
Abstract
Background:
Pressure ulcers are associated with significant morbidity and mortality as well as high cost to the health service. Although often linked with inadequate care, in some patients, they may be unavoidable.
Aim:
This systematic review aims to quantify the prevalence and incidence of pressure ulcers in patients receiving palliative care and identify the risk factors for pressure ulcer development in these patients as well as the temporal relationship between pressure ulcer development and death.
Design:
The systematic review is registered in the PROSPERO database (CRD42017078211) and conducted in accordance with the ‘PRISMA’ pro forma. Articles were reviewed by two independent authors.
Data sources:
MEDLINE (1946–22 September 2017), EMBASE (1996–22 September 2017), CINAHL (1937–22 September 2017) and Cochrane Library databases were searched. In all, 1037 articles were identified and 12 selected for analysis based on pre-defined inclusion and exclusion criteria.
Results:
Overall pressure ulcer prevalence and incidence were found to be 12.4% and 11.7%, respectively. The most frequently identified risk factors were decreased mobility, increased age, high Waterlow score and long duration of stay.
Conclusion:
The prevalence of pressure ulcers is higher in patients receiving palliative care than the general population. While this should not be an excuse for poor care, it does not necessarily mean that inadequate care has been provided. Skin failure, as with other organ failures, may be an inevitable part of the dying process for some patients.
A range of skin changes occurring at the end of life have been described in the literature.
Based on the findings of this systematic review, pressure ulcers may be more common in patients receiving palliative care compared with the general population.
Pressure ulcer prevalence may be higher in palliative care patients in nursing homes compared to those in inpatient or other community settings.
It may be necessary to re-evaluate the appropriateness of including palliative patients in reporting systems that record pressure ulcer formation as healthcare-associated harm.
Failure to recognise this as an issue has the potential to seriously damage reputations of individuals and organisations alike as currently any pressure damage is viewed as a failure of care, and for stage 3 and 4 injuries is often viewed as neglect.
Introduction
Pressure ulcers (also referred to as pressure sores, bed sores and pressure injuries) are defined as ‘localised injury to the skin and/or underlying tissue usually over a bony prominence, as a result of pressure, or pressure in combination with shear’. 1 The recorded incidence and prevalence of these wounds varies throughout the literature and is particularly poorly documented for patients in community rather than inpatient settings. For patients in hospital, the reported prevalence is 3%–14%, but can be as high as 70% in some patient groups. 2 The most common body areas affected by pressure damage are the sacrum (28%–36%), heel (23%–30%) and ischium (17%–20%). 3 Pressure ulcers are associated with significant morbidity and mortality, causing pain and distress to patients both physically and psychosocially. The financial cost to the health service is estimated at £4300–£6400 per patient. 4
Over recent years in the United Kingdom, there has been an increased public awareness of pressure ulcers and the problems they lead to, thanks to greater media attention and campaigns such as ‘1000 lives’. 5 In 2015, the National Institute of Health and Clinical Excellence (NICE) stated that pressure ulcers are ‘often preventable’. 6 The Welsh Government refer to ‘avoidable’ pressure ulcers as those developing in individuals receiving care but who’s caregiver did not evaluate the person’s clinical condition and pressure ulcer risk factors; plan and implement interventions that are consistent with the person’s needs and goals and recognised standards of practice; monitor and evaluate the impact of the interventions; or revise the interventions as appropriate. 7
This is particularly important in the current climate, where pressure ulcers are recorded as patient safety incidents and have often been linked with inadequate care.
It is well accepted that organ failure, such as heart or kidney failure, towards the end of life is often a pre-terminal event, but skin failure is less widely accepted as a phenomenon. In 1989, Karen Kennedy coined the term ‘Kennedy terminal ulcer’ for pressure areas developing over bony prominences in the days preceding death. 8 The concept of skin failure has been discussed in the literature as a state of compromised tissue integrity affecting skin cell survival in times of physiologic stress such as hypoxia, deficiency of nutrients, mechanical stress or toxins. 9 A number of reasons for impaired healing in critical illnesses have been suggested, any of which may be present at the end of life. 10 Respiratory failure impairs gas exchange and oxygen absorption which may impact healing, whereas hepatic or renal failure can affect waste product removal, protein retention, acid base balance and tissue oedema. Poor nutrition has long been recognised as a risk factor for the development or non-healing of wounds, with some evidence suggesting artificial nutrition can improve outcomes in pressure ulcers. 11 Langemo 12 also highlighted a number of risk factors for pressure ulcers that may be present towards the end of life, for example, reduced mobility due to a combination of frailty, pain and sedation from medication which subsequently leads to tissue ischaemia from pressure. Other factors include lower blood pressure and haemoglobin, and the possibility of increased moisture on the skin secondary to sweat, exudate, urine or faeces. However, the degree to which these factors impact on patients at the end of their life compared with their non-palliative counterparts is not clear. In addition, the approach to managing wounds in palliative patients may need adjustment to prioritise comfort, which may occur at the expense of ‘gold standard’ wound care with a curative aim, for example, dressing regimes may be less frequent to limit discomfort or medical contact, repositioning may be limited due to pain, or patients may need to be nursed at greater than 30° to manage dyspnoea, accepting that this may increase shear and pressure on the buttocks.
Expert panels have produced guidelines and consensus documents discussing skin changes and pressure ulcers in patients at the end of their life.8,13 While it is accepted that healing pressure ulcers in patients receiving palliative care is unlikely, both committees highlight the need for further work looking at risk factors, treatment options and prognosis in this group of patients. A preliminary search of the Joanna Briggs Institute database of systematic reviews, the Cochrane database and Prospero database found a number of reviews evaluating various treatments, preventive strategies and risk assessment tools for patients receiving palliative care with pressure ulcers. We did not identify any systematic reviews either completed or in progress looking at whether pressure ulcers in patients at the end of their life could be avoided or are inevitable. If skin failure/terminal pressure ulcers are indeed a common occurrence in patients going through the dying process, this may also have wider implications for the healthcare community, not only in terms of risk assessment and treatment choice but also in terms of quality outcome measurement, litigation and liability.
This systematic review aims to assess the available evidence for any association between the development of pressure ulcers and the terminal phase of illness in those patients receiving palliative care to help inform discussions around appropriate end of life care and protection of the skin and soft tissues. We aim to address the following key questions: What is the prevalence and incidence of pressure ulcers and is this consistent with the wider patient population? What particular risk factors increase the risk of pressure ulcer development? What is the temporal relationship between pressure ulcer development and death in those receiving palliative care?
