
Abstract
Background:
Unused medicines represent a major source of wastage in healthcare systems around the world. Previous studies have suggested the potential cost savings from recycling the waste medicines. However, issues of product safety and integrity often deter healthcare institutions from recycling donated medications.
Aim:
To evaluate the feasibility of medication recycling and to assess the actual cost savings from recycling waste medicines and whether reusability of waste medicines differed among various drug classes and donor sources.
Design and setting:
Donated medications from hospitals, private medical clinics and patients were collected and assessed using a medication recycling protocol in a hospice care setting from November 2013 through January 2014. Costs were calculated using a reference pricing list from a public hospital.
Results:
A total of 244 donations, amounting to 20,759 dosage units, were collected during the study period. Most donations (90.8%) were reusable, providing a total of S$5266 in cost savings. Less than 2 h daily was spent by a single pharmacy technician on the sorting and distributing processes. Medications donated by health facilities were thrice more likely to be reusable than those by patients (odds ratio = 3.614, 95% confidence interval = 3.127, 4.176). Medications belonging to Anatomical Therapeutic Chemical class G (0.0%), H (8.2%) and L (30.0%) were the least reusable.
Conclusion:
Most donated medications were reusable. The current protocol can be further streamlined to focus on the more reusable donor sources and drug classes and validated in other settings. Overall, we opine that it is feasible to practise medication recycling on a larger scale to reduce medication wastage.
Wastage from unused medications is a prevalent and costly issue.
Despite studies suggesting the financial benefits of medication recycling, actual cost savings from recycling waste medicines are not known.
States and healthcare institutions remain divided on recycling waste medicines due to safety concerns.
We developed and implemented a detailed protocol for medication recycling.
With appropriate checks in place, medication recycling can provide cost savings without compromising patient safety.
Reusability of waste medicines can differ significantly among various drug classes and donor sources.
Our medication recycling protocol can be further implemented and validated in other settings to support medication recycling.
Introduction
The World Health Organization reported a total of 0.2–0.5 kg of waste being generated per hospital bed per day, of which 3% was attributable to drug wastage. 1 Every year in the United States, as much as US$5b worth of unexpired medicines from all sources were discarded and as many as 10 million of these medicines could be recycled. 2 Redistributing the unused medications to those who need them may potentially reduce non-compliance and the associated healthcare costs. According to the 2013 report on avoidable costs in US healthcare by IMS Institute for healthcare informatics, cost from non-adherence in general (US$105b) constituted almost half of the total avoidable healthcare costs. 3
In England, cost of waste medications in primary and community care was estimated to be ₤300m a year, of which almost one-fifth of the waste medications were completely unused. 4 Faced with financial challenges in public funding and an ageing population, the National Health Service (NHS) was tasked with finding ₤20b in efficiency savings by 2015 and minimising medicine waste was one of its priorities. 5
To reduce medicine waste, NHS adopted strategies such as restricting prescription lengths, conducting medication reviews, use of patients’ own drugs (PODs) and repeat dispensing schemes.4,6 Limiting the prescription length for newly prescribed drugs minimises drug wastage in the event of discontinuation due to allergy or adverse drug reactions. 6 Medication reviews and repeat dispensing schemes ensure that non-indicated medications are discontinued promptly to avoid unnecessary drug supply. 7
While these measures have been effective in controlling drug wastage, it is not possible to indefinitely shorten prescription lengths, dispense partial supply or perform medication reviews in view of the associated processing time and costs.4,6 Furthermore, there are several major causes of drug wastage such as patient death and adverse drug events which are largely unavoidable.4,8
Several studies have shown that a substantial proportion of the unused medicines can potentially be reused.4,8 Discarding the medicines indiscriminately would mean wasting the opportunity to distribute to the needy and reduce healthcare spending. Drug recycling programmes with appropriate checks can be implemented to allow medications to be safely reused and money to be saved. Several states in the United States have already implemented drug recycling programmes. 9 Donations from patients and healthcare facilities are screened for reusability and redistributed to the needy who cannot afford the medications. In comparison, policies in the United Kingdom mandate that all returned medicine must be destroyed and none to be reused due to concerns such as quality assurance. 8
There are general guidelines on medication recycling by bodies such as the American Society of Consultant Pharmacists (ASCP). However, to provide the assurances that make medication recycling safe, a robust and consistent protocol that offers detailed steps on medication recycling is needed. We conducted a pilot study to evaluate our protocol on medication recycling and to assess the amount of drug wastage and the cost savings from recycling the waste medicines. We also investigated the reusability of the donations by source and drug class which could be used to streamline the recycling process for future studies.
