
Abstract
Background:
Distressing and potentially life-threatening events, such as significant external bleeding, may occur in patients with a known terminal condition. These events are often referred to as catastrophic or crisis events. Pharmacological management varies and there is little evidence to guide practice.
Aim:
The aim of this study was to explore Australasian palliative medicine doctors’ approaches to pre-emptive prescription of medications to manage catastrophic events.
Design:
Anonymous survey data were collected electronically.
Setting/Participants:
Australian and New Zealand palliative medicine fellows and trainees were surveyed.
Results:
Surveys were completed by 121 doctors; 108 (89.2%) who care for adult patients only and 13 (10.8%) who care for paediatric patients or paediatric and adult patients. In all, 74 (61.2%) respondents pre-emptively prescribed medications at least five times per year, and most orders were never administered. Significant visible bleeding and severe, acute airway obstruction were almost universally considered catastrophic events. Many respondents expressed concern about the lack of evidence to guide pre-emptive medication prescription in this setting. Clinicians reported adverse events related to pre-emptive medication orders being available (n = 30, 24.8%), as well as orders not being available (n = 61, 50.4%).
Conclusion:
Our study supports the need for guidelines, as well as formal education programmes for medical trainees and nursing staff about this important area of practice.
Distressing and potentially life-threatening events, such as significant external bleeding, may occur in patients with a known terminal condition. There is little evidence to guide pharmacological management.
Pre-emptive prescription for catastrophic events raises ethical concerns for many palliative medicine doctors, and pharmacological approaches vary. Many doctors worry about the lack of evidence and training to guide practice in this area.
Our study supports the need for standardised guidelines and education programmes for medical and nursing staff in this important area of practice.
Introduction
In palliative medicine, the term catastrophic event is used by some to denote an episode that is acute, potentially predictable and probably (but not always) terminal in a person with a known incurable condition. The terms ‘crisis’ and ‘emergency’ are also used to describe such events or associated symptoms.1–3 Catastrophic events may cause significant distress to the patient, family/carers and responding health professionals. The term catastrophic event is most commonly used in the context of significant, external bleeding and severe airway compromise and less commonly for severe, refractory pain and agitation.1–20 To mitigate the risk of patients suffering while awaiting medical review, doctors sometimes pre-emptively prescribe medications that can be administered by caregivers in such situations. Recommendations or reflections about the pharmacological management of catastrophic events in the palliative medicine setting can be found, at times buried, in the text of articles that discuss specific scenarios.6,8,9,11–15
The incidence of bleeding in patients with advanced cancer is low, but not negligible: significant or terminal bleeding occurs in an estimated 3%–14% of this patient population.6,9 The limited existing literature consistently highlights the need to remain present with and provide reassurance to the patient (and carers) and use dark towels to disguise blood; however, suggestions about pharmacological management vary.2,5,7–9,11,13,14,20 Some health professionals argue against the use of medications for terminal bleeding given that the patient is likely to die before medications have a chance to be effective. 10 Austin Health in Australia, as well as the Scottish and Yorkshire palliative medicine guidelines, provides clear advice about palliative medicine emergencies such as terminal bleeding, albeit with some differences in starting doses, route and interval between doses.16,18,19
Most guidelines cite rapid sedation and amnesia (in the case of survival) as the goals of medication administration, and some suggest that medications provide families or nurses with something meaningful to do in a distressing situation. 8 Few guidelines specifically highlight that the intent is not to hasten death.1,9 Uncertainty about whether the event will resolve, and how long the patient may live, influence how clinicians prescribe in this setting.
Principles and protocols for pain management and terminal restlessness/delirium are covered in palliative medicine guidelines and texts.1,2,5,21,22 In the few guidelines that refer to intractable pain as a crisis requiring emergency intervention, opioids are the mainstay of treatment; some guidelines recommend a reduced interval between doses and others recommend adjuvant medications such as ketamine.2,3,21
The study authors hypothesise that attitudes and practices in this area vary. The aim of this study was to explore and document local palliative medicine doctors’ attitudes and practices in pre-emptive medication prescription for the management of potential catastrophic events in patients with a terminal illness.