Methods
Protocol and registration
The protocol for this systematic review was registered with the PROSPERO database, the international prospective register of systematic reviews (ID CRD42017078211) and followed the ‘Preferred Reporting Items for Systematic Reviews and Meta-Analyses (“PRISMA”) pro forma’ (see Figure 1).
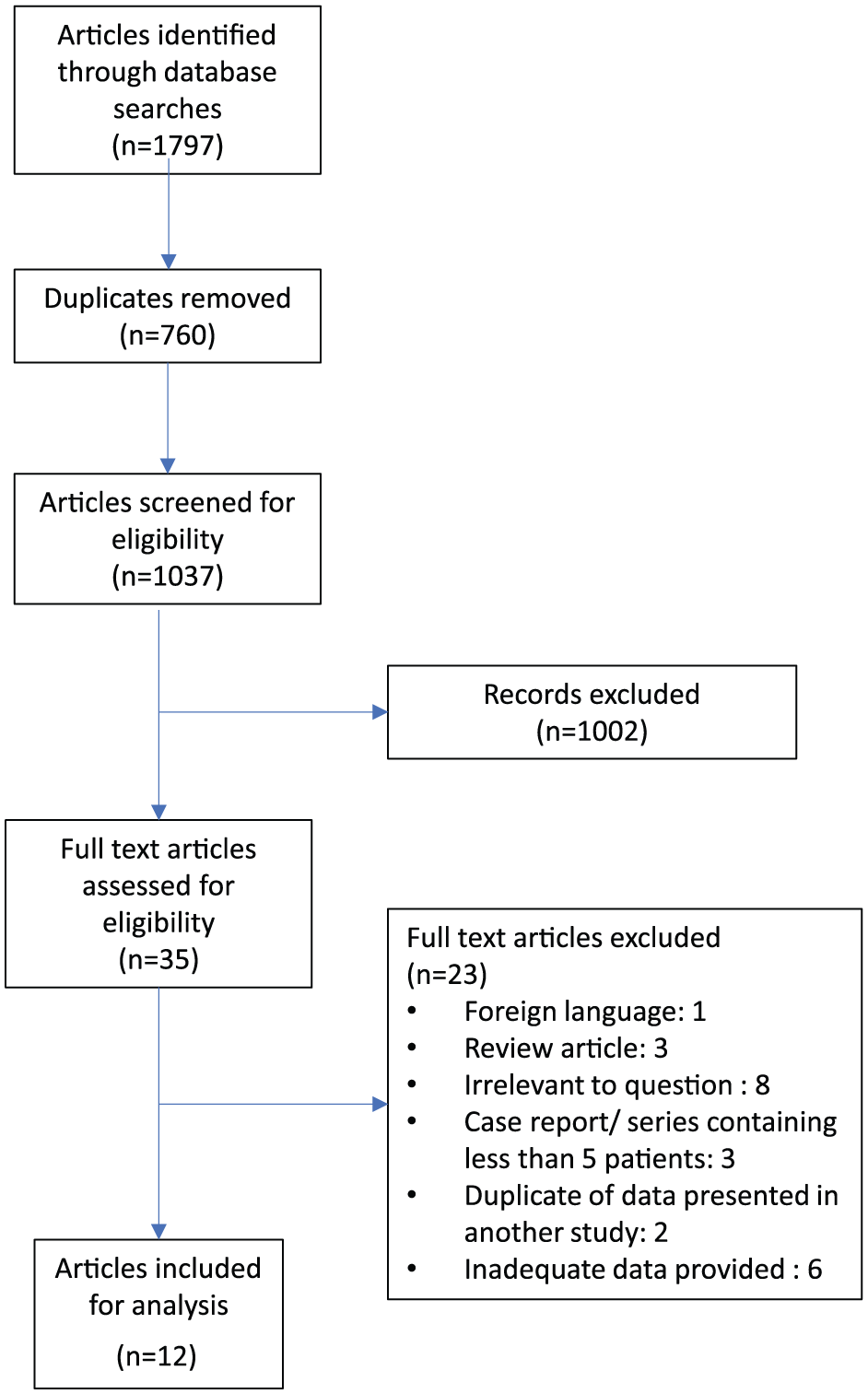
PRISMA diagram demonstrating article selection process.
Search strategy
The databases searched were MEDLINE (1946–22 September 2017), EMBASE (1996–22 September 2017), CINAHL (1937–22 September 2017) and the Cochrane Library. The search was up to date as of September 2017. The search terms were split into two categories (one relating to pressure ulcers and another relating to dying) and combined using the ‘AND’ function to identify appropriate papers. Variations on the search terms in each category were combined using ‘OR’ (see Appendix 1). Reference lists of articles identified for full text review were also searched for any appropriate papers not identified in the initial search.
Eligibility criteria
This systematic review included original articles written in English looking at patients receiving palliative care and identified as having pressure ulcers, looked after in community and inpatient settings. Types of articles included were experimental and epidemiological studies including randomised control trials, non-randomised control trials, cohort studies, case control studies and descriptive evidence such as audits and case series published at any time up until the review start date of September 2017. Review and commentary articles, meta-analyses and consensus documents were excluded, as were any case series describing fewer than five cases or with very little or poor-quality data. Articles were also excluded if they were found to be unrelated to the terminal phase of illness or described wounds other than pressure ulcers.
Study selection
Studies identified in each database search were compiled before removing duplicates. Two authors (A.F. and A.P.) independently screened the identified articles for relevance from their title and abstract, based on the inclusion and exclusion criteria. Articles identified for full text review were then assessed again based on the described criteria. If the two reviewers were unable to reach an agreement for inclusion/exclusion of a particular study, a third reviewer was available to resolve this; however, this was not required.
Data extraction and analysis
Data were extracted independently by the two reviewers and compiled into a Microsoft® Excel spreadsheet for analysis. Data extracted included study type and setting, number of patients, cancer/non-cancer diagnosis, site of pressure ulcer, prevalence and incidence of pressure ulcer, time to formation of pressure ulcer, and time between pressure ulcer development and death. Data were also collected on the risk factors associated with pressure ulcer formation. Where possible, data were pooled for further analysis; however, not all articles included data on all of the measures listed above. For data with a p-value provided, we have only included the results for factors found to be statistically significant (p < 0.05).
Analysis of bias
Due to the observational nature of the data and heterogeneity of methodologies, it will not be possible to perform conventional bias analysis such as through the use of funnel plots. Instead, we will tabulate study limitations that may introduce bias for each paper to enable readers to understand the likely confounding factors.
