
Abstract
Background:
Determining the effect of caregiving and bereavement remains a challenge. To date, no study has employed a comparison group to investigate caregivers’ grief, quality of life and general health in relation to non-caregivers.
Aim:
We aimed to determine how caregivers’ grief, quality of life and general health changed following death compared to non-caregivers and whether pre-death grief predicted these outcomes.
Design:
A prospective, longitudinal study of family caregivers and a comparison group matched for age, gender and postcode was conducted. All participants completed questionnaires at four points – once pre-death and three times post-death (3–4 months, 6–7 months and 9–10 months).
Setting/participants:
Participants (N = 70) were family caregivers of persons receiving palliative care, mostly for cancer, recruited from three palliative care providers in Western Australia and matched comparisons recruited from advertisements.
Results:
There were significant differences between the caregivers’ and comparisons’ grief, general health and quality of life at pre-death, 3–4 months and 6–7 months post-death, but not at 9–10 months post-death. The rate of progression in these constructs following death was independent from the intensity of pre-death grief. However, caregiver prolonged grief score significantly predicted prolonged grief score at 6–7 and 9–10 months post-death.
Conclusion:
It took 9–10 months for the caregivers’ grief, general health and quality of life to correspond to the comparison group. These findings present an opportunity for palliative care research and practice to consider how best to support the majority of caregivers without grief complications so that their pre- and post-death support needs are realised.
What is already known about the topic?
Informal caregivers are central to the provision of end-of-life care.
The experience of caregiving is well-documented, but little is known about the effect of caregiving on bereavement outcomes.
Studies investigating the effects of caregiving and bereavement are limited by a lack of an adequate comparison group.
What this paper adds?
Caregiving significantly affected caregivers’ grief, quality of life, and general health and it took nearly a year for caregivers to adapt to the impact of caregiving and bereavement.
While caring, the caregivers’ quality of life and general health was impaired and their grief was comparable to that at 3–4 months post-death.
Implications for practice, theory or policy
Research and practice must consider the support needs of the majority of caregivers with normal grief.
Comprehensive, systematic and repeated assessment of grief and the provision of tailored support, both before and after death, are needed.
Introduction
Informal caregivers are integral to end-of-life care. 1 Family caregivers report physical and emotional exhaustion,1,2 limited participation in social and recreational pursuits, 3 difficulties preparing for the death of the person for whom they care, 4 and positive aspects of caregiving. 5 A small proportion of caregivers, about 6%–8%, may experience persistent and pervasive grief distress called Complicated Grief or Prolonged Grief Disorder (PGD).6–8 PGD is associated with increased risk of suicide, 9 serious illness,10,11 sleeping problems, 12 social and occupational impairment, 13 and lower quality of life (QoL). 10 Although these outcomes of caregiving are well-documented, determining the effects of caregiving and bereavement remain a challenge.14,15
There is an increasing emphasis on identifying pre-death risk factors of post-death outcomes in caregivers. Studies indicate that high pre-loss grief, determined using a range of measures, is associated with post-loss grief, 16 depressive symptoms, 17 subjective stress 18 and PGD.19–22 One study reported that grief and depressive symptoms were higher during caregiving than 6 months after the loss and showed that severe pre-loss grief and depressive symptoms predicted post-loss complicated grief and depressive symptoms. 8 A systematic review of studies in end-of-life caregiving showed that higher pre-loss grief was associated with higher grief post-death. 23
Demographic factors are less strongly associated with PGD than is pre-loss grief.8,19,20 Characteristics of patient illness, care at end-of-life and circumstances of death do not appear to be associated with PGD. 24 Pre-loss factors associated with post-loss PGD include poor preparation for death,22,25,26 a short caregiving duration, 27 fewer years of education,8,20,22,28 depressive symptoms,16,28 being a partner/spouse,8,20 a history of mental health issues 29 and limited social support.22,27,30 Some studies indicate that caregiver age20,28 and gender31,32 are associated with PGD, but other studies report no such association. 8
The literature on the effects of caregiving and bereavement is hampered by a reliance on cross-sectional and retrospective research designs. Few studies have longitudinal designs with pre- and post-death data collection, 23 and few assessed pre-post grief over four or more time points; one study looked at dementia caregivers, 33 but not palliative care specifically. In addition, no study had a comparison group (matched to family caregivers) to determine the full effects of caregiving and bereavement, although one study did compare the caregivers’ QoL scores with age-matched normative data and showed that caregivers’ QoL was lower while caring and at 2 months post-death than the general population. 34 A comparison group is important because caregivers may be highly distressed upon bereavement due to the tasks of caring. Thus, even if a former caregiver’s distress decreases post-death, it might not be indicative of adaptive functioning.