Methods
The study was conducted by adult and paediatric palliative medicine specialists in Melbourne, Australia. A survey including both closed- and open-ended questions (Appendix 1) was distributed through the Royal Australasian College of Physicians Chapter of Palliative Medicine (RACP ChPM), the Australian and New Zealand Palliative Medicine Society (ANZSPM) and the Victorian Palliative Medicine Training Programme (VPMTP) with the aim of reaching doctors working in the field of palliative medicine.
The secure database, REDCap, was used to design and distribute surveys. The survey consisted of 20 questions with branch logic to allow additional details depending on respondents’ answers and took approximately 10–15 min to complete. The survey enquired about personal experience with pre-emptive medication prescription for potential catastrophic events, prescription practices and ethical or other concerns.
The authors anticipated the potential for ethical issues to arise from information disclosed about medication prescriptions and intent. This was discussed with the Research Governance and Ethics Committee and thought to add further value to the study. Surveys were sent out via a public survey link and responses were anonymous and non-identifiable. Consent was required for respondents to progress through the survey. Survey data were collected between May 2017 and January 2018. Descriptive statistics were utilised to summarise and present findings. Ethics approval was obtained through the Royal Children’s Hospital, Melbourne, Australia (HREC 37053A).
At the time of initial survey distribution, 397 fellows and 140 trainees were registered with the Chapter of Palliative Medicine.
Results
Clinician characteristics
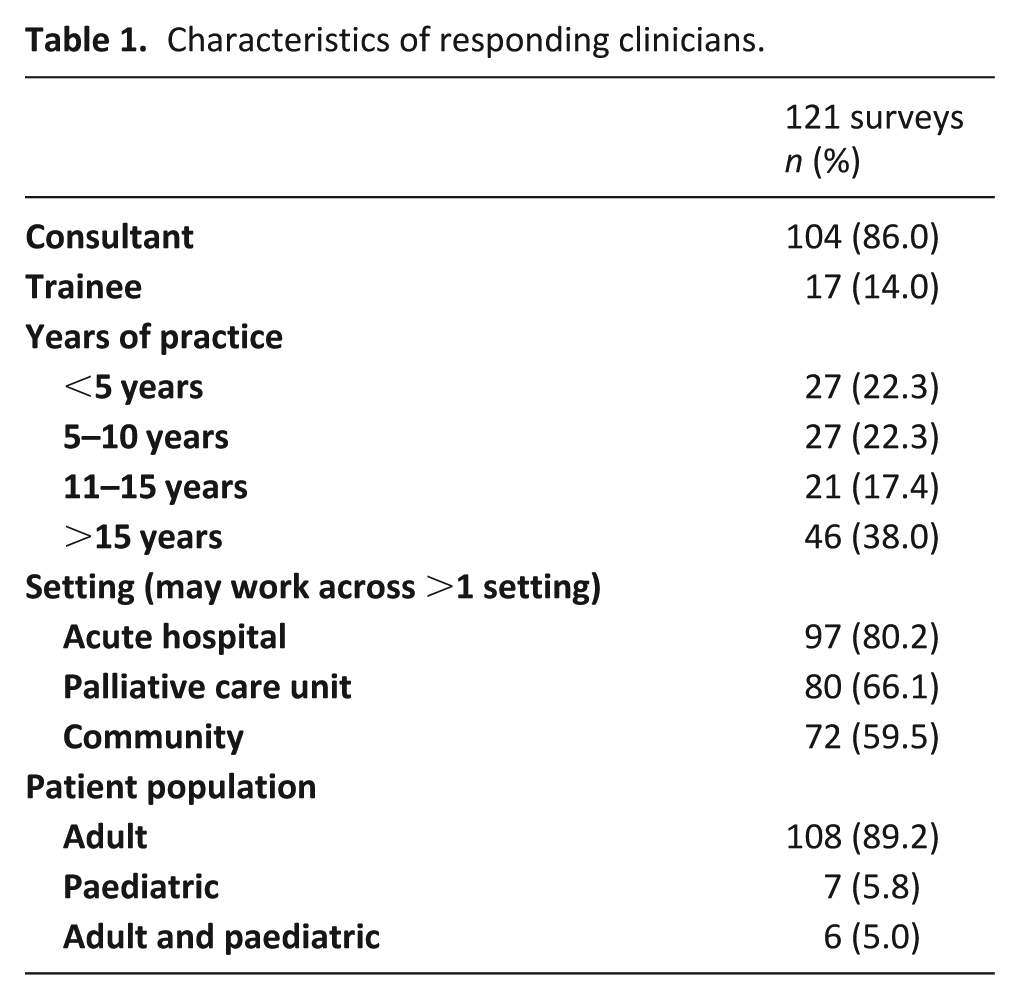
A total of 121 surveys were included in data analysis, giving an estimated response rate of 22.5%. Of these, 114 (94.2%) were completed in entirety. More than half the surveys were completed by clinicians with at least 10 years of experience in palliative medicine (Table 1). Most responding clinicians see only adult patients, and many (n = 47, 38.8%) work across the acute hospital, palliative care unit (PCU) and community settings (Table 1).