Results
The database search identified -1037 articles and no additional papers were identified from the reference lists. After screening, 35 articles underwent full text review and based on the inclusion and exclusion criteria, 12 articles with a total of 63,907 patients were subsequently selected for analysis following the PRISMA protocol (see Figure 1). The types of study included were retrospective cohort studies (n = 5), prospective cohort studies (n = 4), retrospective case control studies (n = 2) and audit (n = 1).
Demographics
The 12 articles included for analysis are summarised in Table 1. Of the 12 articles, 10 included data on average patient age, which ranged from 63 to 82 years (mean 72 years).
Summary of the included studies, the prevalence and incidence of pressure ulcers, and any risk factors identified.
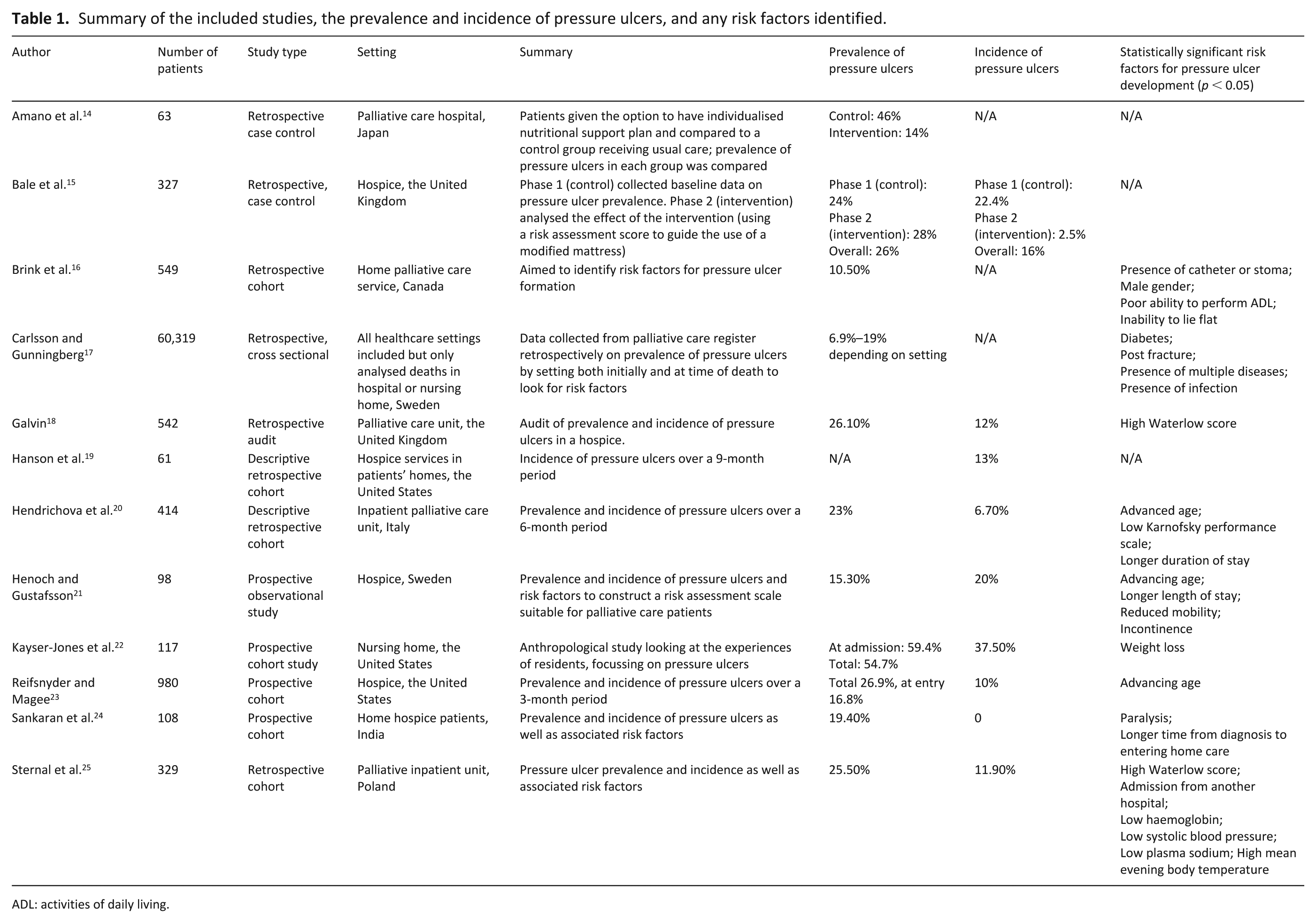
ADL: activities of daily living.
The majority of studies did not define what they meant by ‘palliative’; four studies were restricted to patients receiving palliative care with an underlying diagnosis of cancer and eight included patients receiving palliative care in the terminal phase of any illness. The settings included inpatient/hospice palliative care providers (n = 8), community only (n = 3) and inpatient and community combined (n = 1).
