospice provided only when/if these measures are no longer appropriate. However, many illness situations and personal goals do not lend themselves well to such dichotomous service models. 52 For example, heart failure is characterized by stable disease punctuated by acute exacerbations often requiring hospitalization. During these exacerbations, life-prolonging treatments that also improve symptom burden (such as diuretics) are administered. Within an integrated model of medical care, palliative care is provided at the same time as curative or life-prolonging treatments; however, the fragmented multi-subspecialty US healthcare delivery system makes such integration challenging.
The fee-for-service payment model in the United States also exacerbates this health system fragmentation by paying only for specific services rather than for the comprehensive care of the patient. Although there is reimbursement for palliative care physician consultation, there is currently no reimbursement for non-physician interdisciplinary team members in the acute care setting. There is also no reimbursement for family and goals of care conferences that do not require the patients’ presence, which is a common occurrence when caring for individuals with serious illness. Our analyses of the CAPC data from more than 400 hospital-based palliative care programs across the United States found that the designated palliative care physician, advanced practice nurse, and RN were primarily funded by the hospital or health system. Furthermore, although 83% reported that there was such funding in place for the palliative care physician, only 73% said there was funding in place for the advanced practice nurse and only 55% for the RN.
The impact of the fragmented structure of the US healthcare system is also evident in barriers to greater access to hospice care. Medicare policies state that to elect the Medicare hospice benefit, an individual “… waives the right to receive Medicare covered services for the terminal illness and related conditions.” 53 This criterion creates a difficult dichotomy between pursuing potentially life-prolonging treatments and pursuing palliative treatments.54 –56 A recent national survey of 591 hospices indicated that the majority (78%) had at least one restrictive enrollment policy resulting in only 39% of hospices enrolling patients receiving chemotherapy, one-half enrolling patients receiving total parental nutrition, and two-thirds enrolling patients receiving palliative radiation. 54 In addition, what constitutes care in either category may be interpreted differently by hospices and referring physicians. For example, some hospices only admit patients who have stopped all life-sustaining treatment, including chemotherapy and radiation, whereas other hospices allow some life-sustaining treatments as long as, even with the treatment, the patient is considered terminal. Furthermore, an increasing number of treatments are considered both life-prolonging and palliative (such as diuretic and other therapies for heart failure, chemotherapy, and radiation therapy), and thus the extent to which these types of treatments may be continued once the Medicare Hospice Benefit is elected is unclear. How to integrate hospice care for people whose treatment plans include concurrent disease-specific treatments and palliative care is a consequence of our fragmented system of healthcare delivery and remains a major hurdle to greater palliative care integration in the United States.
Lack of adequate reimbursement and incentives for palliative care for complex patients
Fee-for-service payment remains the dominant financing model in the US healthcare system, especially within the Medicare program which finances care for almost all Americans aged 65 years and older. This payment system provides financial incentives for increasing the volume of care provided to patients rather than the quality of services delivered. 29 Thus, for patients with serious illness at the end of life, there remains an incentive for high intensity, high-cost services, including tests, procedures, and hospitalizations. 29 This system may even discourage timely referral to hospice. A study 57 of more than 286,000 fee-for-service Medicare patients in 2009 found that although 42% were enrolled in hospice at the time of their death, 28% were under hospice care for 3 days or less. In addition, more than 40% of late enrollments in hospice were preceded by an ICU stay. Incentives (e.g. pay for performance programs) that would reward hospitals for offering palliative care consultation or early hospice referral for patients with complex, multiple comorbidity, and end-stage disease do not exist.
In conjunction with the limitations of a fee-for-service payment structure, there are significant gaps in the reimbursement for palliative care services. For example, there is no reimbursement for non-physician interdisciplinary palliative care team members in the acute care setting and no reimbursable code for family and goals of care conferences with family members when (as it is very often the case) the patient is too ill to participate. Medicare similarly does not reimburse interdisciplinary palliative care team services for nursing home residents unless they are enrolled in hospice. Moreover, as detailed in a systematic review of nursing home end-of-life care, 30 a range of other nursing home regulatory and payment policies further impede integrating palliative care services earlier in caring for nursing home residents with advanced illness. In particular, Medicare generally places higher priority on rehabilitative care (e.g. over end-of-life care) in the way it reimburses services, in the way it defines and assesses nursing home quality of care, and even in the way it defines service eligibility standards. 30 Although there is significant ongoing debate within the United States regarding the fee-for-service payment system, it is the model that will likely continue at least in the short term to dominate in the United States, 58 and thus reform efforts to increase access to integrated palliative care must be created to work within this framework, not only in the community but also in other settings of care.
