
Abstract
Background:
Patients with advanced cystic fibrosis have severe symptoms with a complex trajectory of exacerbations and recovery. They are often awaiting lung transplantation, and many die without receiving specialist palliative care.
Aim:
We introduced an integrated model whereby palliative specialists joined the cystic fibrosis team to provide palliative care in parallel with standard care.
Design:
A service evaluation of this model of care was undertaken in a prospective case series documenting symptoms and outcomes, the views of the cystic fibrosis team and the experience of the palliative specialists.
Setting/participants:
Over 3 years, 28 (10%) of 282 patients attending the cystic fibrosis centre had specialist palliative care.
Results:
They had advanced lung disease (mean forced expiratory volume in 1 s (FEV1) = 0.86 L (25% predicted)), and 17 died: 6 were on a transplant waiting list at death; 10 were unsuitable and 1 died post transplantation. All who died over these 3 years had specialist palliative care. Four patients had successful transplants. Assessment showed a high prevalence of breathlessness, cough, pain, vomiting and fatigue, with a significant impact on daily life. The cystic fibrosis team rated this model of care highly, felt that palliative care should be members of the team, and thought that patients had found it helpful. The palliative specialists gained knowledge of cystic fibrosis, found it beneficial to meet patients earlier in the disease, and identified unmet needs in managing bereavement and the effects of deaths on other patients with cystic fibrosis.
Conclusion:
This model has been successful in overcoming the difficulties in access to specialist palliative care for patients with cystic fibrosis.
Keywords
Many patients with cystic fibrosis (CF) are on a transplant waiting list at the time of death.
They are treated in specialist CF centres and often do not receive specialist palliative care.
Integrating palliative specialists into the multidisciplinary CF team was successful in overcoming difficulties in access to palliative care, and all patients who died received specialist palliative care.
This integrated model of care allowed standard CF treatments and palliative interventions to be delivered in parallel.
Both CF and palliative specialists found this model of care useful for patients.
Palliative care is a key component of a comprehensive CF service and palliative specialists should form part of the multidisciplinary team.
Introduction
There are about 140 deaths in the United Kingdom each year from cystic fibrosis (CF) at a median age of 29 years. 1 Many patients are on a lung transplant waiting list during advanced disease but about 33% die before donor lungs become available. 2 For patients who are unsuitable for transplantation, the clinical course is characterised by a trajectory of recurrent exacerbations and recovery, with a slow deterioration over several years (Figure 1). Traditionally, CF teams provide holistic supportive care but have regarded palliative care as a separate phase at the end of life when treatment options have been exhausted.2,3
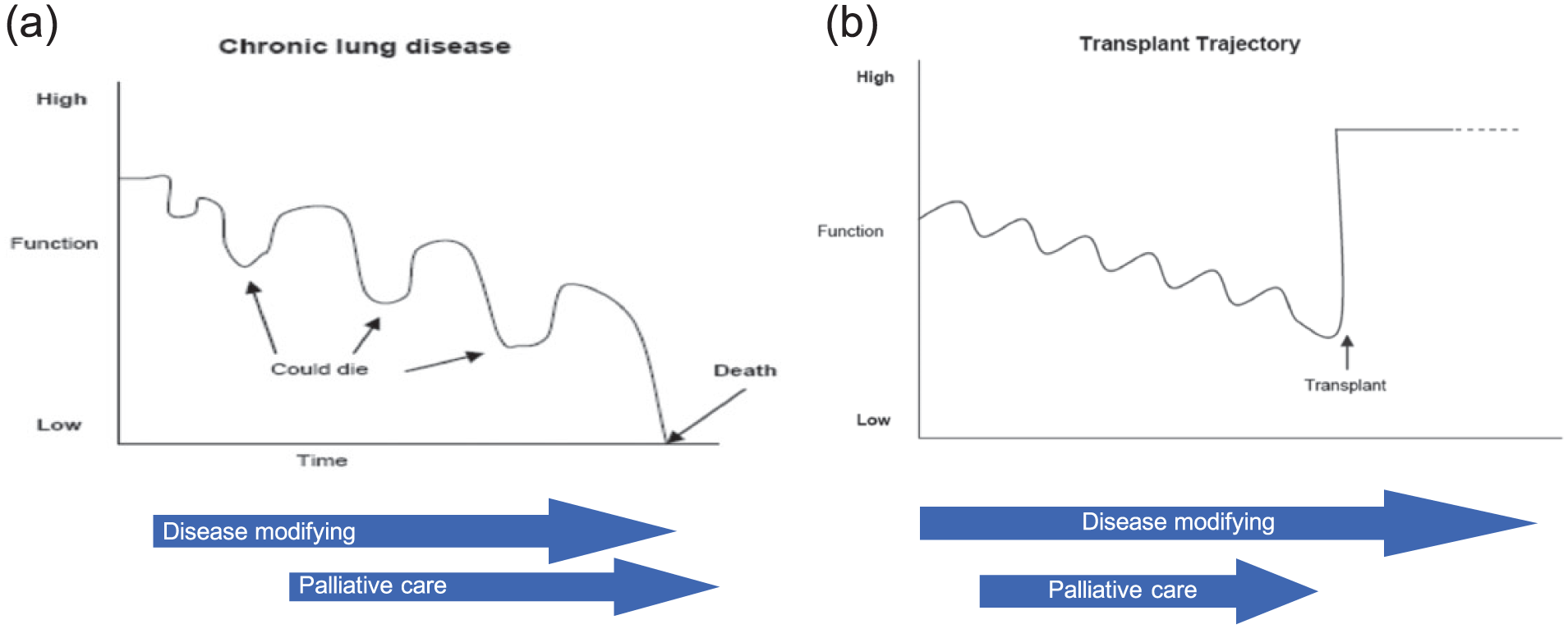