The aim of the study was to determine the effects of caregiving and bereavement on family caregivers of patients receiving palliative care. Prospective, longitudinal studies are required to investigate caregivers’ needs along the caregiving and bereavement trajectory and to also inform the development and implementation of appropriate and targeted interventions.8,35 In addition, comparing caregivers to a non-caregiving group (matched for age, gender and postcode) allows the caregivers’ general health and QoL to be compared to a normative group. 14 We posed two research questions:
Does family caregivers’ pre-death grief predict post-death adjustment?
How do the caregivers’ grief, QoL and general health change over time compared to non-caregivers?
Method
The study was approved by the ethics committees of South Metropolitan Health Service (Ref. number: 12/284), Hollywood Private Hospital (Ref. number: HPH378) and Curtin University (Ref. number: HR131/2012).
Setting
The study was undertaken from 2013 to 2016 in three specialist palliative care services in Western Australia—a private hospital providing in-patient palliative care in a metropolitan area, a public hospital providing consultative palliative care in a metropolitan area and a community-based palliative care service in a public hospital in a regional area.
Design
The Caregiving and Bereavement study was a prospective, longitudinal study of family caregivers’ bereavement. 36 Family caregivers completed questionnaires at four data collection points: once before the death (Time 1) and three times post-death—3–4 months (Time 2), 6–7 months (Time 3) and 9–10 months (Time 4) post-death. At the first data collection point, caregivers were invited to participate in a face-to-face, semi-structured interview about preparedness for bereavement. 4 A comparison group completed related questions at the same time points.
Participants
Caregivers were recruited from the three specialist palliative care services, in collaboration with healthcare staff. To be included, caregivers had to be aged 18 years and over, be an informal caregiver of a patient receiving palliative care and the patients’ health had to be described by the treating healthcare team as ‘stable’. 37 Caregivers were ineligible if they exhibited cognitive decline, as determined by the healthcare team and/or did not speak or understand English.
Comparisons were recruited via advertisements on a university radio station, advertisements in print media and flyers placed on community noticeboards. They were ineligible to join the study if currently, or in the previous 2 years, they had (1) cared for anyone with a life-limiting or terminal illness or (2) they had been bereaved.
Measures
Grief
The Hogan Grief Reaction Checklist (HGRC) is a 61-item measure of the multidimensional nature of grief and comprises six factors: despair, panic behaviour, personal growth, blame and anger, detachment, and disorganisation. 38 The measure does not require participants to evaluate symptoms specifically in relation to a deceased person and is therefore appropriate as a pre- and post-death measure of grief.
Prolonged grief
The Prolonged Grief-12 (PG-12) caregiver version is a 12-item measure of caregivers’ prolonged grief arising from the impending death of a loved one 39 (Time 1 only). The Prolonged Grief-13 40 is a 13-item measure of symptoms of PGD in bereaved people at least 6 months after death (Times 3 and 4 only). Scores of 36 or more or the presence of all five diagnostic criteria indicate the presence of PGD (personal communication with the developer).
QoL
The QOL Index is a two-item instrument measuring QoL. 41
General health and well-being
The Short Form Health Survey (SF-12v2) is the standard 12-item measure of general health and well-being, with eight subscales: physical functioning, role limitations due to physical problems, role limitations due to emotional problems, bodily pain, general health perceptions, vitality and social function. 42
Procedure
Recruitment to the study occurred over a 20-month period, which was slower than anticipated. Data collection at Times 2–4 could only occur after the patients’ deaths and was completed 17 months after recruitment ceased. Date of patient death was provided by the relevant palliative care provider and the questionnaires for Times 2–4 posted from the university to the bereaved caregivers. Each questionnaire pack included an invitation letter, a detailed information document, consent form, questionnaire, list of support services and a reply-paid envelope. Participants had the options of completing it on their own, with the researcher over the telephone or in person at a mutually convenient venue. Pilot testing showed that the questionnaire took 20–30 min to complete.
The comparisons responded to advertisements and were asked to confirm that they were not currently, or in the previous 2 years, caring for anyone with a life-limiting or terminal illness or had been bereaved. They then were asked to provide their date of birth, gender, and postcode, and contact details, and were asked to join the study if their age, gender and postcode matched a caregiver (some were matched to two caregivers). The comparisons received their questionnaires in the mail and posted their completed questionnaires back to the university in reply-paid envelopes. All participants received an AUD$50 voucher after completing the final questionnaire.