Prevalence and incidence
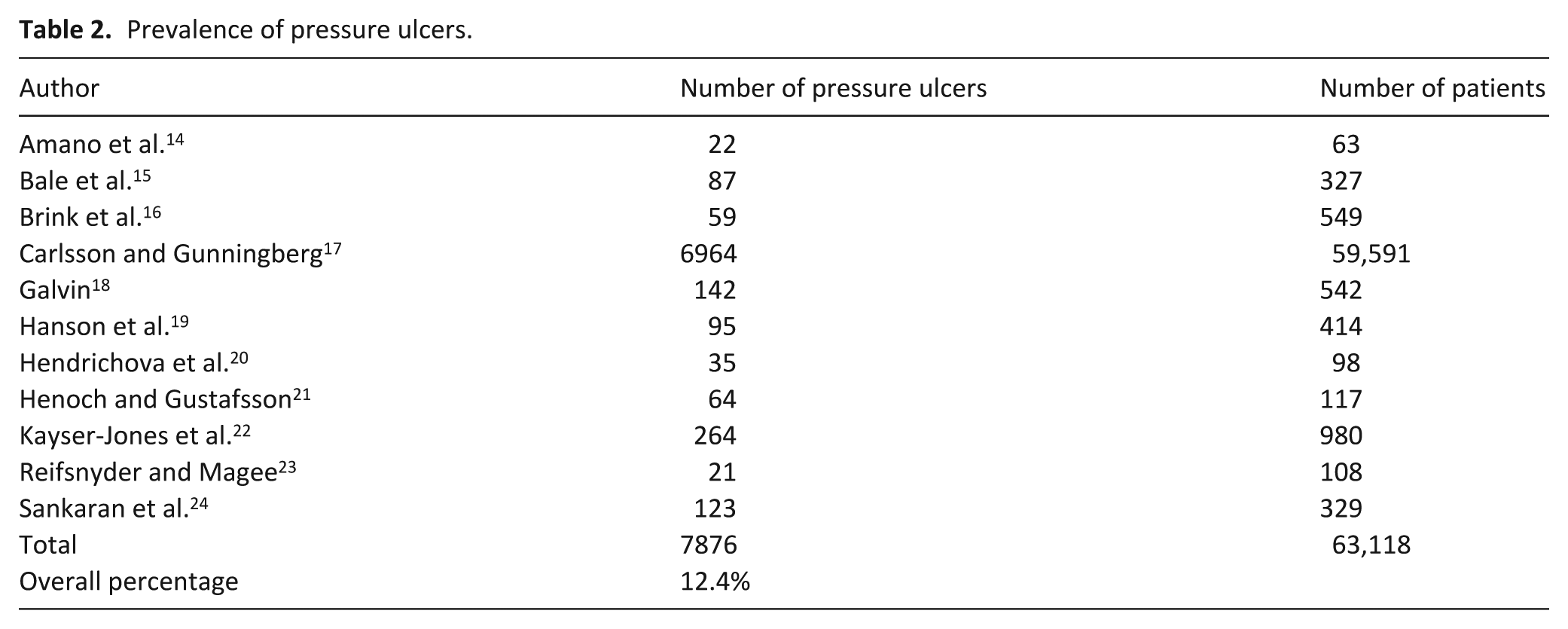
Pooling of data revealed an overall prevalence of 12.4% (see Table 2), with a range of 9.9%–54.7%. This large range may be related to the varied settings and patient demographics. Figure 2 demonstrates the difference in prevalence rates seen in inpatient versus community settings, which overall is higher in nursing home residents compared to patients cared for at home or in hospital. Carlsson and Gunningberg 17 included data from a range of care settings, demonstrating variability in the risk of pressure ulcer formation. Nursing home prevalence was 6.9%–16.2% (depending on whether patients had short or long stays), compared to 13.8%–19% for inpatients and 10.2%–11% for patients managed at home. 17 Ten articles described pressure ulcer incidence with 319 new ulcers forming during the course of the studies. The overall incidence of pressure ulcers in the articles studied was 11.3% (range 0%–37.5%).
Prevalence of pressure ulcers.
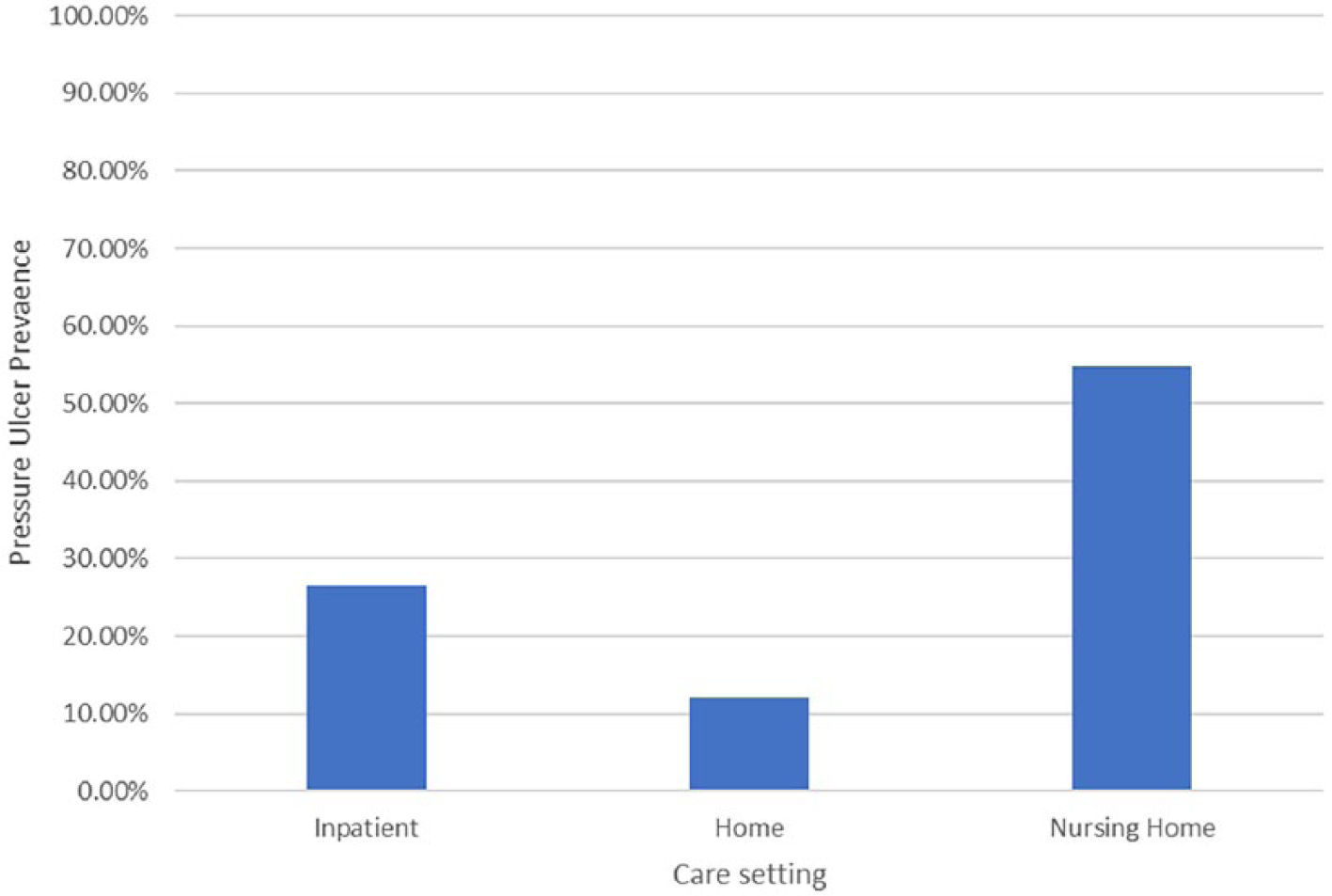
Prevalence of pressure ulcers by setting.