Methods
Participants and study period
All donated medications were collected at the Hospice Care Association (HCA) from 1 November 2013 through 31 January 2014. Donated items, including controlled drugs, were evaluated using a protocol developed by pharmacist volunteers in HCA (Figure 1). Medications were discarded using guidelines recommended by the ministry of health and the national environment agency (see Appendix 1) if they were expired or unlabelled with an expiry date, thermolabile in nature, unsealed in the form of loose tablets, liquid or semi-solid dosage forms or physically degraded. Examples of degradation include discoloration of tablets, precipitation of solutions, caking of suspensions, creaming or coalescence of emulsions or ointments. These criteria were similar to those for the reuse of PODs except the requirement for the reused dosage unit to be in their original sealed packaging. 10 This criterion was important to ensure the safety of the recipient. Additionally, items that were not in the list of registered medicinal products were discarded. 11
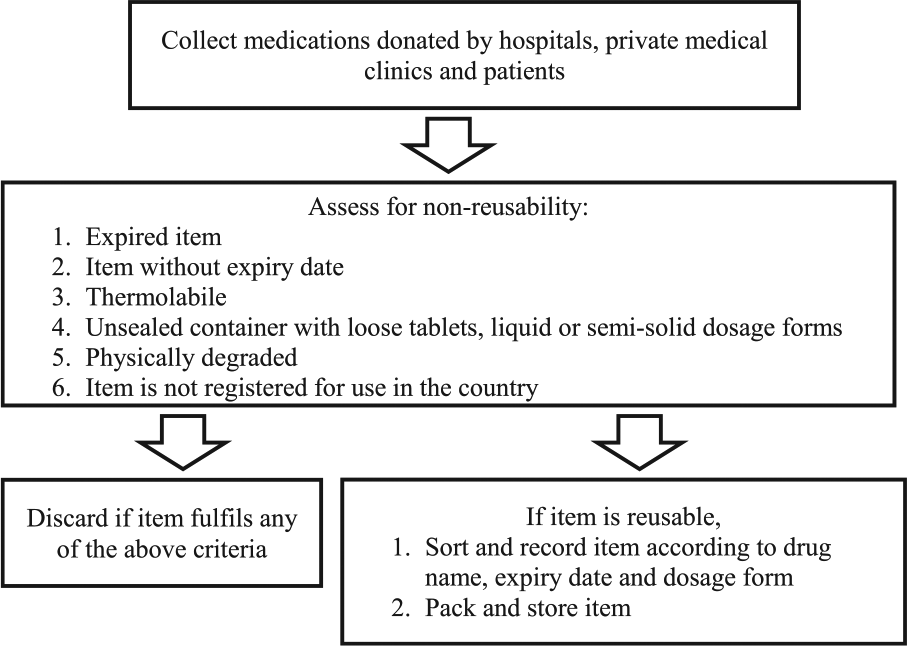
Protocol for evaluation and redistribution of donated medications.
Data collection and analysis
Each drug was counted as one dosage unit regardless of dosage form (e.g. tablet, capsule or syrup). Pricing of medication was obtained from the National Cancer Centre Singapore formulary list. Potential wastage costs were calculated based on the price of the donated medications, assuming that none was reused. Cost savings were based on the total price of the reused medications, excluding the discarded medications.