Need for greater funding for palliative care research
In the United States, federal funding through the National Institutes of Health (NIH), the Veteran’s Administration, and the Agency for Healthcare Research and Quality (AHRQ) is inadequate and is a significant barrier to greater integration of palliative care. 34 A recent study reported that from 2006 to 2010, grants related to palliative care research comprised 0.2% of total grants awarded by the NIH. 59 Furthermore, only three agencies—the National Cancer Institute (0.4% of all NCI awarded grants), the National Institute for Nursing Research (7.6% of all NINR awarded grants), and the National Institute on Aging (0.8% of all NIA awarded grants)—funded 82% of all palliative care research awards. 59 The same study found that of the 1253 original research papers published in palliative care from 2006 to 2010, only one-fifth were supported by federal research dollars. 59
There are a number of reasons for this limited investment in palliative care research. First, there is no federal agency specifically charged with a focus on palliative care and on persons with serious illness. The NIH institutes are largely disease-specific, and thus palliative care, with its applicability to all serious illnesses, does not fit well within a particular institute’s scope. Second, recent budget cuts have further hampered the ability of the NIH to fund new research or new investigators that might be perceived as outside of their core missions. Third, there is no study section that specifically focuses on palliative care, and existing study sections tend to have a maximum of only one to two reviewers with expertise in palliative care research. Study section representation is critical as peers with appropriate content and methodological expertise in palliative care rarely review palliative care grant submissions, reducing their likelihood of being funded. 34
Regulatory barriers to greater palliative care integration in the nursing home setting
Our literature review identified nursing home setting as the one in which significant policy-related barriers to palliative care expansion exist. The goals of palliative care address critical issues for individuals with complex and serious illness residing in nursing homes, including pain and symptom management, communication, preparation for death, decisions about treatment preferences, and caregiver support. Because of the uncertain prognosis associated with chronic nonmalignant diseases such as dementia, many nursing home residents are either not referred to hospice or have very short hospice stays. The integration of palliative care into nursing homes offers a potential solution to the challenges relating to hospice eligibility, staffing, training, and obtaining adequate reimbursement for care that aligns with resident and surrogate’s preferences and needs. However, the delivery of palliative care in nursing homes in the United States is hindered by policy issues related to both regulatory and staffing barriers and, as a result, is rare.22,30,44,60
A recent review article 22 drew on interviews with nursing home executives, practitioners, and researchers to describe the regulatory and staffing-related barriers to nursing home palliative care. This study found that a major regulatory barrier to delivering palliative care in the nursing home is the misperception that palliative care is incompatible with the restorative focus of nursing home reimbursement and regulation. This is demonstrated by the fact that the prospective reimbursement categories that must be used by nursing homes, called Resource Utilization Groups, do not include palliative care. Resource Utilization Groups for intensive rehabilitation or skilled care (e.g. intravenous medications and tube feeding) are far more generously reimbursed than personal care, symptom management, and emotional and spiritual support, creating a direct financial incentive for artificial nutrition and hydration and intravenous therapies even among the very debilitated and dying.
Options to expand integrated palliative care in the United States
Shift to value-based purchasing and reimbursement
Mounting evidence that palliative care improves quality, prevents crises and avoidable hospitalizations, and reduces healthcare costs for patients with serious illness and their families represents an opportunity for palliative care program growth. In 2013, the United States spent US$2.9 trillion on healthcare costs 61 and projections suggest that by 2040, 1 out of every US$3 spent in the United States will be spent on healthcare. 62 Healthcare spending is highly concentrated among a small seriously ill population, whereby 5% of patients account for 50% of total healthcare costs. 63 This population is characterized by both chronic conditions and functional limitations and is thus likely appropriate for integrated palliative care. Expansion of palliative care offers an unrivaled opportunity to increase the value (i.e. better quality leads to lower costs) of healthcare.