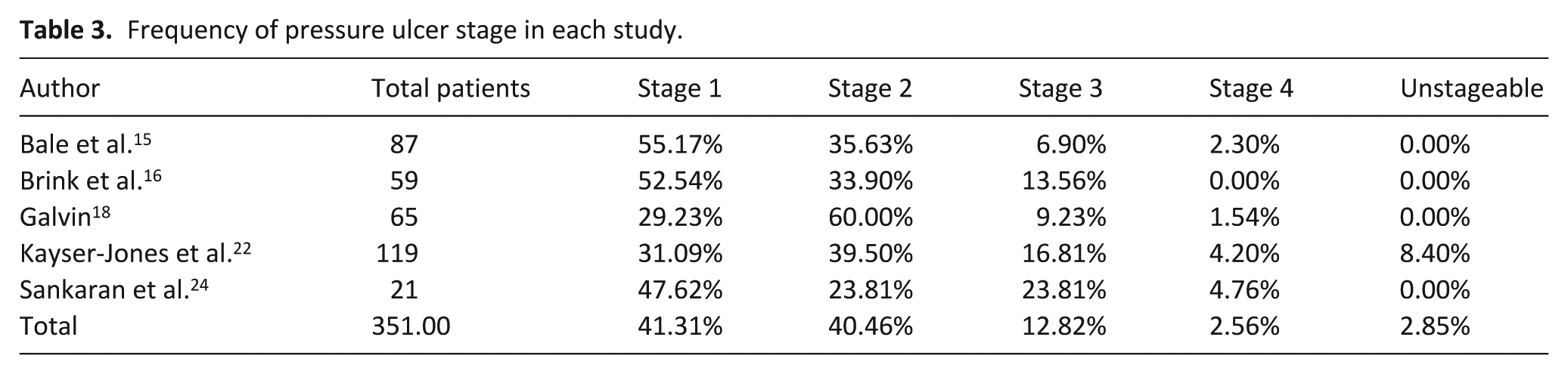
Stage and location
Five articles described pressure ulcer stages (see Table 3) and the majority (82%) were Stage 1 or 2 (see Table 4 for definitions of pressure ulcer stages). Unstageable was introduced as a new stage by the National Pressure Ulcer Advisory Panel (NPUAP) in 2007, so studies prior to this did not include this stage.
Frequency of pressure ulcer stage in each study.
Definitions of ulcer stage compiled from EPUAP. 1 .
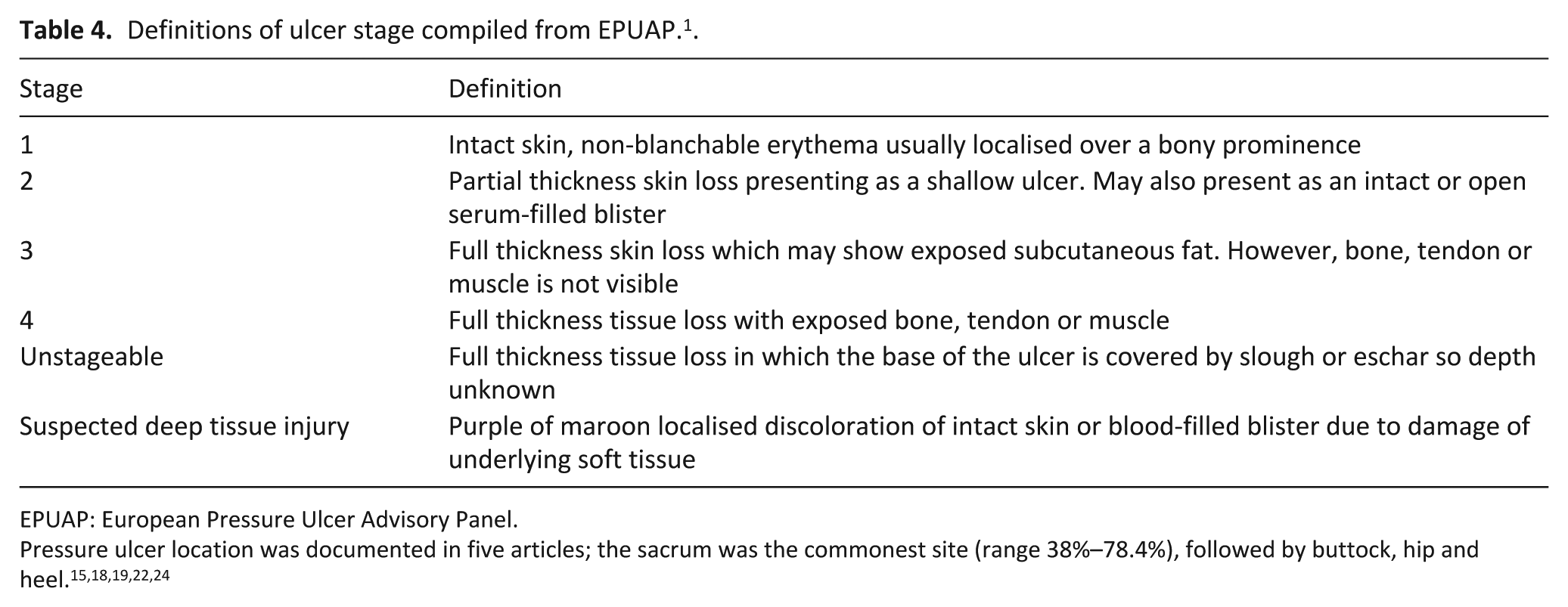
EPUAP: European Pressure Ulcer Advisory Panel.