Characteristics of responding clinicians.
Terminology
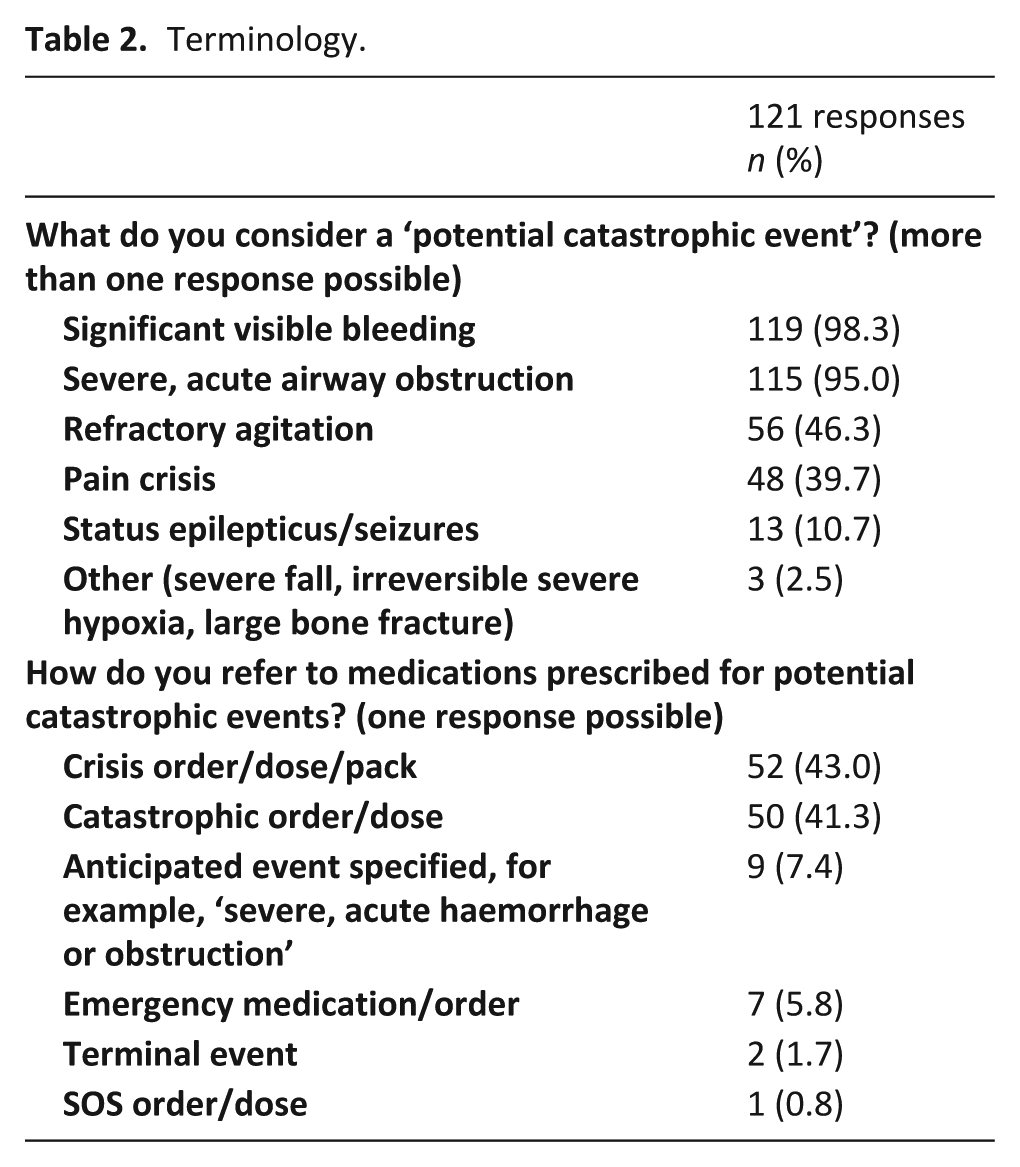
Significant visible bleeding and severe, acute airway obstruction were almost universally considered catastrophic events, and pre-emptively prescribed medications in such settings were most commonly referred to as crisis or catastrophic event orders (Table 2). Some clinicians commented that they specify the anticipated event or use the word ‘terminal’ in the medication order.