Medications were categorised according to the first level Anatomical Therapeutic Chemical (ATC) classification by the World Health Organization Collaborating Centre for Drug Statistics Methodology (WHOCC), which is the gold standard for international drug utilisation research. 12
Donation sources were classified into hospitals, private medical clinics and patients (i.e. patients and their caregivers). Descriptive statistics were used to describe the type, source and usability of donated medications. Chi-square test was conducted to assess the statistical significance of the relation between the donation source and drug usability. Univariate logistic regression was used to assess the relation between the ATC class and drug usability. All statistical analyses were performed using SPSS version 16.0. 13
Results
Types and sources of donated medications
A total of 244 donations, amounting to 20,759 dosage units, were collected during the study period. Using the protocol (Figure 1), less than 2 h a day was required to sort the items by a trained pharmacy technician. Most medications (70.2%) were donated by patients (Table 1). Donations include medications from 10 different ATC classes. A majority of donated medications included agents acting on the alimentary tract and metabolism (35.7%), nervous system (30.0%) and cardiovascular system (17.4%).
Types and sources of donated medications.
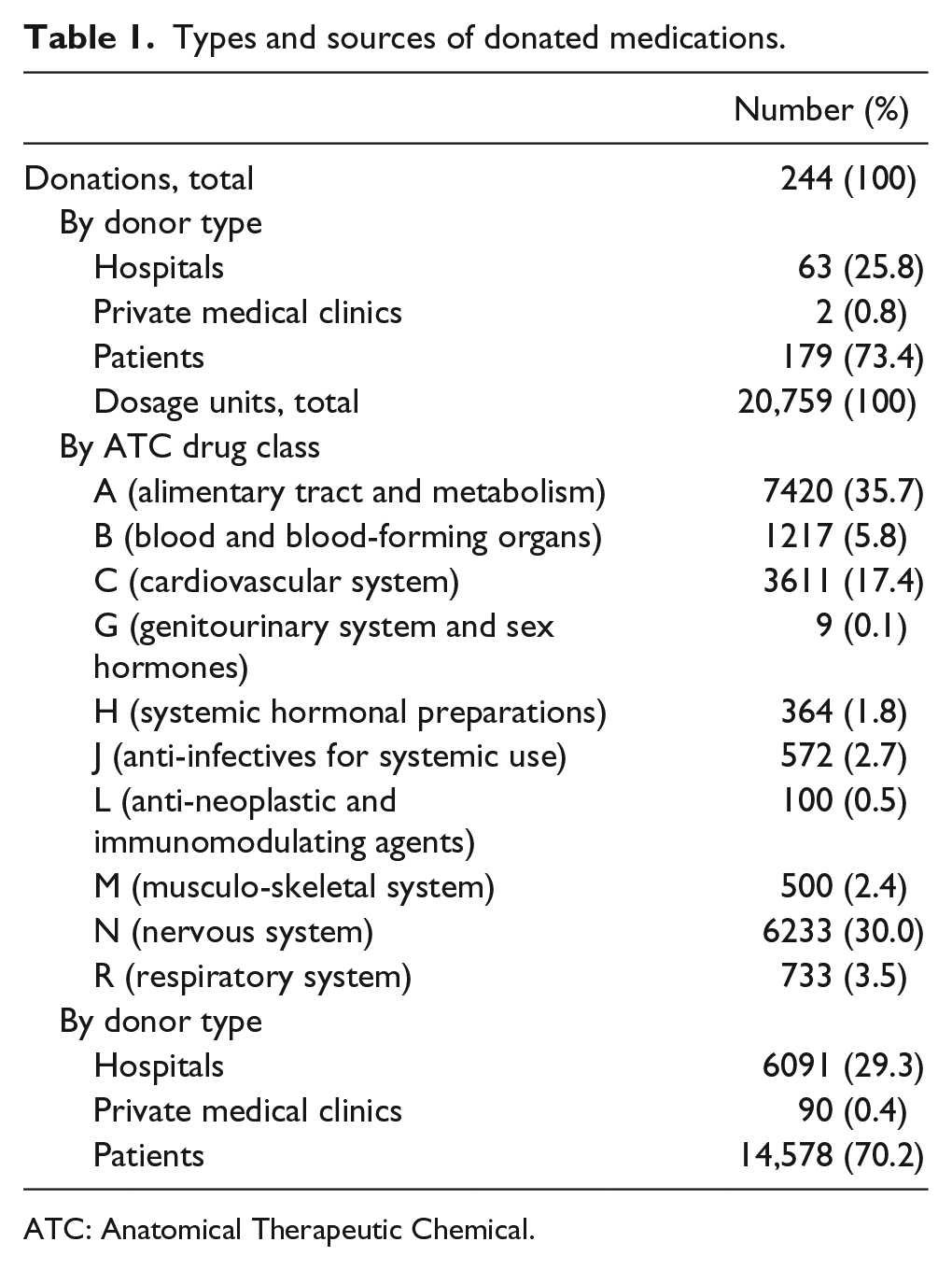
ATC: Anatomical Therapeutic Chemical.