Risk factors
Nine articles commented on possible risk factors for pressure ulcer development (see Figure 3). Worsening physical performance or immobility, advancing age, high Waterlow score and longer duration of stay were identified in more than one article. Worsening physical performance or immobility included a range of terms across the articles. Brink et al. 16 found that patients with limitation of their ability to carry out activities of daily living (ADLs) had a higher risk of pressure ulcers compared to those without limitations (odds ratio (OR) = 1.393). In the article by Hendrichova et al., 20 worse Karnofsky performance scale (severely disabled, very sick or moribund) accounted for 88% of patients with pressure ulcers, and Sankaran et al. 24 found 60% of patients with pressure ulcers had a form of paralysis (p = 0.03). Waterlow score is a validated tool to help stratify the risk of pressure ulcer formation and to guide caregivers towards appropriate preventive protocols. Galvin 18 demonstrated that a Waterlow score of >15 predicted 95.3% of pressure ulcers, and Sternal et al. 25 showed that those patients with pressure ulcers had an average score of 27.4, versus 23.6 for those without. Advancing age was identified as a risk factor in three articles, although there was a relatively small difference in age between those with and without pressure ulcers (79.9 vs 73.4 years, 20 76.43 vs 74.46 years, 23 and 70.9 vs 62.9 years). 21 Duration of stay was identified in two articles, where the average stay for those with pressure ulcers compared to those without was 31 versus 24 days 21 and 57.2 versus 37.4 days. 20
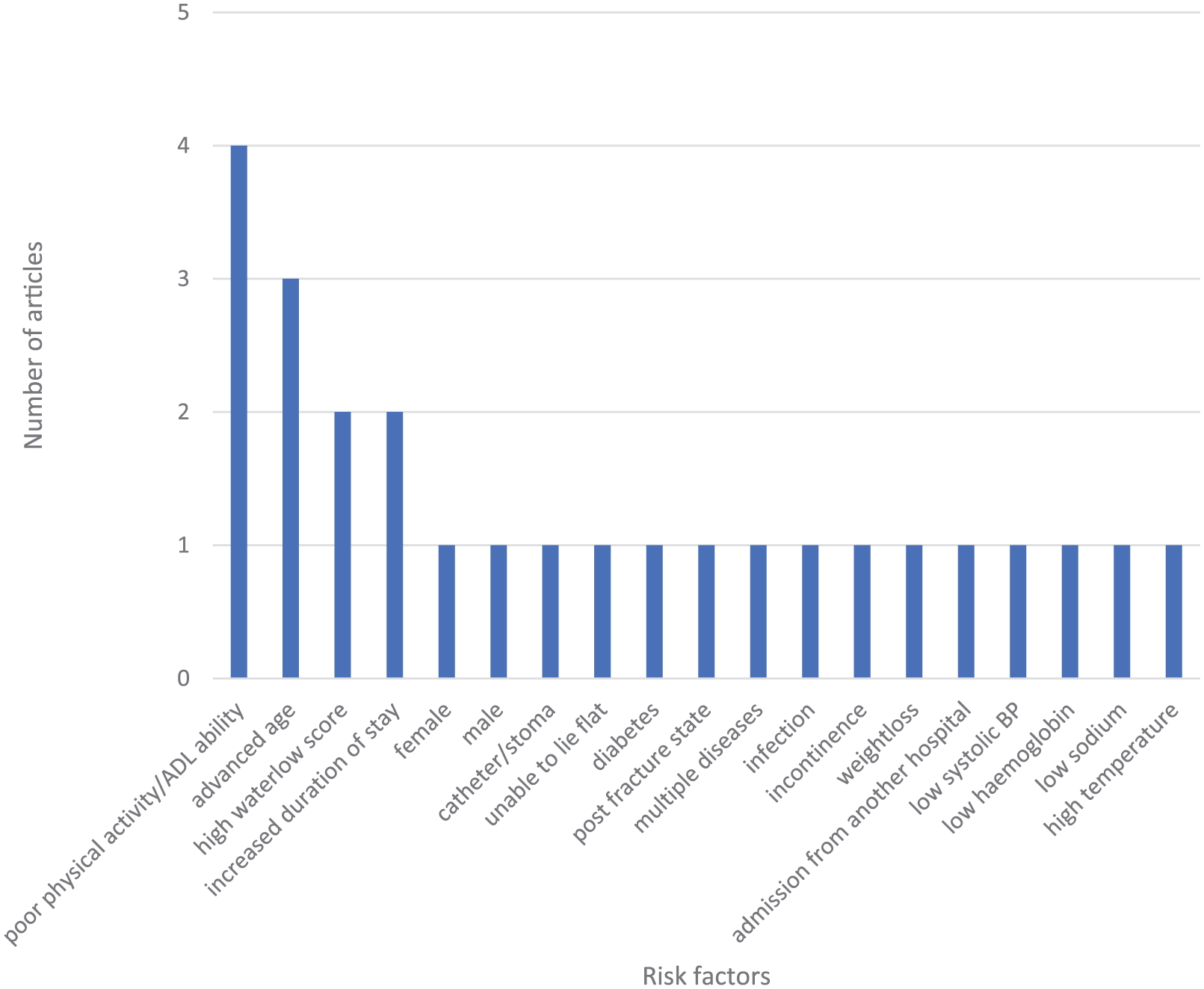
Risk factors for pressure ulcer development that were found to be statistically significant (p < 0.05).
Timeline
Four articles included information on the time to pressure ulcer formation and/or time between ulcer formation and death. The variable methods of reporting made it difficult to interpret and combine the data. Hanson et al. 19 found that 62% of pressure ulcers developed within 2 weeks of death despite ulcers forming any time between 1 and 139 days from admission. Hendrichova et al. 20 found that 53.5% of new ulcers developed within 6 days of death, whereas Kayser-Jones et al. 22 identified a mean of 66.8 days from pressure ulcer formation to death. Henoch and Gustafsson 21 also recorded data on time from ulcer formation to death but used median (12 days, range 1–59 days) rather than mean making it difficult to draw direct comparisons between articles.
Discussion
Main findings
This systematic review aimed to explore pressure ulcer development in patients at the end of their life receiving palliative care, focusing on incidence and prevalence, risk factors and timing. The literature contains a range of descriptions of skin breakdown around the last days to weeks of life, ranging from Kennedy terminal ulcers to pressure ulcers of varying stage and skin failure,26–28 which may all be features along a spectrum of tissue damage that can be found in a variety of physiological states, including terminal illness. The NPUAP advises that in those who are actively dying, ‘prevention and treatment of pressure ulcers may be superseded by the need to promote comfort by minimising turning and repositioning’. 8 However, identifying the time when a patient is actively dying can be challenging to even the most experienced clinicians. Conversely, pressure ulcers themselves can cause significant pain and distress so their avoidance in patients for whom comfort is a priority is important. A better understanding of these processes would allow clinicians to help their patients make informed choices about their pressure relief, continence care and use of pressure relieving devices at the end of life.
This review identified an overall prevalence rate of 12.4% for pressure ulcers in patients receiving palliative care. This is higher than the prevalence of 4.7% quoted by NICE in 2013, which they calculated from patient safety thermometer data for 186,000 patients in community and inpatient settings. 29 Taking only the UK-based studies included in this review to allow for a more direct comparison, the prevalence is even higher, at 25.3%. This suggests that the palliative population are more likely to experience pressure ulcers when compared with the general population. Pooling of data on prevalence in different settings demonstrated that the prevalence was higher in nursing home residents versus patients cared for in their home or in hospital. This could be due to nursing home residents generally having higher care needs and reduced independence and mobility increasing the risk of ulcer formation. However, Carlsson and Gunningberg 17 included data from a range of care settings that did not have similar findings, as the nursing home prevalence was 6.9%–16.2% (depending on whether patients had short or long stays), compared to 13.8%–19% for inpatients and 10.2%–11% for patients managed at home.
The incidence of pressure ulcer formation was 11.3% overall in the articles studied. There are very little national or international data available on pressure ulcer formation in the general population for comparison, especially for the community setting. Even if incidence data for community patients is excluded from analysis, the studies in this review identify an overall incidence of 11% for inpatient settings. This figure is still much higher than those reported by Sardo et al. 30 and Jenkins and O’Neal, 31 who recorded an incidence of 3.4% and 0%–5.4%, respectively, for the wider inpatient population, again suggesting that pressure ulcer occurrence is greater in palliative patients compared with the wider inpatient population.