Trajectories of advanced CF disease. (a) Advanced CF is characterised by exacerbations and recovery with a gradual decline over several years, such that disease-modifying treatments and palliative care run in parallel. (b) Some patients who are critically ill with advanced CF undergo lung transplantation which dramatically alters the disease trajectory.
Service development and evaluation
We introduced an integrated model, whereby a palliative medicine physician and nurse became core members of the CF team, delivering palliative care in parallel with standard CF treatments. They attend the weekly CF clinical meeting, discussing patients at all stages of the disease. Specialist palliative care consultations are offered when there is advanced disease with declining lung function and when lung transplantation is being considered. The service was evaluated by a confidential survey of the CF team using a locally developed questionnaire, and the palliative specialists documented their experience (Appendix 1). The key aim was to assess if this model of palliative care was acceptable to the CF team and their patients, and whether the palliative specialists encountered difficulties in delivering palliative care in parallel with standard CF care, including lung transplantation.
Over a 3-year period from 2011 to 2014, patients who had advanced progressive disease and all who were being considered for lung transplantation had a palliative assessment, and the impact of symptoms was measured using the palliative care assessment tool which is a patient-reported outcome measure rating symptoms. This is a four-point scale: 0 = absent; 1 = present, not effecting daily life; 2 = present, moderate effect on daily life and 3 = present, daily life dominated by symptom. 4 A Macmillan occupational therapist and physiotherapist provided additional assessment and interventions. Members of the CF team attended funerals, and all deaths, and their impact on other patients, were discussed at the team meeting.
This project was registered as a service evaluation and quality improvement audit within our institution. Audit projects and evaluations are undertaken, reported and presented to improve the quality of care for patients, and results are disseminated to spread best practice to other areas.
Results
Patients
Over the 3-year period, there were 282 patients attending the CF centre with an age range of 16–74 years; 28 (10%) had specialist palliative care input. Their mean age was 31 (range = 18–47) years, and they had advanced disease with a mean forced expiratory volume in 1 s (FEV1) of 0.86 L (24.6% of predicted values) and a mean body mass index of 19.3 kg/m2. They had complex lung infections with 26 having chronic Pseudomonas aeruginosa, four Burkholderia cepacia complex and two Meticillin resistant Staphylococcus aureus infection. A total of 11 patients were on oxygen therapy and 4 were receiving non-invasive ventilation; 14 were receiving supplemental feeding via a gastrostomy tube. Many had additional complications: two had renal impairment and one was receiving peritoneal dialysis; one patient had co-incidental motor neuron disease (amyotrophic lateral sclerosis), one had chylous ascites, one had undergone colectomy for Clostridium difficile colitis, one suffered a pneumothorax requiring insertion of a chest tube, two patients had recurrent episodes of distal intestinal obstruction syndrome and two had major haemoptysis treated by bronchial artery embolisation.