Statistical analyses
The caregivers’ PG-12 scores were calculated at Time 1. 43 The PG-13 was used to determine PGD diagnostic criteria and the total symptom score at Times 3 and 4. To answer the research questions, data were analysed using linear mixed models (LMMs) as implemented in the ‘nlme’ package in R 3.5.1. To improve the likelihood of convergence, a separate LMM was estimated for each outcome (HGRC for grief, QoL for quality life and SF-12v2 for general health). Each model was specified with a fixed effect of ‘Time’ (assessment time point), ‘Group’ (Comparisons or Caregivers) and the interaction of the two. The main effect of ‘Group’ represents the difference in mean between comparisons and caregivers at Time 1. The effect of ‘Time’ represents the average amount of change between each time point in the comparison group. Finally, the ‘Time × Group’ interaction is then the difference in the average amount of change over time between comparisons and caregivers. A random intercept and a random effect of ‘Time’ were included for each participant. Given that the data represents repeated measurements of the same individuals, an autoregressive structure was applied to the residuals (AR1). This assumes that measurements that are closer together in time will be more strongly correlated than those further apart. Statistical power for this approach was estimated using the ‘powerlmm’ package 44 with an alpha level of 0.05. An LMM estimated with a caregiver group of n = 38 and comparison group of n = 32 measured at four time points had a power level of 0.82 to detect a medium effect (equivalent to Cohen’s d = 0.5).
For the QoL and general health models, the pre-death grief (HGRC) score and its interactions were included as fixed effects to assess how pre-death levels of grief affect the caregivers’ post-death adjustment. For the grief model, analogous interpretations can be made by inspecting the correlation between the random intercept and slope. This correlation also represents the relationship between the caregivers’ pre-death levels of grief (their intercept) and their post-death changes in grief (their slope). Additional models with just the caregiver data were computed to determine if their PG-12 score (Time 1) predicted changes in grief, quality life and general health at Times 2–4 or predicted prolonged grief score at Times 3 and 4.
Results
Characteristics of the sample
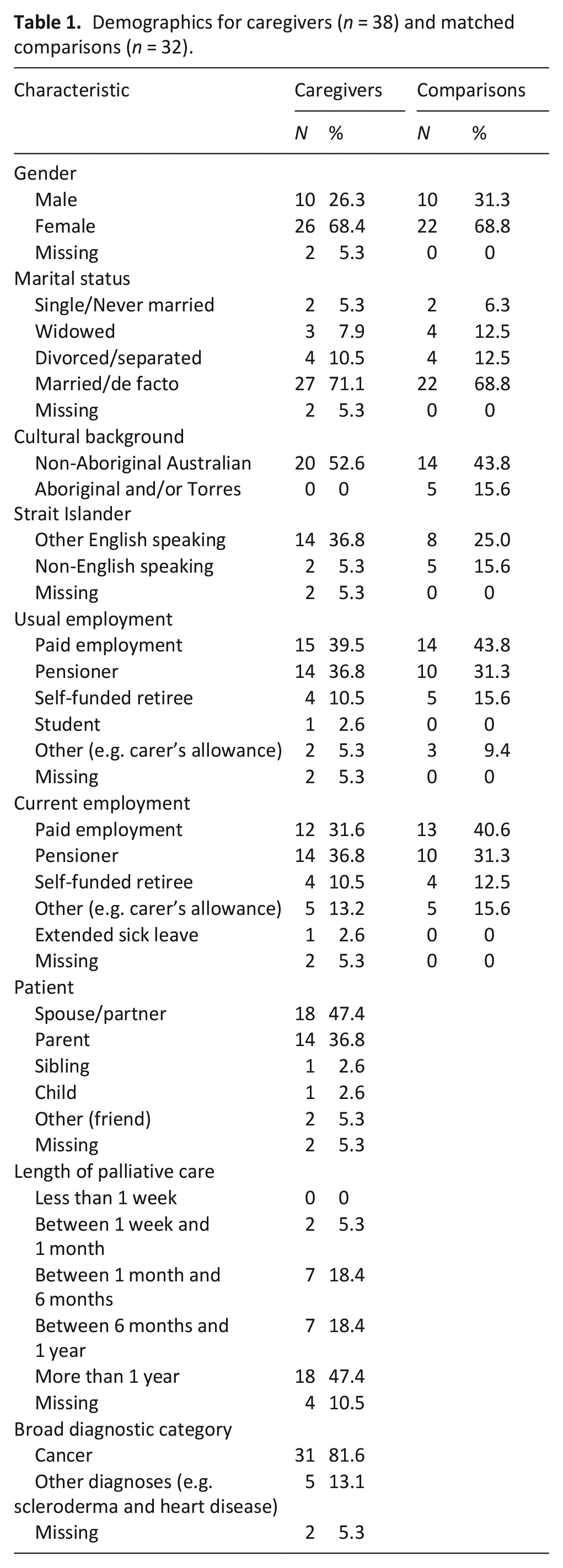
Participants (N = 70) were caregivers (n = 38) and matched comparisons (n = 32). The caregivers were aged 41–77 years (M = 59.25, SD = 10.79). The comparisons were aged 41–82 years (M = 60.53, SD = 9.41). See Table 1 for demographics by group. Fisher’s exact tests showed there were no significant differences between the two groups on any variable. For caregivers, the time between completing the Time 1 questionnaire and the date of death ranged from 1 to 265 days (Mdn = 34). None of the caregivers met criteria or clinical cut-off scores for caregiver prolonged grief or PGD. The mean values and SDs for each measure are shown in Table 2.