Terminology.
Prescribing practice
All clinicians who responded had pre-emptively prescribed medications for a potential catastrophic event on at least one occasion. More than half of the responding clinicians (n = 74, 61.2%) prescribed in this setting at least five times per year, but most orders were never administered (Table 3). Several clinicians elaborated that an estimated ~5%–10% of medications ordered were administered.
Prescribing practice.
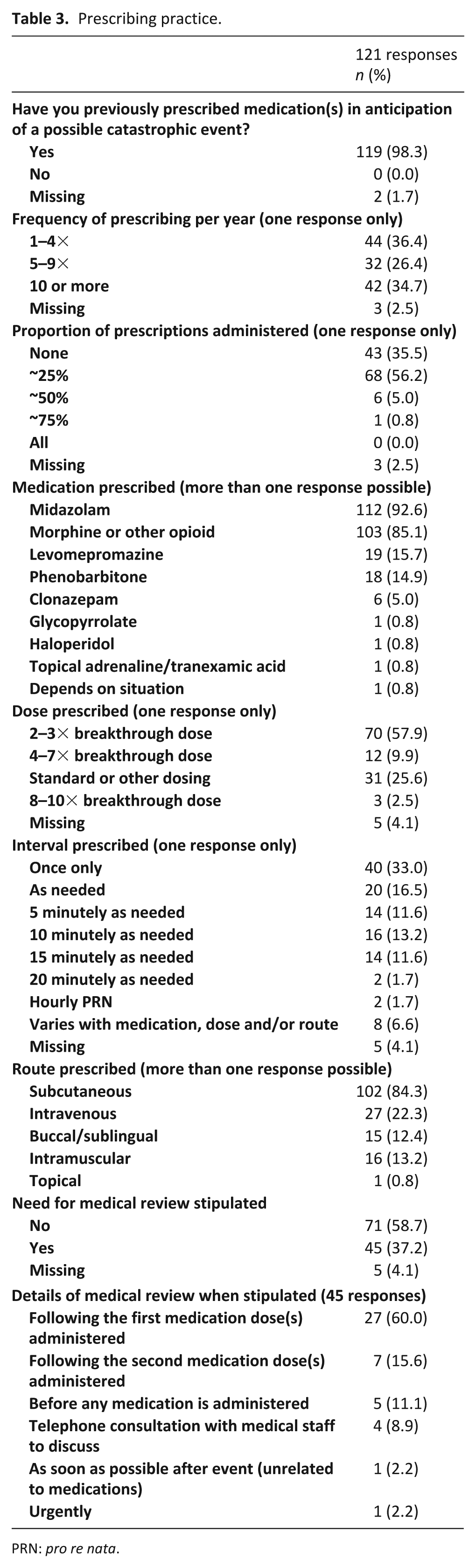
PRN: pro re nata.