Seventeen of these patients died: 6 were on a transplant waiting list at the time of death; 10 were unsuitable for transplantation and one patient died 14 years after lung transplantation of bronchiolitis obliterans. Four patients had successful lung transplantation with a dramatic improvement in their clinical status. Seven patients are in ongoing care, three of whom are awaiting transplantation. Of the 17 deaths, 15 (88%) occurred on the CF ward and 2 patients died at home. Typically, the end-of-life phase was short over a period of a few hours or days when the patient failed to respond to treatment of an exacerbation. Two patients had their own young children, and three patients had siblings with CF visiting during the end-of-life phase. Only 1 of 29 patients approached declined a palliative care consultation; she subsequently underwent successful transplantation. All patients who died over the 3-year period had had specialist palliative input.
Symptoms and palliative interventions
Table 1 shows the prevalence of symptoms at the initial specialist palliative consultation. Breathlessness, cough, pain, nausea, low mood, anxiety, vomiting and fatigue were the dominant symptoms. The initial palliative care assessment (PaCA) scores were high with a mean PaCA score of 2.5 (range = 2–3, standard deviation (SD) = 0.5), indicating that daily life was dominated by the symptom. 4 A range of palliative interventions was applied in managing symptoms, and included pharmacological treatments (e.g. opioid, benzodiazepine, anti-emetic and anti-depressant medications) and non-pharmacological therapies. Therapist input included relaxation techniques, massage, acupuncture/acupressure techniques, cognitive behavioural therapy and assessment of practical daily activities with techniques for management of fatigue and anxiety.5,6 Purposeful activity was used to promote patient control over aspects of daily living, enabling a sense of achievement and facilitating positive change in mood and motivation.
Prevalence of symptoms at initial specialist PaCA.
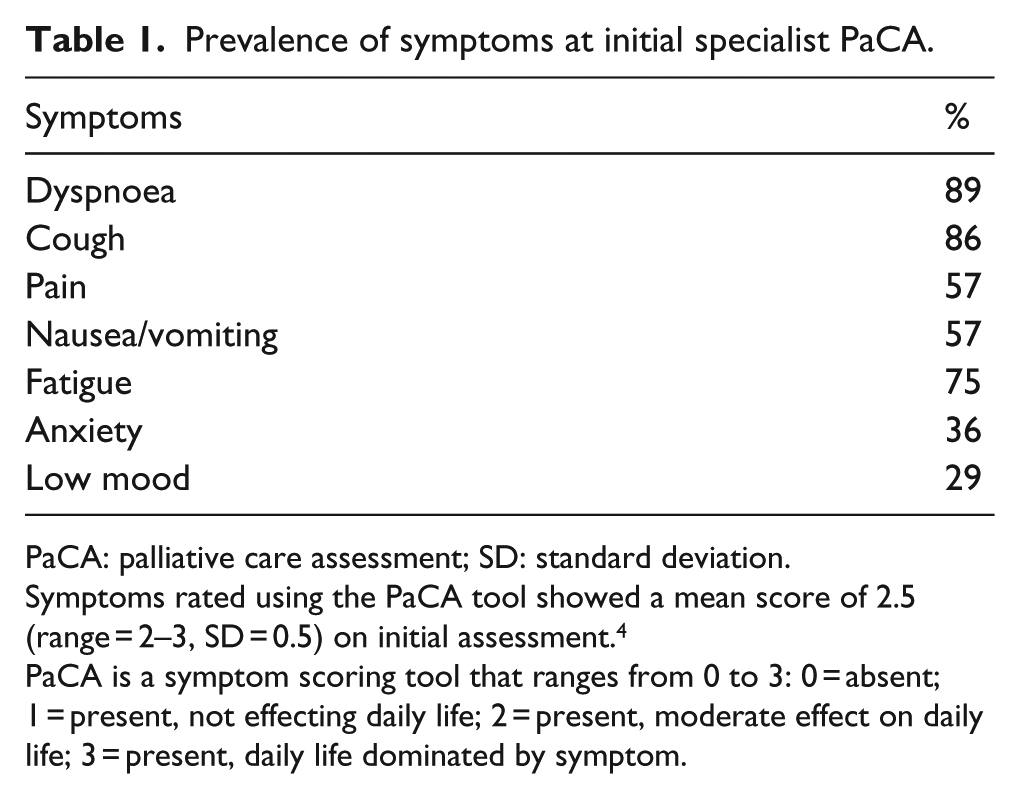
PaCA: palliative care assessment; SD: standard deviation.