Usability of donated medications
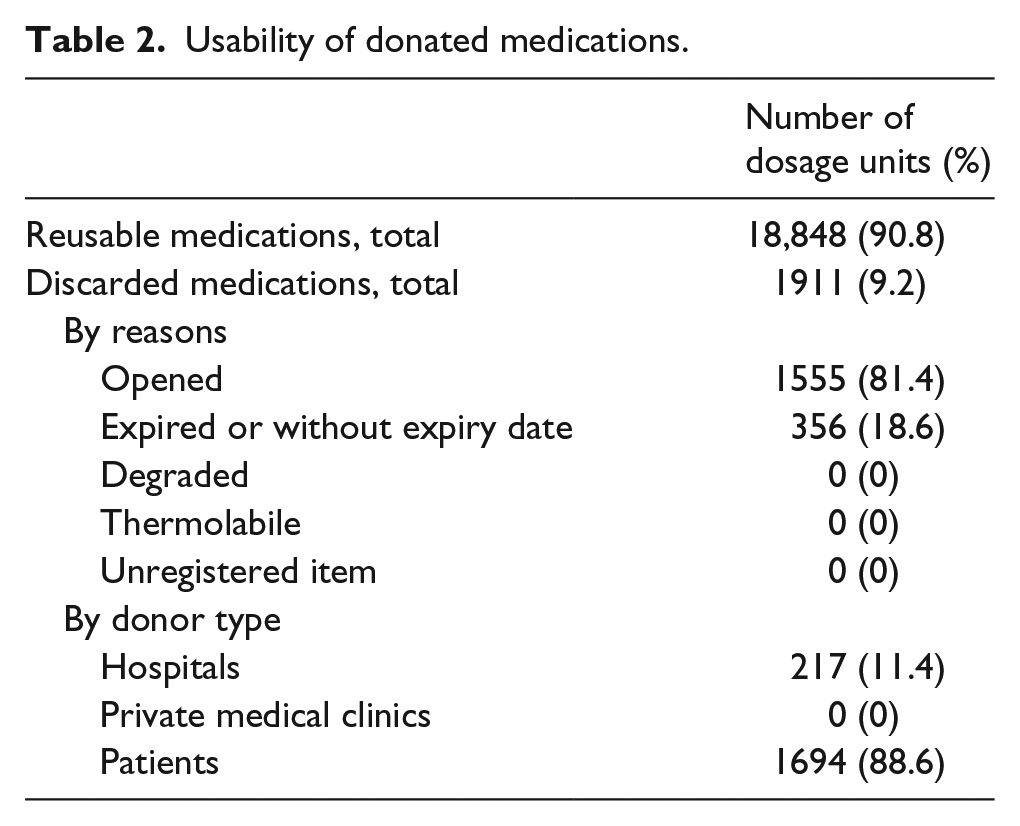
Most medications (90.8%) were suitable for redistribution (Table 2). Only 9.2% of the donated medications were discarded. Among these, 81.4% were opened and 18.6% were past the respective dates of expiry. Discarded donations from patients (88.6%) amounted to several times that of those from hospitals (11.4%). Overall, no medication was discarded due to physical degradation. No thermolabile or unregistered item was collected.
Usability of donated medications.