Closed- and free-text responses about medication prescription were collected; details about medication doses, interval and route of prescription, as well as stipulation about medical review, are shown in Table 3. In all, 10 (8.3%) clinicians specifically commented that they consider liver and kidney function and/or tolerance to medications. The most common ‘standard’ doses reported were 10 mg of morphine and 10 mg of midazolam; however, ranges of 5–20 mg of midazolam and 10–38 mg of morphine were reported. In all, 10 (8.3%) clinicians reported that their orders allowed for a maximum of two or three doses. Some clinicians described medication dosing being challenging, for example, ‘I do this so infrequently I do not have a system’ and ‘It is impossible to know and this is why I further question this practice. I usually just ensure there is normal SC (subcutaneous)/IM (intramuscular) dose available’.
Medications were most frequently prescribed with the aim to relieve patient distress (n = 112, 92.6%). Minimising patient consciousness (n = 56, 46.3%) and providing nursing staff/carers with something to do (n = 45, 37.2%) were also common indications. Some clinicians use anticipatory prescribing as a teaching tool or prompt for advance care planning discussions with health professionals or patients and families.
Training sources
The vast majority of clinicians (n = 107, 88.4%) identified senior colleagues as their source of training in this area. Written guidelines (n = 29, 24.0%), textbooks (n = 17, 14.0%), peer-reviewed papers (n = 14, 11.6%), personal experience (n = 3, 2.5%), conferences (n = 1, 0.8%) and local consensus (n = 1, 0.8%) were alternative sources of information.
Challenges and concerns about this area of practice
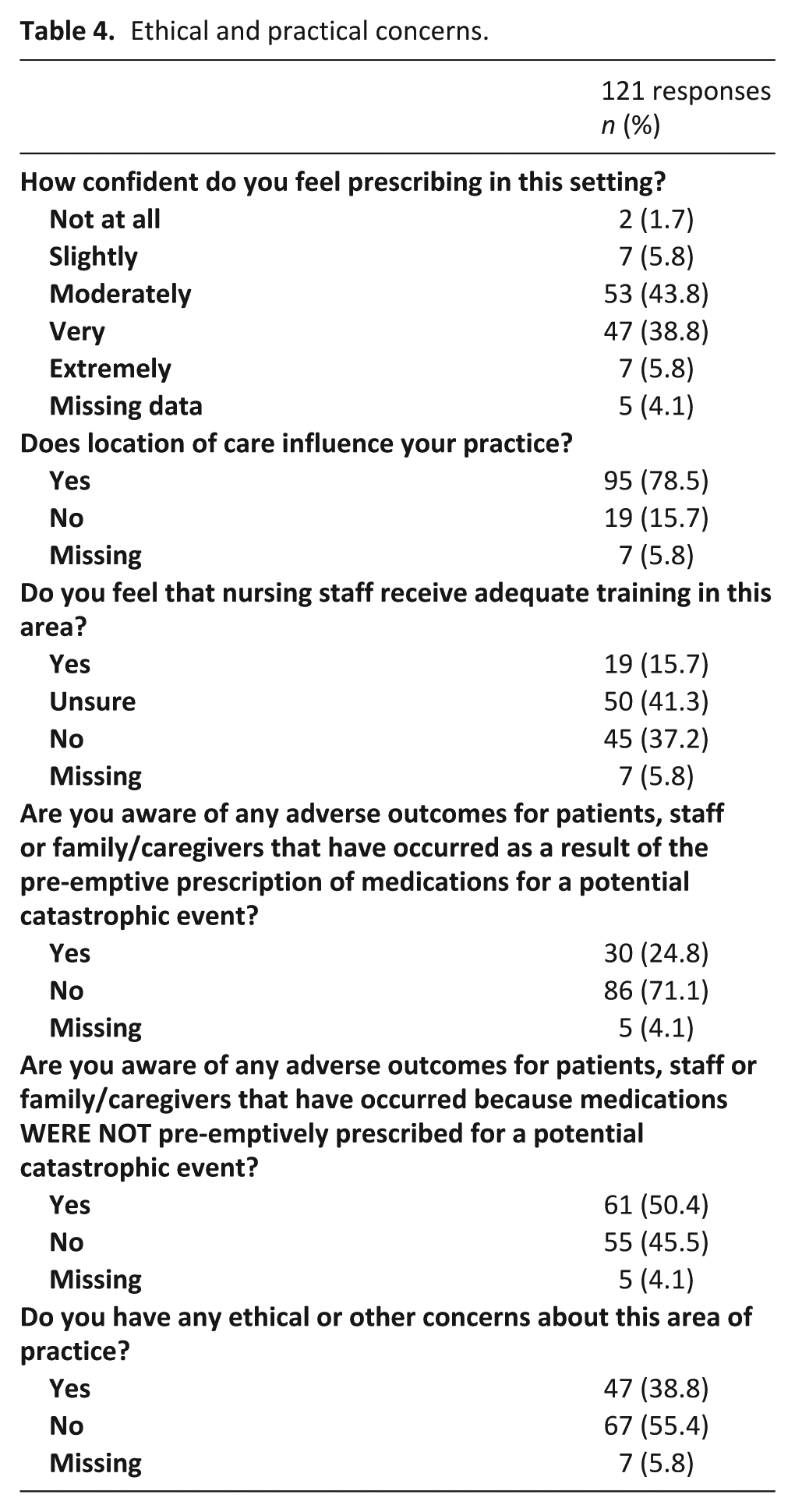
Most clinicians reported that patient location influenced their prescribing practice, taking into consideration the expertise of responding staff, as well as available routes for medication administration (Table 4). Clinicians with more than 10 years of experience were more likely to feel very or extremely confident with pre-emptive prescription of medications for catastrophic events than clinicians with under 10 years of experience (n = 35 (52.2%) versus n = 19 (35.2%)). Only 19 (15.7%) clinicians felt that nursing staff receive adequate training in this area, and all doctors who felt that nursing staff do not receive adequate training shared that this affects whether they prescribe in this setting. Almost a quarter of clinicians reported being aware of adverse outcomes due to medications being prescribed for potential catastrophic events, including one which resulted in policy change regarding stipulation of medical review (Table 4). Half of the responding clinicians were aware of adverse events related to medications not being prescribed (Table 4). Many clinicians reflected on a lack of evidence, a need for dedicated education for junior doctors and nursing staff, and a desire for further studies and standardised approaches to support clinicians in this area of practice.