Demographics for caregivers (n = 38) and matched comparisons (n = 32).
Descriptive statistics for each measure across time.
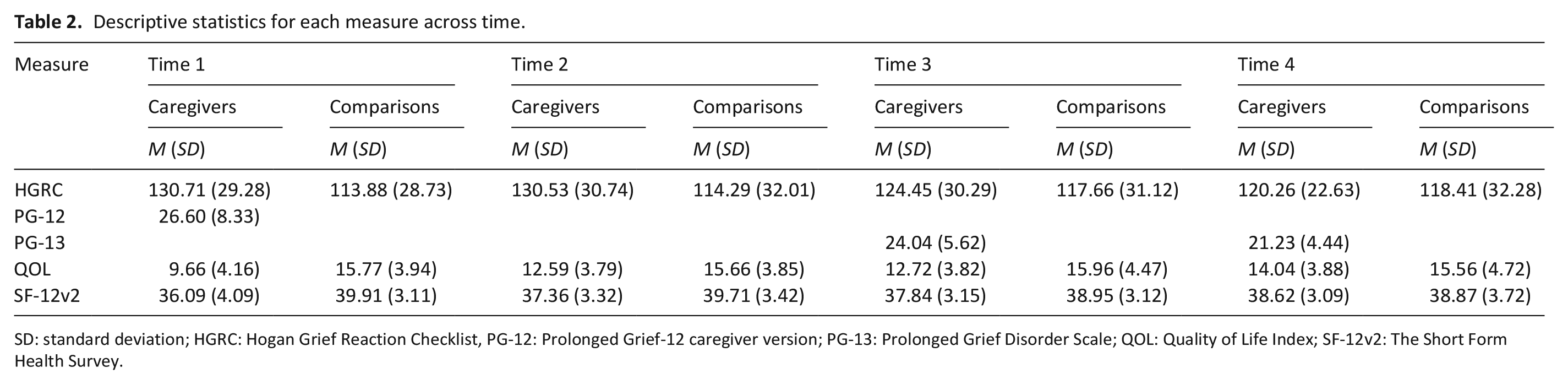
SD: standard deviation; HGRC: Hogan Grief Reaction Checklist, PG-12: Prolonged Grief-12 caregiver version; PG-13: Prolonged Grief Disorder Scale; QOL: Quality of Life Index; SF-12v2: The Short Form Health Survey.
Grief
The results of the LMM for grief indicated that, at Time 1, caregivers had significantly higher levels of grief than the comparisons (β = 17.56 (4.00, 31.12), p = 0.012). As would be expected, the level of grief in the comparison group did not significantly change over time (β = 1.59 (–0.90, 4.09), p = 0.209). In contrast, the level of grief in caregivers significantly declined over time (β = –4.51 (–8.14, –0.87), p = 0.015). Figure 1 shows the mean grief score for each group at each time point. To test if there was a difference between the two groups at the final time point, the ‘Time’ variable was rescaled in the LMM so that the intercept refers to the final time point. With this adjustment, the ‘Group’ coefficient then represents the difference between the caregiver and comparison groups at the final measurement, rather than the first. This re-scaled LMM indicates that the difference in grief between caregivers and comparisons at 9–10 months post-death was not significant (β = 4.03 (–10.87, 18.94), p = 0.591). The correlation between the intercept and slope parameters, however, was very weak: r = –0.059 (–0.53, 0.45), suggesting that the rate of change in grief in the post-death period was not related to pre-death grief. In addition, caregiver prolonged grief score (Time 1) did not predict changes in grief score (HGRC) over time. However, caregiver prolonged grief score (PG-12 at Time 1) significantly predicted PG-13 score at Time 3 (β = 0.56, p =< 0.001) and at Time 4 (β = 0.31, p = 0.014).