The types of pressure ulcer seen most frequently in the palliative population are comparable with those seen in the wider patient population. In this review, stage 1 and 2 pressure ulcers were the commonest, accounting for 82% of all ulcers, which is similar to the findings of a recent national audit of pressure ulcers in hospitals in Wales identifying stage 2 ulcers as the most frequent. 32 Although pressure ulcer location was varied, the sacrum was consistently shown to be the commonest location (29%–78%), which is in keeping with a review by Ricci et al. 3 showing that 36% of pressure ulcers occurred here in the wider patient population.
The varied lists of risk factors for pressure ulcer formation identified in this review highlight how challenging it can be to draw conclusions from observational research for complex individuals with multiple pathologies. Poor physical activity, advancing age, increased duration of stay and high Waterlow score were the factors identified as being most significant in this population. It is worth considering whether these risk factors are actually features of a dying patient rather than risks for an ulcer and demonstrate a patient entering multiorgan failure, with skin failure as an element of this dying process.27,33 In 2009, a consensus statement was produced by a panel of experts stating that ‘skin changes at life’s end (SCALE)’ were recognised as a consequence of physiological changes happening in severe illness, and as such may be inevitable despite optimal care. 13 While there are very few in vitro or in vivo studies confirming the molecular processes that lead to these skin changes, they are thought to occur due to reduced local tissue perfusion (a response to systemic illness) and localised changes to inflammatory processes. 34 Information on time from ulcer formation to death may be helpful to further evaluate the theory that skin failure is an inevitable part of the dying process. Unfortunately only four articles provided timeline data, and while there appeared to be a general trend for the occurrence of pressure ulcers in patients entering the last days or weeks of life, the dataset was too small to be conclusive.
Furthermore, once an ulcer has developed, there are a number of factors that can impair healing, which may also be more prevalent in patients in the palliative phase of their illness. Impaired immune function, biochemical abnormalities, physiological stress, and systemic and local hypoxia are recognised features of critical and terminal illness and these also impair soft tissue healing. Healing may also be affected by medications used in this patient group, particularly those with underlying malignancy who may be receiving chemotherapy or steroids.10,12,35–37 Inadequate blood supply to the affected area can be compounded by hypotension or dehydration. Excess moisture impairs healing, and pressure ulcers can be contaminated with urine or faeces which can also introduce infection.2,35 Malnutrition is associated with worsening wound healing and is correlated with extent and severity of pressure ulceration. 2 As patients approach the end of life, appetite and thirst often reduce, nutrition becomes less of a priority as comfort becomes the focus of care and the underlying physiology switches to a catabolic state. Kayser-Jones et al. 22 found weight loss to be a statistically significant risk factor for pressure ulcer formation. Although there was no significant difference between patients with and without ulcers at entry to the study or at time of death, those with pressure ulcers had a mean weight loss of 30 lb compared with patients without pressure ulcers losing a mean of 6.9 lb. 22 Carlsson and Gunningberg 17 identified intravenous or enteral feeding as protective factors against pressure ulcer formation (OR = 0.703–0.976, p < 0.05) and Amano et al. 14 showed that patients receiving individualised nutritional support had a lower prevalence of pressure ulcers in the last 48 h of life although this was not statistically significant (14% vs 46%, p = 0.12). This last study should be interpreted with some caution as the patients self-selected for the intervention and the control group was not case matched, weakening the evidence.
While a number of these factors can be modified in palliative patients as in any other patients (e.g. use of pressure relieving devices, regular turns in line with comfort, encouraging adequate nutrition and hydration, careful manual handling strategies and impeccable skin and continence care), these factors cannot be mitigated completely and in many patients the desire for comfort and minimal disruption may take priority, making pressure damage or poor healing more likely. Awareness of risk factors and use of risk assessment tools to highlight and quantify these risks are only in themselves useful if this then informs a change in the care delivered to the patient. In the included articles, there was little information on the effectiveness of pressure injury prevention strategies in this population, or indeed how acceptable these were to patients and their carers. For instance, in the study by Bale et al., 15 patients received an appropriate pressure relieving mattress based on their risk scores and following this, pressure ulcer incidence fell from 22.4% to 2.5%. However, the study did not include patient satisfaction or quality of life data on using the specialist mattresses, which may have provided some useful insight on the applicability of this intervention for the palliative population.
Limitations
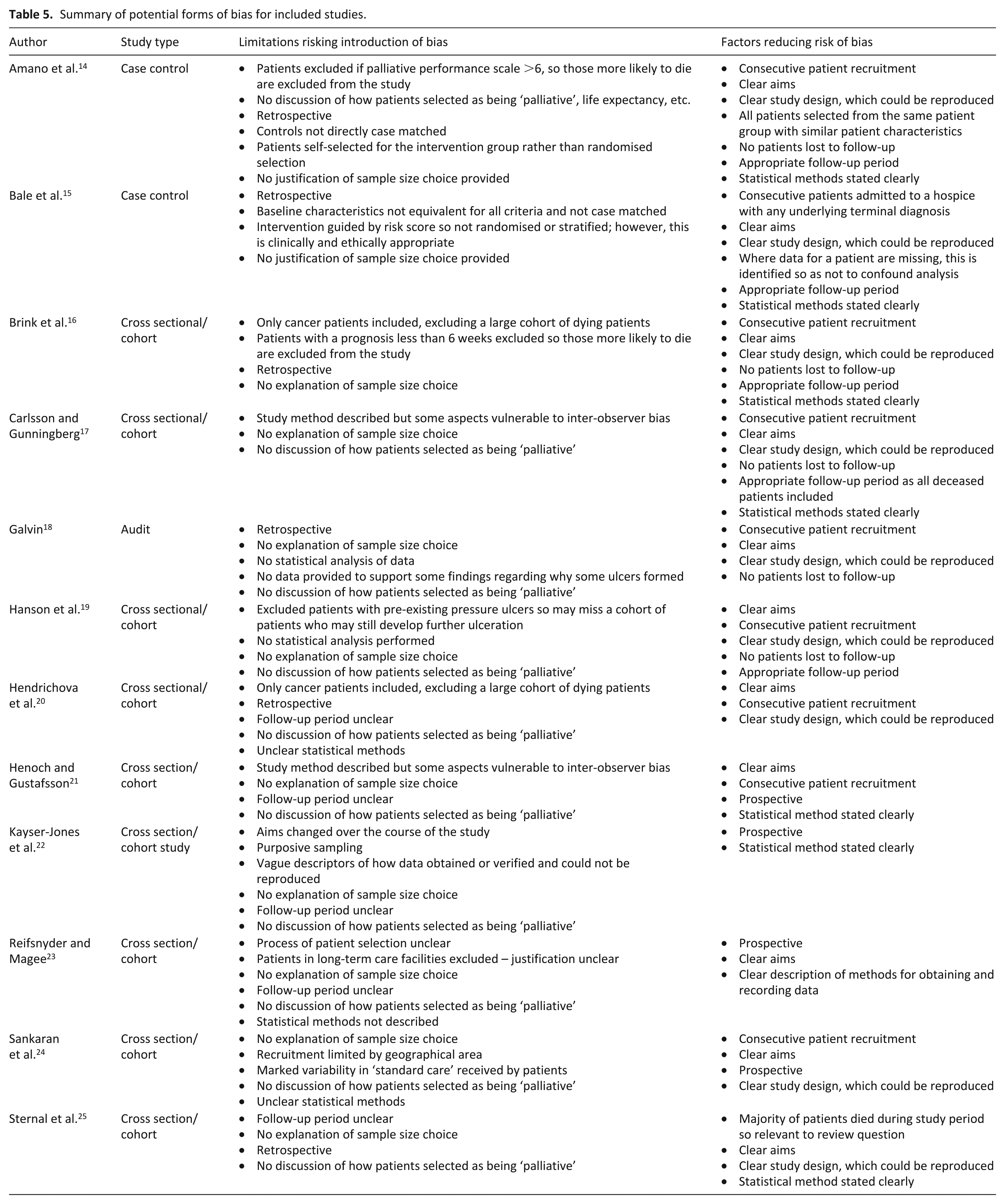