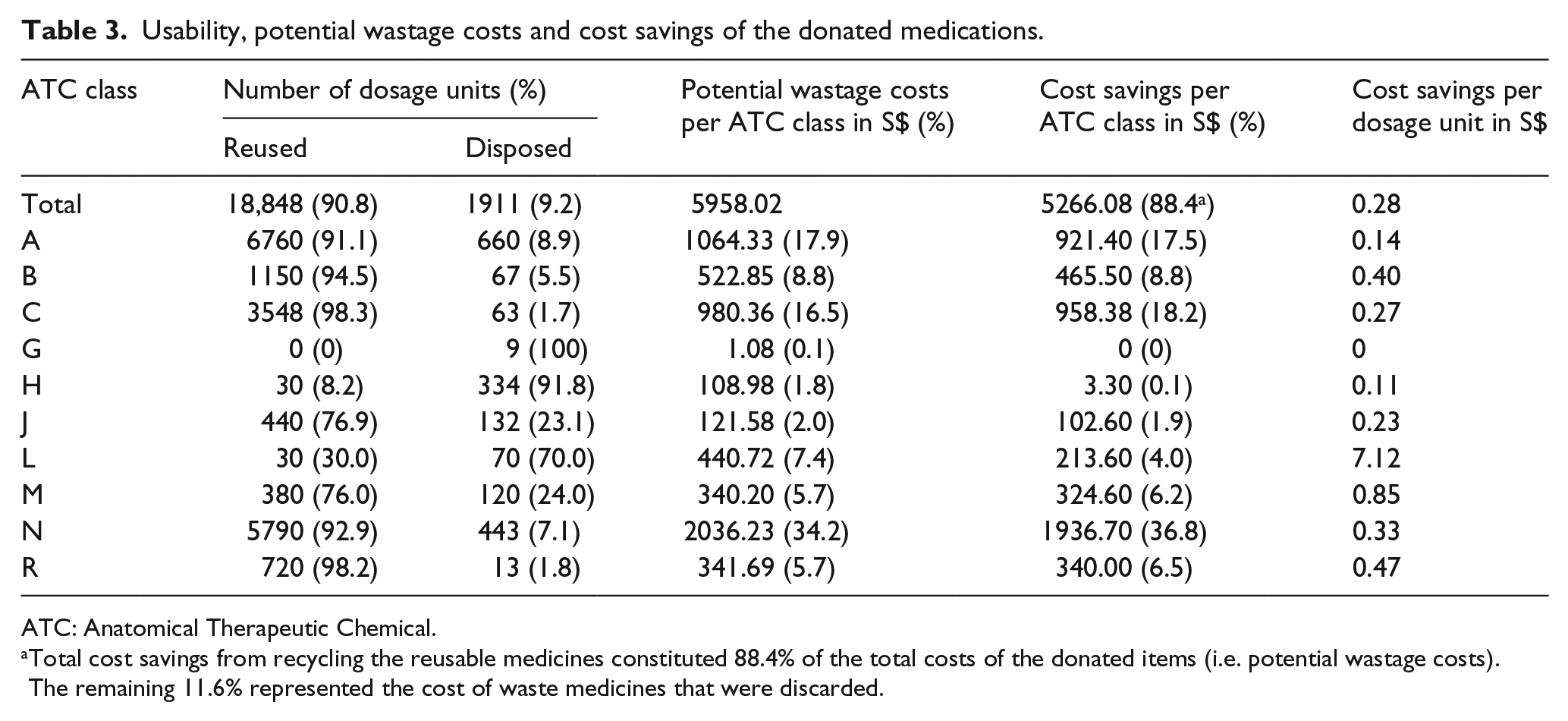
Reusability rates were the highest for medications belonging to ATC class C (98.3%), R (98.2%), B (94.5%), N (92.9%) and A (91.1%) (Table 3). On the other hand, less than half of the medications belonging to ATC class G (0.0%), H (8.2%) and L (30.0%) were reusable. The lower reusability rates of medicines from ATC class H and L when compared to class C were statistically significant (p < 0.005) while that of class G did not show statistical significance (p = 0.998) (Table 4).
Usability, potential wastage costs and cost savings of the donated medications.