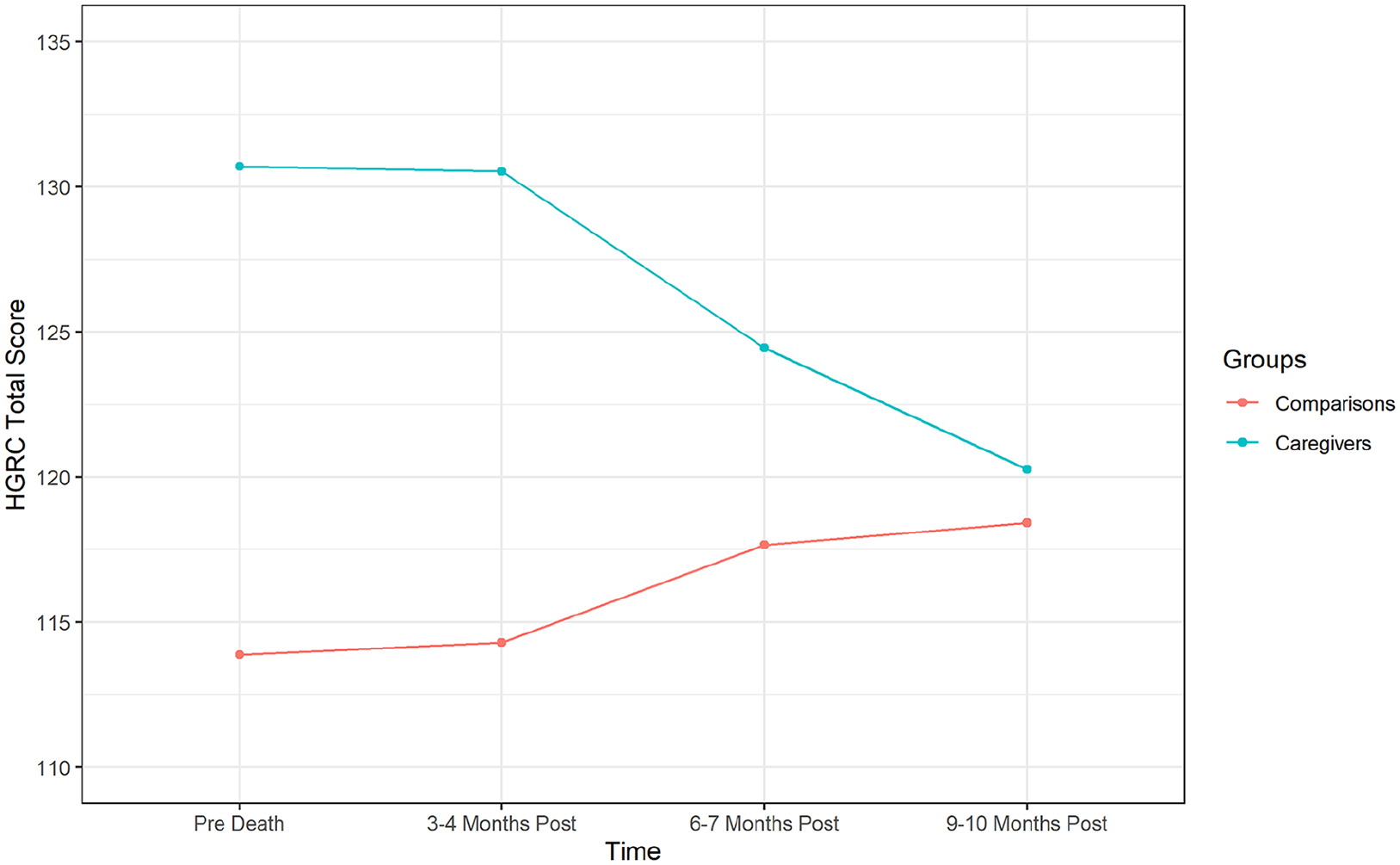
Caregivers’ and comparisons’ grief over time.
QoL
The LMM for QoL showed a similar pattern of results. At Time 1, caregivers demonstrated significantly lower levels of QoL than the matched comparisons (β = –4.85 (–6.61, –3.08), p < 0.001). The QoL in comparisons did not significantly change over time (β = –0.06 (–0.51, 0.40), p = 0.806), whereas it significantly improved over time in caregivers (β = 1.48 (0.83, 2.13), p < 0.001; Figure 2). As with the grief model, the mean level of pre-death grief was not significantly associated with the rate of change in post-death QoL in either the comparisons (β = –0.01 (–0.02, 0.01), p = 0.400) or the caregivers (β = –0.01 (–0.02, 0.02), p = 0.798). As with grief, this pattern of change would suggest that the differences in QoL between the two groups would no longer be significant at the final follow-up. The re-scaled LMM indicates that at 9–10 months post-death, there is no significant difference between caregivers and comparisons (β = 0.40 (–2.32, 1.51), p = 0.675). In addition, caregiver prolonged grief score (Time 1) did not predict changes in QoL over time.