Due to the ethical limitations of performing trials in dying patients, there is a lack of randomised control trial or robust case control data for pressure ulcer formation or prevention in this population. Generally, the quality of data presented was poor. Specific methodological issues for each study that are likely to introduce bias are shown in Table 5. Most of the identified articles described retrospective or prospective observational data, which are vulnerable to reporting bias and confounding factors. Retrospective studies depend on the accuracy of the original notes or databases used to gather data, which can affect their reliability. The groups of patients included in the studies were relatively heterogeneous. While this is realistic as a real-world example of the patients, it does lead to challenges in interpreting the significance of findings in this group and their implications for the wider population. Four studies only included patients with an underlying malignancy,14,16,20,24 which is not necessarily representative of the large number of frail elderly patients dying of chronic health conditions that are increasingly requiring palliative care. Reifsnyder and Magee 23 excluded patients who were residents of long-term care facilities, which would again not be representative of the dying population as a whole. All of the articles studied included patients with the label of being ‘palliative’; however, no definition of this broad term was provided and patients were not necessarily in the last days of their life when they were studied. The mortality rate was only described in five articles and ranged from 77.8% to 98%.18,20,21,23,25 The follow-up time was also variable, and therefore some pressure ulcers may have been missed in shorter studies. Selection bias was a potential issue for the epidemiological study by Kayser-Jones et al., 22 which used purposive rather than random or stratified sampling to select patients and was initially not designed to look at pressure ulcers specifically. Similarly in the article by Amano et al., 14 patients were self-selected for intervention meaning the case control study was not in fact control-matched to allow like-for-like comparison. Risk factors highlighted in this review were described as being statistically significant in the original articles; however, statistical methods were rarely described in detail and were not necessarily clinically relevant. For example, Sternal et al. 25 found a correlation between pressure ulcer risk and an increased temperature, but a mean evening temperature of 36.9°C compared to 36.7°C is more likely to represent physiological variation rather than a true difference in the condition of the patients and is not a practical therapeutic target to reduce risk of ulcer formation.
Summary of potential forms of bias for included studies.
What this review adds and future considerations
In this review, we have demonstrated that pressure ulcers are more prevalent in patients receiving palliative care compared with the general population, supporting the theory of skin failure and skin changes at life’s end described in the wider literature.9,13 Given the increased likelihood of pressure injuries in this patient population, we suggest a re-evaluation of the appropriateness of including palliative patients in the NHS safety thermometer reporting system for pressure ulcers as one of the ‘most common harms occurring in healthcare’. 38 Their formation, as we have discussed, may in fact be an inevitability for some patients or a result of an informed decision by the patient and carers to prioritise comfort over pressure relief. Failure to recognise this as an issue has the potential to seriously damage reputations of individuals and organisations alike, as currently any pressure damage is viewed as a failure of care and for stage 3 and 4 injuries is often viewed as neglect.
There is a lack of large robust studies looking at the prevalence and incidence of pressure ulcers in the palliative population. National point prevalence audits may be the first step in quantifying the scale of the problem in comparison with the general population, but ideally multicentre observational data covering a large population of patients are needed to further evaluate the risk factors for pressure ulcer formation. This would allow the consideration of appropriate preventive strategies in the context of maintaining patients’ dignity and comfort. In addition, pressure ulcers occurring as a result of unavoidable disease states can be accepted and managed appropriately, rather than being viewed as a failure of care. Qualitative research considering the views of palliative patients and their families on pressure relieving strategies and devices and their effects on quality of life are also necessary to determine the applicability and acceptability of interventions.
Conclusion
As patients approach the end of their life, treatment goals change from curative and life prolonging to comfort and supportive care, even if this may make death more likely as a consequence (the doctrine of double effect). This should include wound management, and modifying approaches to dressing changes, wound debridement, continence care, pressure relieving equipment and turning, among others factors, may be necessary. This review has shown that pressure ulcer prevalence is higher in palliative patients compared with the general population, especially for those in nursing homes, although the reason for this is not clear. While these findings should not be used as an excuse for poor practice, we suggest that pressure ulcer formation in this population may not always reflect the standard of care and may instead be a feature of complex circumstances, some of which are not modifiable. As such, skin failure, as with other organ failures, may be an inevitable part of the dying process for some patients.
Footnotes
Appendix 1
Search terms used for search strategy.
Terms marked with ‘*’demonstrate a truncation search to include all variations on that root word including plurals.
Author Contributions
Dr Amy Ferris designed the review and constructed the search criteria as well as performed the initial database search. Dr Ferris critically appraised the articles for inclusion and performed data extraction and analysis. Dr Ferris also drafted the published article. Dr Annie Price contributed to the review design, reviewed articles for inclusion and performed data extraction and analysis as the other independent reviewer. Dr Price revised the article for intellectual content and made appropriate amendments. Professor Keith Harding provided guidance and revised the article critically for intellectual content. All three authors have approved the final version for publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.