Ethical and practical concerns.
A number of concerns about orders being pre-emptively prescribed were raised. First, discussing an unlikely event may cause disproportionate and often unnecessary anxiety: ‘Warning patients of a possible event (which probably won’t happen) can cause them to experience significant distress’. Second, it can be challenging to know when to administer medications: ‘My concern is about writing an order and leaving it to someone else to make the call that this is actually a catastrophic event. I have seen it being used inappropriately for an asymptomatic GI (gastro-intestinal) bleed’. In addition, medications may detract from non-pharmacological management, ‘I think these orders are overprescribed … and distract staff and carers from valuable activities around calm presence, reassurance, loving touch’. Finally, health professionals/carers who administer these medications may feel ‘… responsibility for the outcome’.
Clinicians also described how a lack of medication prescription and availability may lead to inadequate symptom control and unrelieved distress for patients and carers. For example, one clinician described that ‘A patient with a head and neck cancer was discharged home from hospice without any subcut midazolam for a catastrophic haemorrhage. He died, from carotid haemorrhage, in distress, in an ambulance’. The potential for subsequent difficult bereavement was also raised: ‘Perceived bad dying/staff distress, carer bereavement issues – which would have been avoidable.’
Discussion
Our study did not specifically seek to evaluate medication efficacy, but rather to explore practice and attitudes of local palliative medicine doctors in this field of practice. Survey responses supported our hypothesis that approaches and attitudes vary and that this area of practice evokes strong reactions and raises ethical concerns for many clinicians.1,2,5,8,11,13,14,20
Not surprisingly, significant visible bleeding and severe, acute airway obstruction were almost universally considered ‘catastrophic’ events, but many clinicians also referenced refractory agitation and pain crises. Refractory agitation or pain may require different approaches to acute external haemorrhage or upper airway obstruction. The terms ‘catastrophic’ and ‘crisis’ orders are most commonly used to denote medications prescribed in this setting, but alternative terms such as ‘emergency’ orders may be used. The study highlighted the potential for language to be ambiguous and lead to miscommunication and even error: for example, ‘Emergency Medication Kits’ (EMKs) may refer to ‘standard’ palliative care medication supplies in the home 23 or to medications for use in the event of a catastrophic event. Given that patients are cared for by different services and clinicians over the course of their illness, consistent language is vital to minimise errors.