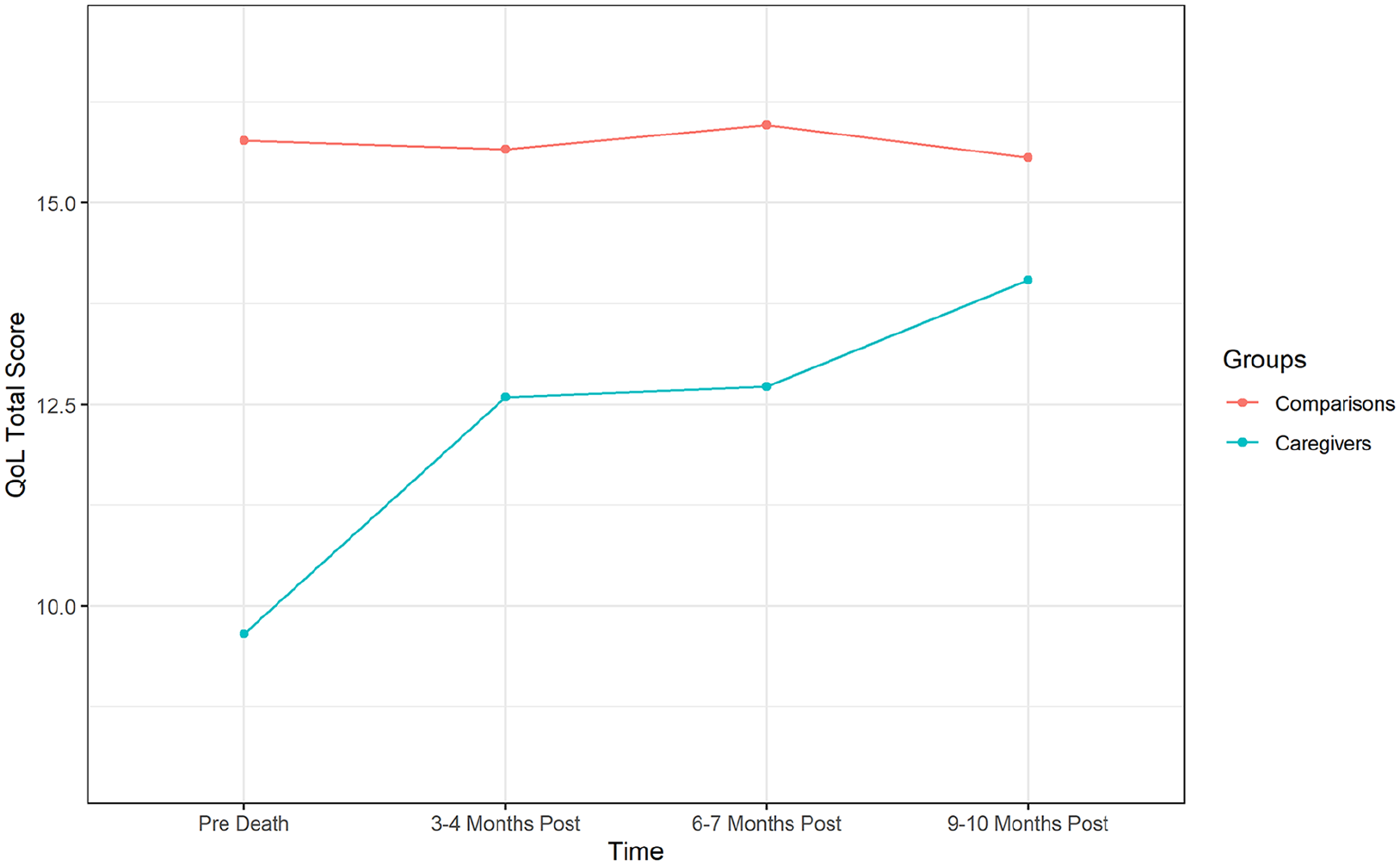
Caregivers’ and comparisons’ quality of life over time.
General health
The results for general health were consistent with those of grief and QoL. At Time 1, caregivers showed significantly poorer general health and well-being than the matched comparisons (β = –2.93 (–4.43, –1.42), p < 0.001). The comparisons again displayed no significant change over time (β = –0.34 (–0.76, 0.08), p = 0.109), while the health and well-being of caregivers significantly improved (β = 1.15 (0.59, 1.75), p < 0.001; Figure 3). There was also no relationship between the mean level of pre-death grief and the rate of change in post-death general health scores in either the comparisons (β = 0.01 (–0.01, 0.02), p = 0.721) or the caregivers (β = 0.01 (–0.01, 0.03), p = 0.568). Finally, the time-rescaled LMM showed no significant difference in general health and well-being between caregivers and matched comparisons at 9–10 months post-death (β = 0.53 (–1.03, 2.08), p = 0.501). In addition, caregiver prolonged grief score (Time 1) did not predict changes in general health over time.