There is an increasing body of research demonstrating that inpatient palliative care lowers costs by preventing symptom crises and matching treatments to patient goals thereby reducing misutilization. A recent review of 46 studies evaluating the impact of palliative care interventions on cost or healthcare utilization found that despite wide variation in study type, characteristic, and study quality, palliative care was found to be less costly relative to comparator groups, and in most cases, the difference in cost was statistically significant. 64 For example, one study estimated the financial impact of palliative care across eight hospitals in six states to assess its potential cost savings in a hospital setting. 16 Palliative care patients discharged alive had net savings of US$1696 in direct costs per admission and US$279 per day, and those who died in the hospital had adjusted net savings of US$4908 in direct costs per admission and US$374 per day. 16 Two studies analyzing the impact of palliative care consultations in the hospital on costs for veterans hospitalized with advanced disease found average savings of US$464 in direct costs per day 65 and US$239 in direct costs per day. 66 Cost savings in a sample of 3605 patients hospitalized in two academic medical centers were estimated to be US$2141 per admission for those with stays of 1 week or less, US$2870 in savings for those with stays of 1 week to 1 month, and no cost savings for those with stays of more than 1 month. 67 Focusing on the Medicaid population in a single state (New York), another study attributed an average savings of US$4098 in hospital costs per palliative care consult for patients discharged alive and a savings of US$7563 for patients who died in the hospital. 15 A more recent study evaluating the impact of hospital-based palliative care consultation on direct costs found savings of US$3426 per inpatient stay for those who died in the hospital although no cost savings for those discharged from the hospital alive. 68
A smaller group of studies have also demonstrated reduced costs associated with outpatient palliative care across the entire course of illness, as summarized in a recent review article. 69 For example, a randomized control trial of outpatient palliative care in addition to usual care among 151 patients newly diagnosed with stage IV non-small cell lung cancer found that those in the palliative care intervention group were less likely to have depressive symptoms, had improved survival (a gain of almost 3 months), and lower rates of ED visits and hospital admissions. Palliative care was also associated with less aggressive end-of-life care including less chemotherapy within the last 14 days and earlier referral to hospice—measures indicative of higher quality and lower costs. 70 Similarly, a randomized control trial of home-based palliative care for 298 homebound, terminally ill patients demonstrated improved satisfaction, fewer hospital days and ED visits, and lower costs (mean reduction of US$7552 per capita, in 2002 dollars). 71 A randomized control trial of palliative care consultation in a primary care clinic setting resulted in fewer primary care and urgent care visits, yet no difference in use of the ED and hospital. 72 Finally, a recent observational study of 686 decedents found cost savings associated with a home-based palliative care program of US$3908 per patient per month during the last 3 months of life and US$7172 per patient per month in the last 2 weeks of life. 73
The combination of fiscal pressures and mounting evidence supporting palliative care’s ability to reduce costs has led to greater investment in palliative care programs by private insurers. Medicare and Medicaid are increasingly privatized, with some states already exceeding 40% penetration of Medicare Advantage plans. 74 The Congressional Budget Office estimates that an additional 38%, totaling 22 million beneficiaries, will enroll in Medicare Advantage plans by 2020. These managed care plans are rapidly building and expanding palliative care programs as a means of achieving better value. The private insurer’s capacity to integrate palliative care to a level that the government could not do represents an important opportunity for the growth of integrated palliative care programs in the United States.