ATC: Anatomical Therapeutic Chemical.
Total cost savings from recycling the reusable medicines constituted 88.4% of the total costs of the donated items (i.e. potential wastage costs). The remaining 11.6% represented the cost of waste medicines that were discarded.
Association between ATC class and medication reusability.
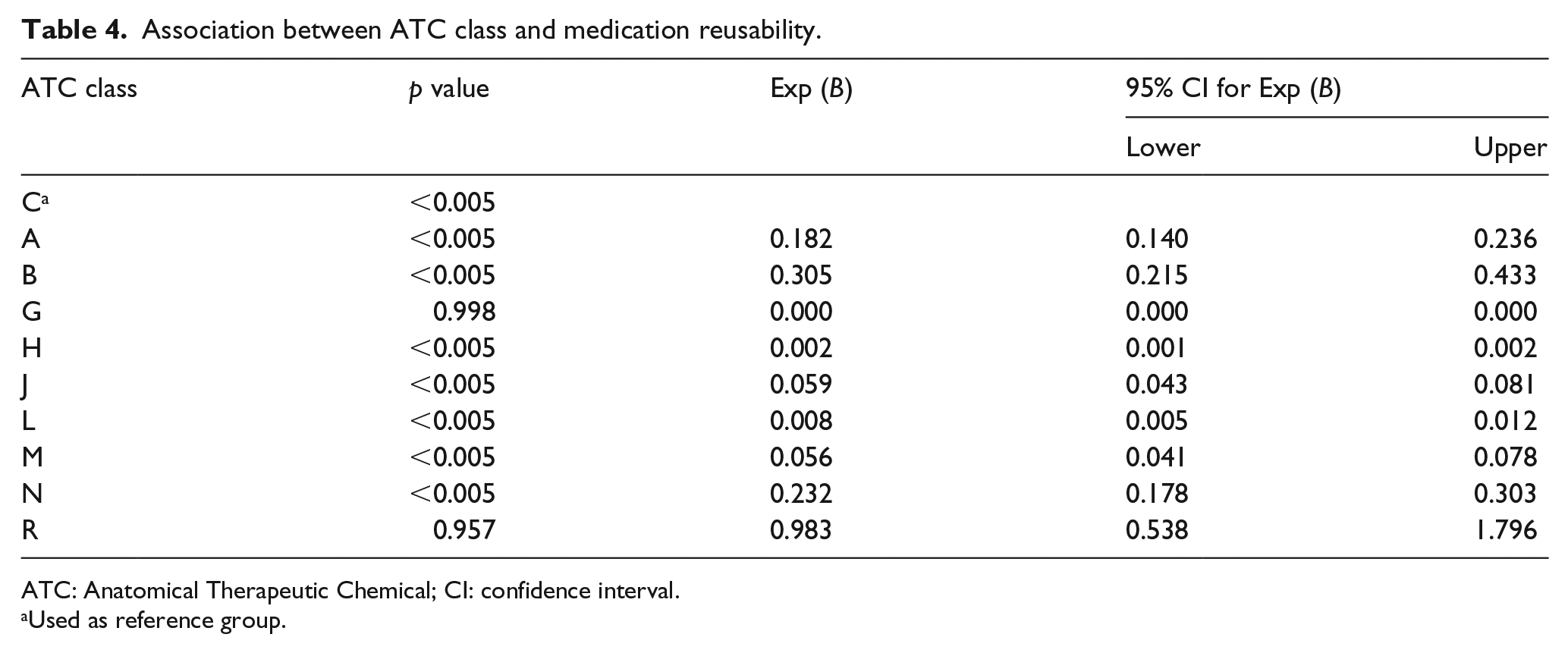
ATC: Anatomical Therapeutic Chemical; CI: confidence interval.
Used as reference group.
Cost savings of donated medications
All donated items cost a total of S$5958.02 and the reused donations provided cost savings of S$5266.08 (88.4%). Drugs belonging to ATC class N (36.8%), C (18.2%) and A (17.5%) contributed most to the overall cost savings (Table 3). Other classes contributed less than one-tenth of the total cost savings. Of note, ATC class L drugs contributed the highest cost savings per dosage unit (S$7.12 per unit) though it was one of the least reusable medicines. ATC class G and H drugs were the least reusable and provided the least cost savings.