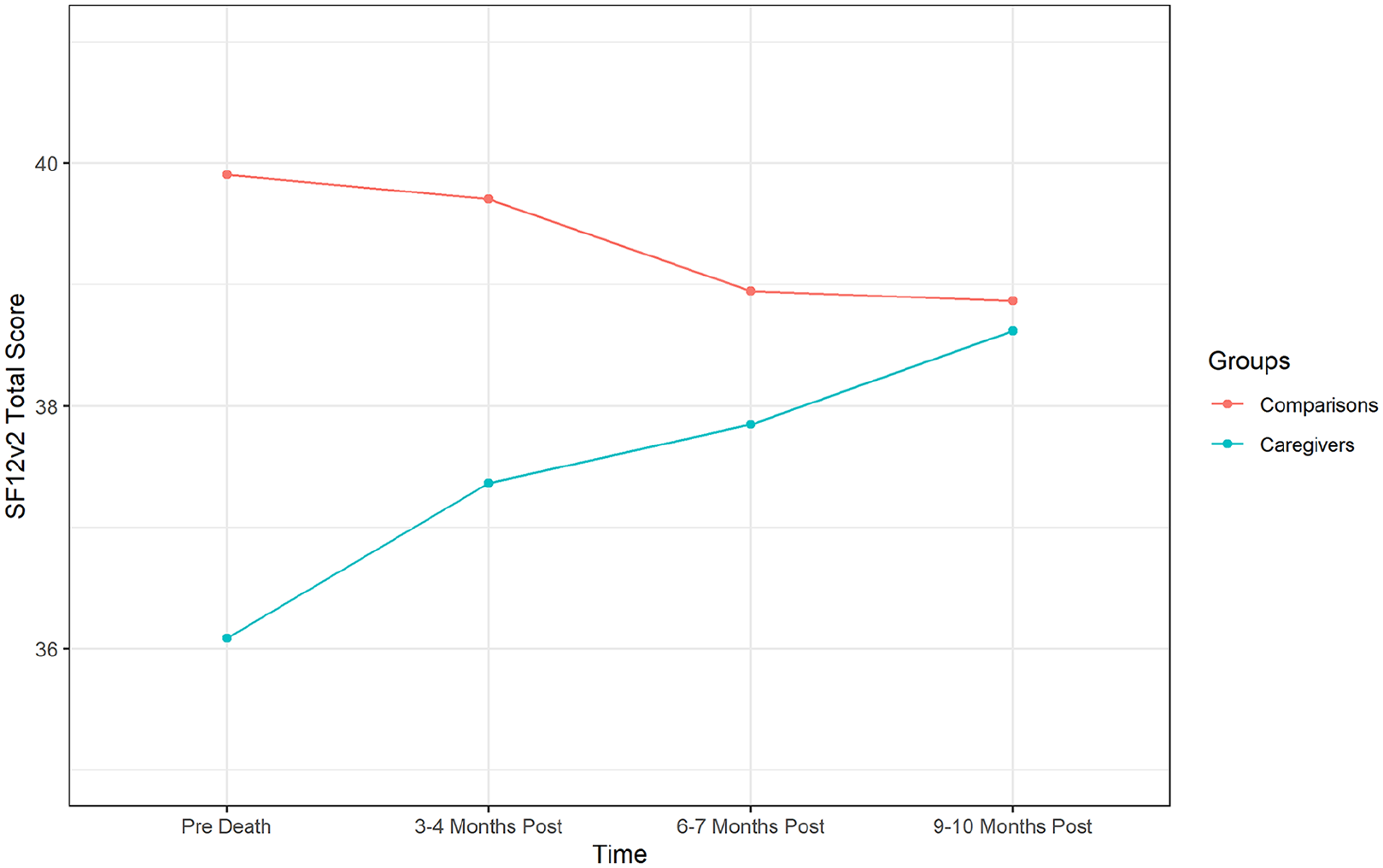
Caregivers’ and comparisons’ general health over time.