Although often not ultimately administered, the prevalence of pre-emptive medication prescription in anticipation of a catastrophic event or symptom was high in our study. Benzodiazepines and opioids were by far the most commonly prescribed medications, but there was variability in the dose, route and interval of medication prescription. This is consistent with the variability in existing literature and guidelines.2,5,7–9,11,13,14,16,18,19 Responses highlighted various factors that may contribute to variability in medication prescription, including site of care, route of administration and concern about absorption, medication tolerance and timing and availability of medical review. Incorporating such considerations into consensus guidelines and education is likely to be helpful for clinicians and enhance patient care and safety.
While minimisation of patient distress was the most common reason for responding clinicians to prescribe in this setting, over a third felt that medications provide carers with ‘something to do’. Providing ‘something to do’, however, may result in focus on drawing up medications and must be weighed up against the risk of leaving a distressed, and possibly dying, patient alone. 10 Furthermore, as described by Bidet et al., 24 there is a potential for medications to be administered for an indication other than that intended by the prescriber.
It was not surprising that most clinicians identified senior colleagues, rather than formal training, as their source of knowledge in this area of practice. We were struck by clinicians’ concern about the lack of evidence and standardised approaches to guide practice for both medical and nursing staff in this area. The issue is complex: distress may arise when medication orders are available, and when medication orders are not available, and both elements would need to be incorporated into education and standardised approaches. While there is unlikely to ever be a randomised controlled trial in this area of practice, retrospective or prospective cohort studies would strengthen the literature. Studies suggest that established protocols improve patient care by minimising room for individual clinician opinion.25,26 This could be done in collaboration with other professional groups who encounter such scenarios, such as Ear, Nose and Throat (ENT) and Oncology. Standardised guidelines would provide a framework for clinical practice and could be incorporated into formal training and education programmes for medical and nursing staff.
This is a high-stake area of practice with potential for significant patient, carer and health professional distress, both from the catastrophic event itself and related to the use of medications to manage the catastrophic event. Doctors prescribe, carers or nurses administer, patients are given medications and family members bear witness. Good communication and trust are vital for everyone to feel comfortable and supported in their role. In our study, participating doctors’ prescribing practice is influenced by their perception of nursing experience and training, but nursing autonomy is important too. 24 Our study adds weight to the value of standardised guidelines, formal education for junior medical and nursing staff and good communication between doctors who prescribe and nurses who administer these medications. 27
Strengths and limitations
To the best of our knowledge, this is the first peer-reviewed study to explore practices of palliative medicine doctors across various ‘catastrophic’ events in the end-of-life setting. Our study only surveyed palliative medicine doctors, and future studies should include clinicians in other disciplines and fields, for example, nurses, radiation and medical oncologists and ENT specialists. While valuable to have paediatric palliative medicine specialists’ input, the relatively small sample size is a limitation. In addition, we acknowledge that surveys may have been completed more than once as an open survey link was necessary for anonymous responses although we think this is unlikely. Finally, selection and non-response bias may be an issue. Doctors who are particularly interested in this area of practice may have been more likely to respond, perhaps because of experience with adverse events. Non-response may have been related to a number of factors, for example, clinicians being time poor or having practices and opinions that they preferred not to share despite the survey being anonymous.
Conclusion
Palliative medicine specialists vary in their attitudes and prescribing practice for potential catastrophic events in terminally ill patients. Both presence and absence of medication availability in a catastrophic event may lead to significant distress for health professionals, patients and carers. Our study supports the need for standardised language and guidelines, as well as formal education programmes for medical trainees and nursing staff about this important area of practice.
Footnotes
Appendix 1
Acknowledgements
N.T.K. and B.H.S. conceived and designed the study. All authors contributed to the survey design. N.T.K. managed the survey responses, analysed the data and drafted the manuscript, and J.L.H., B.H.S. and B.H.L. critically reviewed and approved the manuscript for publication. All authors participated sufficiently and agreed to be accountable for the work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.