Symptoms rated using the PaCA tool showed a mean score of 2.5 (range = 2–3, SD = 0.5) on initial assessment. 4
PaCA is a symptom scoring tool that ranges from 0 to 3: 0 = absent; 1 = present, not effecting daily life; 2 = present, moderate effect on daily life; 3 = present, daily life dominated by symptom.
Evaluation of palliative care
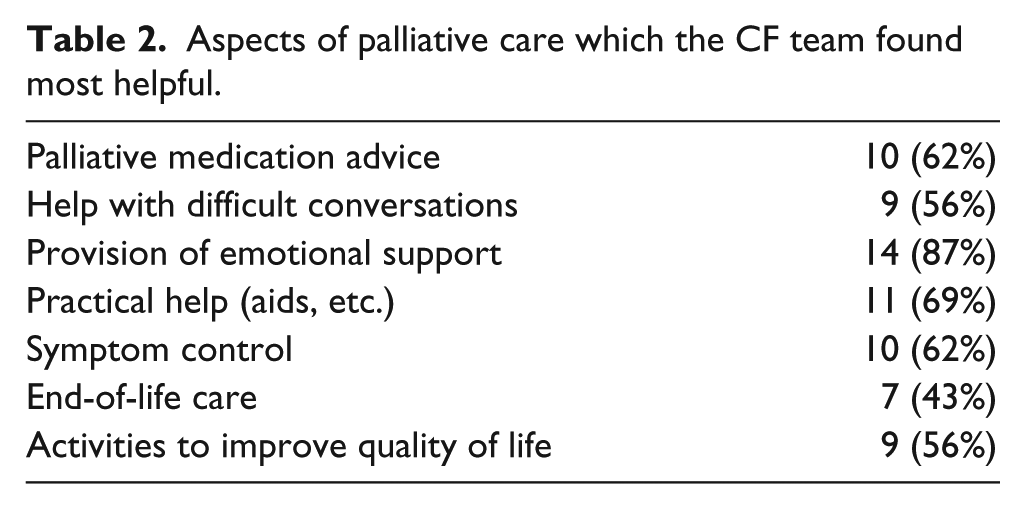
The survey was completed by 16 (89%) of 18 members of the general CF team. All rated the model of care highly with a mean score of 4.1 on a scale from 1 (poor) to 5 (excellent), and all felt that palliative specialists should be core members of the team. Table 2 shows which aspects of palliative care were considered to be particularly helpful; 11 thought that patients had found input ‘very helpful’, 5 thought it had been ‘helpful’, and none thought that it was ‘not helpful’. The main issue raised was that patients needed help in understanding the role of palliative care as some patients felt that a palliative care consultation indicated that death was imminent. The palliative specialists found it helpful to meet patients earlier in the course of the disease, they had an initial learning curve about CF, and the workload was significant in managing the complex needs of these young adults. They identified further unmet needs particularly relating to bereavement support of families and the impact of deaths on other patients.
Aspects of palliative care which the CF team found most helpful.
Discussion
This model of integrated palliative care was successful in improving specialist palliative care involvement and adding to the care given to these patients. All patients who died at our CF centre over the 3-year study period had specialist palliative care input. Patients and families found specialist palliative care acceptable with only one patient declining a palliative consultation. Standard disease-modifying treatments and palliative interventions were applied in parallel without difficulties.7–9 Both CF and palliative specialists derived benefit in the exchange of knowledge and skills.
Recent CF guidelines refer to the need for palliative care as part of a comprehensive CF service.10,11 In CF, advance care planning is inherently complex because of the dichotomy in the trajectory of the disease as to whether successful transplantation occurs or whether the patient dies before donor organs become available. Many specific disease-modifying treatments remain effective in relieving symptoms such that they are continued late into the course of the disease. The specialist palliative care consultations focussed on symptom management, supportive care and quality of life at an earlier stage, and end-of-life care in those who progressed to the dying phase.5,12 Deaths predominantly occurred in the specialist CF ward, which is familiar to these patients and their families, and is often their preferred place of care. There are close links with community-based palliative teams, and two patients died at home.
This project focussed on evaluating the development of an integrated palliative care service rather than assessing the efficacy of palliative interventions. The introduction of palliative care at an earlier stage of the disease was perceived as being helpful for patients and their families. Further research is needed to define the most effective interventions for relief of symptoms, to assess the patients’ perspective on the support needed and to develop bereavement services for families and friends.13–15
Footnotes
Appendix 1
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.