Discussion
Caregiving has a significant impact on caregivers. While caring, the caregivers’ QoL and general health was low in comparison to their post-death scores. Their grief while caring was comparable to that at 3–4 months post-death, and it took 9–10 months post-death for caregivers’ grief, QoL and general health to return to a normative standard. These novel findings present a challenge to research and practice that has moved towards focusing upon the small minority of bereaved caregivers with PGD and not on the more common experiences of grief. 45
The rate of change in grief, QoL and general health following death was unrelated to the intensity of pre-death grief, whether measured by the HGRC or the PG-12. Caregiver prolonged grief (PG-12) predicted post-death prolonged grief (PG-13) scores, and this finding aligns with previous studies showing the predictive utility of the PG-12.8,19–21 However, several factors contribute to prolonged grief symptoms post-death,20,22,25–27 which is why comprehensive, systematic and repeated assessment of grief, both before and after death, is recommended in research,20,23,46,47 policy 48 and practice guidelines. 49 Pre- and post-death support that is tailored to the needs of ‘normal’ grievers, who are the majority of bereaved caregivers, might best work in partnership with explicit and careful attention to promoting informal support, 50 and could focus on bereaved caregivers’ wishes for more information on preparing for bereavement, how to harness their social networks and developing strategies for dealing with grief. 51
This study demonstrates the need for palliative care services to support family caregivers while caring and after the death, including those with normal grief. Palliative care services are moving towards harnessing a suite of strategies to meet the varied support needs of caregivers pre-death. These strategies have benefits pre- and post-death, 52 but we should not overlook the importance of post-death support. Palliative care services already have contact with family caregivers, yet do not always systematically assess caregivers’ grief support needs prior to or after the patient’s death. One study showed that only 75% of caregivers were asked about their coping, 39.4% were asked about emotional or psychological problems and 62.9% were offered information about grief and bereavement services. 53 Following the death, only 50.9% received contact from staff about coping or questions they would like answered. 53 Services could therefore capitalise on the pre-death ‘window of opportunity’ to support caregivers 54 and to build relationships in order to offer appropriate post-death support.
Limitations
Due to attrition rates, gatekeeping and the passive recruitment of participants, which most often relies on clinician invitation, participant numbers in palliative care research are relatively small. 55 Our sample was smaller than expected, despite doubling the study’s recruitment duration and attempts to recruit from additional services. We have no information about caregivers who were not invited, or declined, to participate. To avoid participant burden, we did not systematically gather information about the supports the caregivers received to assist them with care. Given that invitations to participate came from service staff, it is possible that staff were more inclined to invite caregivers who were coping better and had less pre-death grief than those who were not invited; this could explain why none of the caregivers met criteria for pre-death prolonged grief or for PGD at 6–7 or 9–10 months post-death. This contrasts with population-based studies of bereaved people,6,7 a cohort study of bereaved caregivers in Denmark, 8 as well as an Australian study of palliative care caregivers, which reported that 6.7% of the sample at 6 months post-death and 11.3% at 13 months post-death met diagnostic criteria for PGD. 20
Patients’ imminent death has been reported by caregivers as a factor for declining study participation, 8 where in the aforementioned study, the median time from recruitment to patient death was 58 days compared to the much shorter period in our study (34 days), which could explain why recruitment was challenging. Our sample size and heterogeneity were hampered by a lack of systematic data collection relating to caregivers from their enrolment in palliative care to post-death follow-up, unlike some contexts where systematic data collection is the norm (e.g. Thomas et al. 20 ). A larger sample would also allow more complex statistical analyses related to identifying additional factors that could predict caregivers’ post-death outcomes.
Conclusion
The majority of family caregivers adapt well to bereavement. The number of prospective studies encompassing pre and post-death time points remains small, and this is the first to have a matched comparison group to determine the ‘true’ impact of caregiving and bereavement. Increasingly, attention is paid to predicting which caregivers may develop prolonged grief and less is known about the course of normative grief in this population. Our data show that caregiving significantly affects caregivers’ grief, QoL and general health, and it takes nearly a year for caregivers to accommodate and adapt to the impact of caregiving and bereavement. These findings may assist in developing the evidence base concerning bereavement care so that the pre- and post-death support needs of the majority of caregivers are addressed.
Footnotes
Acknowledgements
The authors acknowledge and express deepest gratitude to the participants of this study. The authors thank the palliative care services for their interest in this research and for assisting in recruiting participants.
Authorship
All authors made substantial contributions to the conception (L.J.B.) or design (L.J.B., S.M.A. and M.O.) of the study, to the acquisition (L.J.B. and D.H.), analysis (A.R.J.) or interpretation of data (L.J.B., S.M.A. and M.O.), or to the drafting and critical revision of the manuscript (L.J.B., S.M.A., M.O., A.R.J. and D.H.). All authors approved the final version of the manuscript and participated sufficiently in the work to take public responsibility for appropriate portions of the content.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was funded by an Australian Research Council Discovery Early Career Researcher Award (DE120101640).