Discussion
General findings
Within the period of 3 months at a single collection site, we have collected up to 20,759 dosage units. Over 90% of the donated items were redistributed, giving rise to S$5266 of cost savings.
Cost savings from medication recycling
Informal drug reuse practices are not uncommon in some hospitals, even where medication recycling has yet been accepted as the norm. 9 However, the actual cost savings attainable from these recycling programmes are not known. Figures available in the literature were mostly values predicted from medication return programmes rather than cost savings from actual implementation of medication recycling.4,8 Our findings help to shed some light on the actual quantity of reusable waste medicines and cost savings, demonstrating that medication recycling can be a valuable solution to reducing medicine wastage and healthcare expenditure.
Fundamentally, the intent of medication recycling is to redistribute the medications to those who cannot afford them. In the United States, almost 8% of adult patients did not take their medications as prescribed due to financial issues and there were 29 million persons of all ages who were uninsured.14,15 Many were thus noncompliant and suffered from avoidable disease progression and complications. 15 Most recycled medications were indicated for chronic conditions such as cardiovascular diseases, which are associated with serious and costly complications. Redistributing these medications to those who cannot afford the medications would facilitate better disease control and reduce complications, addressing one key area of avoidable cost (i.e. non-adherence) identified in the 2013 IMS report. 3
For publicly funded healthcare systems such as NHS, reusing the waste medicines is financially desirable and helps to optimise the use of medications. In the 2012 Action Plan put forth by the Steering Group on improving the use of medicines, medication recycling was not considered due to concerns over the integrity of medicines among other practical, technical and ethical factors which were not specified. 16 Of the 20,759 dosage units collected in this study, none was degraded and most were suitable for reuse. With proper checks for product integrity in place, medication recycling will be a useful addition to the existing waste reduction programmes in minimising unnecessary public spending.
With drug recycling, most of the waste medicines can be redistributed and 88.4% of the potential wastage costs could be converted into cost savings. However, the reusability of the donated item may vary depending on the donor source and ATC class.
Reusability and donor source
In the United States, several medication programmes would only accept drug donations from health facilities. 9 A main reason for the criterion was the general belief that donations from private individuals were more prone to tampering and poor storage conditions.9,17 Indeed, compared to patients’ donations, medications from healthcare facilities were generally in a better condition and almost thrice more likely to be reusable (odds ratio (OR) = 3.614, p < 0.005) (Table 5). In view of this, it may be wise to focus on recycling medications from healthcare facilities where there is an unbroken chain of accountability for the medicine. Medications in these facilities are always handled by healthcare workers, and the details of the medications’ movement are closely monitored – when they were purchased, for whom they were purchased and why they were not used.
Association between donor source and medication reusability.
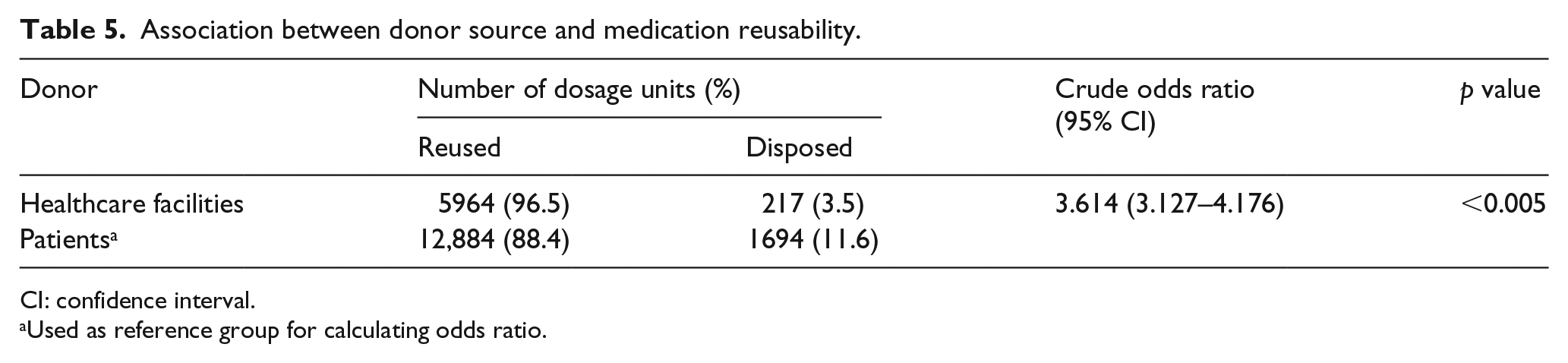
CI: confidence interval.