Greater investment in palliative care research
Our review of the literature on barriers to palliative care expansion in the United States underscores the need for increased funding for palliative care research and investigators. Building the evidence base for the impact of palliative care on both quality of care and healthcare costs is crucial to its expansion across settings and is dependent upon funding from at the federal level. Funding mechanisms for palliative care research should be developed in all NIH institutes, the AHRQ, as well as in the Veterans Administration. Specific policy initiatives regarding palliative care research investment could be integrated within the current biomedical research funding structures and include the following: 34
NIH/AHRQ should allocate 2% of their current budgets to focus on the needs of patients with serious illness and their families, and developing and evaluating new models of care delivery, symptom relief, and communication and research focused on the impact of concurrent palliative care along with disease-directed therapies for patients with serious illness. 34
Development of a Center for Scientific Review study section that specifically focuses on serious illness and moves beyond disease and biology-specific topic areas. 34
NIH should establish an Office of Palliative Care Research modeled after the Office of AIDS Research to oversee and ensure appropriate distribution of research funding. This is particularly important given that the priorities for palliative care research cross multiple diseases and conditions and are not well matched by the current disease-specific silos of NIH. 34
NIH, AHRQ, and Patient-Centered Outcomes Research Institute need to develop specific Program Announcements and Request for Applications targeted to the research priorities in palliative care. 34
Existing NIH career development award mechanisms should be utilized to support junior investigators and midcareer palliative care investigators in order to build a critical mass of established palliative care researchers. 34
Expansion of the palliative medicine–trained workforce
To address the significant workforce-related barriers identified in this report, a multipronged approach to training professionals in palliative medicine is required to ensure that Americans with serious illness and their families have access to quality palliative care. First, palliative medicine is the fastest growing medical subspecialty in the United States, and thus expansion and support of fellowship programs is needed. Second, a substantial number of midcareer physicians are seeking training in order to transition from their current field of practice into palliative medicine, and supporting these individuals is crucial to address the workforce shortage in palliative medicine. Third, all physicians who care for patients with serious illness should be trained in the core principles of palliative medicine to ensure that they know how to communicate with seriously ill patients and treat pain and other distressing symptoms. Several policy initiatives are likely to have a major impact on increasing the current number of palliative care clinicians, including proposals to the following:
Lift the Graduate Medical Education cap on Medicare-funded residency positions and redistribute unused Graduate Medical Education slots to support ACGME-approved palliative medicine fellowship training.
Establish loan-forgiveness programs for palliative care physicians and nurses through the Health Resources and Services Administration to promote palliative care as a viable career path for young healthcare professionals.
Create Health Resources and Services Adminis-tration Title VII–supported career development awards (similar to Geriatric Health Professions Training Programs) to support clinician-educators who can integrate palliative care into medical, nursing school, and postgraduate training curricula.
Establish Health Resources and Services Administration awards to support retraining of midcareer current medical and nursing workforce for this new specialty.
Require Continuing Medical Education training for referring physicians as a condition of licensure at the state level—similar to California’s provision for pain management training—that would ensure physician’s competency in the core principles and practice of palliative medicine.
Establishment of guidelines to “trigger” palliative care consultation
To address the need to more easily identify patients appropriate for palliative care referral, a 2011 consensus statement from the CAPC proposed criteria for identifying patients in need of palliative care assessment in the hospital setting. 75 The palliative care needs of patients meeting one or more of these criteria should be addressed by their primary medical team, with consultation by palliative care specialists to assist with time-intensive complex decision-making regarding goals of care and treatment options; to make recommendations regarding pain and symptom management; and to help address complicated psychosocial, spiritual, and social issues.
While criteria for palliative care assessments are not available for patients in the outpatient setting, the primary care clinician should consider consultation to a palliative care specialist team for patients who have poorly controlled symptoms, frequent visits to the emergency room, one or more hospital admissions in 30 days, a prolonged hospitalization, and/or a prolonged ICU stay. An affirmative answer by the primary care clinician to the consideration (or “surprise question”): “Would you not be surprised if the patient died within 12 months, or did not live to adulthood” might also guide the identification of patients who would benefit from a palliative care assessment.
Similarly, there is a need to develop and test a tool to identify patients with chronic conditions in need of palliative care in the general population. Efforts to do this are already underway. A recent population-based study 76 in Spain aimed to determine, by direct measurement, the prevalence of people in need of palliative care among a sample of advanced chronically ill patients. They found that based on clinician’s responses to the surprise question and other indicators, 1.5% of study population were in need of pal-liative care demonstrating that direct measurement of prevalence of palliative care needs on a population basis is feasible. Early identification and prevalence determination of these patients is likely to be the cornerstone of palliative care public health policies.
In summary, there are numerous opportunities to increase access to integrated palliative care in the United States and options to do so exist for multiple stakeholders within the healthcare system. Table 3 summarizes some of the most pertinent options in the United States for increasing the penetration of integrated palliative care.
Options for advancing integrated palliative care in the United States.
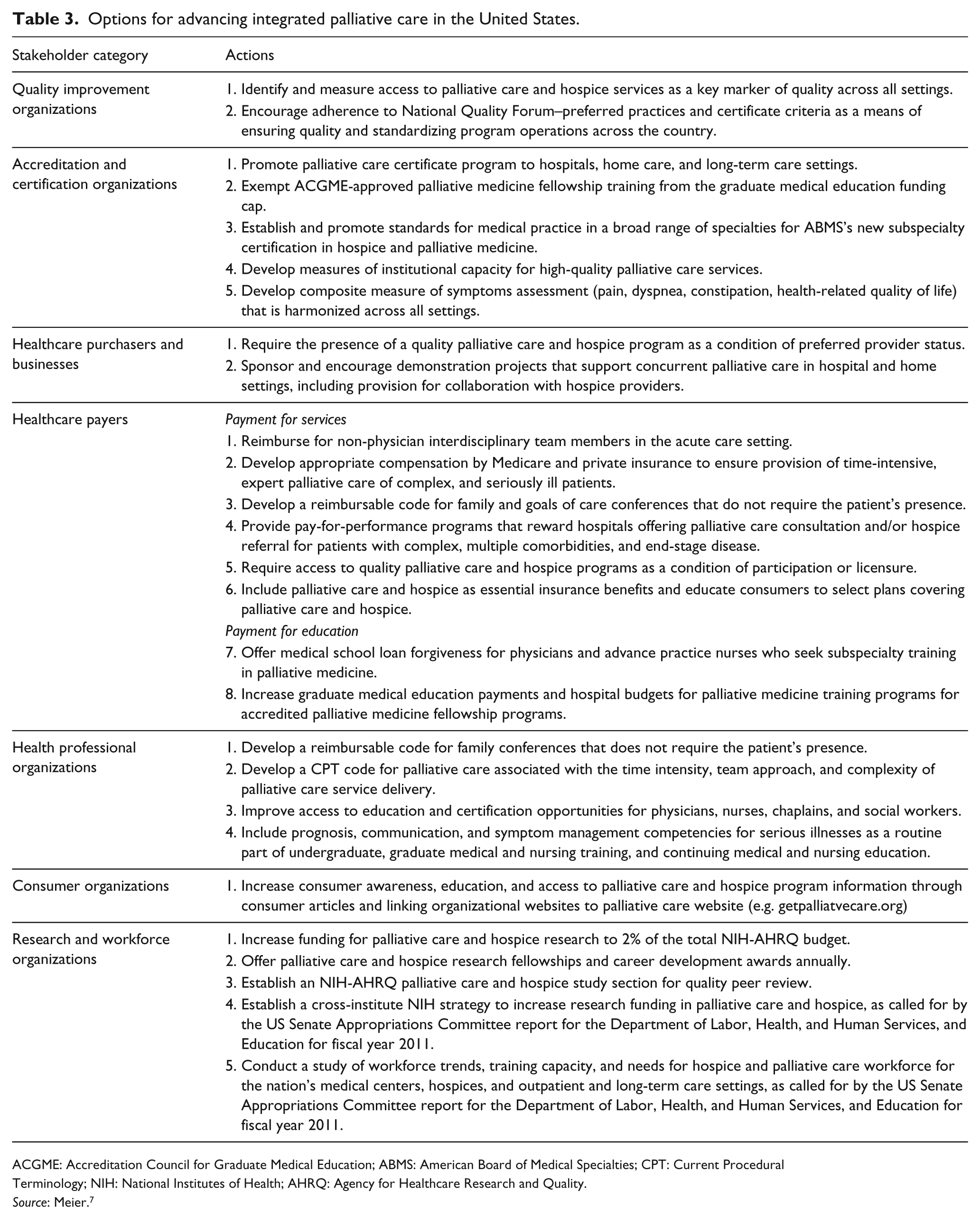
ACGME: Accreditation Council for Graduate Medical Education; ABMS: American Board of Medical Specialties; CPT: Current Procedural Terminology; NIH: National Institutes of Health; AHRQ: Agency for Healthcare Research and Quality.
Source: Meier. 7
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was conducted on behalf of the InSup-C project on patient-centered integrated palliative care. An EU Framework 7 Programme (FP7/2007-2013).