Used as reference group for calculating odds ratio.
Nonetheless, patients’ medications will still be a valuable source of donations given that the quantity of reusable dosage units from patients (n = 12,884) exceeded that from healthcare facilities (n = 5964) by more than twofold (Table 5). This source of waste medicines can be considered in medication recycling programmes in the future when such programmes have become more established and time-effective. Public education on the proper storage and prompt return of unused medicines will be needed to improve the reusability of patients’ waste medicines.
Reusability and drug class
Previous studies on return of waste medicine have consistently showed that medicines for the cardiovascular and central nervous system (CNS) were the two most frequently collected, ranging from 26.3% to 28.5% and 18.8% to 25.8%, respectively.4,8,14 In our study, most donated medications were for conditions related to the nervous system (30.0%), cardiovascular system (17.4%) and alimentary tract (35.7%). Collectively, these three classes were among the most reusable classes and provided more than 70% of the total cost savings from the recycling programme.
In comparison, medicines for ATC classes G, H and L were the least reusable and constituted less than 5% of the total cost savings. For class G, only nine tablets of phenazopyridine were collected. The lower reusability of class G was not statistically significant (p = 0.998) and probably not representative of the drug class (Table 4). It might still be worthwhile collecting and processing medications from this class. Donated items under class H included prednisolone, dexamethasone and hydrocortisone tablets. All the medicines except prednisolone were dispensed in amber bottles. Not surprising, all the hormonal tablets were discarded except the prednisolone tablets in the intact blister packs. In addition to the low reusability, this class provided the lowest cost savings per dosage unit (S$0.11). In comparison, the anti-neoplastic and immunomodulating agents (class L) provided the highest cost savings per dosage unit (S$7.12); a total of 30 capecitabine 500 mg tablets amounting more than S$200 were collected. Given the relative lack of generics in this class, donations from this class will still be valuable in spite of its low reusability.
Study limitations
This is a cross-sectional study involving a single collection site. The quantity, quality and type of donated medication may not be representative of unused medications in other non-hospice settings. Nonetheless, the most frequently returned drug classes in this study were similar to those of other studies based in the community setting.4,8,14 Future studies will be conducted on the other settings (e.g. primary healthcare institutes and hospitals) to validate the recycling protocol and the findings of this study. Another study limitation is that the reported cost savings might be an underestimation of the overall cost savings as the indirect cost savings to the healthcare system (e.g. reduced hospitalisations from better compliance and disease control) were not taken into account.
Conclusion
To date, many healthcare institutes remain divided on medication recycling. Objections largely revolve around the issues of patient safety and processing costs. While influential associations such as the American Medical Association and ASCP support the practice of medication recycling, there are no detailed guidelines on this practice. 6 Our protocol for medication recycling would be a useful scaffold for developing national guidelines. Given that the programme required less than 2 h/day of a pharmacy technician, we opine it is feasible to implement similar medication recycling programme and protocol. To further streamline the medication recycling process, we suggest focusing on donations from healthcare facilities and the higher yield drug classes (i.e. all the classes except class H). With a streamlined protocol and greater public awareness, medication recycling can be a safe and effective approach to reducing medication wastage.
Footnotes
Appendix
Acknowledgements
The authors thank Ms Tan Gek Lya Angela, Senior Manager (Nursing), and staff from HCA for their help in facilitating the collection and documentation of all donated drugs during the study period.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.